detection and control of mrsa in healthcare facilities - who · detection and control of mrsa in...
TRANSCRIPT

Detection and control of MRSA in healthcare facilities
E. Tacconelli
Dept. Infectious Diseases
Catholic University, Rome, Italy

• EARS-Net (198 laboratories in 22 EU countries up to 2009): the number of bloodstream infections caused by S. aureus increased by 34%. However, the proportion of meticillin resistant isolates decreased.
1. Lack of awareness
Non-medical specialists
Junior doctors
Subspecialties of ID / CM
2. High level evidence not always available
3. Local implementation of international protocols not always possible

Road map
1. MRSA+ pt at hospitalisation
2. MRSA+ pt before surgery
3. MRSA+ pt during hospitalisation
4. MRSA+ pt at hospital discharge
5. MRSA+ pt in ambulatory setting

Tackling resistance of HA-MRSA
Prevention of
resistance
development
Antimicrobial
stewardship
1 - Pathogen
2 - Patient
Prevention of
infection
Screening
Surgical
prophylaxis
Decolonization
Prevention of
intrahospital
spreading
Patient
Isolation
Cohort
Contact prec.
Hand hygiene
HCW
Education
Individual
protection
Environment
3 – Hospital

Tackling resistance of MDR resistant bacteria
2 - Patient
Prevention of
infection
Screening
Surgical
prophylaxis
Decolonization

Colonisation precedes the infection
MRSA infections develop in 11% to 33% of colonized patients
Nasal carriage of MRSA increases risk of MRSA infections by 4 fold
Mest, Anesth Analg, 1994; Jernigan, ICHE, 1995; Sadfar, Am J Med 2008

Guidelines SHEA, 2003
CID / CAMS, 2004
HIS, ICNA, British Society of Antimicrobial Chemotherapy, 2006
Hospital-acquired MRSA
Center for Diseases Control and Prevention, 2007
MDR-bacteria
British Society of Infection Control, 2008 Prophylaxis and treatment update Community-acquired MRSA
Consensus ESCMID-ISC 2010
ECDC guidance document 2011 (under revision)
Harbarth, CMI 2010; Tacconelli CMI 2010; Garau CMI 2010

Paterson, JCM, 2010
Universal versus targeted screening

Multivariables risk factors screenings
Haley, J Clin Microbiol, 2007
Universal versus targeted screening

Collins, JHI 2011
Scotland challenges the UK..
Targeted vs Universal

Collins, JHI 2011
Scotland challenges the UK.. Targeted vs Universal

MRSA detection rates did not increase despite an exponential increase in lab workload
1-month period: 7 cases missed using targeted S&D approach. Detection of these additional pts: lab costs £20,000 / 4200 neg screens
Screening strategy based upon clinical risk is more pragmatic and more cost-effective than the universal programme
Scotland challenges the UK..
Targeted vs Universal

Type of test for MRSA screening
PCR-based vs chromogenic-based
Tacconelli, Lancet Infectious Diseases 2009

MRSA Decolonisation
Cookson et al., CMI 2010 ESCMID-ISC, Expert Consensus 2010
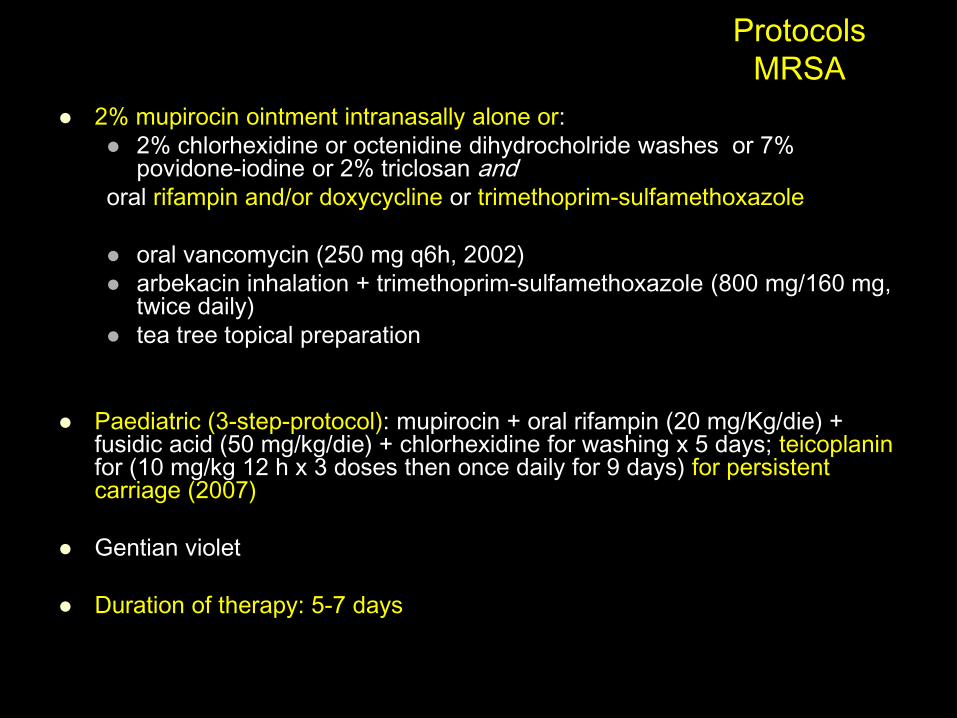
Protocols
MRSA
2% mupirocin ointment intranasally alone or:
2% chlorhexidine or octenidine dihydrocholride washes or 7% povidone-iodine or 2% triclosan and
oral rifampin and/or doxycycline or trimethoprim-sulfamethoxazole
oral vancomycin (250 mg q6h, 2002)
arbekacin inhalation + trimethoprim-sulfamethoxazole (800 mg/160 mg, twice daily)
tea tree topical preparation
Paediatric (3-step-protocol): mupirocin + oral rifampin (20 mg/Kg/die) + fusidic acid (50 mg/kg/die) + chlorhexidine for washing x 5 days; teicoplanin for (10 mg/kg 12 h x 3 doses then once daily for 9 days) for persistent carriage (2007)
Gentian violet
Duration of therapy: 5-7 days
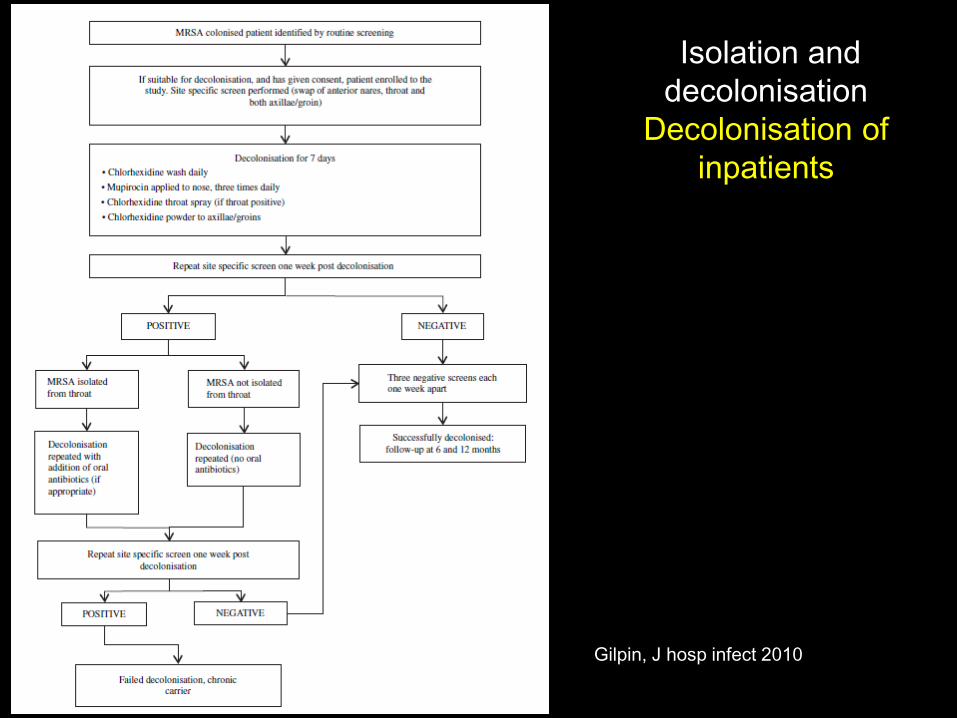
Gilpin, J hosp infect 2010
Isolation and
decolonisation
Decolonisation of
inpatients

Ammerlaan et al., JAC 2011

Ammerlaan et al., JAC in press

Decolonisation: who, where, how and when
Implementation of GL increases treatment success
60% of MRSA carriers were successfully decolonised
after the first eradication
Risk factors for decolonisation failure: CPD, throat-
perineum carriage, and carriage among household
contacts (uncomplicated); throat carriage and
dependence in activities of daily living (complicated)
Ammerlaan et al., JAC in press

First trial on mupirocin efficacy
Ammerlaan HS, JAC 2011
Current evidence, further supported by the first trial on mupirocin
efficacy, suggests that a decolonization protocol including local and
oral antibiotic therapy and decolonization of household contacts of
complicated MRSA carriers, combined with the introduction of
national guidelines endorsing decolonization, is highly efficacious in
populations with a low endemic level of MRSA.
However, the measures required to control MRSA in hospitals,
including decolonization protocols, where MRSA is highly endemic
may be different from those required in other institutions.
Tacconelli & Johnson JAC 2011

Isolation and decolonisation
Decolonisation of household
Bocher, CMI 2009

Manian, CID, 2003

Lee, CID 2011
Risk factors for MRSA persistent colonisation
Low level mupirocin resistance and genotypic chlorexidine resistance

Tackling resistance of HA-MRSA
Prevention of
intrahospital
spreading
Patient
Isolation
Cohort
Contact prec.
Hand hygiene
HCW
Education
Individual
protection
Environment
3 – Hospital

BMJ, 2004
No well designed studies exist that allow
the role of isolation measures alone to be
assessed.
None the less, there is evidence that
concerted efforts that include isolation can
reduce MRSA even in endemic settings.
Current isolation measures recommended
in national guidelines should continue to
be applied until further research
establishes otherwise.

Monthly Incidence of Colonization or Infection
with MRSA or VRE among Patients in ICUs
The mean ICU-level incidence of MRSA/VRE colonization/infection
per 1000 pts-days at risk, adjusted for baseline incidence, did not differ
significantly between the intervention and control ICUs (40.4±3.3 vs 35.6±3.7; P
= 0.35).

• Most of the evidence for HCW screening comes
from outbreak reports where the outbreak was
brought to an end following the introduction of
staff screening as part of a suite of infection
control measures
• Further research is required before a
recommendation could be made to introduce
routine MRSA screening of HCWs
Hawkins, J hosp infect 2011

Wilson, Crit Care Med 2011
Enhanced cleaning of the near-patient environment and hospital pathogens
from the bed area and staff hands

Datta, Arch Intern Med 2011
Enhanced cleaning
and risk of acquiring MRSA and VRE from prior room occupant

Tekerekoglu, AJIC 2011
Mobile phones
how many risks..

Bray, CMI 2011
Mobile phones how many risks..

Tackling resistance of MDR resistant bacteria
Prevention of
resistance
development
Antimicrobial
stewardship
1 - Pathogen

Tacconelli, Journal of Antimicrobial Chemotherapy (2008) 61, 26–38
Systematic review
Gram-positive bacteria: MRSA
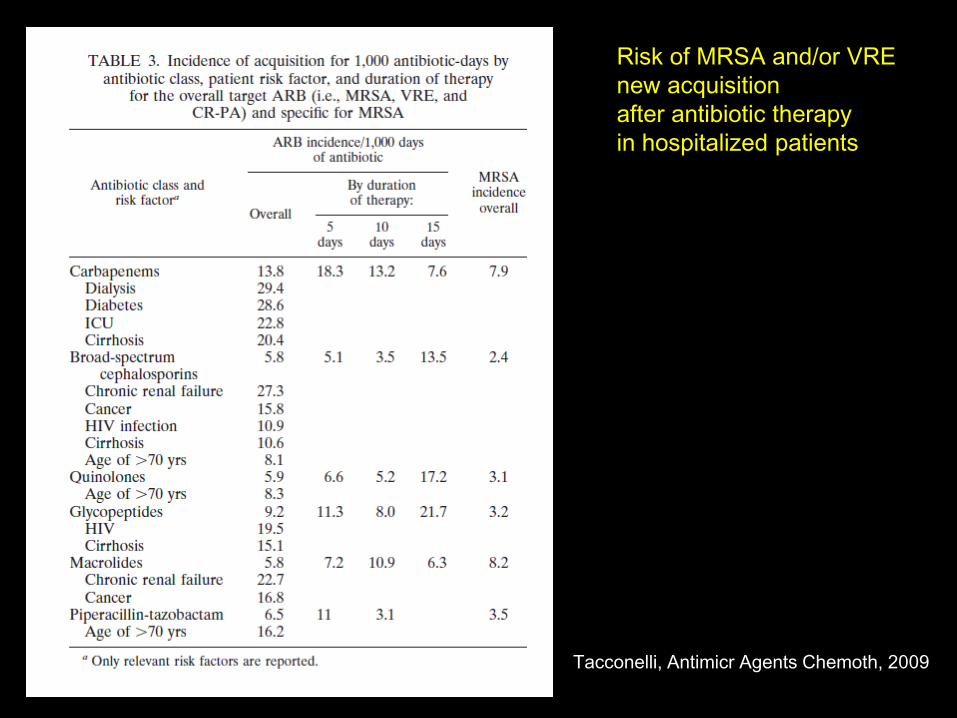
Tacconelli, Antimicr Agents Chemoth, 2009
Risk of MRSA and/or VRE
new acquisition
after antibiotic therapy
in hospitalized patients

MRSA+ pt before surgery

Isolation and decolonisation
High risk patients: surgery
Bode et al., NEJM 2010

MRSA bundle
Surgery patients
1. MRSA nasal screening
upon admission
2. Contact isolation
3. Handhygiene
4. Antimicrobial
stewardship
5. Outcome measures
Awad, ICHE, 2009

MRSA+ pt during hospitalisation
Rymzhanova, ICHE, 2009

“Real life”
1. MRSA+ pt at hospitalisation
Target screening of high risk patients
Universal sreening if MR > 35% on blood cultures
Contact precaution
Decoloniization if LOS > 7 days
In case of failure: pharingeal screening
2. MRSA+ pt before surgery
Decolonization for S aureus!
3. MRSA+ pt during hospitalisation
Periodic screening of high risk patients
4. MRSA+ pt at hospital discharge
Decolonization + household dec. – envirom. If needed

Health economic evaluation of prevention of MRSA infections or
-colonisations at hospitals: A systematic review (2004-2009)
829 economic publication reviewed 8 economic studies analysed
Limited quality
The break even point of cost-effective prevention and control measurements for MRSA cannot be finally clarified
There is a need for additional cost-benefit analyses
Korczak, GMS HTA 2010
Cost-effectiveness studies and MRSA
23 papers
costing studies to establish the
excess cost of MRSA infection or an
estimate of the national burden (n = 7)
economic evaluations comparing the
costs and benefits of an intervention
with the pre-existing service (n = 15)
All evaluated screening in hospital
with one exception (cleaning)
Gould, CMI 2010

Major pitfalls of cost analyses for reducing MRSA
No studies on IC measures
Majority of interventions were 7–8 years old
Different countries with different health care systems and cost structures USA (9)
UK (5)
Germany (3)
One southern European country (Spain)
Lack of generalizability
Single hospital study
Specific population
ICU
Emergency population
High risk patients
Surgery patients
Gould, CMI 2010

Olchanski, ICHE 2011
Cost effectiveness
universal vs targeted screening
PCR-based vs chromogenic media

Universal screening
Admission prevalence 7.5%
PCR screening (94.6% / 96.6%)
Strategy Active surveillance + decolonisation
Vs
Active surveillance
No screening
Outcomes HAI MRSA infections
Deaths avoided
Nelson, CMI 2010

Special setting
Cardiac surgery
Lee, Am J Manag Care 2010

Special setting
Orthopedic surgery
Lee, ICHE 2010
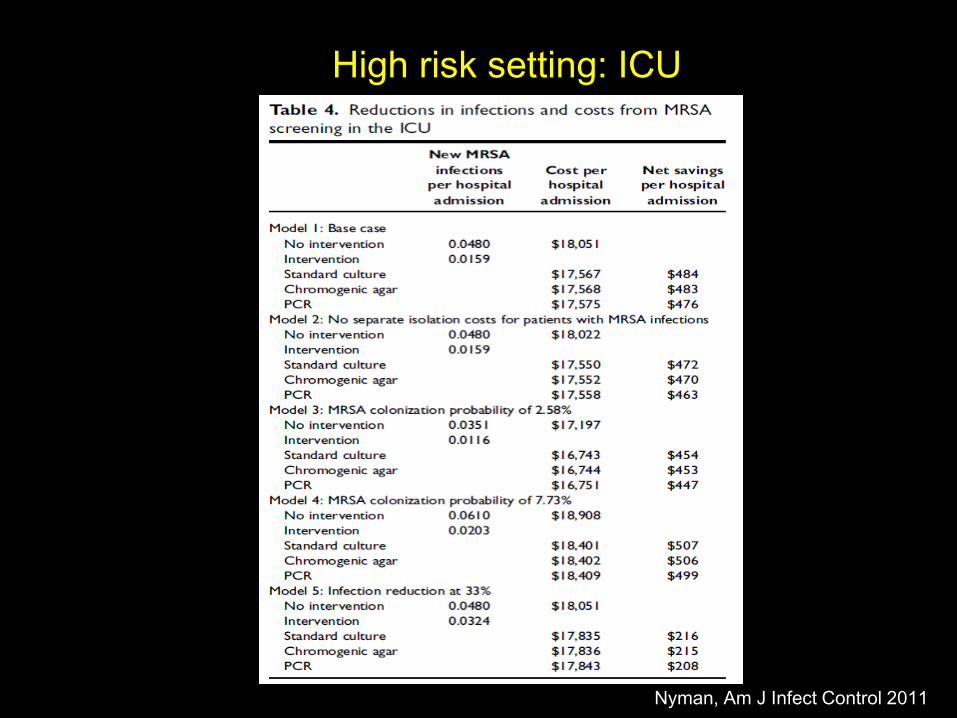
High risk setting: ICU
Nyman, Am J Infect Control 2011

Hospital admission Medium MRSA prevalence (5%):
Targeted screening with
chromogenic media is cost-
effective versus PCR-based
screening
High MRSA prevalence (15%):
PCR-based targeted screening
is cost-effective versus
chromogenic-media
Cardiac and orthopedic surgery / ICU:
Universal screening with PCR is
cost-effective versus chromogenic
media
Implications for
practice

Cost-effectiveness is only one of a number of criteria that should be employed in determining whether interventions are made available.
Issues of equity, needs, priorities and so on should also form part of the decision-making process.
Consider whether the cost-effective interventions would address major sources of the MRSA disease burden in your country and determine whether the cost-effective interventions would be feasible given existing institutions and experiences with implementation in their countries.
Implications for practice

Could the risk of MRSA hospital acquisition
have been reduced?
Preoperative screening: POSITIVE for S. aureus
Decolonisation NO early PJI NO long LOS NO UTI NO antibiotic therapy
Preoperative screening: NEGATIVE
No decolonisation early PJI long LOS HIGH RISK PATIENT !!!! Screening at hospital admission: positive for MRSA!!! No endocarditis……