detection and quantitation of chromosomal mosaicism in ... · pdf fileoriginal article...
TRANSCRIPT
ORIGINAL ARTICLE
Detection and quantitation of chromosomal mosaicism in humanblastocysts using copy number variation sequencingTida Ruttanajit1†, Sujin Chanchamroen1†, David S. Cram2,3†, Kritchakorn Sawakwongpra1, Wanwisa Suksalak1, Xue Leng3, Junmei Fan4,Li Wang4, Yuanqing Yao4* and Wiwat Quangkananurug1*
1Safe Fertility Center, Bangkok, Thailand2Department of Anatomy and Developmental Biology, Monash University, Melbourne, Australia3Berry Genomics, C., Limited, Beijing, China4Department of Obstetrics and Gynecology, PLA General Hospital, Beijing, China*Correspondence to: Yuanqing Yao. E-mail: [email protected]; Wiwat Quangkananurug. E-mail: [email protected]†Equal authorship contribution.
ABSTRACTObjective Currently, our understanding of the nature and reproductive potential of blastocysts associated withtrophectoderm (TE) lineage chromosomal mosaicism is limited. The objective of this study was to first validate copynumber variation sequencing (CNV-Seq) for measuring the level of mosaicism and second, examine the nature andlevel of mosaicism in TE biopsies of patient’s blastocysts.
Method TE biopy samples were analysed by array comparative genomic hybridization (CGH) and CNV-Seq todiscriminate between euploid, aneuploid and mosaic blastocysts.
Results Using artificial models of TE mosaicism for five different chromosomes, CNV-Seq accurately and reproduciblyquantitated mosaicism at levels of 50% and 20%. In a comparative 24-chromosome study of 49 blastocysts by arrayCGH and CNV-Seq, 43 blastocysts (87.8%) had a concordant diagnosis and 6 blastocysts (12.2%) were discordant.The discordance was attributed to low to medium levels of chromosomal mosaicism (30–70%) not detected by arrayCGH. In an expanded study of 399 blastocysts using CNV-Seq as the sole diagnostic method, the proportion ofdiploid-aneuploid mosaics (34, 8.5%) was significantly higher than aneuploid mosaics (18, 4.5%) (p< 0.02).
Conclusion Mosaicism is a significant chromosomal abnormality associated with the TE lineage of human blastocyststhat can be reliably and accurately detected by CNV-Seq. © 2015 John Wiley & Sons, Ltd.
Funding sources: The study was supported by grants awarded by the Key Program of the Twelfth Five-year plan of the People’s Liberation Army (BWS11J058) andthe National High Technology Research and Development Program (SS2015AA020402) to YY.Conflicts of interest: David Cram and Xue Leng are employees of Berry Genomics, Beijing.
INTRODUCTIONChromosomal aneuploidy is a major cause of implantationfailure in patients undergoing assisted reproductive treatment.1,2
Pioneer fluorescent in situ hybridization (FISH) studies of pre-implantation embryos first showed that in patient groups witha poor prognosis for pregnancy, the rate of aneuploidy oftenexceeded 50%.3–5 Based on these early observations,preimplantation genetic diagnosis (PGD) has since been offeredbymany in vitro fertilization (IVF) clinics to patients as a first linetreatment to identify euploid embryos in the cohort for transfer,in the hope of achieving an ongoing pregnancy that develops to ahealthy term baby with a normal karyotype.6 Currently, 24-chromsome array-based technologies such as array CGH (aCGH)and single nucleotide polymorphism arrays have supersededFISH as the main methodology for screening embryos forchromosomal abnormalities.7,8 More recently, several next-
generation sequencing (NGS) protocols have been developedand validated for PGD of aneuploidy at the cleavage7–12 and theblastocyst stage13–15 of preimplantation development and holdpromise for clinical application.
The human preimplantation embryo, unlike othermammalianembryos, is highly susceptible to the development ofchromosomal errors.16,17 Themajor error that arises is aneuploidycaused by gametal meiotic I and II errors, particularly in theoocyte.16,18,19 During the early cleavage-stage, the embryo isfurther prone to develop mosaicism via mitotic errors in one ormore cells, creating diploid-aneuploid mosaics.20 While someaneuploid and diploid-aneuploid mosaic embryos succumbbecause of growth arrest, a significant proportion still developto the blastocyst stage with the potential to implant.20–22 Thevarious types of chromosomal abnormalities exhibited bysome human embryos at different stages of preimplantation
Prenatal Diagnosis 2016, 36, 154–162 © 2015 John Wiley & Sons, Ltd.
DOI: 10.1002/pd.4759

development have created a conundrum for PGD, and there hasbeen much debate concerning the disadvantages and advantagesof polar body, blastomere and trophectoderm (TE) biopsy.23
However, for a variety of reasons, including improved culturemedia for blastocyst development, access to more cells to makea reliable and accurate diagnosis, and efficient cryopreservationprotocols for biopsied blastocysts, there has been a major shifttowards blastocyst biopsy in many IVF and PGD centres.24
For comprehensive PGD of aneuploidy in blastocysts, it istherefore imperative that any diagnostic technology used notonly has the ability to reliably and accurately detect whole andpartial aneuploidies but also mosaicism. FISH can detect lowlevels ofmosaicism in the single cells of a fixed TE biopsy samplebut is restricted to the analysis of a small sub-set ofchromosomes.25 In two studies, aCGH has also been shown tobe capable of detecting mosaicism using the whole genomeamplification (WGA) product of a multiple TE cell biopsysample.26,27 However, identification and quantitation ofmosaicism by aCGH can be technically problematic particularlywhen the chromosome gain or loss is less than than 50%.28 Ourrecent studies have shown that an NGS-based method termedcopy number (CN) variation sequencing could detect mosaicismas low as 5% at the genomic DNA level29 and correctly quantitatetrisomy and monosomy in single blastomeres.10,30 We thereforespeculated that CNV-Seq could also identify the nature and levelof mosaicism in a blastocyst TE biopsy sample.
METHODS
Study oversightThe specific aims of the study were threefold. The first was tovalidate CNV-Seq for detectingmosaicism, the second to comparethe gold standard aCGH method with CNV-Seq for diagnosis ofeuploidy, aneuploidy and mosaicism and the third to determinethe incidence and type of mosaicism in human blastocysts. Thefirst and third parts of the study were performed at the IVF clinicof the Department of Obstetrics and Gynaecology, PLA BeijingHospital, and approved by the Human Ethics Committee of theChinese PLAGeneral Hospital (S2013-092-02). All Chinese patientsprovided written informed consent for IVF, PGD and provision ofresearch material. The second part of the study was performed atthe Safe Fertility and Genetics Center, Bangkok. All Thai patientsprovided written informed consent for IVF and PGD.
IVF and embryo cultureOocytes were collected at 35 h post-human chorionicgonadotrophin (hCG) administration and denuded from thecumulus oophorus by brief exposure to hyaluronidase. Post-hCG administration (36–38 h), MII oocytes were fertilized byintracytoplasmic sperm injection. Oocytes displaying twopronuclei were cultured further in an atmosphere of 5%oxygen, 5% carbon dioxide and 90% nitrogen at 37 °C andmaximum humidity using Cook MINC incubators. All one-cellembryos were cultured to the blastocyst stage in 10 μL drops ofsequential media covered with oil (Cook cleavage medium:Cat. no. K17065 and blastocyst medium: Cat. no. G20929).
Blastocyst biopsy, cryopreservation and transferOn day 3 when embryos were at the 6–8 cell stage, a laser(Lykos Hamilton Thorne; USA) was used to create a 6–9 μMdiameter opening in the zona pellucida. This breach enabledsubsequent biopsy of TE cells on either day 5 or 6 ofdevelopment from expanding and expanded blastocysts withor without herniating cells. TE cells (5–10 cells) were aspiratedwith a TE biopsy pipette followed by laser-assisted removal ofthe target cells from the body of the embryo. Harvested TE cellswere washed in PBS and placed in 2.5 μL of PBS in a 200 μL PCRtube. Biopsied blastocysts were vitrified using the Cryotopdevice and commercially available vitrification solutions(Kitazato BioPharma Co., Shizuoka, Japan). Transfer ofvitrified-warmed blastocysts to the uterus was performed underultrasound guidance, and luteal-phase support was achievedwith intramuscular injections of 80mg of progesterone, whichwas continued daily for at least two weeks after embryo transfer.Serum hCG concentrations were measured 17days after oocyteretrieval, and fetal heartbeats monitored by ultrasound at5weeks after embryo transfer.
Whole genome amplificationTE biopsy samples collected in 2.5 μL of sterile PBS were lysedand subjected to WGA using the single cell SurePlexamplification kit (SurePlex, Rubicon). Gel electrophoresis wasused to assess the yield and quality of the WGA products.
Array comparative genomic hybridizationThe aCGH procedure was performed using 24 SureV3 arrays(Illumina, USA) in accordance with manufacturer’s guidelines.Briefly, equal amounts of test and control DNA were labelledwith Cy3-dCTP and Cy5-dCTP (Illumina, USA) for 4–18 h.Labelled DNA was precipitated, resuspended in dexsulphatehybridization buffer and then hybridized to arrays overnightunder cover slips. Slides were washed in a solution of 2×saline sodium citrate (SSC) and 0.05% Tween-20 at roomtemperature, and then for a further 10minutes in 1× SSC. Ahigh stringency wash was then performed in 0.1× SSC for5min at 60 °C. Slides were finally washed at room temperaturein 0.1× SSC for 1min and then dried by centrifugation for3min. Laser scanning at 10 μm (InnoScan 710 AL MicroarrayScanner, Innopsys, USA) was used to detect bound fluorescence.Microarray data was collated and analysed with BlueFusesoftware (Illumina, USA) to measure relative loss or gain acrossall 24 chromosomes. Two technicians independently assessedthe aCGH profiles to make the final chromosome diagnosis ofeach blastocyst.
Copy number variation sequencingPreparation of sequencing libraries from 50 ng of WGA productwas performed as previously described.31,32 Low coveragemassive parallel sequencing was conducted on the IlluminaHiSeq2500 platform. Approximately 5 million 45 bp sequencingreads (9 bp barcode and 36 bp genome sequence) weregenerated per sample, and approximately 3 million reads(60%) were mapped to the 24 chromosomes (22 autosomesand 2 sex chromosomes) using the Burrows Wheeler alignmentalgorithm.33 Uniquely mapped sequencing reads from each
Blastocyst mosaicism 155
Prenatal Diagnosis 2016, 36, 154–162 © 2015 John Wiley & Sons, Ltd.

test sample (minimum batches of 15 samples) were allocatedto 20 kb sequencing bins along the length of each chromosomeand then mean reads per bin internally compared with eachother to identify and quantitate CNV in individual samples.29
The sequencing data for all 24 chromosomes were plotted asthe log2 value of the mean sequencing read number per 20 kbbin (y-axis) versus sequential 20 kb sequencing bins (x-axis),using theoretical reference points of log2[0] for two copies(normal), log2[1.5] for three copies (duplication) and log2[0.5]for one copy (deletion). A continuous blue line was applied totrack the mean CNV from p to the q arm of each chromosome,allowing measurement of CN, as previously described.29 Forcalling euploidy, aneuploidy or mosaicism, CN thresholds wereset as 2.9–3.1 for trisomy, 1.9–2.1 for disomy and 0.9–1.1 formonosomy.
RESULTS
Validation of CNV-Seq for measuring chromosome mosaicism inTE biopsy modelsIn preliminary experiments, we assessed the sensitivity andreproducibility of CNV-Seq to detect chromosomal mosaicismin artificially created samples. Sample models with 50% and20% mosaicism for representative chromosomes 12, 16, 18, 21and X were generated to mimic medium and low levelsmosaicism respectively, in a blastocyst biopsy of 10 TE cells.Two types of models were created comprising either a mixtureof diploid and aneuploid cells confirmed by karyotyping or amixture of WGA products from known diploid and aneuploidblastocysts previously diagnosed with the correct CNs for all24 chromosomes by quantitative CNV-Seq10 and with noevidence of any level of background chromosome mosaicism.
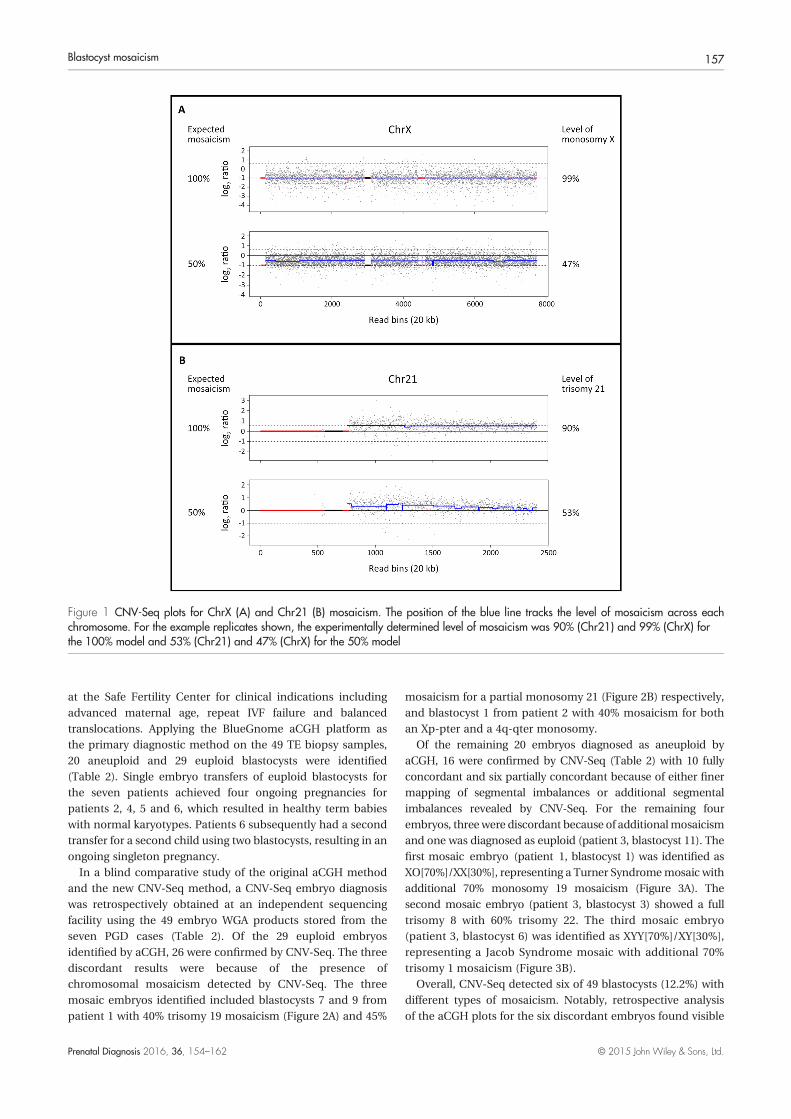
In the first experiment, a cell model with 50% mosaicism fortrisomy 21 and monosomy X was first prepared by mixing five47, XY,+21 lymphocytes with five 46,XX lymphocytes, using 1047,XY,+21 lymphocytes as a control (100% trisomy). Threereplicates of test and two replicates of control samples were
then subjected to WGA and CNV-Seq. For both chromosome21 (Chr21) and chromosome X (ChrX), the experimentallydetermined levels of mosaicism were very similar to theexpected levels of 100% and 50% (Table 1; Figure 1).Importantly, for the 100% and 50% mosaicism models oftrisomy 21, the determined CNs were consistently 2.9 and 2.5respectively, across the entire 21q region (Figure 1A). Likewise,for the 100% and 50% models of monosomy X, the determinedCNs were 1.0 and 1.5 respectively, across the entire Xp and Xqregions (Figure 1B). In addition, for all model replicates, theother remaining autosomes and chromosome Y (ChrY) showedthe expected CNs of two and one (no mosaicism) respectively.This initial experiment suggested that CNV-Seq was sensitiveand specific for detecting Chr21 and ChrX mosaicism at a levelof 50%.
To further validate CNV-Seq for detecting mosaicismassociated with other chromosomes and at lower levels, in asecond experiment, we tested additional models using twoblastocyst biopsyWGAsamples;onewithtrisomy16(47,XX,+16)and one withmonosomies 12 and 18 (44,XY,�12,�18) that wereoriginally identified by aCGH and then verified for CN by CNV-Seq. Triplicate models of 100%, 50% and 20% mosaicism wereprepared from each abnormal WGA sample by dilution with anormalWGAsamplefromaknown46,XXblastocystandanalysedby CNV-Seq (Table 1). Based on the starting level of each fullaneuploidy (slightly less than 100% for trisomy 16 andmonosomies 12, 18 and X), themeasured levels ofmosaicism for50% and 20% replicate samples closely paralleled the expectedvalues. These findings indicated that CNV-Seq is also sensitiveand specific for measuring levels of chromosomal mosaicism of50%and20%.
Comparison of aCGH and CNV-Seq for detecting mosaicism inPGD blastocystsThe ability of CNV-Seq to detect mosaicism in actual TE biopsysamples was tested retrospectively in a group of 49 PGDblastocysts from seven patients who had received treatment
Table 1 CNV-Seq analysis of mosaicism in artificial blastocyst biopsy models
Actual levels of mosaicism by CNV-Seq (%)
Mosaicism model Replicate 1, Replicate 2, Replicate 3 (Replicate Mean)
47, XY,+21 46,XX Mosaicism Trisomy 21 Monosomy X
10 cells + 0 cells = 100% 90%, 87%, 93% (90%) 98%, 99%, 100 (99%)
5 cells + 5 cells = 50% 54%, 54%, 50% (53%) 48%, 53%, 39% (47%)
47,XX,+16 + 46,XX Trisomy 16
50 ng WGA + 0 ng WGA = 100% 87%, 88% (88%)
25 ng WGA + 25 ng WGA = 50% 44%, 45%, 43% (44%)
10 ng WGA + 40 ng WGA = 20% 17%, 16%, 17% (17%)
44,XY,�12,�18 + 46,XX Monosomy 12 Monosomy 18 Monosomy X
50 ng WGA + 0 ng WGA = 100% 95%, 96% (96%) 97%, 97% (97%) 98%, 98% (98%)
25 ng WGA + 25 ng WGA = 50% 46%, 46%, 47% (46%) 44%, 46%, 47% (46%) 46%, 47%, 47% (47%)
10 ng WGA + 40 ng WGA = 20% 16%, 17%, 17% (17%) 18%, 18%, 18% (18%) 16%, 17%, 17% (17%)
T. Ruttanajit et al.156
Prenatal Diagnosis 2016, 36, 154–162 © 2015 John Wiley & Sons, Ltd.
at the Safe Fertility Center for clinical indications includingadvanced maternal age, repeat IVF failure and balancedtranslocations. Applying the BlueGnome aCGH platform asthe primary diagnostic method on the 49 TE biopsy samples,20 aneuploid and 29 euploid blastocysts were identified(Table 2). Single embryo transfers of euploid blastocysts forthe seven patients achieved four ongoing pregnancies forpatients 2, 4, 5 and 6, which resulted in healthy term babieswith normal karyotypes. Patients 6 subsequently had a secondtransfer for a second child using two blastocysts, resulting in anongoing singleton pregnancy.
In a blind comparative study of the original aCGH methodand the new CNV-Seq method, a CNV-Seq embryo diagnosiswas retrospectively obtained at an independent sequencingfacility using the 49 embryo WGA products stored from theseven PGD cases (Table 2). Of the 29 euploid embryosidentified by aCGH, 26 were confirmed by CNV-Seq. The threediscordant results were because of the presence ofchromosomal mosaicism detected by CNV-Seq. The threemosaic embryos identified included blastocysts 7 and 9 frompatient 1 with 40% trisomy 19 mosaicism (Figure 2A) and 45%
mosaicism for a partial monosomy 21 (Figure 2B) respectively,and blastocyst 1 from patient 2 with 40% mosaicism for bothan Xp-pter and a 4q-qter monosomy.
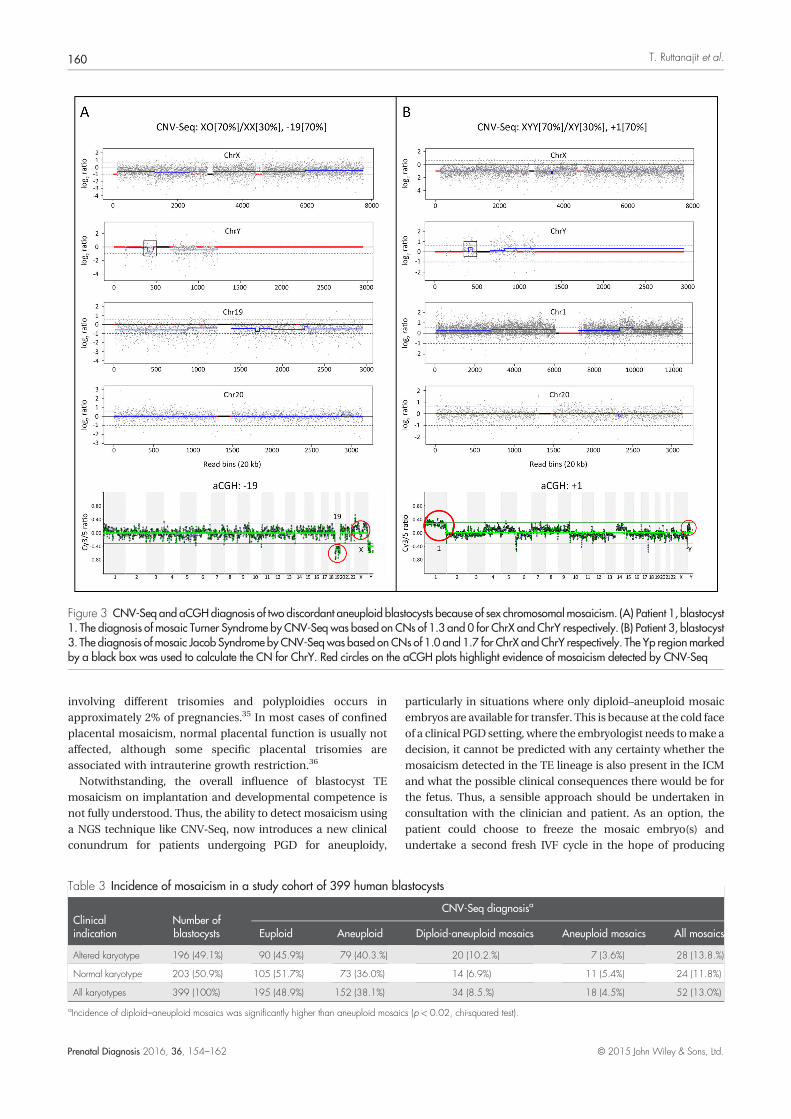
Of the remaining 20 embryos diagnosed as aneuploid byaCGH, 16 were confirmed by CNV-Seq (Table 2) with 10 fullyconcordant and six partially concordant because of either finermapping of segmental imbalances or additional segmentalimbalances revealed by CNV-Seq. For the remaining fourembryos, threewere discordant because of additionalmosaicismand one was diagnosed as euploid (patient 3, blastocyst 11). Thefirst mosaic embryo (patient 1, blastocyst 1) was identified asXO[70%]/XX[30%], representing a Turner Syndromemosaic withadditional 70% monosomy 19 mosaicism (Figure 3A). Thesecond mosaic embryo (patient 3, blastocyst 3) showed a fulltrisomy 8 with 60% trisomy 22. The third mosaic embryo(patient 3, blastocyst 6) was identified as XYY[70%]/XY[30%],representing a Jacob Syndrome mosaic with additional 70%trisomy 1 mosaicism (Figure 3B).
Overall, CNV-Seq detected six of 49 blastocysts (12.2%) withdifferent types of mosaicism. Notably, retrospective analysisof the aCGH plots for the six discordant embryos found visible
Figure 1 CNV-Seq plots for ChrX (A) and Chr21 (B) mosaicism. The position of the blue line tracks the level of mosaicism across eachchromosome. For the example replicates shown, the experimentally determined level of mosaicism was 90% (Chr21) and 99% (ChrX) forthe 100% model and 53% (Chr21) and 47% (ChrX) for the 50% model
Blastocyst mosaicism 157
Prenatal Diagnosis 2016, 36, 154–162 © 2015 John Wiley & Sons, Ltd.
evidence of mosaicism detected by CNV-Seq (Figures 2 and 3).However, because of some background hybridization noiseassociated with the acGH plots, mosaicism of the involvedchromosomes could not be confidently called in all six cases.Nonetheless, on this basis, the aCGH data did provideconfirmatory evidence that the CNV-Seq diagnoses ofmosaicismwere indeed true.
Incidence of chromosomal mosaicism in a larger cohort of PGDblastocystsThe incidence and nature of chromosomal mosaicism wasfurther evaluated in an additional 399 blastocysts from patientsundergoing either PGD for aneuploidy (normal karyotype) or
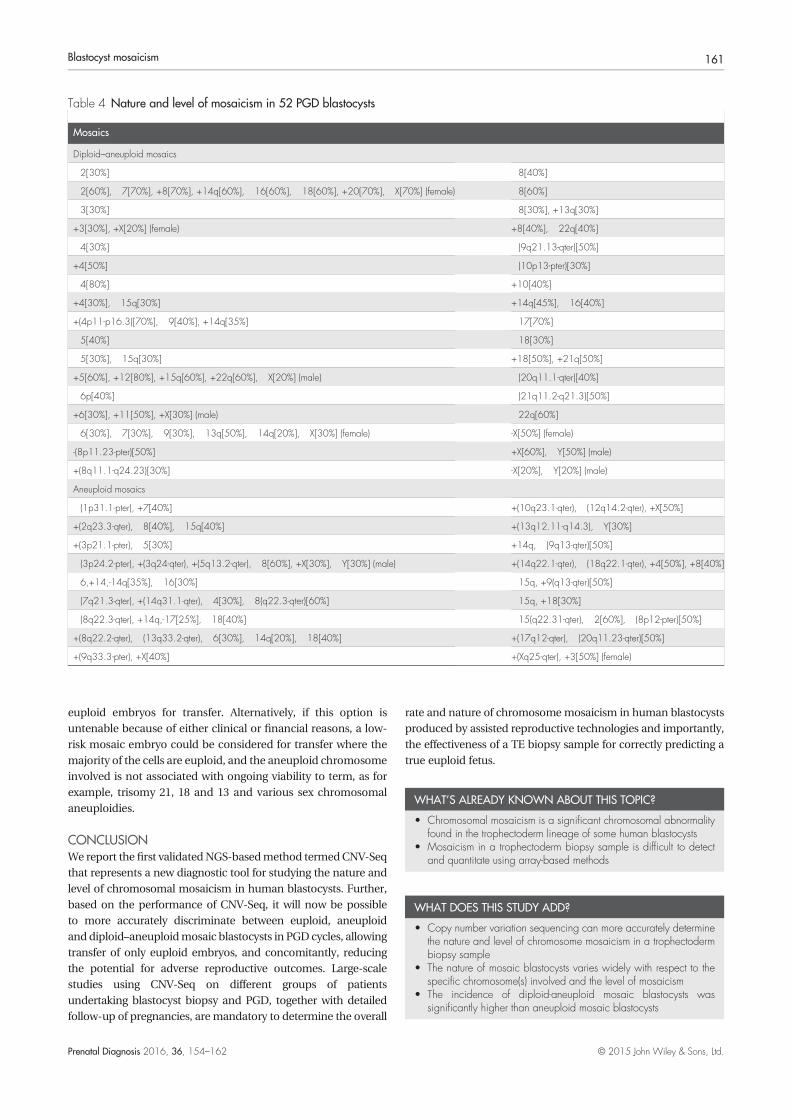
PGD for a balanced translocation (altered karyotype) usingour validated CNV-Seq protocol as the sole diagnostic method.The overall incidence of euploidy, aneuploidy and mosaicismis summarized in Table 3. Overall, a total of 52 blastocysts(13.0%) were identified as either diploid-aneuploid mosaicsor aneuploid mosaics. The incidence of diploid–aneuploidmosaics (34, 8.5%) was significantly higher than aneuploidmosaics (18, 4.5%) (p< 0.02). There was no significantdifference in mosaicism rates between embryos produced bypatients with an altered or normal karyotype (p< 0.05). All 52blastocysts exhibited a unique pattern of chromosomalmosaicism (Table 4). Both simple and complex types ofchromosomal mosaicism were observed, involving either
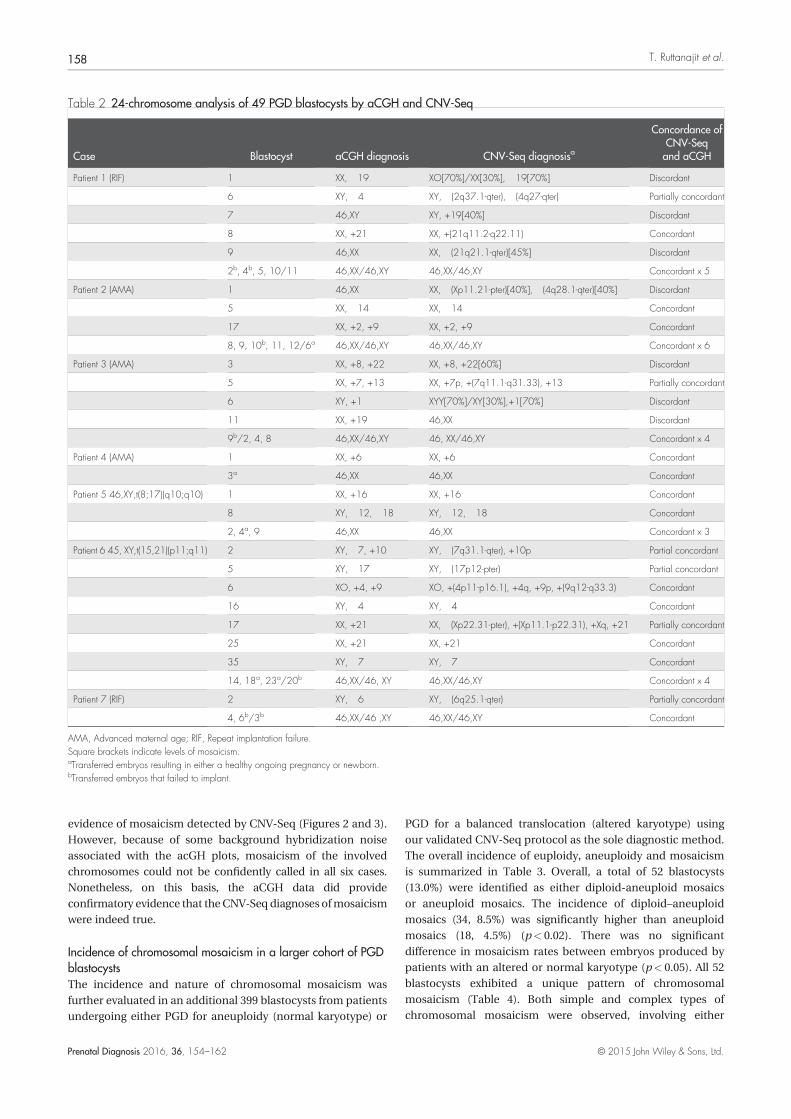
Table 2 24-chromosome analysis of 49 PGD blastocysts by aCGH and CNV-Seq
Case Blastocyst aCGH diagnosis CNV-Seq diagnosisa
Concordance ofCNV-Seqand aCGH
Patient 1 (RIF) 1 XX, �19 XO[70%]/XX[30%], �19[70%] Discordant
6 XY, �4 XY, �(2q37.1-qter), �(4q27-qter) Partially concordant
7 46,XY XY, +19[40%] Discordant
8 XX, +21 XX, +(21q11.2-q22.11) Concordant
9 46,XX XX, �(21q21.1-qter)[45%] Discordant
2b, 4b, 5, 10/11 46,XX/46,XY 46,XX/46,XY Concordant x 5
Patient 2 (AMA) 1 46,XX XX, �(Xp11.21-pter)[40%], �(4q28.1-qter)[40%] Discordant
5 XX, �14 XX, �14 Concordant
17 XX, +2, +9 XX, +2, +9 Concordant
8, 9, 10b, 11, 12/6a 46,XX/46,XY 46,XX/46,XY Concordant x 6
Patient 3 (AMA) 3 XX, +8, +22 XX, +8, +22[60%] Discordant
5 XX, +7, +13 XX, +7p, +(7q11.1-q31.33), +13 Partially concordant
6 XY, +1 XYY[70%]/XY[30%],+1[70%] Discordant
11 XX, +19 46,XX Discordant
9b/2, 4, 8 46,XX/46,XY 46, XX/46,XY Concordant x 4
Patient 4 (AMA) 1 XX, +6 XX, +6 Concordant
3a 46,XX 46,XX Concordant
Patient 5 46,XY,t(8;17)(q10;q10) 1 XX, +16 XX, +16 Concordant
8 XY, �12, �18 XY, �12, �18 Concordant
2, 4a, 9 46,XX 46,XX Concordant x 3
Patient 6 45, XY,t(15,21)(p11;q11) 2 XY, �7, +10 XY, �(7q31.1-qter), +10p Partial concordant
5 XY, �17 XY, �(17p12-pter) Partial concordant
6 XO, +4, +9 XO, +(4p11-p16.1), +4q, +9p, +(9q12-q33.3) Concordant
16 XY, �4 XY, �4 Concordant
17 XX, +21 XX, �(Xp22.31-pter), +(Xp11.1-p22.31), +Xq, +21 Partially concordant
25 XX, +21 XX, +21 Concordant
35 XY, �7 XY, �7 Concordant
14, 18a, 23a/20b 46,XX/46, XY 46,XX/46,XY Concordant x 4
Patient 7 (RIF) 2 XY, �6 XY, �(6q25.1-qter) Partially concordant
4, 6b/3b 46,XX/46 ,XY 46,XX/46,XY Concordant
AMA, Advanced maternal age; RIF, Repeat implantation failure.Square brackets indicate levels of mosaicism.aTransferred embryos resulting in either a healthy ongoing pregnancy or newborn.bTransferred embryos that failed to implant.
T. Ruttanajit et al.158
Prenatal Diagnosis 2016, 36, 154–162 © 2015 John Wiley & Sons, Ltd.

whole autosomes, partial autosomes (loss of sequences in p orq arms) or the sex chromosomes. In addition, different levels ofmosaicism were observed ranging from as low as 20% to ashigh as 70% in some TE biopsy samples.
DISCUSSIONIn human embryos produced by assisted reproductivetechnologies, aneuploidy and mosaicism arising in the earlyembryo commonly persists to the blastocyst stage ofdevelopment.20 With the increasing use of TE biopsy for PGD[24], the main aim of the study was to evaluate the ability ofthe NGS protocol CNV-Seq [29] to reliably and accuratelydetect chromosomal TE mosaicism. In validation studieswhereby samples mimicking a 10-cell TE biopsy were analysedby CNV-Seq, the actual levels of mosaicism determined for fiverepresentative chromosomes were virtually identical to theexpected values. Further, we demonstrated that 50% and 20%mosaicism, representing five and two aneuploid cells in a10-cell TE biopsy respectively, could be accurately andreproducibly measured. Moreover, in a clinical follow upstudy comparing the diagnostic performance of aCGH versusCNV-Seq for 49 PGD blastocysts, we showed that our CNV-Seqhad the capability of detecting and quantitating chromosomalmosaicism in six blastocysts (12.2%) that could not beconfidently called by aCGH. Collectively, these validation studiesconfirm that CNV-seq is a quantitative NGS protocol10 with highsensitivity and reproducibility for also detecting chromosomemosaicism in a TE biopsy sample.
In a second study of 399 PGD blastocysts, CNV-Seq detected52mosaics (13%). The nature of the TEmosaicism varied widely,
involving either whole chromosomes, partial chromosomesand/or sex chromosomes at significant levels ranging from 20to 70%. The two types of mosaic blastocysts identified werediploid-aneuploid mosaics (8.5%) comprising a mixture ofeuploid cells and aneuploid cells and, aneuploidy mosaics(4.5%) consisting of a mixture of cells with a specific aneuploidyand cells with the same aneuploidy plus an additionalaneuploidy. However, it is important to note that because asecondary confirmation of mosaicism using a differenttechnique was not performed in this study, the overall rate of13% mosaicism can only be considered an estimate. As acomparison, in two other published studies of TE mosaicism inPGD blastocysts using array-based methods, the incidence ofmosaicism reported was 33%26 and 16%.37 We speculate thatthe different levels of mosaicism detected in these previousstudies may be because of a number of factors, includingdifferences in patient cohorts, blastocyst quality and thesensitivity of diagnostic techniques used.
A TE biopsy is considered to be the earliest form of chorionicvillous sampling. In blastocyst development, the TE lineageforms the cytotrophoblast and, together with extraembryonicmesoderm, forms the chorion and placenta.20 In contrast, theinner cell mass (ICM), which is not biopsied, forms the epiblastand then the fetus. Several studies analysing the TE and ICMlinage cells from the same blastocyst using either acombination of FISH and aCGH25 or aCGH34 alone have shownthat in the vast majority of blastocysts the chromosomeconstitution is identical or very similar, with most variationassociated with mosaicism.25 However, from prenatalchorionic villous biopsies, confined placental mosaicism
Figure 2 CNV-Seq and aCGH diagnosis of two discordant euploid blastocysts because of mosaicism. (A) Patient 1, blastocyst 7 and (B)Patient 1, blastocyst 9. Red circles on the aCGH plots highlight evidence of mosaicism detected by CNV-Seq
Blastocyst mosaicism 159
Prenatal Diagnosis 2016, 36, 154–162 © 2015 John Wiley & Sons, Ltd.
involving different trisomies and polyploidies occurs inapproximately 2% of pregnancies.35 In most cases of confinedplacental mosaicism, normal placental function is usually notaffected, although some specific placental trisomies areassociated with intrauterine growth restriction.36
Notwithstanding, the overall influence of blastocyst TEmosaicism on implantation and developmental competence isnot fully understood. Thus, the ability to detect mosaicism usinga NGS technique like CNV-Seq, now introduces a new clinicalconundrum for patients undergoing PGD for aneuploidy,
particularly in situations where only diploid–aneuploid mosaicembryos are available for transfer. This is because at the cold faceof a clinical PGD setting, where the embryologist needs tomake adecision, it cannot be predicted with any certainty whether themosaicism detected in the TE lineage is also present in the ICMand what the possible clinical consequences there would be forthe fetus. Thus, a sensible approach should be undertaken inconsultation with the clinician and patient. As an option, thepatient could choose to freeze the mosaic embryo(s) andundertake a second fresh IVF cycle in the hope of producing
Table 3 Incidence of mosaicism in a study cohort of 399 human blastocysts
Clinicalindication
Number ofblastocysts
CNV-Seq diagnosisa
Euploid Aneuploid Diploid-aneuploid mosaics Aneuploid mosaics All mosaics
Altered karyotype 196 (49.1%) 90 (45.9%) 79 (40.3.%) 20 (10.2.%) 7 (3.6%) 28 (13.8.%)
Normal karyotype 203 (50.9%) 105 (51.7%) 73 (36.0%) 14 (6.9%) 11 (5.4%) 24 (11.8%)
All karyotypes 399 (100%) 195 (48.9%) 152 (38.1%) 34 (8.5.%) 18 (4.5%) 52 (13.0%)
aIncidence of diploid–aneuploid mosaics was significantly higher than aneuploid mosaics (p< 0.02, chi-squared test).
Figure 3 CNV-Seq and aCGHdiagnosis of two discordant aneuploid blastocysts because of sex chromosomal mosaicism. (A) Patient 1, blastocyst1. The diagnosis of mosaic Turner Syndrome by CNV-Seq was based on CNs of 1.3 and 0 for ChrX and ChrY respectively. (B) Patient 3, blastocyst3. The diagnosis of mosaic Jacob Syndrome by CNV-Seq was based on CNs of 1.0 and 1.7 for ChrX and ChrY respectively. The Yp regionmarkedby a black box was used to calculate the CN for ChrY. Red circles on the aCGH plots highlight evidence of mosaicism detected by CNV-Seq
T. Ruttanajit et al.160
Prenatal Diagnosis 2016, 36, 154–162 © 2015 John Wiley & Sons, Ltd.
euploid embryos for transfer. Alternatively, if this option isuntenable because of either clinical or financial reasons, a low-risk mosaic embryo could be considered for transfer where themajority of the cells are euploid, and the aneuploid chromosomeinvolved is not associated with ongoing viability to term, as forexample, trisomy 21, 18 and 13 and various sex chromosomalaneuploidies.
CONCLUSIONWe report the first validatedNGS-basedmethod termedCNV-Seqthat represents a new diagnostic tool for studying the nature andlevel of chromosomal mosaicism in human blastocysts. Further,based on the performance of CNV-Seq, it will now be possibleto more accurately discriminate between euploid, aneuploidand diploid–aneuploidmosaic blastocysts in PGDcycles, allowingtransfer of only euploid embryos, and concomitantly, reducingthe potential for adverse reproductive outcomes. Large-scalestudies using CNV-Seq on different groups of patientsundertaking blastocyst biopsy and PGD, together with detailedfollow-up of pregnancies, aremandatory to determine the overall
rate and nature of chromosomemosaicism in human blastocystsproduced by assisted reproductive technologies and importantly,the effectiveness of a TE biopsy sample for correctly predicting atrue euploid fetus.
WHAT’S ALREADY KNOWN ABOUT THIS TOPIC?
• Chromosomal mosaicism is a significant chromosomal abnormalityfound in the trophectoderm lineage of some human blastocysts
• Mosaicism in a trophectoderm biopsy sample is difficult to detectand quantitate using array-based methods
WHAT DOES THIS STUDY ADD?
• Copy number variation sequencing can more accurately determinethe nature and level of chromosome mosaicism in a trophectodermbiopsy sample
• The nature of mosaic blastocysts varies widely with respect to thespecific chromosome(s) involved and the level of mosaicism
• The incidence of diploid-aneuploid mosaic blastocysts wassignificantly higher than aneuploid mosaic blastocysts
Table 4 Nature and level of mosaicism in 52 PGD blastocysts
Mosaics
Diploid–aneuploid mosaics
�2[30%] �8[40%]
�2[60%], �7[70%], +8[70%], +14q[60%], �16[60%], �18[60%], +20[70%], �X[70%] (female) �8[60%]
�3[30%] �8[30%], +13q[30%]
+3[30%], +X[20%] (female) +8[40%], �22q[40%]
�4[30%] �(9q21.13-qter)[50%]
+4[50%] �(10p13-pter)[30%]
�4[80%] +10[40%]
+4[30%], �15q[30%] +14q[45%], �16[40%]
+(4p11-p16.3)[70%], �9[40%], +14q[35%] �17[70%]
�5[40%] �18[30%]
�5[30%], �15q[30%] +18[50%], +21q[50%]
+5[60%], +12[80%], +15q[60%], +22q[60%], �X[20%] (male) �(20q11.1-qter)[40%]
�6p[40%] �(21q11.2-q21.3)[50%]
+6[30%], +11[50%], +X[30%] (male) �22q[60%]
�6[30%], �7[30%], �9[30%], �13q[50%], �14q[20%], �X[30%] (female) -X[50%] (female)
-(8p11.23-pter)[50%] +X[60%], �Y[50%] (male)
+(8q11.1-q24.23)[30%] -X[20%], �Y[20%] (male)
Aneuploid mosaics
�(1p31.1-pter), +7[40%] +(10q23.1-qter), �(12q14.2-qter), +X[50%]
+(2q23.3-qter), �8[40%], �15q[40%] +(13q12.11-q14.3), �Y[30%]
+(3p21.1-pter), �5[30%] +14q, �(9q13-qter)[50%]
�(3p24.2-pter), +(3q24-qter), +(5q13.2-qter), �8[60%], +X[30%], �Y[30%] (male) +(14q22.1-qter), �(18q22.1-qter), +4[50%], +8[40%]
�6,+14,-14q[35%], �16[30%] �15q, +9(q13-qter)[50%]
�(7q21.3-qter), +(14q31.1-qter), �4[30%], �8(q22.3-qter)[60%] �15q, +18[30%]
�(8q22.3-qter), +14q,-17[25%], �18[40%] �15(q22.31-qter), �2[60%], �(8p12-pter)[50%]
+(8q22.2-qter), �(13q33.2-qter), �6[30%], �14q[20%], �18[40%] +(17q12-qter), �(20q11.23-qter)[50%]
+(9q33.3-pter), +X[40%] +(Xq25-qter), +3[50%] (female)
Blastocyst mosaicism 161
Prenatal Diagnosis 2016, 36, 154–162 © 2015 John Wiley & Sons, Ltd.
REFERENCES1. Munné S. Preimplantation genetic diagnosis and human implantation--
a review. Placenta 2003;24(Suppl B):S70–6.2. Farfalli VI, Magli MC, Ferraretti AP, et al. Role of aneuploidy on embryo
implantation. Gynecol Obstet Invest 2007;64(3):161–5.3. Munné S, Lee A, Rosenwaks Z, et al. Diagnosis of major chromosome
aneuploidies in human preimplantation embryos. Hum Reprod1993;8(12):2185–91.
4. Gianaroli L, Magli MC, Ferraretti AP, et al. Preimplantation geneticdiagnosis increases the implantation rate in human in vitro fertilizationby avoiding the transfer of chromosomally abnormal embryos. FertilSteril 1997;68(6):1128–31.
5. Wilton L. Preimplantation genetic diagnosis for aneuploidyscreening in early human embryos: a review. Prenat Diagn2002;22(6):512–8.
6. Coco R. Reprogenetics: Preimplantational genetics diagnosis. GenetMol Biol 2014;37(Suppl 1):271–84.
7. Munné S. Preimplantation genetic diagnosis for aneuploidy andtranslocations using array comparative genomic hybridization. CurrGenomics 2012;13(6):463–70.
8. Handyside AH. 24-chromosome copy number analysis: a comparison ofavailable technologies. Fertil Steril 2013;100(3):595–602.
9. Wang L, Wang X, Zhang J, et al. Detection of chromosomal aneuploidyin human preimplantation embryos by next-generation sequencing.Biol Reprod 2014;90(5):95.
10. Wang L, Cram DS, Shen J, et al. Validation of copy number variationsequencing for detecting chromosome imbalances in humanpreimplantation embryos. Biol Reprod 2014;91(2):37.
11. Fiorentino F, Biricik A, Bono S, et al. Development and validation of anext-generation sequencing-based protocol for 24-chromosomeaneuploidy screening of embryos. Fertil Steril 2014;101(5):1375–82.
12. Huang J, Yan L, Fan W, et al. Validation of multiple annealing andlooping-based amplification cycle sequencing for 24-chromosomeaneuploidy screening of cleavage-stage embryos. Fertil Steril2014;102(6):1685–91.
13. Yin X, Tan K, Vajta G, et al. Massively parallel sequencing forchromosomal abnormality testing in trophectoderm cells of humanblastocysts. Biol Reprod 2013;88(3):69.
14. Wells D, Kaur K, Grifo J, et al. Clinical utilisation of a rapid low-passwhole genome sequencing technique for the diagnosis of aneuploidyin human embryos prior to implantation. J Med Genet2014;51(8):553–62.
15. Fiorentino F, Bono S, Biricik A, et al. Application of next-generationsequencing technology for comprehensive aneuploidy screening ofblastocysts in clinical preimplantation genetic screening cycles. HumReprod 2014;29(12):2802–13.
16. Vanneste E, Voet T, Le Caignec C, et al. Chromosome instability iscommon in human cleavage-stage embryos. Nat Med 2009;15(5):577–83.
17. Mantzouratou A, Delhanty JD. Aneuploidy in the human cleavage stageembryo. Cytogenet Genome Res 2011;133(2–4):141–8.
18. Vialard F, Boitrelle F, Molina-Gomes D, et al. Predisposition toaneuploidy in the oocyte. Cytogenet Genome Res 2011;133(2–4):127–35.
19. Kuliev A, Zlatopolsky Z, Kirillova I, et al. Meiosis errors in over 20,000oocytes studied in the practice of preimplantation aneuploidy testing.Reprod Biomed Online 2011;22(1):2–8.
20. Taylor TH, Gitlin SA, Patrick JL, et al. The origin, mechanisms, incidenceand clinical consequences of chromosomal mosaicism in humans. HumReprod Update 2014;20(4):571–81.
21. Magli MC, Jones GM, Gras L, et al. Chromosome mosaicism in day 3aneuploid embryos that develop to morphologically normal blastocystsin vitro. Hum Reprod 2000;15(8):1781–6.
22. Daphnis DD, Fragouli E, Economou K, et al. Analysis of the evolution ofchromosome abnormalities in human embryos from Day 3 to 5 usingCGH and FISH. Mol Hum Reprod 2008;14(2):117–25.
23. Scott KL, Hong KH, Scott RT Jr. Selecting the optimal time to performbiopsy for preimplantation genetic testing. Fertil Steril 2013;100(3):608–14.
24. Practice Committees of the American Society for ReproductiveMedicine and the Society for Assisted Reproductive Technology.Blastocyst culture and transfer in clinical-assisted reproduction: acommittee opinion. Fertil Steril 2013;99(3):667–72.
25. Capalbo A, Wright G, Elliott T, et al. FISH reanalysis of inner cell mass andtrophectoderm samples of previously array-CGH screened blastocystsshows high accuracy of diagnosis and no major diagnostic impact ofmosaicism at the blastocyst stage. Hum Reprod 2013;28(8):2298–307.
26. Fragouli E, Alfarawati S, Daphnis DD, et al. Cytogenetic analysis ofhuman blastocysts with the use of FISH, CGH and aCGH: scientific dataand technical evaluation. Hum Reprod 2011;26(2):480–90.
27. Liu J, Wang W, Sun X, et al. DNA microarray reveals that highproportions of human blastocysts from women of advanced maternalage are aneuploid and mosaic. Biol Reprod 2012;87(6):148.
28. Mamas T, Gordon A, Brown A, et al. Detection of aneuploidy by arraycomparative genomic hybridization using cell lines to mimic a mosaictrophectoderm biopsy. Fertil Steril 2012;97(4):943–7.
29. Wang Y, Chen Y, Tian F, et al. Maternal mosaicism is a significantcontributor to discordant sex chromosomal aneuploidies associatedwith noninvasive prenatal testing. Clin Chem 2014;60(1):251–9.
30. Wang H, Wang L, Ma M, et al. A PGD pregnancy achieved by embryocopy number variation sequencing with confirmation by non-invasiveprenatal diagnosis. J Genet Genomics 2014;41(8):453–6.
31. Liang D, Lv W, Wang H, et al. Non-invasive prenatal testing of fetalwhole chromosome aneuploidy by massively parallel sequencing.Prenat Diagn 2013;33(5):409–15.
32. Song Y, Liu C, Qi H, et al. Noninvasive prenatal testing of fetalaneuploidies by massively parallel sequencing in a prospective Chinesepopulation. Prenat Diagn 2013;33(7):700–6.
33. Li H, Durbin R. Fast and accurate short read alignment with Burrows–Wheeler transform. Bioinformatics 2009;25(14):1754–60.
34. Johnson DS, Cinnioglu C, Ross R, et al. Comprehensive analysis ofkaryotypic mosaicism between trophectoderm and inner cell mass. MolHum Reprod 2010;16(12):944–9.
35. Kalousek DK, Barrett IJ, Gärtner AB. Spontaneous abortion andconfined chromosomal mosaicism. Hum Genet 1992;88(6):642–6.
36. Miura K, Yoshiura K, Miura S, et al. Clinical outcome of infants withconfined placental mosaicism and intrauterine growth restriction ofunknown cause. Am J Med Genet 2006; 140A(17):1827–33.
37. Northrop LE, Treff NR, Levy B, et al. SNPmicroarray-based 24 chromosomeaneuploidy screening demonstrates that cleavage-stage FISH poorlypredicts aneuploidy in embryos that develop to morphologicallynormal blastocysts. Mol Hum Reprod 2010;16(8):590–600.
T. Ruttanajit et al.162
Prenatal Diagnosis 2016, 36, 154–162 © 2015 John Wiley & Sons, Ltd.