developing cancer and palliative care within south … · developing cancer and palliative nursing...
TRANSCRIPT

DEVELOPING CANCER AND PALLIATIVE NURSING CARE WITHIN THE SOUTH EAST LONDON CANCER NETWORK
A Cancer & Palliative Care Nursing Rotation Project
Final Report
Alison Richardson, Professor of Cancer & Palliative Nursing Care Anna Menon, Lecturer
Matthew Johnson, Lecturer Practitioner. Emma Ream, Senior Lecturer
A project supported by Guy’s & St. Thomas’ Charitable Foundation
November 2004.

2
ACKNOWLEDGEMENTS
The project team would like to thank the Special Trustees of Guy’s and St. Thomas’ Charitable Foundation for their generous grant without which this project would not have been possible. In addition they wish to express their gratitude to: The South East London Cancer Network and all the stakeholders involved in establishing and maintaining this project The rotation students for all their hard work, commitment and flexibility in learning on a new project, and also to the practitioners who supported them in their clinical learning The managers of the wards and departments where rotation students undertook their clinical placements.

3
SUMMARY
� In February 2001 an idea was put forward by a group of nurses in the South East London Cancer Network to develop the skills and knowledge of cancer and palliative care nurses through means of a clinical rotation programme. Early development work to establish the rotation programme commenced. In the summer of 2001 a service development award from the Guy’s and St. Thomas’ Charitable Foundation made it possible to press forward with this proposal, turning ideas into reality.
� The specific aims of the project were to facilitate individual nurses to develop clinical knowledge and skills in both cancer and palliative care nursing and to foster inter agency and network wide working. In doing so, the project wished to evaluate how feasible and practicable such a programme would be within the network and whether it had any wider relevance.
� Additional aims included contributing to the development of the cancer and palliative care workforce across the network, increasing the body of cancer nursing expertise and fostering links between clinical and educational service providers.
� Two Lecturer Practitioners (LPs) were employed, based at King’s College London, to co-ordinate the project and facilitate rotation participants’ clinical and academic learning.
� A cohort of 8 participants commenced an eighteen-month rotation in February 2002. They completed a portfolio of clinical competencies, academic essays and undertook a number of additional cancer and palliative care courses whilst on the rotation at King’s College London.
� Due to the small numbers recruited to the first cohort, an additional cohort commenced in September 2002, consisting of 5 participants. Overall, from both cohorts, 9 participants completed the programme.
� An evaluation of the rotation programme was undertaken, including the views of participants, LPs and clinical stakeholders, in the form of questionnaires, interviews and focus groups.
� Evaluation indicated that: o Participants gained valuable knowledge and skills and over time
established themselves as competent cancer and palliative care nurses
o Travel expenses, shift times and managing academic study and clinical commitments proved challenging and this type of educational experience is not likely to suit everyone
o There were significant challenges to overcome for all the organizations involved in hosting rotation students and the programme itself required considerable effort to manage. These included financial arrangements, mis-matches between pre existing skills and experience of students and demands of specific clinical areas, and the perceived lack of parity in host nursing teams in terms of support and supervision

4
o Whilst tensions naturally arose over the course of the project through collaboration across the various stakeholders in the Network these were resolved and the project was broadly viewed as a successful venture
o The rotation programme served to strengthen the links between educational and service representatives, working together for a common purpose
� A sustainable model for future rotations continues to be debated following lessons learned from the first two rotations. The rotation programme has now been integrated into the cancer and palliative care course provision provided by King’s College London, in collaboration with the Network. It is anticipated it will continue to evolve over time to achieve a model that best meets the demands of the workplace and aspirations of participants.

5
TABLE OF CONTENTS Page number Acknowledgements 2 Summary 3 Table of contents 5 Introduction 7 Background to the project 9 Groundwork 11 Management of the project 13 The evaluation 18 Findings 21 Discussion 57 Conclusion 61 References 62 Appendices 63

6
List of tables Table 1: Rotation study days Table 2: Evaluation programme Table 3: Key milestones in the evaluation Table 4: Routes through which students learnt of Rotation Programme Table 5: Participants’ principal objectives of participating in Rotation Table 6: Specific skills participants wished to enhance Table 7: Career aspirations 1 year after Rotation Scheme Table 8: Career aspirations 3 years after Rotation Programme Table 9: Challenges of Rotation Programme Table 10: General issues relating to the allocation Table 11: Issues related to clinical work and studying Table 12: Issues related to learning resources Table 13: Progress made in developing desired skills/knowledge Table 14: General issues relating to the allocation Table 15: Issues related to clinical and studying Table 16: Issues related to learning resources Table 17: General issues relating to the allocation Table 18: Issues related to clinical and studying Table 19: Issues related to learning resources Table 20: Destination of participants post rotation programme Table 21: Demography of stakeholders that were interviewed
List of figures Figure 1: Sketch map showing stakeholders within the South East London Cancer Network involved in the rotation programme Figure 2: Project management structure Figure 3: Development of competency tool List of boxes Box1: Rotation project participant case vignette
List of appendices Appendix 1: Service level agreement Appendix 2: Cohort 1 rotation programme Appendix 3: Cohort 2 rotation programme Appendix 4: Extract from competency document Appendix 5: Courses undertaken by participants whilst on the rotation programme Appendix 6: Characteristics of rotation programme participants Appendix 7: Questionnaires used in the evaluation
Rotation project in cancer and palliative care – students’ pre course views Rotation project in cancer and palliative care – students’ end of allocation views Rotation project in cancer and palliative care – students; end of programme views Topic guide for stakeholder interviews

7
INTRODUCTION
The South East London Cancer Network Rotation Project was concerned with establishing, delivering and evaluating a career development rotation programme in cancer and palliative nursing care for nurses who wished to develop their knowledge and skills in these specialties. It was designed with the intention of increasing the number of cancer and palliative care nurses who have been appropriately prepared to deliver high quality cancer and palliative nursing services in cancer centres, cancer units and palliative care settings. In the past individual organisations had found it challenging to provide the range of educational experience necessary to prepare a cancer or palliative care nurse. One of the main reasons for this was that comprehensive cancer services are now provided across a ‘network’, with each provider making a significant, but very specific contribution, in relation to cancer management, whether it be diagnosing, treating or symptom management. The novel element of this project involved engaging multi agency stakeholders from across a Cancer Network to develop an approach to training whereby acute trusts, community care providers and voluntary agencies (for example hospices), worked in collaboration to provide an educational programme that reflected contemporary health care organisation. The overall aim of the project was to establish a rotation programme that involved service providers of the South East London Cancer Network, embracing a rotation through different clinical areas, a structured professional development programme and access to relevant academic modules at King’s College London. Specific objectives of the project were to:
• Facilitate individual nurses to develop competent clinical skills in cancer and palliative care nursing
• Foster multi professional, inter agency and network wide work practice
• Allow nurses to gain skills in a range of clinical environments across the cancer network
• Enable nurses access to relevant academic courses to complement clinical learning
• Evaluate the feasibility, impact and practicality of such a programme within the network and beyond as a component of future cancer and palliative care nursing education provision.
On a network-wide level the project objectives were to:
• Sustain the development of a managed clinical cancer nursing network through the provision of cancer nursing expertise.
• Support the development of cancer nursing career pathways within the cancer network
• Build upon existing relationships between clinical and educational service providers.

8
This report provides a summary of this project. It starts with some background to the project and an outline of the groundwork undertaken in the early days of developing the programme and details on how the project was managed. A description of the nature and shape of the first and subsequent rotation programme is presented. The scope of the accompanying evaluation is detailed, followed by the main findings. Finally, a short discussion draws together the learning achieved through this project.

9
BACKGROUND TO THE PROJECT The government has clearly set out an agenda for change within cancer care in England (Department of Health, 2000). Those responsible for delivering cancer and palliative nursing education are having to respond to policy directives in the context of a national programme of action to eradicate variations in the availability of, and access to, high quality cancer and palliative care services. Provision of cancer services has, over the last five years, been brought together into 34 cancer networks across the country. Each network has one or more cancer centres where specialist services are provided, together with a number of cancer units providing cancer diagnosis and often treatment for the common cancers. Palliative care providers and primary care trusts are also central to the networks. The networks are intended to facilitate co-operative working between providers of cancer care from prevention, through screening, diagnostics, treatment, supportive care, palliative care and rehabilitation. The demand for competent and confident nurses to work in the fields of cancer and palliative care has never been higher. Whilst the lack of nursing manpower was recognised as far back as 1997 (Cancer Research Campaign 1997) a more recent document prepared by the Department of Health entitled The Nursing Contribution to Cancer Care (DoH 2000) served to highlight the challenges that nursing continues to face in terms of training, recruitment and leadership. The document underscores the importance of seeing the needs of patients with cancer as not just having relevance to specialist services, but to nursing across the board. Specialist cancer and palliative care services account for only a small proportion of the time that cancer patients have contact with health services. Patients are considerably more likely to be cared for by trained and untrained staff in general clinics, surgical wards, general medical wards, or by district nurses than to meet nurses who have undergone specialist cancer and palliative care training. Cancer and palliative care education for pre-registration students is patchy at best (Corner & Wilson Barnett 1992, Ferguson 1994). Post-registration education is dependent on the practitioner’s interest and the availability of, and access to, relevant education. Closs et al (1997) found that in some trusts, as little as 2% of nurses caring for patients with a primary diagnosis of cancer had any post registration qualification in cancer nursing and even in specialist areas the numbers of nurses with a specialist cancer qualification were often still very low. Commissioned by the English National Board, in 1999 Helen Langton and colleagues undertook an extensive review of the literature in the field of cancer care related to education and the preparation of cancer nurses. This revealed several desirable features of educational preparation. A key finding of the literature highlighted the importance of clinical experience within educational programmes. This review also underlined the importance of cancer care courses being designed so as to take account of the views of all the various groups of stakeholders.

10
Agreed national outcomes regarding competence in key areas of cancer nursing practice would be advantageous. Where courses have a clear practice focus it is assumed that some assessment of student’s clinical competence is being undertaken. Watson et al’s (2003) project demonstrated the challenges likely to be encountered when determining the reliability and validity of such assessments, but underlined how important an aspect of education competence is, underpinning excellence in patient care. This fact has been recognised by the cancer nursing community and the first national competency framework has just become available. These should inform the shape of our future provision of cancer nursing education. A recent piece of work undertaken by a Cancer Nursing Advisory Group at the Department of Health in 2003 sought to review, analyse and collate relevant information to facilitate the development of a model framework for a managed career pathway for specialist cancer nurses. The Nursing Contribution to Cancer Care (2000a) emphasised the importance of showing cancer nursing as an attractive career choice, with clear pathways and opportunities for development, specialisation and career progression for those who want it. It recognised that the design and implementation of rotation programmes might be one solution in a multifaceted portfolio of training opportunities. Nationally, the managed career pathway concept for cancer nursing is likely to be the subject to pilot implementation some time in the future. Some of the characteristics of any future programme were detailed as follows:
• Accountable and closely managed
• Curriculum based
• Require formal entry requirements As well as having far-reaching implications for the organisation and management of cancer services, creating a quality cancer service produces substantial challenges in education and training. It is vital we develop programmes that are visionary and responsive to the demands of contemporary cancer nursing services (Royal College of Nursing 2003). There is obvious enthusiasm and commitment to finding new ways of preparing cancer nurses, both at foundation and specialist levels. It is also clear that workforce planning and development are a major concern. The project that is the subject of this report is concerned with establishing and evaluating a rotation programme (characterised by a pathway of structured blocks of experience in clinical areas working through competency-based portfolio) in cancer and palliative care nursing in South East London, where nurses could gain experience in different care settings. Such a programme embraces the need for nurses to gain experience in diverse practice settings and harnesses the resources of a cancer network (service and education) to support workforce development.

11
GROUNDWORK During early 2000, a senior nurse (Catherine Miller) and a professor (Alison Richardson) located in South East London met and discussed concerns regarding the current lack of skilled nurses in the specialist areas of both cancer and palliative care. An idea was discussed that centered around supporting the development of the broad spectrum of skills necessary to practice as a cancer nurse, whilst simultaneously supporting individuals in their academic studies. The cancer network was identified as the ideal location for such learning to occur, which at the time was seen as a virtual organization, but in reality could offer broad clinical experiences that would reflect the cancer patient journey. Stakeholders from within the network met in Autumn 2000 to discuss the possibility of this concept of simultaneous clinical and academic learning, achieved through placement with different clinical areas across the network. Stakeholders included representatives from six primary care trusts (or their constituent organisations), four acute trusts with cancer units, two acute trusts comprising the cancer centre and five palliative care providers (Figure 1 gives a sketch map showing stakeholders in the South East London Cancer Network and their locations). Considerable progress was made in determining the format of the rotation programme and possible clinical experiences. Perhaps most vitally, commitment from each of these stakeholders was obvious and subsequent decisions could be made regarding how the rotation programme would work in practice. It was clear early on that it would be necessary to have a coordinator for the project and support for the nurses who participated in the rotation. The most appropriate professionals for this role were identified as LPs, who could facilitate the clinical and academic learning needs of the participants. Discussion also centred on the financial demands of the project and various organisations were approached to fund the rotation posts to allow nurses to be supernumerary in their positions whilst learning clinically, and also to cover the academic element of the project. These were rejected but successful funding was achieved through a grant from the Guy’s & St Thomas’ Hospital Charitable Foundation to support the employment of two LPs as well as funding for administrative, incidental and evaluation costs. However, the nurses on the rotation would have to be part of the establishment where they were working.

Figure 1: Sketch map showing the stakeholders within the South East London Cancer Network involved in the Rotation Programme
from interim report
KEY: Cancer Centre Cancer Unit Hospice University
Primary Care Trust Area
Figure 1: Sketch map showing the stakeholders within the South East London Cancer Network involved in the Rotation Scheme
12

MANAGEMENT OF THE PROJECT Further discussion enabled dedicated groups to be established responsible for managing specific elements of the project. Two dedicated LPs were recruited to co-ordinate the development and running of the rotation programme. These LPs were in post by Autumn 2001 and the project rapidly moved forward from then on. The various groups set up to manage the project can be seen in Figure 2.
Figure 2: Project management structure
Project Management Group
Manages project on day to day basis
Membership: Stakeholders
Project Steering Group
Provides expert advice and a
forum for reflection on progress and outcomes
Membership:
PMG plus invitations to external evaluation
consultant, Macmillan, Marie Curie, pan London education
representatives
Service Agreement Group
To generate operating principles and service agreement across
Trusts and organisations Membership: Managers across
stakeholders
Competency Group Development of competency
framework that will underpin the rotation and interface with
education framework in university Membership: Representation from
clinical and educational stakeholders
Evaluation Group Development of evaluation
strategy for project
Membership: Researcher and representation from
stakeholders
A Project Management Group (PMG) was formed. This group had a development, co-ordination and monitoring function. Three work groups were established to report to the PMG and responsible for developing the fine detail necessary to operationalise the project. These were a Service Agreement Group, a Competency Group and an Evaluation Group. The Project Management Group consisted of representation from all the stakeholders involved in the project and was chaired by Alison Richardson, Professor of Cancer & Palliative Nursing Care at the Florence Nightingale School of Nursing & Midwifery. The PMG met on a one to two monthly basis, with the other groups meeting on an ad hoc basis. In addition, there was a Project Steering Group. This group acted in an advisory capacity to the project and involved a wider group of interested professionals. Invitations to attend this group were extended to other educational establishments within London, representatives of cancer education charities, such as Macmillan Cancer Relief and Marie Currie, as well as the education
13

14
confederation, although none attended. This group was chaired by Cath Miller, Head Nurse, Cancer & Haematology Services, Guy’s & St Thomas’ Hospitals NHS Trust and Jackie Green, Lead Cancer Nurse, King's College Hospital NHS Trust. An Evaluation Group was established as one of the working groups and consisted of a university-based researcher, a clinical representative and the LPs. The group was chaired by the university-based researcher, Dr. Emma Ream. Links were made with an external evaluator, an independent consultant, Gill Collinson, who undertook certain elements of the evaluation. Evaluation was established as an ongoing process and planned to reflect each stage of the project from multiple viewpoints. Opinions were sought from students, LPs and the clinical stakeholders. The Service Agreement Group was responsible for resolving a whole variety of organisational issues prior to commencing recruitment and establishing the rotation. This largely took the form of developing a “memorandum of co-operation” between all the participating organisations, so that personnel, disciplinary, finance, leave and sickness issues could be addressed (The Service Agreement Document is included in Appendix 1). The group was chaired by the Nurse Director of South East London Cancer Network, Margaret Brennan and consisted of managers from the constituent organisations and representatives from the university. For specific matters as they arose, human resource and finance managers were invited to the group in an advisory capacity. The Competencies Group worked on the academic component and clinical assessment strategies of the rotation. The group consisted of senior clinical practitioners from across the network along with representatives from the university and was initially chaired by Steve O’Connor, and subsequently Matthew Johnson (both from the School). The group worked to produce a clinical competencies portfolio document. Each of the management groups aided the development of the rotation project and ensured its smooth running.
Establishing the first rotation Once the groundwork and foundation for the project had been established, recruitment for a first cohort began in December 2001 and 21 places were offered at various locations throughout the South East London Cancer Network. The LPs were new in post and so took this opportunity to meet all the clinical areas involved and publicise the rotation. There was a lot of initial enthusiasm, but the application process only yielded eight applicants. These eight participants commenced the rotation in February 2002 for 18 months. Placements were offered in a cancer centre or unit, palliative care and the community for three or six months at a time and participants spent their last three or six months back at their employing trust (see Appendix 2 for the rotation pattern for cohort 1).

15
The original number of participants was much lower than anticipated, so following discussion with stakeholders a second rotation was proposed. Changes were made to this rotation based on initial feedback and response to the first rotation. The changes were as follows:
• Recruitment through an external advert placed in the RCN Bulletin, to increase workforce in the South East London Cancer Network
• Employed by Trust following successful interview on a 12 month contract
• 12 months rotation
• Two six month placements in cancer centre or unit & palliative care
• 5 participants commenced September 2002 (see Appendix 3 for rotation pattern for 2nd cohort).
Components of the rotation The two main components of the rotation were the clinical and academic learning opportunities made available to the participants. Clinical learning was facilitated through a number of different clinical placements, which offered a variety of learning opportunities. An example of one participant’s experience can be seen in Box 1. BOX 1: Rotation Project Participant Case Vignette
D is a 23-year-old nurse who qualified just over a year ago with a degree in Nursing Studies and a Registered Nurse qualification. Since qualifying, D has worked in a bone marrow transplant unit. D joined the rotation to broaden her knowledge of cancer and palliative care nursing with a view to using that knowledge within her current work setting. Prior to joining the rotation, D had completed a King’s College London module in the care & management of clients receiving cytotoxic chemotherapy. D’s first allocation was on a specialist breast cancer unit at Guy’s Hospital. Once she settled into her new ward environment, she found that the she gained considerable experience in caring for women with breast cancer, both during the surgical management and for clients with more advanced cancer. D was able to work alongside the specialist Breast Care Nurses and gained experience in caring for women going through the diagnostic process and receiving the diagnosis of their cancer. During her time on the ward she was also able to work alongside the LP within the clinical area. In view of D’s primary interest in bone marrow transplant nursing, D undertook a module at King’s College London in haemato-oncology nursing during this placement. D’s second allocation was at Greenwich and Bexley Cottage Hospice for three months and then into community nursing. She gained a lot of experience in symptom management and undertook a relevant course at King’s on symptom management, which was able to support her learning during these placements. Her final placement was back on her own ward in bone marrow transplantation where she was able to utilise all the skills she had gained. On completing the rotation project, D had gained a rounded cancer and palliative care clinical experience.

16
The use of a competency tool developed for the rotation, with its requirement for the practitioner to produce evidence, was used with the intention of capturing direct clinical learning. Competencies were structured to reflect the cancer journey and key professional skills and were developed in such a way to ensure they:
• built in an element of objectivity into the assessment process
• directed student to gain skills across the “patient journey” from screening, to diagnosis, treatment, rehabilitation, or terminal care
• helped draw knowledge and experience together to expedite the process of learning in the clinical setting
• helped development of general nursing and managerial skills Through using the competency tool students built a portfolio, containing a record of evidence of learning during the rotation. The process adopted to develop the competency document can be seen in Figure 3. By following the concept of a patient journey in the themes of the document, this helped ensure student exposure to all aspects of cancer and palliative care and so gain the broadest experience during the rotation. Frequently this involved following a patient through their care, allowing a deeper understanding of the patient’s experience of their illness to develop.
Figure 3: Development of the competency tool
The competencies consist of a series of statements relating to a particular area of care, an example of which can be seen in Appendix 4. Presentation of evidence
Competency away day Clinical nurses from all
settings
Competency work group
HEI, acute care, palliative care & community nurses
Draft competency documents
Wide circulation to clinical staff and external education review
Competency document Trialed with first rotation cohort
Ongoing development
FEEDBACK

17
by the nurse was a key principle and was adopted in preference to the nurse’s mentor simply ‘signing off’ achievement of the competency. This mechanism was included to encourage nurses to make use of learning opportunities in a meaningful way, introduce a reflective element into learning and to reduce the subjectivity of the assessment process. Presented evidence consisted of:
• Reflective accounts of clinical situations
• Shorter notes on actions taken by the nurse
• Accounts of difficult or extraordinary situations
• Anonymised copies of patient documentation
• Anonymised copies of patient referrals, and
• Relevant patient information leaflets. Academic learning was facilitated through three weeks spent with the LPs at the School. Subjects covered are summarised in Table 1. Participants were also encouraged to undertake additional courses offered as part of the cancer and palliative care programme of education offered at King’s College London University. The additional courses the participants undertook whilst on the rotation are summarised in Appendix 5. Table 1: Rotation study days
Day one & two Introduction to the rotation project & the Cancer Network
Week one
Days three to five Introduction to Cancer Care study days
Days one to three Communication skills workshop
Day four Complimentary therapies
Week two
Day five Focus group evaluation
Days one to three Career development workshop
Day four Visit to Cancer BACUP
Week three
Day five Focus group evaluation
Optional action learning sets were also offered to the students on a monthly basis. Action learning sets are seen as an excellent way of facilitating learning through reflection whilst being supported by peers. It is a process that brings people together to find common solutions and in doing so develops the individual. Participants from both cohorts were able to come and safely discuss with the group ‘real’ issues and incidents that had occurred in practice and learn together and support each other through them. Academic assessment of the rotation comprised six assessed essays and the successful completion of the competency portfolio. The essays were graded, while the competency portfolio was awarded a pass or fail.

18
THE EVALUATION Evaluation was established as an ongoing process running throughout the project, gaining feedback from all those involved in the project. Primarily data were gathered from the participants at various time points, but also from the stakeholders who played a key role in the development and continuation of the project, along with LPs’ perspectives of the day to day running and initial establishment of the rotation. The method of evaluation was influenced by an action research approach. This approach attempts to solve problems through change management strategies. In particular, this method was used to clarify the process of implementing the programme and it was anticipated would:
• Generate appropriate processes necessary to underpin the delivery of the rotation programme
• Identify contextual factors that contribute to or inhibit the implementation of the programme
• Identify structures necessary for ongoing support of such a programme The action research process was used to continuously monitor modifications made during the life of the rotation programme with the objective being improvement. Such an approach aided the development of the project through continual cycles of feedback, particularly elements concerned with the process of programme delivery, so that aspects amenable to change could be adjusted during the life of the programme. The strategy for the evaluation is laid out in Table 2. TABLE 2: Evaluation scheme
LPs Students Stakeholders (Service managers, ward managers, Clinical Nurse Specialists)
1. Journal keeping & review
2. Interview with external
consultant, topics of interest:
• Barriers/actions
• Skills/instruction needed for post
1. Pre-course questionnaire:
• Aims
• Expectations
• Hopes/fears 2. Demographic profile 3. Learning portfolio 4. Student evaluations 5. Focus groups
1. Telephone interviews
• Perceptions of students & their competency
• Added value of LPs in supporting clinical area
Data were gathered at various key milestones and these are detailed in Table 3.

19
Table 3: Key milestones in the evaluation
COHORT 1
COHORT 2
Feb 02 START
Pre Course Questionaire
Mar
Apr
May
Jun
Jul
Aug End of Placement Questionaire
Focus Group
Sep
START
Pre Course Questionaire
Oct Mid point Course questionaire
Nov Lecturer/Practitioner Interviews
Dec
Jan 03
Feb End of Placement Questionaire
Focus Group
End of Placement Questionaire
Focus Group
Mar
Apr
May
Jun
Jul
Aug End of Course Questionaire
Focus Group
FINISH
End of Course Questionaire
Focus Group
FINISH
Sep
Lecturer/practitioner interviews
Stakeholder interviews

20
Evaluation data were gained through completion of questionnaires pre, during and following the completion of the rotation by the participants and focus groups facilitated by the independent evaluator. LPs were also interviewed by this evaluator to gather their opinions on the experience of setting up the rotation and also managing it throughout the two years. Finally, when both rotations had been concluded stakeholders, including Directors of Nursing, Ward Managers and Clinical Nurse Specialists, were interviewed over the telephone. This was to establish their perspective and viewpoints on what the rotation had meant for them and also as a channel for suggestion for improvements. Gathering data from many sources was intended to provide a wide perspective of individuals’ experiences of the rotation programme along with the opportunity to draw broad conclusions that would benefit future developments in cancer nursing education in the network. The findings from the evaluation will now be presented.

21
FINDINGS
Introduction
This section of the report will draw together the findings from the different data collection exercises, namely the questionnaires and focus groups involving the participants, the interviews with the LPs mid point and at the close of the project and the interviews with stakeholders, again at the close of the project. Data from the three groups of informants will be presented sequentially, participants, LPs and finally stakeholders.
Rotation programme participants
Appendix 6 contains a description of the characteristics of the rotation participants. In total 13 nurses started the rotation programme (8 in cohort 1 and 5 in cohort 2). From the original number recruited 1 participant in the first rotation withdrew early on for reasons of family commitments and childcare. A further participant left after one year as a result of a decision not to complete the academic work. Towards the end of the first placement of the second cohort, two participants left, one wanted a complete career change and the other was making limited progress in clinical and academic work. This resulted in 9 completing the programme.
Results from the pre course questionnaire - cohort 1 and 2 (n=13)
This section details the characteristics and aspirations for the programme held by the 13 people that commenced the Rotation Scheme. These data were attained from two sources. First from their application forms and second from the questionnaire titled Rotation Project in Cancer and Palliative Care – Students’ Pre Course Views (see Appendix 7 for data collection tools used in the evaluation). Students recruited to the project ranged in age from 23-47 years but typically they were a mature group of individuals (mean age 32 years). The length of time they had been registered nurses once again varied, between 1-25 years. The mean time they had been in oncology and/or palliative care was 0.8 months. 4 of the sample were graduates whilst another 6 were diplomats, and a further 2 whose sole qualification was the RGN (Appendix 6). The students were asked to detail how they had come to know of the rotation programme. In response, many differing routes were acknowledged (Table 4). The most common response was through their manager. There was a difference between the cohorts as it was more widely advertised for the second intake with advertisements on this occasion being placed in the RCN bulletin and Nursing Standard. Most of those recruited to the scheme were local and already working within the Trust (those comprising cohort 1). Table 4: Routes through which students learnt of Rotation Programme Route Number Percent Ward manager 3 23 Advertisement in nursing press
3 23
Poster 2 15 Leaflet 2 15 Internal advertisement on website
1 8
Multiple/combination 2 15

22
Information provided to candidates about the scheme was perceived as clear and easy to read, and the LPs that answered individuals’ queries about it were perceived as easy to access. However, the application process and the students’ views of it differed over time. The first time the scheme ran it transpired there was little time between recruitment and the scheme’s commencement. This period was reflected in students’ comments. They explained that ‘the application process did seem quite rushed’. Initially, there was little knowledge about it in some clinical areas, as one person detailed ‘…it is such an excellent project. However, after speaking to my colleagues I was dismayed at their lack of awareness.’ Comment was also made about the information provided as it was felt that the organisation ‘could have provided more detail about what the course involves & what is expected (of us) academically’. The second time the course was advertised it appeared that the information provided was adequate but one individual suggested that it would have been better had ‘more information been included about job prospects one can explore after the course.’ Students were asked to record three principal objectives they hoped to achieve by undertaking the scheme (Table 5). In the main they wished to enhance their skills, knowledge and experience with working in cancer and palliative care. Over a fifth of responses alluded to hopes of furthering their career through the scheme. Table 5 : Participants’ principal objectives for participating in Rotation Programme Objective Number Percent Increase skills/knowledge/ experience
16 46
Enhance career prospects
9 22
Enhance care 4 10 Increase understanding of other agencies
4 10
Other 5 12 The skills they specifically wished to enhance varied according to their previous experience and future aspirations. Most common responses to questions inquiring about skills they wished to progress were communication skills (20%), general oncology and palliative care skills (18%) and skills/knowledge with regards to administering chemotherapy (11%) (Table 6). The other category included references made to enhancing general management, organisational and supervisory skills.

23
Table 6: Specific skills participants wished to enhance Skill Number Percent Communication skills 9 20 General oncology/palliative care
8 18
Administration of chemotherapy
5 11
Symptom management 4 9 Palliative care 3 7 Other 16 36
The group recorded few specific learning needs but included wishing to know about pertinent government initiatives and policy. Mention was made of their desire to effect change, contribute more in the workplace – not least through cascading knowledge on return to their work base. The group were invited to detail their career aspirations, and to provide information on where they hoped to be working 1 and 3 years after completing the rotation programme. In response only 1 person stated that they were definite about the position they wished to hold a year after the Rotation whilst a further 6 were reasonably clear and 3 had a vague notion. The remaining 3 people were apparently uncertain in this respect. The majority stated that they hoped to be full time D or E grade members of staff in a variety of clinical settings. Three people reported that by this stage they hoped to be progressing towards attaining an F-grade (Table 7). Table 7: Career aspirations 1 year after Rotation Scheme Number Percent Clarity of vision Definite 1 8 Reasonably clear 6 46 Vague 4 31 Unclear 1 8 Missing data 1 8
Intended grade D grade 2 15 E grade 5 38 F grade 3 23 G grade 1 8 Uncertain 2 15
Intended area Oncology/haemato-
oncology 5 38
Palliative care 4 31 Community 1 8 Uncertain 3 23
As might be expected the students were less certain about where they hoped to work three years after completing the rotation programme. Notably, they were unclear in many instances over what their likely grade would be. However, many more hoped to be an F grade or higher by this stage as would be expected. A

24
number envisaged (n=3) that they could make the transition to research, education or practice development by this stage (Table 8). For some, this was clearly a future aim.
Table 8: Career aspirations 3 years after Rotation Programme Number Percent Clarity of vision Definite 0 Reasonably clear 6 46 Vague 3 23 Unclear 4 31
Intended grade D grade 1 8 E grade or higher 1 8 F grade or higher 4 31 G grade or higher 1 8 Uncertain 6 46
Intended area Oncology/haemato-oncology 1 8 Research/Education/Practice
development 3 23
Palliative care 4 31 Community 1 8 Uncertain 4 31 Challenges they perceived associated with the rotation programme related in the main to having to adapt to work and care effectively for patients in different settings whilst fulfilling academic obligations. Table 9: Challenges of Rotation Programme Challenge Number Percent Having to adapt to work & care effectively in different settings
11 38
Pressures of academic study & meeting deadlines
10 34
Juggling family/personal commitments
3 10
Other 5 17 Some commented on the personal commitments that could be compromised through undertaking it (Table 9). Results from questionnaire at end of 1st placement – cohort 1 only (n=7) Programme participants were invited to provide feedback at the end of their first clinical allocation (6 months into the rotation). This was achieved through completion of an investigator-designed questionnaire, and a focus group. The former allowed structured data to be collected about their transition to working in a new clinical environment, the support they received in their clinical and

25
academic work, the learning resources they utilised and their progress towards attaining their desired skills (Appendix 6). These data provided an overview of participants’ views and were complemented by those gained from the focus group. The latter provided opportunity for issues related to the project to be explored in greater detail. They provided some context for the responses recorded on the questionnaires. General Participants recorded diverse views about the ease with which they had transferred to working in their new clinical environments. Responses ranged from ‘Very easy’ to ‘Very difficult’, although the most commonly recorded response was ‘Very difficult’. Two participants had undergone two allocations during the 6-month period and were asked to comment on both experiences. Hence, the sample size in Table 10 is 9 rather than 7. Their responses may have related to the ease with which they travelled to and from work. Once again, responses to the question concerning travel to work indicated great variation. Some participants had evidently found travelling to their workplace relatively easy, whilst others had found it very difficult. This is reflected by the time taken to travel to work. On average participants had a lengthy journey (mean 78 minutes one way), which cost on average £21.25 per week. It should be noted that cost for some individuals was considerable. One person paid £66.50 per week on work-related travel. TABLE 10: General issues relating to the allocation
1 Very easy n (%)
2 n (%)
3 n (%)
4 Very difficult n (%)
Transition to working in a new clinical environment
2 (22) 2 (22) 2 (22) 3 (33)
Travel to/from work 2 (22) 2 (22) 2 (22) 3 (33)
Journey time to work (one way)
Range 35-150 minutes. Mean 78 minutes.
Cost of travel to work (per week)
Range £4-66.50. Mean £21.25
Clinical and studying Without exception, participants found it difficult to combine working in a new clinical environment alongside the requirement to study (Table 11). However, it would appear that this was relieved to an extent by support offered both within King’s College and their clinical workplace. Few individuals reported feeling unsupported in either environment. The LPs guiding their work and study were considered to be ‘Very supportive’. Respondents explained that they assisted ‘by providing support and advice – a godsend’. They were perceived as ‘very supportive, constructive and approachable’ and assisted through being ‘an independent professional with whom to discuss issues, concerns and feelings regarding placements and academic issues/concerns and progress regarding the courses and the portfolio’. They assisted participants to ‘focus’ during their time on the ward, ‘guiding them to members of the MDT to reach objectives’. Their knowledge base was recognised and appreciated. Most participants had met

26
with their LP at least once a month, and three of them as frequently as once a fortnight. They stated that the optimal arrangement would be to meet fortnightly. The few negative comments recorded in response to questioning about the least useful contribution made by the LPs related in the main to the completion of the competency document. Two individuals alluded to discovering through conversation with others that the LPs had offered them ‘differing advice’ regarding its completion. However, it was acknowledged that ‘the Rotation is a new project… and that this is also a learning period for the LPs’. A further comment lamented that the LPs had not negotiated one individual’s supernumerary status for a ‘couple of shifts’ on the busy ward they moved to. The length of the placements, which varied between 3 and 6 months, were perceived as appropriate and sufficient to meet the given competencies. There was recognition that the optimal length of placement will depend on ‘speciality and nature/number of learning outcomes to be achieved within that placement area’. One participant commented that during the final 2 months of the 6-month placement, members of the nursing team were ‘taking them for granted, and it became very difficult to meet competencies.’ TABLE 11: Issues related to clinical work and studying
1 V. easy n (%)
2 n (%)
3 n (%)
4 V. difficult n (%)
Combining work & study 0 1 (14) 3 (43) 3 (43)
V. supported n (%)
2 n (%)
3 n (%)
V. unsupported n (%)
Support from King’s College
1 (14) 5 (71) 0 1 (14)
Support of LPs 6 (86) 1 (14) 0 0
Support in placement (n=9) 4 (44) 3 (33) 1 (11) 0
Learning resources Six of the seven respondents stated that they had found the competency portfolio difficult to complete. They did, however, recognise its value as all except one recorded that it had supported their clinical development (Table 12). The learning sets were another feature that participants praised. They had successfully provided support and clinical supervision to those that had attended them. Five of the seven had taken part in at least one of these monthly meetings, and each had perceived that they had gained from it. Comments included ‘I think the learning sets are an excellent idea for providing support and clinical supervision’. Another stated that they were ‘very useful in the early stage of the project as a way of meeting with peers, comparing experiences, problems and feelings and discussing these within the structure of a supportive group facilitated by one of the LPs.’ The process was ‘reassuring’ as participants recognised they ‘were all having similar problems’.

27
Those that had not attended them commented that this had not been possible due to ‘timing… 2-4pm’ as they ‘would still be at work regardless of shift – early or late’. Further comments explained that attendance was impossible because of the ‘ward being short staffed’. TABLE 12: Issues related to learning resources
1 v. easy n (%)
2 n (%)
3 n (%)
4 V. difficult n (%)
Portfolio completion 0 1 (14) 4 (57) 2 (29)
1 Greatly n (%)
2 n (%)
3 n (%)
4 Not at all n (%)
Competencies supported clinical development
2 (29) 4 (57) 1 (14) 0
1 V. useful n (%)
2 n (%)
3 n (%)
4 Not at all useful n (%)
Utility of learning sets (n=5 attendees)
4 (80) 1 (20) 0 0
One item in this section of the questionnaire required participants to reflect on the skills that they identified at the start of the programme as ones they wished to develop. To this end, they were reminded of them and requested to indicate their progress towards meeting them. On average, individuals had made some progress, and recorded a value of >2, where 1 represented no progress made and 4 indicated that were competent in the given area (Table 13). Only 2 people recorded one area in which they had made no progress. For both, this was the administration of chemotherapy. Both individuals had been working in palliative care, and it was unrealistic to have supposed that they would have had sufficient opportunity to progress in this area. Most progress was made in the advancement of palliative care and communication skills. TABLE 13: Progress made in developing desired skills/knowledge
1 no progress n (%)
2 n (%)
3 n (%)
4 competent n (%)
Modal value
Palliative care (n=6) 0 1 (16) 1 (16) 4 (67) 4 (competent)
Communication skills (n=5)
0 0 2 (40) 3 (60) 4 (competent)
Treatment options (n=4)
0 0 4 (100) 0 3
Psychosocial care (n=3)
0 0 3 (100) 0 3
Chemotherapy administration (n=3)
2 (67) 1 (33) 0 0 1 (no progress)
Patient education (n=2)
0 0 2 (100) 0 3
Liaison skills (n=2) 0 0 2 (100) 0 3
Symptom 0 0 2 (100) 0 3

28
management (n=2)
Time management (n=2)
0 2 (100) 0 0 2
Surgical procedures (n=1)
0 0 1 (100) 0 3
Knowledge of disease process (n=1)
0 0 1 (100) O 3
Knowledge of haematology (n=1)
0 0 1 (100) 0 3
Confidence (n=1) 0 0 1 (100) 0 3
Knowledge of oncology
0 1 (100) 0 0 2
New placement The questionnaire inquired about participants’ feelings towards their next placement. Comments they made in reply comprised a range of emotions from apprehension, to growing confidence and eager anticipation. Three of the seven participants recorded that they had concerns about their ongoing participation in the Rotation Project. Their comments related to the completion of the competency document, keeping up with the workload and the expense of travel. Some additional comments written at the end of the questionnaire summarised some of the participants’ thoughts and feelings. These included:
‘Despite the expense and the travel difficulties I have enjoyed and benefited professionally from this allocation.’ ‘Participation in the Rotation Project has been worthwhile and (generally) enjoyable so far, but I feel certain issues have been highlighted with the portfolio and with changing LPs… which might affect my progress over the next part of the project… Have felt well supported by my LP within my first two clinical areas and have achieved some of my initial aims already.’ ‘Good course so far, let’s hope it continues!’
Results from focus group at end of 1st placement The focus groups were undertaken at three points over the course of the rotation programme. The first was held after the first clinical placement and attended by cohort one only. The second was held mid way, when cohort one had completed two placements and cohort two had completed one placement. The final event was held in September 2003 when both cohorts had completed the programme. Results from the latter two appear in a later section of the report. Each was led by the same external facilitator, and was supported by the same note taker (Gill Collinson and Emma Ream) to ensure continuity of approach. Each focus group was held at Kings College London and lasted for approximately two hours. On each occasion participants were invited to share their individual experiences, prompted by some focused questions, through drawing or writing on a piece of flip chart paper. This approach enabled participants to be creative in how they expressed their experience and gave a template for them to focus their thoughts. The sharing of experiences was followed by a general discussion on each occasion, questioning for clarity and to draw out common themes.

29
All eight participants of cohort 1, the external facilitator and note-taker, attended the focus group at the close of the first placement. Following introductions, an explanation of the planned process and setting ground-rules for working together, the participants were asked to write and/or draw, on a piece of flipchart paper, their experiences of their first placement. The following is a synthesis of this work and subsequent discussions
Reasons for joining the rotation project. All the participants regarded the rotation project as primarily an opportunity to develop their career path. All were interested in gaining a breadth of practice-based experience, within an educationally supportive environment. The individual experiences and motivations for applying to the rotation however varied considerably. The security provided by the secondment type arrangement, enabled some participants to explore the range of opportunities available and to gain knowledge and experience, without the anxiety associated with changing employment. Still others were feeling stifled within their role, to the point where confidence was undermined and uncertainty regarding their next career move was present. The project was therefore an opportunity to explore and gain confidence, before deciding on any particular direction. In contrast “wanting to get teeth into a specialty” was also described by a participant, who having explored a number of clinical specialties had come to a point of needing focus and developing a depth of knowledge and experience. Being involved in the first cohort of this innovative project was also an attraction to some participants. It was however the innovative combination of acquiring specialist clinical skills and knowledge, within a supportive educational environment that primarily attracted the participants to the rotation project. Issues arising from 1st placement. All the participants had a wide, if somewhat different range of experiences throughout their first placement. Some stayed at their “home base” for the first placement, whilst others were in very different environments. Some participants were warmly welcomed and supported by staff, others less so. There were however a number of themes evident. Staffing. Most of the clinical areas were experiencing a shortage of qualified, experienced nursing staff. This resulted in a number of issues for the participants, including lack of opportunity to leave the practice area for visits to related departments and spending time with members of the multi-disciplinary team. Time with senior staff and or mentors was also limited, although they were reported to be generally very supportive of the individual and the programme as a whole. Peer grades appeared to be less well informed about the rotation project and were perceived to be less supportive in some instances, particularly in recognising when participants felt out of their depth and in unfamiliar territory. Travel. The most significant practical issue, for the majority of participants was problems related to travel and in particular using public transport. Placements in organisations further away from home and different shift systems created varying levels of difficulty. There was greater financial outlay and no short-term

30
accommodation available. There was also reluctance on the part of managers to offer flexibility in terms of shift patterns and in particular the opportunity to work long days, which would have helped in some circumstances. It was acknowledged however, that at least some participants would be experiencing problems with transport, were they not participating on the rotation project. The problems associated with travelling were largely accepted as part of living and working in London and whilst tiring and irritating, were not seen as a reason for not participating in this form of programme. Confidence. Being in a different environment was both exciting and anxiety provoking for participants. Many were unsure of their ability to function within a new practice setting and some initial anxiety and self-doubt was reported. However over time participants discovered new skills and that many of their existing skills were transferable. Participants found that there prior experience, for example in palliative care, was valued and appreciated in more high tech areas. Participants discovered that they had something to offer the new practice setting as well as having much to learn and recognised that their confidence had grown. Coping strategies. Some participants reported the challenges associated with working within an environment in which death and dying were constant features and that they found it emotionally “demanding and draining”. Individuals found that their own experiences of loss were revisited and that it was a time of personal as well as professional learning. The support of the unit staff and LPs was particularly important, during such experiences. For others, more experienced with working in a palliative care environment it was the aggressiveness of the high tech areas and the staff’s difficulty in accepting when a patient was going to die that was challenging. The emotionality of working in such areas is both part of the intrinsic fulfilment of helping others but also personally challenging for all practitioners. The educational experience was interpreted by participants as that relating to the formal modules on offer as part of the rotation. Individuals were able to choose which modules they took and when they took them, depending on the university timetable. Some chose not to do any modules during the first placement whilst others did. Some practical issues were also confounding participants in particular difficulties accessing the library and computer facilities. For those undertaking courses, managing work, home and studying proved to be the major challenge. The first placement appeared to have been the time when participants tested how much they could reasonably take on, recognising their individual circumstances and learning styles. The content of courses raised little comment. Participants who had undertaken courses enjoyed the challenge and stimulation of learning new knowledge and skills and found their own way to manage the extra work associated with assignments. Portfolios. Participants reported how completing their portfolios was time consuming and that it was both “tedious” and hard finding “evidence for

31
everything”. The need for patient confidentiality, also posed some difficulties when acquiring evidence, as did finding the time to achieve all the required visits associated with a specialist area. It also felt uncomfortable, “constantly reminding” staff to verify portfolios, particularly when wards and units were so busy and often short of staff. Participants generally reported management of the programme to be positive. The support mechanisms put in place was particularly appreciated. Lecturer/practitioner role. The support provided by the two LPs was highlighted by all as being very positive, and for particular individuals the key reason for staying with the project during difficult periods. They particularly appreciated knowing that they were available for professional and personal support, as aspects of the placements raised personal issues for some participants. Most found working with Matt or Anna in the clinical area quite daunting at first, describing it as if they were being watched or tested in some way. But over time this one to one support within the practice area became a much appreciated aspect of the support offered by the LPs. There was some anxiety expressed that the LPs would not be as available after the second cohort started in September and recognition that they had received a lot of support. Learning sets. Generally about 50% of the group attended the learning sets. These were not obligatory, but those attending, had found it useful to get together and share experiences. Some went away feeling better, knowing that everyone is in the same boat and others felt worse listening to another’s experience of the clinical area that they were about to go to! Spotlight. Many of the participants enjoyed being involved in the project, which was attracting interest and attention. Some felt that managers were only interested in the kudos of being part of the programme and neglected the day-to-day concerns of clinical staff having to supervise another group of learners. Participants appreciated that there would be teething problems associated with the newness of the project and realised that they were “guinea pigs”. Consistency of approach. The lack of consistency across the placement areas regarding the amount of supernumerary time for participants on the rotation project was a cause for concern amongst participants. Some found themselves being “part of the numbers” all of the time and having to negotiate time away from the ward area. Others had a period of supernumerary time built in to the off duty to support the acquisition of competency and completion of portfolios. For those participants already graded at E there was also an expectation that they would be able to fulfil E grade responsibilities, for example being in charge of the area over the period of a shift, when the individual did not have the required specialist knowledge and understanding. Participants agreed that a more consistent approach to these issues should be sought by those responsible for the programme.

32
Results from questionnaire at 12 month point – cohort 1 only (n=7) Participants in cohort 1 provided feedback on the Rotation Project at the end of their second clinical allocation (after 12 months of being on the programme). The same questionnaire was utilised for this as was used following the first placement, and again these data were augmented with data from a focus group.
As previously, the end of allocation questionnaire comprised four sections: general issues, issues related to clinical and studying, a section on learning resources, and questions related to their next placement. The findings from this questionnaire are presented under these headings. General As found when data were collected following the first 6 months, participants recorded diverse views about the ease with which they had transferred to working in their new clinical environments. Responses ranged from ‘Very easy’ to ‘Very difficult’, although in general the group had found it relatively easy (64% recorded that it was relatively easy/easy). Four people had worked in 2 locations over the 6-month period and provided data on both of these. As regards travelling to work (Table 14), participants once again reported that this had not been easy. In fact 64% rated it as fairly/very difficult. Typically travel to work was lengthy averaging around 1 hour and for someone it had taken around 2 hours each way. Travel costs averaged £22.75 a week. Again there was some variation with one person paying £40 a week for travel. TABLE 14: General issues relating to the allocation
1 Very easy n (%)
2 n (%)
3 n (%)
4 Very difficult n (%)
Transition to working in a new clinical environment
1 (9) 6 (55) 2 (18) 2 (18)
Travel to/from work 2 (18) 2 (18) 6 (55) 1 (9)
Journey time to work (one way)
Range 30-120 minutes. Mean 58 minutes.
Cost of travel to work (per week)
Range £8-40. Mean £22.76
Clinical and studying Without exception, participants found it difficult to combine working in a new clinical environment alongside the requirement to study (Table 15). However, it would appear that the support provided by the LPs from King’s College continued to be valued highly. (86% of the cohort rated the LPs as very supportive, whilst the other 14% as supportive). Three students commented that the LPs were most helpful ‘with completion of academic work’. However, it appeared that they provided considerable ‘ reassurance and encouragement’. Through ‘visiting regularly’ it appeared they provided opportunity to be good listeners and acted as a ‘sounding board’. Four students had met with their LP fortnightly during their

33
placement and the other three reported that they typically met with them monthly. The frequency with which they met with them appeared to meet students’ approval. For some individuals the LPs helped them cope with both personal and professional crises. They appeared to have gained both the trust and respect of the student cohort who found their feedback ‘constructive and informative’. The only shortfalls alluded to by the students with respect to the LP input related to lack of time. Three of the student group referred to insufficient opportunity to work with them clinically, thus they did not find them especially helpful with regards to developing skills in practice. Views on support provided by clinical placements varied. The majority of students (73%) found they were well supported on placement, however, one individual reported that they had felt very unsupported. TABLE 15: Issues related to clinical and studying
1 V. easy n (%)
2 n (%)
3 n (%)
4 V. difficult n (%)
Combining work & study
0 0 3 (43)
4(57)
1 V. supported n (%)
2 n (%)
3 n (%)
4 V. unsupported n (%)
Support from King’s College
3 (43) 3 (43) 1 (14)
0
Support of LPs 6 (86) 1 (14) 0 0
Support in placement (n=11)
2 (18) 6 (55) 2 (18)
1 (9)
Learning resources Students were asked to record how easy/difficult the competency document was to complete. As when asked this following the first 6 months of the programme, the student cohort feedback that this remained difficult. Once again, six of the seven respondents stated that they had found the competency portfolio difficult. Views about its contribution to clinical learning varied. Whist 4 of the student group (57%) believed it supported their learning the remaining students (43%) appeared to question its value at this point in the programme (Table 16). It appeared that as time progressed the learning sets were less well attended. During the second 6-months of the programme only 2 of the group attended these. Reasons for not attending related to lack of time – either because they were working clinically or because they were studying. Two individuals had missed the learning sets as they had been unaware of times they were provided.

34
TABLE 16: Issues related to learning resources
1 V. easy n (%)
2 n (%)
3 n (%)
4 V. difficult n (%)
Portfolio completion 0 1 (14) 4 (57)
2 (29)
1 Greatly n (%)
2 n (%)
3 n (%)
4 Not at all n (%)
Competencies supported clinical development
1 (14) 3 (43) 3 (43)
0
One item in this section of the questionnaire required participants to reflect on the skills that they identified at the start of the programme as ones they wished to develop. To this end, they were reminded of them and requested to indicate their progress towards meeting them. In response, the students recorded that they had made great progress towards meeting the majority (90%) of their aims. Two individuals recorded that they had made limited if any progress with enhancing palliative care skills, one individual stated that they had made no progress with regards to administering chemotherapy, and one person believed that they had made little progress as regards time management. However, taken overall the progress made between the 6 and 12-month points in the programme were evident and provided understanding of the areas of professional development that the Rotation was contributing to. Concerns regarding rotation At the 12-month point in the programme, there were still individuals (4 of the 7) that still had concerns about the programme. These related principally to difficulties with completing the portfolio in addition to managing clinical commitments.
Mid programme focus group
The mid programme focus group was held in Spring 2003 King’s College London. The event was attended by a total of nine participants (cohort one (n 6) and two (n 3)), the facilitator and note taker. Participants were asked to reflect on the high and low points of their experience of the rotation project to date in the form of a mind map. Participants from cohort one had completed two placements and those from cohort two had completed one placement at this time. Whilst participants had unique individual experiences of the programme, a number of key themes emerged to describe these experiences. Placements in clinical practice Culture. The culture of the clinical practice areas where participants on the rotation project were placed had a major impact on how participants regarded their experience of the placement. The attitude of the permanent staff members and their understanding of the rotation project were critical in determining how

35
participants were welcomed to the practice area and subsequently supported throughout their stay. There was a large variation both between and within participating organisations as to the level of support offered and degree of interest in the rotation project as a whole. Some participants experienced a high level of support, which they described as “feeling part of the team” and “excellent support” and were given time to take advantage of the learning opportunities particular areas had to offer. Others felt that there was an expectation from clinical areas that they would be fully competent to practice at a high level within the specialty area form day one of their placement and that they were left to find their own way and then criticised if they made mistakes. One participant described her experience as “horrible 2nd placement, I lost all enthusiasm, no support offered by the ward”. The way in which participants were either included in or excluded from the social aspects of ward life was another critical factor in how easily they settled into a particular placement. Where areas had a strong group identity and staff had worked together for a long time some participants found it difficult to feel accepted as part of the team. Some participants found that staff in particular areas made assumptions about them as illustrated by this comment. “There was some bias from nurses who had been there a long time who thought I was too young to be in palliative care” Organisation. Aspects of how the participating organisations operated were challenging for some participants. For some being within a hospital ward environment after a long period of working in other settings was particularly challenging, for others it was issues such as shift times and patterns that were difficult Staffing. As in the first round of focus groups staffing issues within the clinical areas affected the experience of participants. Many of the areas continued to experience staff shortages that stretched the expert resource available to the students. This manifested as a lack of time and opportunity to work with mentors and visit other departments associated with the clinical placement. For some it also meant that the opportunities to develop new skills or consolidate others were reduced and that they felt as if the were left “to sink or swim”. For others it had an impact on their own morale” fed-up of giving sub-standard care and feel like a crap nurse”, whilst questioning “are the managers aware? Do they care?” Travel. Travel continued to be a significant issue for many participants, primarily because of the distances to be travelled at unsocial hours, coupled with the frustrating inefficiency of the London transport system, However there was much more of a resigned nature to the expression of frustration compared to the first focus group event. Participants appeared to be more accepting of the situation despite its negative impact on their experience, with comments such as the “travel is still a drag but not as bad as previous placement”.

36
Learning
Educational aspects. During the focus group event participants once again discussed the challenge of completing assignments and portfolio’s. It was generally agreed that the work associated with completing the competency framework was excessive and the group recommended that the portfolio be tailored to particular placements and be reduced in overall size. Some participants commented that they were “not coping with competency folder” and felt “no good at academic writing”. There was some frustration expressed that this received such little formal recognition in terms of marks and also some disappointment and a little cynicism regarding the lack of academic recognition associated with the rotation project when compared to other programmes such as the Royal Marsden Diploma in Cancer Care. All participants were however very pleased with how much they had learnt in the previous few months despite some of the practical difficulties of studying whilst working full time, “still loads to do for the portfolio and the clock is ticking”. Confidence. Overall, participants had found their confidence had increased. All of them had experienced peaks and troughs during their experience of the project, with some participants having serious thoughts as to whether they could continue, as described by one participant as “why am I doing this? I’ve really had enough”. The support of the LPs was considered to have been critically important to individuals at these times. Results from end of rotation programme – cohort 1 and 2
General The findings presented regarding views at the end of the programme are those from both cohorts that completed the programme (n=9). During the final rotation, most students were working back at the Trust employing them (their home base). As a result, it is unsurprising to see that both time spent travelling to allocations (mean 32 minutes) and the costs involved (£11.30) were lowest at this time (Table 17). Most students reported that they found transition to working on this final rotation relatively easy. Given that for many this was where they had worked previously, this was expected and notably different from the difficulties expressed with commencing new placements on previous occasions. Although as previously responses ranged from ‘Very easy’ to ‘Very difficult’, in general the group had found it easy (77% recorded that it was relatively easy/easy). Once again 2 people had worked in 2 locations over the 6-month period and provided data on both of these.

37
TABLE 17: General issues relating to the allocation
1 Very easy n (%)
2 n (%)
3 n (%)
4 Very difficult n (%)
Transition to working in a new clinical environment
5 (39) 5 (39) 2 (15) 1 (8)
Travel to/from work 10 (77) 3 (23) 0 0
Journey time to work (one way)
Range 5-75 minutes. Mean 32 minutes.
Cost of travel to work (per week)
Range £0-25. Mean £11.30
Clinical and studying Towards the end of the programme the students reported having less difficulty combining clinical commitments alongside the requirements of academic study (Table 18). This may reflect the relative ease with which they returned to working in familiar surroundings that required little reorientation before they reintegrated into nursing teams. Alternatively, this may have arisen if they had successfully completed the majority of the academic requirements of the programme by this stage. The LPs continued to provide support to students until they completed the study. Students wished to meet with LPs fortnightly or monthly and this was in the main what was provided. They commented without exception that the LPs were supportive. They were praised for the ‘support’, ‘time’, ‘understanding’ and ‘encouragement’ they provided. Further, they were singled out for their accessibility. Once again, the support provided in the clinical settings varied considerably. Whilst the majority of workplaces were regarded as supportive, 3 (23%) were not. TABLE 18: Issues related to clinical and studying
1 V. easy n (%)
2 n (%)
3 n (%)
4 V. difficult n (%)
Combining work & study
2 (22) 3 (33) 3 (33)
1(11)
1 V. supported n (%)
2 n (%)
3 n (%)
4 V. unsupported n (%)
Support from King’s College
8 (89) 1 (11) 0 0
Support of LPs 6 (75) 2 (25) 0 0
Support in placement (n=13)
6 (46) 4 (31) 2 (15)
1 (8)
Learning resources Students persisted in their reports that the competency document was difficult to complete – all students bar one perceived it as a difficult course requirement. Towards the end of the programme they did appear to see its relevance and value for development of clinical competence. Three of the students (33%)

38
recorded that the document greatly supported their acquisition of skills and competencies and a further 5 (56%) perceived that it had been of some value (Table 19). Learning sets were attended by some of the students. Over the final 6 months of the programme they were attended by four of the 9 individuals. Of these 3 reported that they had been useful. Reasons for not attending included being unaware of their conduct (n=2), shift patterns e.g. night duty (n=2) and being unable to leave the ward but feeling supported by them and thus not needing to attend the sets in any case (n=1). TABLE 19: Issues related to learning resources
1 V. easy n (%)
2 n (%)
3 n (%)
4 V. difficult n (%)
Portfolio completion 1 (11) 0 6 (67)
2 (22)
1 Greatly n (%)
2 n (%)
3 n (%)
4 Not at all n (%)
Competencies supported clinical development
3 (33) 5 (56) 1 (11)
0
The students did report difficulties with leaving the ward to visit other areas and departments. This was required for the fulfilment of all competencies. Reasons explaining this shortfall included: ‘did not feel supported by any placements to make visits required for competencies’, ‘not given time for visits’ ‘the ward is too busy’, ‘visits made in own time’ (students cohort 1) and ‘did not complete all the recommended visits due to staffing levels’ (student cohort 2). When asked to reflect on their progress towards meeting their aims for the programme – the skills they wished to attain - the 9 students that completed the programme recorded that they had made good progress with meeting these. Only 1 student recorded that limited progress had been made towards meeting one aim, related to time management. Across all others, good progress had been made and the students reported that they had entirely met 19 (35%) of them. Reflections on entire programme At the end of the programme the students were asked to report on the degree to which the programme had met their expectations, to comment on the relevance of the programme to their clinical role and to state whether they would recommend it to others. All students reported that the programme had met their expectations. Five individuals (63%) stated that it had completely met expectations. One person suggested that there was ‘more academic work than I expected from original programme information… left less time to continue outside interests/hobbies’ (cohort 2). Comments did suggest ways that it could be improved. Included were the following: ‘(I) feel that some community experience and possibly primary care experience would have been useful’ (student cohort 1)

39
‘More guidelines for the clinical areas about the rotation. For example my second rotation was reluctant to give me time to complete visits’ (cohort 2) ‘Both clinical areas gave me 3 weeks supernumerary at the start – which I did not feel I needed. This could be clarified so that students could use the supernumerary time later to complete visits etc… for the portfolio.’ (cohort 2). All viewed the programme as relevant for their clinical role. Comments in support of this included: ‘it has developed my skills greatly both clinically and professionally. Also feel more confident academically… It’s an excellent experience to understand cancer nursing and cancer patients’ experiences.’ (cohort 1). ‘(I have) greater understanding of the cancer journey, and how different clinical areas fit into the cancer network, better appreciation that a diagnosis of cancer does not mean necessarily a death sentence (home area very palliative!) and people can literally ‘live’ with cancer for many years’ (cohort 1). Another individual that worked in the community explained the particular relevance for them: ‘ I am more confident with clients and relatives especially around death and dying… Working in the community we nurse clients who want to die in their own home or who are currently dealing with a cancer diagnosis. The rotation has given me the confidence to deal with (this)’. (cohort 1) Seven out of 9 perceived it as entirely relevant. All would recommend the programme to others. As they explained ‘I have found the rotation an excellent experience. It has allowed me to gain experience in different clinical environments and different NHS Trusts. Also the options and availability of courses is excellent’ (cohort 1). Two people had already recommended it to others. As one person explained: (I) have recommended to lots of people who want a better understanding and experience of cancer and palliative care (cohort 1). Another said simply: ‘It’s been invaluable (cohort 1). Table 20 details the destinations of the participants on completion of the programme.
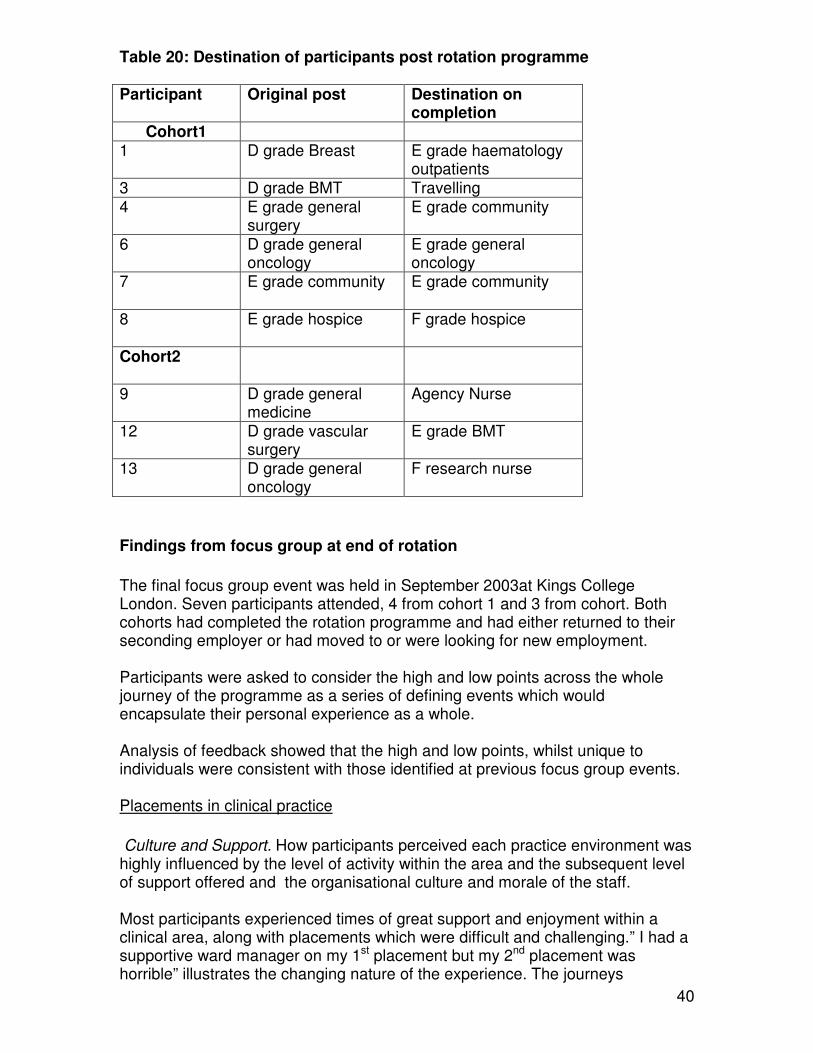
40
Table 20: Destination of participants post rotation programme Participant Original post Destination on
completion Cohort1
1 D grade Breast E grade haematology outpatients
3 D grade BMT Travelling 4 E grade general
surgery E grade community
6 D grade general oncology
E grade general oncology
7 E grade community E grade community
8 E grade hospice F grade hospice
Cohort2
9
D grade general medicine
Agency Nurse
12 D grade vascular surgery
E grade BMT
13 D grade general oncology
F research nurse
Findings from focus group at end of rotation
The final focus group event was held in September 2003at Kings College London. Seven participants attended, 4 from cohort 1 and 3 from cohort. Both cohorts had completed the rotation programme and had either returned to their seconding employer or had moved to or were looking for new employment. Participants were asked to consider the high and low points across the whole journey of the programme as a series of defining events which would encapsulate their personal experience as a whole. Analysis of feedback showed that the high and low points, whilst unique to individuals were consistent with those identified at previous focus group events. Placements in clinical practice
Culture and Support. How participants perceived each practice environment was highly influenced by the level of activity within the area and the subsequent level of support offered and the organisational culture and morale of the staff. Most participants experienced times of great support and enjoyment within a clinical area, along with placements which were difficult and challenging.” I had a supportive ward manager on my 1st placement but my 2nd placement was horrible” illustrates the changing nature of the experience. The journeys

41
described by participants in this final focus group, were a series of peaks and troughs, which were generally associated with how each participant experienced a particular placement. The following two comments from the same participant illustrate this well, “my patients actually enjoy my care, they have given me back my confidence” and “here we go again…no support, family crisis…. I don’t want to do this anymore”. Participants described a series of transitions, from placement to placement where their ability to adjust to a different environment, pace of work, different patient groups and treatment modalities was determined by the way in which they were initially welcomed and then supported by the permanent staff in the clinical area as illustrated by, “It was hard breaking in (to the ward team), felt very shut out and isolated”. In previous focus groups participants had accounted for lack of support with the fact that clinical areas were so short staffed. On this occasion however participants were able to discern that negative experiences of an area were not necessarily a result of poor staffing levels but could be attributed to attitude, culture and lack of clinical leadership. Travel. The challenges of travelling in London had caused difficulties for most participants at different times throughout the rotation. However there were also some positive experiences of being near to home on particular placements and enjoying walking the patch whilst working in the community. “I was close to home, on this placement – no travelling”. Learning
University experience. The educational resources available to participants were perceived to be very good and the library made returning to study a much less daunting experience than had been anticipated. The support of the “friendly, helpful librarian” was much appreciated by more than one participant. Participants perceived the support received from academic staff and their peers as critical to their success, using phrases like “not going it alone” to describe the importance of this support. They were however disappointed that the programme only accrued 30 credits. They were also appreciative of the opportunity of being exposed to leaders in the field of cancer nursing both within the university and clinical settings. “Nice to meet people who’ve written books and done research” were comments made in this regard. LP role It was universally agreed by participants that “Matt and Anna made the programme”. The ongoing personal and professional support in the practice areas and academic environment was critical to all the students and for some a major reason for staying with the programme during challenging times. The fact that “Matt and Anna were always on the end of the phone” and “A lot of support”

42
during a difficult placement illustrate how important these roles were to the success of the programme form the perspective of the participants. Portfolio and essays The portfolio continued to be regarded as a valuable learning resource, despite being considered “time consuming” and on occasions “tedious and boring”. Participants were pleased that changes to the portfolio were being made on the basis of their experiences. The essay titles had created anxiety for some participants as they were “open and vague” and the support of the staff in interpreting them was appreciated. Some participants were still feeling the anxiety of recent deadlines to complete and hand in work “Felt panic. Too much work and only a month to go”. Confidence Participants unanimously agreed that they felt much more confident as a result of taking part in the rotation programme and that despite the highs and lows it was a “fabulous experience” and “would recommend it”. Being able to “see the cancer journey and understand what people go through” was a particularly important aspect of the learning. One participant’s comment “I can do this …this is what nursing is all about”, sums up the feeling of the group, that despite the challenges they all felt much more able to deliver nursing care to patients with cancer, wherever they may be in their journey. Findings from interviews with LPs The LPs appointed to support the rotation programme were interviewed on two occasions to ascertain their experience of working on this unique project. The first interview took place in the first few months of the programme commencing. The second interview was held in October 2003 at the end of the project, when they were interviewed together. Each interview lasted for approximately one hour. The interview was unstructured in that it proceeded as a flow of dialogue rather than a series of questions, but centred on experiences to date, learning accumulated and other issues or concerns. Interview One The first interview focused primarily on the early development of the rotation programme, the development of relationships with stakeholders and the development of the working relationship between the two LPs. Each of these areas was interlinked but is separated here for the purposes of analysis. Development of the rotation programme. At the time of the interview both LP’s described the intense pressure of getting the programme started, in particular the recruitment of participants, understanding university procedures and working with the partner organisations. They felt the “honeymoon” was over. The beginning was considered “a crazy time” particularly in regard to recruiting participants and both had been challenged by the level of independence associated with their role, i.e. in managing their own time etc. Some challenges also emerged for the LP’s as one had been appointed before the other and some people had a

43
perception that one was in charge rather than it being a more equitable partnership. This manifested itself primarily in other people’s perceptions. Development of working relationship between LPs. Both LP’s recognised early on that they had different strengths and that they could compliment each other “one being organised and one academic. They also recognised that the conflicts that emerged between them came from a lack of confidence in themselves in a new and unfamiliar role, some jockeying for position and some different views about how the programme should be organised. In the whole they felt that they worked through these issues to resolution and that having to manage the stakeholders, university and participants together made it in their best interests to work together constructively. Working with stakeholders. Both LPs found working with the diverse group of stakeholders challenging and a real learning experience. The frustrations experienced arose mainly from a lack of decision making and people attending meetings without organisational authority. In addition they found the local political agenda could be played out in meetings associated with the programme, along with some fundamental misunderstandings on the part of NHS organisations on how universities do business. Problem solving regarding clinical placements and dealing with the range of policies operating within each hospital were major challenges along with the lack of secretarial support and the administrative aspects of managing the programme. Second Interview The two individuals clearly complimented each other and had found a level of synergy in their joint approach to managing the project and supporting the participants. They played to their strengths and were highly aware of how their differences in approach were both an asset and at times a liability. The highlights of the programme were considered to be:
• Completing the project successfully
• Witnessing the growth and development of the participants
• Exposure to and learning to manage the local political agenda
• Being involved in and understanding the cancer network
• Developing personal networks
• Developing “intelligence” regarding how to obtain resources etc Both LPs valued being involved in a new and innovative project and being able to influence the development of the programme and the LP role.
44
The challenges at the beginning of the project centred on difficulties arising from the recruitment process for participants and the lack of understanding of some stakeholders. In addition both were new to working within a university environment and found themselves on a very steep learning curve regarding the institutions policies and procedures along with difficulties in obtaining sound advice. The LP role. It was perceived that the role of LP developed in a way that bore little relation to the original job description. Both felt that at the beginning the project was too ambitious and that the boundaries were unclear. It was regarded as being a valuable experience, despite not being quite what they thought it would be like when they applied for the post and it was recognised that this is the nature of such innovative ventures. They recognised that they had developed a broad range of new skills as a result of the role and these were identified as being
• Course and curriculum development
• Working with stakeholders
• Project management
• Influencing skills
• Problem solving
• Managing uncertainty
• Consolidating teaching skills They also discovered that they developed a greater understanding of the voluntary and hospice sectors and the strategic aspects of cancer policy. Concerns. The major concern of the LPs at this point in the project was the sustainability of the programme and how it could make the transition from being an innovative project to being part of what is offered by the university and healthcare organisations within the cancer network. There was some concern that because the programme did not fit the traditional portfolio of the university it was not valued or taken as seriously as more traditional routes of learning. Engaging fellow lecturers to participate in the programme was also a concern as university resources are as stretched as those within clinical placement areas. It was also recognised that there would need to be ongoing dialogue and work with key stakeholders because of the ever changing landscape of the health sector, whether in terms of individuals moving on or changes in broader organisational arrangements.

45
Summary Both post holders had clearly developed personally and professionally from the experience of working as LPs with the cancer nursing rotation project and neither regretted being involved in this innovative programme. How their level of self-awareness and professional maturity had deepened was evident over the course of these interviews. Both were able to look objectively and strategically at the impact of the rotation programme on participants, organisations and themselves. Stakeholder Interviews Sample Stakeholders from across the South East London Cancer Network were sampled to gain Trusts’ views on the efficacy and potential of the rotation programme as it drew to a close. They were selected purposively to ensure cross network representation, and guarantee inclusion of individuals from acute cancer, palliative care and community settings. Care was made to incorporate views at ward and organisational level. In the event, telephone interviews were conducted with 11 individuals, and included nursing personnel from the Network Lead Cancer Nurse, organisational leads, and ward managers (Table 21). Table 21: Demography of stakeholders that were interviewed Network Cancer
Centre Cancer Unit
Hospice PCT
Lead Nurse 1 1 1 1 1
Ward/team manager
1 1 1 1
Day Unit manager
1
Practice Development Nurse
1
Stakeholders’ opinions of the rotation project did vary greatly; variations occurred both within and between clinical settings. A consistently held view was that students’ clinical performance was influenced by their nursing backgrounds and influenced the ease with which they adapted to new clinical challenges. Some students enjoyed challenges associated with working in new and diverse clinical settings. They ‘threw themselves into all areas they worked in, even those alien to them’ (Network Lead); they ‘grasped opportunities that came their way and integrated in to the ward team easily (hospice-based Practice Development Nurse). This positive approach impacted on the wider nursing team who in some cases were inspired and motivated by the students’ approach (Lead Nurse).
46
Conversely, other students were perceived as having made a negative impact on the team through ‘not being up to scratch’ (Lead Nurse), or needing ‘coaxing’ (hospice-based Practice Development Nurse). Some individuals appeared to display limited commitment to the ward area outside their own agenda of needing to complete the competency document. ‘For one (student), their own agenda was their only agenda, and the team got tired of that’ (hospice-based Practice Development Nurse). Whilst others cared about their learning, but displayed more commitment to the organisation in which they worked; ‘it was not just everyday work’ (Network Lead). However, taken as a whole rather than on individual basis, the programme was seen with potential to challenge existing practice, bring about change, and enhance the knowledge base of individuals in the SELCN. Seeing with fresh eyes A commonly voiced view of stakeholders related to how personnel with different experiences and perspectives of caring could look critically at new clinical areas in which they worked. This was seen in a positive light: ‘We take for granted what we do… they bring some new skills and fresh new opinions about our work… You don’t want a ward to be static.’ (Ward manager cancer care). One ward manager suggested that since rotation students do not ‘stay for ever, they may feel freer to comment constructively on care provided’ (Hospice Ward Manager). Another stakeholder perceived the potential for enhanced evidence-based practice with host areas having to justify their practice and move away from care based on ‘feeling rather than fact’ (Hospice Lead Nurse). Some rotation students came with a ‘thirst for knowledge that inspired, or almost re-motivated, the team’ (Lead Nurse). Another Ward Manager from a Cancer Unit provided an instance of one rotation student that was ‘experienced, calm, yet grasping opportunities that came her way’ who provided other members of staff ‘a good role model’. Also, newcomers to a centre from the cancer unit served to remind the former of difficulties encountered in caring for patients without the expertise available at the centre. The same Lead Nurse explained that the intensive nursing care that is part of everyday work in a centre is far from normal in a cancer unit where a person requiring such support might normally be in HDU. She suggested that such understanding made staff in the centre more understanding of referrals made to them when the level of care needed exceeded what units felt able to provide. This can only enhance common understanding of how care can be provided across the network. She stated that this ‘woke a lot of people up, and unsettled others.’ Bringing valuable skills Personnel from different areas brought a range of skills that often were unavailable to the ward team. For example those that came from haematology were able to take blood and cannulate. These skills were deemed useful transferable skills to own, which made them valued new members of the team. Nurses rotating to the community were valued for the up to date cancer nursing knowledge they were willing to share with the District Nursing team who were able to ‘pick their brains’ (PCT Lead Nurse). One rotation student had recently completed the chemotherapy course and gave a teaching session to the

47
community team on the topic. Similarly, those with community experience made particular contributions when ward-based during discharge planning, and individuals with palliative care skills were perceived as adding particular value in acute cancer settings. If the nurse rotating to the new clinical setting was relatively ‘confident, competent and senior’, the benefits for the host clinical area were perceived as greater. Flexibility was another characteristic identified as helping individuals to integrate and settle into the host nursing team. It appeared that ‘mature individuals integrated well’ over those more newly registered. One newly qualified nurse allocated to a hospice ward appeared to find the placement ‘overwhelming’(Hospice-based practice development nurse). Individuals needed to have enough confidence in their own knowledge to fit in easily’ (Hospice ward manager). Raising the profile of cancer and palliative nursing Stakeholders did identify the impact of the rotation on the profile of cancer nursing. It was perceived that it raised its profile and promoted it as a ‘possible career choice.’ Furthermore, it illustrated how it is possible ‘to develop skills and progress in a (cancer nursing) career in different ways… need to be flexible … (the rotation) shows nurses working in different organisations which lead to a roundness in their experience’ (Cancer Unit Lead Nurse). The rotation was perceived as an innovative approach to developing cancer and palliative care nurses with a ‘roundness’ and depth of experience. The hospice-based ward manager perceived benefits from the Rotation project for the palliative nursing profession. It fitted the ‘philosophy’ of their organisation… trying to spread the word. We invest a lot of financial and personal energy (in this), we have a national and international responsibility (to raise its profile, and enhance understanding of the hospice’s work). It’s not just here…’ The Lead Nurse for the PCT that was involved in the rotation also asserted that their involvement in the rotation initiative had raised their profile over other PCTs. Change catalysts Stakeholders were able to identify changes in practice that arose from rotation students locating to their clinical settings. A hospice-based Practice Development nurse referred to the competency document they had developed for newly qualified nursing staff from the one used on the Rotation. A ward manager at a different hospice had used the competency document to assist their development of a Learning Needs Programme for new members of staff. Another nurse, a manager from a Day Unit in the Cancer Centre, explained how nurses in their team had to hone their teaching skills through having a rotation student on placement. This particular Day Unit did not usually have students on placement and were not regularly engaged with teaching other staff members. The increased emphasis on teaching and revision of skills needed to educate and support the student were seen as advantageous and an opportunity to be capitalised on.

48
However, not only did the Rotation project contribute to local changes in practice, it also played a role in national initiatives through dissemination of the Competency Document. The Network Lead was chairing a subgroup guiding the development of National Competencies for cancer and palliative nursing care, and used the SELCN document as a ‘template’. Furthermore, the Network Lead having left her post continues to use the SELCN Competency Document to inform debate about the use of competencies in another area of the country. As she stated, ‘it’s better not to re-invent the wheel.’ Culture shock Ward managers and Lead Nurses did allude to the stress for both them and the student when the latter rotated to their area, particularly if they came from a very different clinical area. Some students tended to have anxieties over being somewhere new and ‘I needed to constantly reiterate things… (explain) that the ward was busy, stressful, might feel messy… some students found it difficult despite these reassurances.’ (Ward manager cancer care). Such individuals were perceived as rather needy. Community nurses on the rotation were singled out as a group for whom transfer to an acute ward environment posed particular challenges. It was perceived that they were ‘used to working at a different pace’ compared to that in acute cancer services in a busy hospital. Furthermore they were used to working in ‘an established team’ different from that of a ward where ‘most nurses were under 25 years’. These differences were conceived as a ‘culture shock’. (Ward manager cancer care). In fact many stakeholders referred to the ‘shock’ they perceived community nurses experienced when returning to acute ward settings. Admiration was voiced at their decision to undertake the rotation given this change to acute work. One ward manager from a cancer centre said ‘All credit to her. She worked like a Trojan.’ This view was reiterated by one Lead Nurse who stated, ‘Hats off to them!’ However, she did also fear that for some the learning curve was ‘far too steep’. ‘In some respects having students from the community didn’t work (because of these challenges)’ (Ward manager cancer care). This had repercussions for the ward team, as exemplified by the following comment made by a ward manager from a cancer unit ‘it was unfair on her and my staff… whilst it’s all very good on paper… (should try not to) expose this much stress and pain to anyone in future.’ The support provided to community nurses rotating to acute care was perceived as important. Not least as the hospital-based hosts had their ‘eyes fully open’ from the outset. As one Cancer Unit Lead Nurse explained: ‘(we knew) that they would have relevant community experience but may have problems in transferring to acute care.’ In their setting they perceived that ‘some members of staff may not have been fully supportive of this and did not enter (the initiative) in the spirit in which it was intended.’ Conversely, it appeared relatively easy for rotation students to adapt to community nursing where managers commented that students were ‘absolutely fantastic… they all settled in well and took on the responsibility of a team member’ (District nursing Sister).
49
Hospice-based stakeholders described the potential for difficulties when rotation students new to palliative care rotated to the hospice. One person explained ‘It’s not everyone’s bag (palliative care nursing)… how hospices handle things can be difficult… you minimise death in acute trusts; you maximise death in the hospice… perhaps you need some middle ground.’(Hospice Lead Nurse). It was also perceived as difficult for rotation students to settle in if they came from outside the home trust, as not only was there a new clinical area to understand, but also a new organisation. It was questioned whether those recruited to the SELCN at the start of the programme were as committed to the Rotation initiative as those already within the network. Those from within the network prior to the programme were likely to have had a better understanding of its aims and structure and furthermore were likely to stay within the network on completion (Network Lead). These factors may have accounted for their apparently relatively greater drive to get as much out the initiative as possible. Balancing act From a management perspective it was not always easy to ‘lose a member of staff who knows the ward routine and what is known of them’ to the rotation project. (Ward manager cancer care). Not least as they realised that the individual may not be replaced, and where they were it could be with a ‘highly competent but inexperienced D-grade’ (Day Unit Manager Cancer Centre). It was recognised that ‘you have to take what you get and work with it,’ but that on a small unit the skill mix was very important with individual capacity and attitude impacting widely on the entire team (hospice-based Practice Development Nurse). Many ward managers voiced great concern over finding sufficient time to educate the students satisfactorily. Although they conceded that this was a pressure that was not unique to their setting or the Rotation Programme. One ward manager from a cancer unit conceded that whilst she recognised and accepted that the unit had ‘obligations to the network… (the) DGH doesn’t want to bear that… (it’s)not interested in training cancer nurses for the NHS’. She stressed the need for funding which would allow students ‘time to adjust and experience (the placement)… otherwise (they) might as well sign up with an agency for long term placements with different environments…’ Further difficulty arose in community placements where it became evident that some District Nursing teams were providing care to few patients with cancer. This meant that students hosted in such areas were unlikely to gain the experience required. In light of this, one student was moved between teams to counteract this. However, as the PCT Lead Nurse explained, the learning environment and profile of patients being cared for is necessarily less predictable in the community than in acute cancer or hospice settings, rendering their involvement with the rotation problematic. The balance between cancer and other nursing care being provided by the district teams was difficult to gauge or predict. A balance had to be struck between the educational/experiential needs of the rotation student and the needs of other staff members or of patients. The rotation required students to leave the clinical area to visit areas of interest but this left some managers questioning ‘who will look after patients on the ward? They

50
easily recognised the benefits for the individual and the ward team of facilitating this process. Although it left the team ‘short on numbers’ it did contribute to the ‘knowledge base’ available to the entire team and ‘enhance team-working’ as the new recruit would meet members of the wider team caring for their patients and become integrated more quickly into the department (Day Unit Manager in Cancer Centre). Although they wanted to give opportunities to the rotation students, managers lamented that there was a difficult balance between letting this cohort of students see things and learn about them against the needs of ward staff as a whole. ‘Everyone should get these (learning) opportunities. The rotation people got preference because of the competency document, they needed to see ultrasound, they needed to see… But others (staff members) didn’t necessarily get a chance.’ (Ward manager cancer care). Some compensation was gained from having rotation students as ‘at least some members of staff get these opportunities.’ However, concerns over parity were very real and, for many, unsolved. Staffing Some stakeholders alluded to the impact of staffing levels on the area’s ability to support rotation students. Where staffing levels were low in some acute settings it was problematic trying to provide the level of support needed by rotation students when trying to deliver a service at the same time. Once again, there was a balance but this time between individual and service needs. One Lead Nurse commented that some students found it difficult being part of the staff compliment rather than supernumerary. This was perceived as particularly difficult for those not used to acute services but being rotated to them. It was stated that if vacant nursing posts within the team were filled then provision of support and tailoring of learning and placement to individuals need could be optimised. Whilst they strove to tailor the experience this became difficult when poor staffing precluded it. This view was supported by a hospice ward manager who explained that they ‘can absorb new staff more easily (than other clinical placements) as their pace of work was different and they had more staff than an NHS ward’. They also saw that this enabled them to establish and share good multidicsiplnary team working, and provide optimal nursing care… which drives (students) to see that it can be done… (an insight) they take with them. Students were ‘included in the numbers despite not having the (required) skills (Day Unit Manager). This meant that many students were ‘thrown in at the deep end’ and had to ‘hit the ground running’. They had to quickly pick up new skills to allow them to integrate quickly into the nursing team; there was little, if any supernumerary period available to students and the nursing management. As a consequence, it was difficult for managers to ease the pressure of rotation students with limited required skills, entering busy clinical settings that often had low staffing levels.
51
Documentation The host managers and staff initially conceived the competency document as rather overwhelming. It was difficult for them to ‘get their heads around what they were supposed to do.’ It was also seen as a big investment of time and effort for students, but all had managed it despite this. And it was recognised by host staff that it did build up a personal body of evidence and collection of experience that was personally relevant. It was seen as a ‘practical way to understand issues and develop learning’ that did require rotation participants to apply themselves; ‘to learn you need to apply yourself a lot. If you don’t apply yourself you won’t learn…’ (Unit Lead Nurse). The competency document was perceived as a vehicle for guiding application of individuals’ effort. Headaches Stakeholders were asked to reflect on any headaches associated with the programme. Responses included (it is difficult to) ‘adapt staff from other areas’ (ward manager cancer care). As with all staff development, this can be especially difficult where students are not ‘forthcoming’ which can lead the team seeing it as a ‘burden’ rather than an ‘opportunity to pass on skills and knowledge’ (Network Lead). Both the Network Lead and a Centre Lead Nurse alluded to the financial difficulties that the Rotation Project posed. The Lead Nurse explained that the ‘financial arrangements were the first thing that pop into her head when asked about the rotation – the nightmare finances!’ This related to difficulties in recouping salaries paid. At one point the particular trust was in ‘a lot of debt’, largely as financial departments found it difficult to grasp the process of paying out and recouping funds. Stakeholders in the community raised difficulties that arose when students were unable to drive. A lot of nursing provided in the community requires travelling between patients that in many cases becomes easier when travelling by car. This also raised issues over the organisation that would pay for the students mileage. However, this was resolved. The Network Lead summarised the importance of institutional flexibility in resolving many of the headaches that were encountered by participating organisations. She explained that a ‘degree of organisational flexibility … and (being able to) think outside the box’ were needed to work through these.’ Financial constraints within an organisation were compounded when a member of staff from a clinical area left it to join the Rotation but was not replaced necessitating payment of agency cover in addition to the member of staff’s salary costs. However, this lead nurse did also identify that on the following rotation they gained where previously they had lost out, as later they had two members of the rotation allocated to them. Reference was also made to difficulties in attaining health clearance for people rotating to an area. This meant that there was a potential for incoming members of staff being unable to start work at the correct time. A further stakeholder stated that for them the greatest headache had been the ‘rumblings and mutterings’ from discontented staff about the Rotation that served to undermine the initiative.

52
Rewards Stakeholders were asked to reflect on any rewards associated with the programme. Responses included: ‘Having people with different experience coming through, and back (students returning to original workplace following the rotation) (Ward manager cancer care). It was recognised how pleasing it was seeing people who had been on the rotation doing so well following it, perhaps moving on to better jobs. ‘You helped some people to move along’ (Lead Nurse). Further understanding of this perceived reward was provided by the Manager of a Day Unit in the Cancer Centre who said, ‘… (the student) did learn so much and flourish in the area…’ Enjoyment at seeing students flourish in the host setting was also alluded to by stakeholders in the community ‘It was really nice to see them (students) develop in the community team, and enjoy it’ (District Nursing Sister). The Network Lead provided a different, and wider, perspective of the contribution made by the programme. She explained that for her the initiative had been ‘about working together’. She explained that the Rotation showed how ‘a lot of different organisations can work together as a united team’. She conceded that including primary care in the initiative had been complicated but valuable, ‘contributing to strengthened relationships across the whole patch.’ Another stakeholder iterated that the Rotation had been about ‘Linking people at the coalface’ (Unit Lead Cancer Nurse). This individual included academic partners at the ‘coalface’ and stated the initiative enhanced links between academic and clinical partners in the SELCN. Involvement with the programme Some stakeholders (notably ward managers) noted they had not been very involved with the development of the project but did feel appraised of its aims and progress. ‘It is a bit of an unknown entity… (I) understand the principles but not the detail’ (Hospice Ward Manager). The LPs were identified as key to their being informed of changes and progress with the rotation. One individual stated that they had a good relationship with the LP that ‘made a heap of difference’. They were commonsense, supportive… had candid discussions about students. We worked well together.’ (hospice-based Practice Development Nurse). The general view was that ‘you could be as involved as you wanted to be’, and ‘in appropriate areas’ (Network Lead). The organising team were ‘open for people to be involved’. The programme itself was perceived as being developed ‘close to the ground’ (hospice-based Practice Development Nurse). Despite this, any well conceived projects will have teething problems. One ward manager explained that their Lead Nurse had represented them but was ‘not on the factory floor’. Thus, ‘gaps had arisen’, but were identified with the LPs and ‘sorted out’. The links provided by the LPs were perceived by clinical hosts as ‘vital. They kept the organisations and wards abreast of progress and were efficient at quickly updating new areas as to what was involved. It appeared that without their support ‘the programme would not have happened’ (Cancer Unit Lead Nurse).

53
Happy endings Some stakeholders could provide examples of the benefit derived by individuals that had taken part in the Rotation. They could see that when a nurse returned to their clinical area, having completed the programme, they returned more confident. Perhaps as ‘they had seen the whole cancer picture… (and had) greater understanding (Ward manager cancer care). Another stakeholder referred to the evident progress made by a member of staff returning to their clinical workplace with a ‘wider appraisal and understanding of the acute sector’ who was promoted to a Junior Sister position (Hospice-based practice development nurse). The same individual noted that freeing people to undertake the rotation had associated risk; based on their experience the student may decide to work elsewhere on completion of the project. However, this risk was perceived more a ‘consideration’ than a ‘stopping factor’. The potential benefits outweighed the risk. One example of where the benefits had certainly outweighed the difficulties relates to a community nurse on the programme who had not found transition to acute services easy. However, a Lead Nurse from the Cancer Unit explained how the time invested in them had paid off as they retained their interest in cancer nursing on return to the community and is working to enhance cancer nursing in the community. This individual, referred to as a ‘great resource for the community’, is now intending to further develop their cancer nursing skills so that they may become a designated nurse within the district nursing team with advanced skills in cancer care. The manager of a Day Unit in the Cancer Centre explained, ‘It couldn’t have worked out better. (The student) was motivated, enthusiastic, great fun, threw themselves in and was popular with the patients, nursing team and whole department and taught us heaps too! We also established links with X Trust where they had been based and where a lot of our patients come from. The link remains…’ District nursing teams also identified benefits from having staff members that rotated from the local cancer unit or hospice to their community-based teams. ‘A lot of them (rotation students) had had contact with the ward at X hospital and knew who we could speak to if we had a problem… (we have got) a better understanding of how the wards work, particularly X (the oncology) ward.’ (District Nursing Sister). The future Stakeholders were generally positive about the Rotation and expressed their ongoing support of it. ‘It is good for the unit to be part of the rotation. It helps growth and development both of the individual and the ward.’ (Ward manager cancer care). This view was voiced by a Hospice Ward Manager who explained that in ‘the long term it is fantastic what the student (that participates in the programme) will bring back… well beyond what you are losing (when they join it)…. The same manager added that participation in the programme helped her hospice to ‘keep linked in with the NHS’. The only area where some uncertainty was voiced about the future of the rotation was within the community. The PCT Lead reflected that there had been

54
difficulties associated with their involvement and determined that they would ‘need to look long and hard’ before committing themselves in the future. A word of caution was provided by one stakeholder who was concerned that the thrust of the programme had changed from enhancing the education of the future workforce to alleviating staffing problems. The second rotation had been used to advertise and fill job vacancies. This individual worried whether this shift in perspective could ‘compromise the education of the future workforce for difficulties of today’ (Hospice Lead Nurse). This individual voiced strongly that they did not wish to see the rotation compromised through priority shifting from education to combating service shortfalls. Overall, feedback from stakeholders about the rotation was positive; most individuals enthused about its future potential. At a network level, the Network Lead suggested that it provided ‘an excellent way of increasing skills across different areas’. She added, ‘I definitely think it should continue… a lot of hard work has been put in, it would be a shame not to… shame if the trail blazing stopped there.’ Recommendations Recommendations made by stakeholders for future rotations varied in scale from micro to macro issues. Academic workload. On a micro scale reference was made, predominantly by nurse managers, to the timing and requirements of academic courses that students were expected to undertake. A District Nursing Sister suggested that ‘the workload of the competency document and academic courses appeared at times excessive.’ In recognition of this, one ward manager from a cancer unit made a similar suggestion to participants themselves regarding the academic credit ascribed to the academic portfolio. She had discussed this with her member of staff on the rotation and perceived that there had been ‘limited academic reward… for the pain (of participation). She recommended increasing the credit for completing the portfolio. A further issue related to the timing of courses provided by the academic partner. A District Nursing Sister mentioned one student in the community who was ‘meant to be doing the chemo course during their community experience, (which would have) detracted but was cancelled in the end’. The same District Nursing Sister alluded to particular difficulties towards the end of the course where (students) were getting a bit bogged down (in completing academic requirements alongside clinical ones). Structure of rotation. On a wider scale, many recommendations that were made by stakeholders related to the structure of the rotation itself. These included restricting the rotation to a smaller geographical area. The SELCN was regarded by some stakeholders as a large area that required individuals to rotate between organisations and clinical areas. This could be achieved in different ways. First, by restricting the rotation to one Trust, the perceived difficulties that arose when people moved between organisations would be removed. Second, a Lead Nurse conceived that with more Trusts becoming involved, individuals would not need to rotate over such a wide geographical area but be able to do a local rotation yet

55
‘see the ideals (rotating between centre, unit and palliative care) that were had at the beginning coming to fruition’ (Lead Nurse). The Network Lead suggested that differing levels of rotation could hold value, not least as ‘some people might be put off by the academic and time commitment needed (for the current rotation), but who may want something - a flavour… it might then encourage them to do more…’ She suggested a 4-tier approach. The first being a programme provided at a local level, which could incorporate week-long rotations through the local centre or unit, one hospice and a Primary Care Trust, with a basic range of competencies to fulfil. She then suggested two further tiers with longer placements, possibly 1- and 3-months, with associated academic support and competency attainment. The fourth level she termed ‘the ultimate’ level which is fulfilled by the current programme that ‘allows time to consolidate skills and opportunity to learn advanced skills … in the real world…to compliment (their ongoing) learning’. She conceived of this tiered approach as a ‘sliding scale’ where individuals could select a Rotation according to the requirements of their workplace and their previous experience of caring for people with cancer. Recruitment. Stakeholders commented on the type of individual that adapts to, and gets the most out of, the Rotation initiative. To summarise these are mature, flexible individuals with confidence in their cancer and general nursing skills. They tended to be personnel working within the SELCN, with an apparent intent on continuing to work within it. Feedback from stakeholders suggest that to ensure success, these characteristics should be borne in mind when recruiting individuals to the programme. Parity within clinical nursing team. One ward manager wished to make learning opportunities more equal across staff members in future rotations. Presumably this would curb any feelings of favouritism shown to those on the Rotation. She recognised that she ‘should perhaps look at how she could make sure others do also get similar learning opportunities. (Ward manager cancer care). A Lead Nurse at one of the Cancer Units referred to inequality in provision of LP support. During the Rotation a LP had been ‘available and visible in the clinical area’ which hitherto had not been the case. This led to a degree of frustration for the clinical team with realisation that this would later be withdrawn. This created tension with the awareness of the differing resources, and availability of LP support, in a large teaching hospital versus their District General Hospital. Skill revision. A Lead Nurse voiced concerns over rotation between acute settings and other working environments (notably community). Whilst it was seen as important to involve community teams in the initiative this individual reflected on the value of having a ‘back to basics update on clinical skills’ for community nurses prior to their returning to an acute ward environment. Similarly, she suggested that an induction for those moving to unknown community environments may also facilitate their speedy uptake of a different style of nursing care. Reflexivity within host organisations. A hospice-based Practice Development nurse emphasised the need for organisations to rise to the challenge of hosting

56
Rotation Students, and foster changes in accordance with their feedback. She explained, ‘…individuals can learn but are institutions? Some (students) talk of poor skill mix – pretty terrible experiences. They (Rotation students) have fresh eyes, (institutions) need to listen and affect policy to enhance experiences. If students raise issues they should look to their practice for example by asking, How good are you at providing care once treatment is finished? It appeared to hinge on ‘What will organisations be willing to learn?’ From this comment it appears that the students could act as greater catalysts of change where institutions are open to questioning and change. Financial constraints. Recommendations were made to lessen the financial constraints referred to in the Headaches section. The Network Lead suggested that attempt should continue to be made to involve the Workforce Confederation. She spoke of ‘embracing Directors of Nursing… (to have) champions in organisations… selling the benefits (of the Rotation) to other students… cancer is one cohort, but the skills - communication, assessing, team working - are transferable.’ Opening up the debate. One Lead Nurse from a Cancer Unit reiterated that on balance they had a positive view of the Rotation Project. However, they recognised that for its ‘sustainability and development it was important to widen the debate to all stakeholders once the evidence (from its evaluation) was available’. They recognised that it was not possible to ‘take it forward in isolation’ or reflect on whether it was the best way to develop cancer and palliative nursing skills without such debate. They stated that ‘although it could be one way of developing nurses for the future, there are other possibilities for developing them… (such) debate is healthy and should include Nurse Directors and the Workforce Confederation. The rotation required considerable effort from stakeholders to work across institutions to get the Rotation project off the ground. However, through their collaborative and sustained effort the project came to fruition and although they met challenges on the way they identified the many fruits of their labours during this component of the evaluation. As one stakeholder summarised: It represents a ‘great opportunity. It has inherent risks, but I’m glad we’ve done it’ (Cancer Unit Lead Nurse).
57
DISCUSSSION
This was an ambitious project in terms of its objectives. The project set out to establish, deliver and evaluate a career development rotation programme within the field of cancer and palliative care across a cancer network. The novel element of this project involved engaging stakeholders across the cancer network from both the statutory and voluntary sector, involving care providers in the primary, secondary and tertiary sectors. It was executed as a partnership between education and service providers. The evaluation incorporated a number of different approaches including focus groups, telephone interviews and structured questionnaires and included rotation participants, stakeholders and the LPs. It was both process and outcome orientated. The rotation programme represents a significant step forward in working towards the network’s ambition of developing a managed cancer nursing network. Such a network will be contingent on the provision of cancer nursing expertise. The contribution of rotation programmes to the career path of those working in cancer and palliative care was recently acknowledged in the document ‘A Strategy for Cancer and Palliative Care Adult Nursing Across London 2003-2006’. The desire to develop and evaluate rotation programmes, where nurses can gain experience in different care settings, was underlined in this strategy. To date robust career pathways in cancer nursing remain elusive, and it was perhaps naive to expect that this project would have a major impact in this area in the short time it has been in operation. It has, however, raised debate, both within the network, and across London and has been referred to as an exemplar in papers produced by the Cancer Nursing Advisory Group (under the auspices of the Department of Health). The notion of what a managed career pathway in cancer nursing would look like and some of the ways in which this vision might be achieved have become much clearer in the last 12-18 months. On an individual participant basis it is clear from the evaluation data that the programme was successful in its aim to develop a mechanism to equip them to work as competent cancer or palliative care nurses. A consistent theme to emerge was that it was felt to be a valuable learning experience and through which they felt more equipped and confident to care for patients at any point along the cancer pathway. The programme represents a viable option for those who wish to familiarise themselves with a variety of different care contexts in a relatively short period of time. We are now able to predict with some confidence the characteristics of nurses most likely to reap benefit from this type of programme and those most likely to be perturbed and less likely to accommodate the various challenges confronted whilst moving from one setting to another, simultaneously carrying a demanding course assessment workload. It was an ambition that the rotations for individual nurses would be tailored as much as possible to their career aspirations. Moreover, clinical learning opportunities would accommodate students’ desires to be exposed to different aspects of care provision. A large portfolio of clinical learning opportunities were made available, but sometimes compromises had to be made. This was due in large part to the necessity to overcome the operational challenges inherent in the rotation, sometimes these had to assume more importance than meeting individual students wishes. On the whole however, students who undertook the

58
rotation were exposed to infinitely more choice in terms of learning opportunities than those who undertook a conventional educational programme. The rotation aimed to produce rounded individuals who could work across a variety of different contexts, and the generic, rather than specialist experience they gained made a major contribution here. To this end it succeeded. Finally, the project had as one of its objectives to build on existing relationships between clinical and education providers. This was achieved with some measure of success. There was significant interchange between the lecturer/practitioners employed to facilitate the rotation and the clinical stakeholders who provided both students and placements. The project served to draw in an eclectic group of stakeholders, and at a time when the cancer network was in its relative infancy, served as a model in how to achieve objectives in the light of often severe operational and strategic constraints. It illustrated how a large number of organisations could work across the locality as a united team. Unexpected achievements There were in addition to the original objectives a number of unexpected benefits that resulted from the project. Most striking was the impact of the programme, both directly and indirectly, within both the academic and clinical setting. A commonly voiced view was the way in which rotation participants brought a ‘fresh pair of eyes’ to a clinical area and often acted as catalysts for change. They challenged existing practice, often brought about change and enhanced clinicians’ knowledge base. The LPs, with their unique perspective of the network, were able to influence the portfolio of clinically relevant educational provision. Their expertise was in great demand, particularly with respect to designing assessment schemes with the ability to capture clinical competence. The relevance of the portfolio and competency-based approach to learning was recognised by the wider teaching team within the School of Nursing and incorporated as an approach into a number of clinically focussed courses. They were able to enhance the links between other cancer and palliative care lecturers in the School and the various clinical sites, as one stakeholder commented ‘linking people at the coalface’ both in education and practice. The competency assessment tool developed during the course of the project has influenced the national cancer nursing competency project that is currently being driven forward by the Department of Health. The LPs contributed to a number of working groups, and learning accumulated in developing the assessment procedures and the accompanying portfolio had been fed in. The opportunity to run two rotations, of different lengths and with cohorts recruited from either within or external to the network provided the opportunity to learn about the advantages and disadvantages of these two different approaches. During the course of the project the core team became aware of a number of other rotation initiatives around the country. A seminar was organised to share learning and identify features critical for success. This event served to pool expertise and as a result a paper has recently been published to enable the proceedings to reach a larger audience (Johnson et al. 2003).

59
Benefits relative to costs The main costs for this project were the salary costs of the two LPs. These posts were critical to the success of the project and this was underlined by comments received from stakeholders and students alike. They were the lynch pin for much of the development work needed to establish the rotation and took a primary role in ensuring structures and processes were in place to secure day to day running of the programme. And whilst the development work undertaken for this project was costly, the costs of maintaining the system now it has been established are significantly less. If the number of students to benefit is taken as a primary measure of benefit the project incurred high costs relative to benefit. There were however a significant number of wider benefits to the organisations involved and the network as a whole. These included the influence of participants on the practice areas where they were placed, gains made with respect to cross-organisational working (between different services and between education and practice) and the collaborative spirit fostered across the network. The participants who accessed the programme from within the network have on the whole remained within the network and many achieved promotion either during or on completion of their rotation. Factors contributing to success There were a number of different factors that contributed to the success of this project. The LPs through their skill and commitment were significant drivers for change and served to link the many disparate elements of the project together. In particular, the time they spent first preparing and then maintaining the commitment of the clinical areas was fundamental to the sustainability of the initiative. The support and supervision they offered the rotation nurses was very well received and there was overwhelming praise for the contribution they had made to the working and learning experience. The diversity of clinical areas included in the rotation meant the LPs were essential to ensuring a consistent high quality learning experience. The stakeholders demonstrated a commitment to the ideals of the project and were willing to think flexibly to achieve desired outcomes. In part this could be attributed to the manner in which the project was conceived and the ground work undertaken early on to develop a proposal that met diverse, and at times, conflicting needs. There was willingness on the part of all concerned to think ‘out side the box’ and try new ways of working to reach a common goal. There was a sense, for both individual students and the organisations themselves, of learning through the process. Shared ownership was perceived to operate at every level. Factors inhibiting success The pick up of participants was lower than expected. It had been anticipated that a total cohort of up to 20 students would be enrolled on the programme. In the event two cohorts were enrolled, 8 on an 18-month programme, the remainder (5) on a 12- month programme. Whilst it was disappointing that maximum numbers were not reached difficulties in the sector with respect to recruitment and retention generally contributed to this. The fact that the programme was highly innovative and involved a certain amount of risk on the part of the participants who had to up root from their current clinical area for a significant period of time was also a factor. For a workforce that is predominately female this had potential to pose a number of challenges, balancing work, home and

60
academic commitments. One of the early challenges recognised by both students and stakeholders was the energy required to adapt to working and caring for patients in different settings. The wide geographical spread of the network did impact on rotation opportunities and led to issues around travel to work which were a recurrent concern. Restrictions to the rotation pattern for individuals developed with the 2nd programme, paying more attention to individual rotations with geographically adjacent placements. This was based on learning that occurred during the first programme. The challenges of living and working in the capital and having to rely on public transport were clearly lived out in the project, and serve to highlight some of the specific issues experienced by health care organisations with regard to recruitment and retention. A positive outcome of experimenting with the format (12 versus 18 months) and number of participants (8 versus 5), based on experiences with the two rotations is that we have been able to develop a ‘model’ programme. This is sustainable within current resources (and based on numbers of rotation students that can be facilitated by the network at any point in time), without unduly compromising the learning experiences of individual students or placing undue burden on clinical areas.

61
CONCLUSION Rotational training programmes are well established in medicine but there are few working examples of such programmes in nursing generally, or cancer and palliative care specifically. They are seen as a method to enhance recruitment and retention and demonstrate commitment to professional development. Whilst we are aware a number of organisations have developed internal rotation programmes, we believe this one to be unique as it involved all the care providers in the network, both statutory and voluntary.The rotational idea incorporated a number of themes: clinical skills development, academic input, supervision and support, professional development and reward and incentives. The various stakeholders worked together over a period of 2 years within the context of a cancer network to develop, deliver and evaluate the programme aimed at nurses wishing to develop the knowledge and skills necessary to care for a patient with cancer over the course of their cancer journey. The aims of the project were largely met and its success is clear: it provided an opportunity for junior nurses to improve their clinical skills, develop academically and network with individuals, teams and organisations across the local cancer network. The organisation of cancer care has changed dramatically over the last ten years and working to raise the quality of cancer care across an entire network is a key political priority. One important route to enhancing care is through the provision of education and training. Up until this point this has rarely been attempted on a network basis. This project represents an example of how this might be achieved in relation to a particular group of staff. This innovative approach to supporting the development of clinical skills and knowledge also served to challenge practice in individual organisations and brought clinical and educational colleagues together for mutual gain. But most important it was seen as an invaluable learning experience with the capability to produce confident and competent nurses able to care for patients with cancer in different care contexts. It represents a positive practice example in developing the cancer care workforce.

62
REFERENCES Watson R Porock, D Topping, A (2003) Evaluation of the effectiveness of educational preparation for cancer nursing and palliative care. Unpublished report of research commissioned by the English National Board for Nursing, Midwifery and Health Visiting. Department of Health 2000a The NHS Cancer Plan. A plan for investment. A plan for reform. Department of Health, London. Department of Health 2000b The Nursing Contribution to Cancer Care. A strategic programme of action in support of the national cancer programme. HMSO, London Langton,H Blunden,G Hek,G 1999 Cancer nursing education: literature review and documentary analysis. English National Board for Nursing, Midwifery and Health Visiting. Cancer Research Campaign, King’s Fund. Macmillan Cancer Relief 1997 The workforce and training implications of the Calman-Hine cancer report. The Cancer Collaboration. Cancer Nursing Advisory Group 2003 Managed career and training pathway. Meeting the needs of cancer patients. Unpublished. Johnson, M., Menon, A., Richardson,A. (2003). Establishing clinical rotation programmes in cancer and palliative care nursing. Cancer Nursing Practice, 3(1): 29-34. Royal College of Nursing 2003 A framework for adult cancer nursing. RCN, London
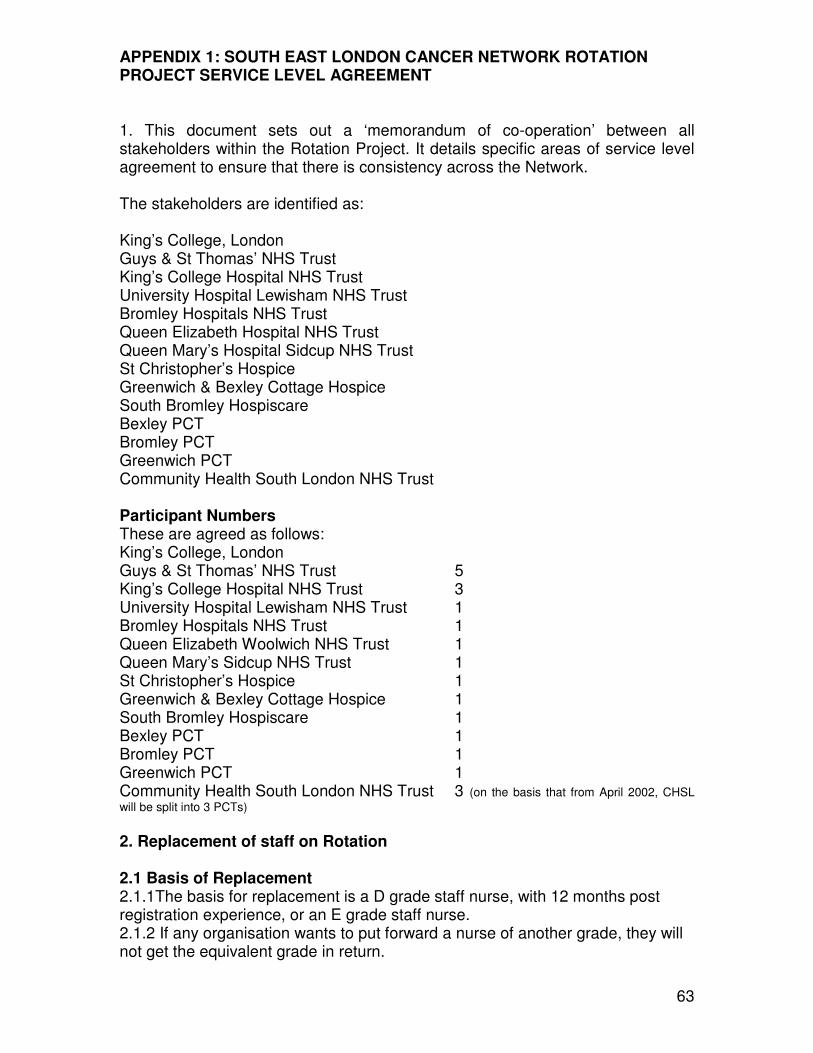
63
APPENDIX 1: SOUTH EAST LONDON CANCER NETWORK ROTATION PROJECT SERVICE LEVEL AGREEMENT 1. This document sets out a ‘memorandum of co-operation’ between all stakeholders within the Rotation Project. It details specific areas of service level agreement to ensure that there is consistency across the Network.
The stakeholders are identified as:
King’s College, London Guys & St Thomas’ NHS Trust King’s College Hospital NHS Trust University Hospital Lewisham NHS Trust Bromley Hospitals NHS Trust Queen Elizabeth Hospital NHS Trust Queen Mary’s Hospital Sidcup NHS Trust St Christopher’s Hospice Greenwich & Bexley Cottage Hospice South Bromley Hospiscare Bexley PCT Bromley PCT Greenwich PCT Community Health South London NHS Trust Participant Numbers These are agreed as follows: King’s College, London Guys & St Thomas’ NHS Trust 5 King’s College Hospital NHS Trust 3 University Hospital Lewisham NHS Trust 1 Bromley Hospitals NHS Trust 1 Queen Elizabeth Woolwich NHS Trust 1 Queen Mary’s Sidcup NHS Trust 1 St Christopher’s Hospice 1 Greenwich & Bexley Cottage Hospice 1 South Bromley Hospiscare 1 Bexley PCT 1 Bromley PCT 1 Greenwich PCT 1 Community Health South London NHS Trust 3 (on the basis that from April 2002, CHSL
will be split into 3 PCTs)
2. Replacement of staff on Rotation 2.1 Basis of Replacement 2.1.1The basis for replacement is a D grade staff nurse, with 12 months post registration experience, or an E grade staff nurse. 2.1.2 If any organisation wants to put forward a nurse of another grade, they will not get the equivalent grade in return.

64
2.2 Placement 2.2.1 A matrix of placement availability sets the format for allocating placements. 2.2.2 Each placement will be for 6 months. 2.2.3 Released staff from one organisation will be filled with released staff from another organisation. 2.2.4 Host organisations will look at ways in which they can facilitate the participants’ learning needs across the organisation, to reflect the requirements of the practice portfolio. 2.2.5 If a stakeholder does not want to use their place then it can be out into a ‘central’ bank for another organisation to use. 2.2.6 One of the placements will be in the employing organisation. 2.3 Contractual variations 2.3.1 These are honoured from employing organisations. 2.3.2 The host organisation is to provide a ‘letter of attachment’ to enable an individual to practice in another area. 2.4 Working patterns 2.4.1This is set 2.5 Identification 2.5.1 Participants will be issued a King’s College name badge and ID card. They will use their employing Trust’s uniform, unless the host organisation requires that they wear there’s. 2.6 Personal Training Days 2.6.1 Each participant will be required to complete a portfolio of clinical competencies as a minimum requirement. This will incur PTD costs. It is anticipated that this will lead to the award of 30 Level 2 or 3 credits. 2.6.2 Where participants access additional courses provided by King’s College London, the rotation nurses’ employer will be responsible for the PTD cost of the said courses. 2.7 Withdrawal from Project 2.7.1 1 months’ notice is required for withdrawal from the Rotation Project. 2.7.2 Prolonged, or frequent absence, will be referred to the employing Trust’s Occupational Health Service, to determine whether the participant is fit to continue on the project. 3. Leave 3.1 Participants are expected to comply with all of their contractual requirements with their employing Trust, with regard to maternity, paternity, adoption, sick, annual and compassionate leave. 3.2 The compulsory study leave requirement is 15 days, over the eighteen-month project, as set out by the College. The dates are 18-22 February and 29 April to 3 May 2002, inclusive. The third block of dates is to be confirmed. These days are mandatory at full-time.3.3 Participants will also be entitled to access a 15-credit course per semester. This is additional study to that set out in 3.2. 3.4 The LPs will verify and co-ordinate the recording of sickness, maternity leave and annual leave. It is their responsibility that the employing organisation is made

65
aware of the records on a regular basis. This is to ensure that accurate records are kept. 4. Remuneration 4.1 Travel costs 4.1.1 Participants are to pay their own costs, to and from any work base. 4.1.2 All participants should be willing and able to travel within the South East London Cancer Network area (LSL & BBG Health Authorities). 4.1.3 Remunerations will be made by the employing organisation. 4.2 Extra duty payments 4.2.1The LPs will verify & co-ordinate the recording of extra duties, and inform the employing organisation. 4.2.2 Payment is per normal practice of the employing organisation. 4.2.3 Participants will be expected to work an off duty, which reflects the host organisations’ normal working practice. 5. Disciplinary Procedures 5.1 Clinical disciplinary matters are to be investigated by the host organisation, and if warranted, action will be taken by the employing organisation. 6. Educational audits 6.1These are required from all participating organisations. 6.2 King’s College London recognises the validity of an audit undertaken by another educational establishment. Director of Nursing Director of Finance --------------------------- ----------------------------

66
APPENDIX 2: Cohort 1 Rotation Programme Participant Placement 1
25.02.02-18.08.02 Placement 2 19.08.02-23.02.03
Placement 3 24.02.03-24.08.03
1 (Centre 1)
Greenwich PCT
Greenwich & Bexley Cottage Hospice
Derek Mitchell Unit, King's College Hospital NHS Trust
Headley Atkins Unit, Guy's & St Thomas' NHS Trust
2* (Unit 1) Greenwich & Bexley Cottage Hospice
Greenwich PCT
Stanley ward, Guy's & St Thomas' NHS Trust
Macmillan Brook Unit, Queen Elizabeth Hospital
3 (Centre 2)
Headley Atkins Unit, Guy's & St Thomas' NHS Trust
Greenwich & Bexley Cottage Hospice
Greenwich PCT
Derek Mitchell Unit, King's College Hospital NHS Trust
4 (Unit 2) Stanley ward Greenwich PCT
Greenwich & Bexley Cottage Hospice
Gillies ward, Queen Mary’s Hospital NHS Trust
5 (Centre 1)
Gillies ward, Queen Mary’s Hospital NHS Trust
Withdrew
6 (Centre 1)
Stanley ward, Guy's & St Thomas' NHS Trust
Macmillan Brook Unit, Queen Elizabeth Hospital
St Christopher’s Hospice
Headley Atkins Unit, Guy's & St Thomas' NHS Trust
7 (Community)
Macmillan Brook Unit, Queen Elizabeth Hospital
Headley Atkins Unit, Guy's & St Thomas' NHS Trust
Greenwich & Bexley Cottage Hospice
Greenwich PCT
8 (Hospice)
Derek Mitchell Unit, King's College Hospital NHS Trust
Stanley ward, Guy's & St Thomas' NHS Trust
Greenwich PCT
Greenwich & Bexley Cottage Hospice
*withdrew during final placement

67
APPENDIX 3: Cohort 2 Rotation Programme Participant Placement 1
16.09.02-16.03.03 Placement 2 17.03.03-14.09.03
9 (Centre 1)
Samaritan ward, Guy's & St Thomas' NHS Trust
Greenwich & Bexley Cottage Hospice
10 (Centre 2)
Derek Mitchell Unit, King's College Hospital NHS Trust
Withdrew
11 (Hospice 1)
Greenwich & Bexley Cottage Hospice
Withdrew
12 (Hospice 2)
St Christopher’s Hospice Derek Mitchell Unit, King's College Hospital NHS Trust
13 (Unit 3)
Queen Mary’s Hospital NHS Trust
Stanley ward, Guy's & St Thomas' NHS Trust
Chartwell Unit, Princess Royal University Hospital

68
APPENDIX 4: Extract from competency document
3: Cancer Treatment
Practitioners are expected to gain experience of caring for patients undergoing all of the main cancer treatment modalities; surgery, radiotherapy and chemotherapy. They are also expected to gain some knowledge and experience of caring for patients receiving other forms of cancer treatment, such as immunotherapy, hormone therapy and biotherapies. Particular emphasis is placed on supportive strategies and information. 3.1 Academic assignment Level 2: Write a short paper outlining the main modes of action, indications and side effects of one cancer treatment modality given to a patient you have cared for. By conducting a taped patient interview, present a short analysis of the patient’s experience of this treatment modality, supporting your findings from the literature. (Guide 1200 words) Level 3: Critically evaluate the evidence base for one cancer nursing intervention used in relation to a side-effect that you have witnessed in a patient you have cared for in response to the administration of chemotherapy, radiotherapy, or a bio-therapy. (Guide 1500 words)

69
3.2 Essential experience and observation Visit to signed date Surgical outpatient clinic: Pre and postoperative patients.
Radiotherapy clinic: Pre-treatment, on-treatment and follow-up.
Radiotherapy planning.
CT radiotherapy planning.
Radiotherapy treatment room.
Chemotherapy clinic: Pre-treatment, on-treatment and follow-up.
Reconstitution of chemotherapy.
Day-unit Chemotherapy Department.
Research Trial Nurse.
Optional experience and observation ♦ Mould Room
♦ Brachytherapy
♦ Selectron
♦ Specialist nurses
♦ Community chemotherapy service
♦ Observation of cancer related surgical procedures

70
3.3
Specific Competency area:
Chemotherapy Evidence No.
Competency met (mentor)
Student Date
i. Gives appropriate, accurate and sensitive explanation of the mechanisms of chemotherapy treatment and its effect on cancer cells and the rest of the body to a patient, involving carers if appropriate.
ii. Provides appropriate verbal explanation and written material to a patient and their carers (if appropriate) regarding self care requirements following commencement of chemotherapy treatment; e.g. fluid intake, mouth care, early signs of infection, anti-emetic use.
iii. Anticipates the likely side effects of chemotherapy treatment and implements appropriate strategies for their prevention or management.
a. bone marrow depression b. nausea & vomiting c. extravasation d. alopecia e. stomatitis f. tumour lysis syndrome g. anaphylaxis
iv. Provides safe ongoing care for a patient receiving chemotherapy via a previously established administration route.
a. patency of access route b. infusional devices c. fluid and electrolyte balance
safe disposal of waste
v. Describes the different routes used to administer chemotherapy and is conversant with all policies and procedures necessary for its administration.
vi. Conversant with the Department of Health guidelines for the prescription, storage and administration of intrathecal drugs.
vii. Provides safe and appropriate care for a patient with bone marrow depression.

71
viii. Identifies the early signs of neutropenic sepsis and institutes appropriate urgent care.
ix. Provides a balanced and non-judgemental attitude to clinical trials and uses this to support patients in their decision making when considering entering a clinical trial.

72
3.4
Specific Competency area:
Radiotherapy Evidence No.
Competency met (mentor)
Student Date
i. Describes the different techniques employed to deliver radiation therapy, e.g. electron beam, mega-voltage, radical, palliative and brachytherapy.
ii. Gives an appropriate, accurate and sensitive explanation of the mechanism of radiotherapy treatment and the effect it has on the cancer and the rest of the body.
iii. Provides appropriate patient education regarding self-care whilst undergoing radiotherapy treatment to a patient and/or their carers.
a. skin care b. site specific alopecia c. dietary and fluid intake d. fatigue
iv. either:
Provides the specific information and advice required by a patient undergoing radiotherapy to the head & neck region.
a. stomatitis and mouth care b. dysphagia and nutritional support c. skin care d. communication problems e. body image concerns
iv. or:
Provides the specific information and advice required by a patient undergoing radiotherapy to the pelvic area.
a. skin care b. diarrhoea and dietary restrictions c. dysuria d. fertility and/or sexuality issues
v. Acts as the patient’s advocate in relation to appropriate timing, delivery and preparation for radiotherapy.
vi. Is aware of, and complies with, Local Rules for working with ionising radiation.

73
3.5
Specific Competency area:
Surgery Evidence No.
Competency met (mentor)
Student Date
i. Provides an appropriate, sensitive and accurate explanation to a patient and their carers due to undergo surgery for cancer.
ii. Provides pre-operative education to enable patient to minimise self care deficits following surgery.
iii. Delivers safe and comprehensive care to a patient in the immediate post operative period on return to the ward area with attention to:
a. haemodynamic monitoring b. fluid and nutritional requirements c. acute pain management d. general comfort e. wound management f. mobility needs
iv. Identifies immediate rehabilitation needs of a patient having undergone surgery for cancer and involves appropriate Specialist and Multidisciplinary Team members including prosthetic support, stoma care, or tracheal stoma care.
v. Discusses the principles of the staging system used for one common cancer and aware of the significance of histological findings.
vi. Addresses patient’s anxieties relating to receiving or waiting for histological findings following surgery.
vii. Provides suitable explanation of on-going care and continuity where a patient is having surgery as part of planned multi-modal therapy.

74
3.6
Specific Competency area:
Other treatments Evidence No.
Competency met (mentor)
Student Date
i. Provides suitable written material and clear verbal explanation to a patient, and their carer if appropriate, receiving hormone therapy.
ii. Provides clear verbal explanation (and suitable written material if required) to a patient receiving immunotherapy, cytokines, or other cancer treatment modality.
iii. Identifies possible side effects of treatment and institutes appropriate strategies for their management or prevention.
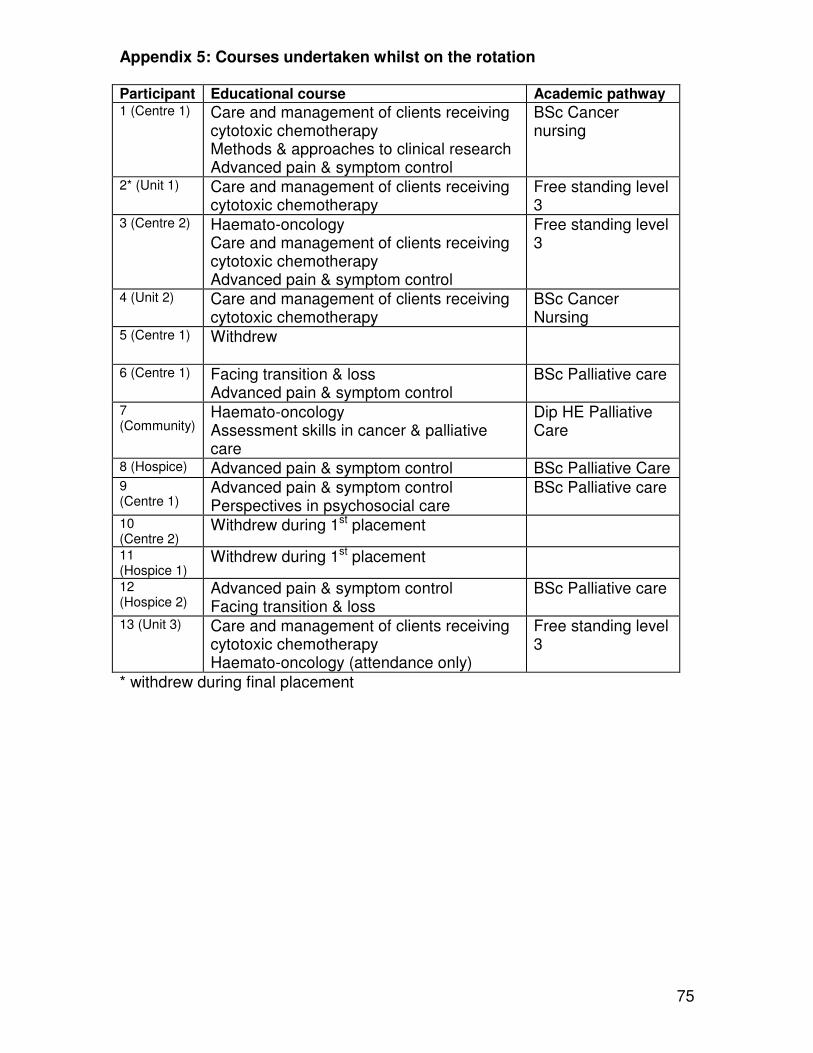
75
Appendix 5: Courses undertaken whilst on the rotation
Participant Educational course Academic pathway 1 (Centre 1) Care and management of clients receiving
cytotoxic chemotherapy Methods & approaches to clinical research Advanced pain & symptom control
BSc Cancer nursing
2* (Unit 1) Care and management of clients receiving cytotoxic chemotherapy
Free standing level 3
3 (Centre 2) Haemato-oncology Care and management of clients receiving cytotoxic chemotherapy Advanced pain & symptom control
Free standing level 3
4 (Unit 2) Care and management of clients receiving cytotoxic chemotherapy
BSc Cancer Nursing
5 (Centre 1) Withdrew
6 (Centre 1) Facing transition & loss Advanced pain & symptom control
BSc Palliative care
7 (Community)
Haemato-oncology Assessment skills in cancer & palliative care
Dip HE Palliative Care
8 (Hospice) Advanced pain & symptom control BSc Palliative Care 9 (Centre 1)
Advanced pain & symptom control Perspectives in psychosocial care
BSc Palliative care
10 (Centre 2)
Withdrew during 1st placement
11 (Hospice 1)
Withdrew during 1st placement
12 (Hospice 2)
Advanced pain & symptom control Facing transition & loss
BSc Palliative care
13 (Unit 3) Care and management of clients receiving cytotoxic chemotherapy Haemato-oncology (attendance only)
Free standing level 3
* withdrew during final placement

76
Appendix 6: Characteristics of rotation programme participants Cohort 1
Applicant Age Years qualified
Years in cancer or PC
Current education level
Seconding employer
Planned career path
1 27 2 0.7 Dip HE Centre Cancer
2 23 1.5 1.4 BSc Unit Cancer
3 23 1.3 1.3 BSc Centre Haematooncology
4 47 10 0 Dip HE Unit Surgery
5 40 18 2.5 Dip HE Centre Unsure
6 29 1.5 1.5 Dip HE Centre Pall care
7 46 25 0 RGN PCT Primary care
8 37 15 1 RGN Hospice Pall Care
Cohort 2
Applicant Age Years
qualified Years in cancer or PC
Current education level
Allocated employer
Planned career path
9 39
4 0 Dip HE Unit Cancer
10 33
1.5 0 BSc Centre Pall care
11 25
1 1 Dip HE Centre Pall care
12 27
2 0 BA Hospice Pall care
13
24 2 0 BSc Unit Cancer

77
Appendix 7: Telephone interview schedule for stakeholders
Introduce self. Researcher/lecturer from King’s. Phoning to gather views about the outcomes from the rotation project.
Phoning all areas and individuals that had contact with the students on the programme.
I am outside of the programme & looking to gain frank, honest, wart-and-all views.
Good time now. What time phone back later?
Will be taking notes. May be a bit slow. May have to ask you to repeat things if I miss
them. May use anonymous quotes in report & subsequent publications. Before I start
can I check you are happy with this?
�
Thinking about the contribution made
by those on the programme…
What contribution have these nurses
on the programme made in your
clinical area(s)?
• Personal/individual level?
• Within team and amongst
colleagues?
• To the organisation as a whole?
What impact have they had within the
team?
• Positive – what they have to
offer?
• Negative – Anything detracted
from having them? (Feelings of
other team members at
opportunity offered to
colleague, support they’ve
needed, time away from clinical,
competency document)
• Have you had any dealing with
the competency document they
complete? What are your views
on it?
• Have other colleagues voiced an
opinion on this?
• What have been the biggest
headaches – if any – associated
with the rotation programme?

78
• What have been the greatest
rewards – if any - associated
with the rotation programme?
Thinking about how the programme
may have evolved or changed with
time?
• What changes have you
noticed?
• Why did these come about?
How involved did you feel with the
preparation for the programme?
How involved have you felt with its
delivery?
What future does the Rotation Project
have?
• Should it continue?
• In what format/guise?
• How could it be improved?
• What changes do you wish to
see?