development and evaluation of a multiplex polymerase chain reaction for the detection of ...
TRANSCRIPT

Correspondence: S. Sethi, STD and TB Division, Department of Medical Microbiology, Postgraduate Institute of Medical Education and Research, Chandigarh, India 160012. Tel: � 91 172 2755161. Fax: � 91 172 2744401. E-mail: [email protected]
(Received 3 September 2011 ; accepted 5 April 2012 )
Scandinavian Journal of Infectious Diseases, 2012; 44: 739–744
ISSN 0036-5548 print/ISSN 1651-1980 online © 2012 Informa HealthcareDOI: 10.3109/00365548.2012.684219
ORIGINAL ARTICLE
Development and evaluation of a multiplex polymerase chain reaction for the detection of Mycobacterium tuberculosis from pulmonary specimens
SHIV KUMAR SHARMA 1 , SUNIL SETHI 1 , MEERA SHARMA 1 , SANDEEP K. MEHARWAL 1 , V. M. KATOCH 2 , S. K. JINDAL 3 & RUPINDER TEWARI 4
From the 1 Department of Medical Microbiology, Postgraduate Institute of Medical Education and Research, Chandigarh, 2 Central Jalma Institute for Leprosy and Other Mycobacterial Diseases, Agra, 3 Department of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh, and 4 Department of Biotechnology, Panjab University, Chandigarh, India
Abstract Background: The diagnosis of pulmonary tuberculosis is still a major challenge. Using a polymerase chain reaction (PCR), one can detect Mycobacterium tuberculosis in clinical samples within a few hours. However, single gene targets may result in false negativity due to the absence of target DNA in some M. tuberculosis isolates. The objective of this study was to develop and evaluate a multiplex PCR (M-PCR) using IS6110 and devR primers for the detection of M. tuberculosis in sputum samples. Methods: Sputum samples were collected from: (1) 200 confi rmed cases of tuberculosis; (2) 100 suspected cases of tuberculosis diagnosed on the basis of clinical and radiological fi ndings; (3) 200 non-tubercular patients suffering from respiratory diseases other than tuberculosis, in whom tuberculosis had been excluded. All 500 sputum samples were subjected to PCR using IS6110 primers, and M-PCR using IS6110 and devR primers; results were compared with con-ventional techniques. Results: It was found that M-PCR was 97.5% successful in detecting the presence of tuberculosis in the confi rmed tuberculosis group as compared to 84.5% by IS6110 -based PCR. In the suspected tuberculosis group, M-PCR could detect 45% of cases as compared to 40% by IS6110 -based PCR. Overall, the specifi cities of both the PCR and M-PCR were found to be 96.5%. Conclusions: This study demonstrated that the M-PCR assay is more sensitive than the IS6110-based PCR for the detection of M. tuberculosis in sputum specimens and could be applied in situations of highly suspected tuberculosis when all others tests including IS6110 PCR are negative.
Keywords: Multiplex PCR , Mycobacterium tuberculosis
Introduction
Tuberculosis is a signifi cant cause of morbidity and mortality in developed and developing countries. The traditional detection of tuberculosis based on culture and phenotypic identifi cation is time-consuming. A new generation of automated methods (BACTEC, MGIT 960) has reduced the time of detection to less than 2 weeks, particularly in smear-positive cases, but these methods are expensive [1]. Using molecular biology tests such as the polymerase chain reaction (PCR), one can detect the presence of Mycobacte-rium tuberculosis in clinical samples within a few hours; this method is fairly rapid and is sensitive and specifi c.
In most PCR studies for the specifi c identifi cation of M. tuberculosis , a single gene has been used as the tar-get for amplifi cation [2 – 4]. However, single gene tar-gets may result in false negativity due to the absence of target DNA in some M. tuberculosis isolates [4,5]. More reliable results would be expected using more than 1 target gene for amplifi cation, i.e. the develop-ment of a multiplex PCR (M-PCR).
The basic requirement for M-PCR is that the entire selected target DNA should be amplifi ed under 1 set of reaction conditions, and that each product should be suffi ciently different in size from the others so that they can be analyzed independently by agarose
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le o
n 03
/17/
14Fo
r pe
rson
al u
se o
nly.

740 S. K. Sharma et al.
gel electrophoresis [6]. M-PCR has been used mostly in genetic disorders [7]. This technique has also been applied to the detection of bacteria and viruses by amplifying segments of 2 different genes [8,9].
The aim of the present study was to develop an M-PCR using IS6110 and devR primers in order to increase the detection rate. IS6110 is an insertion sequence specifi c to M. tuberculosis complex and is repeated 1 – 25 times in the M. tuberculosis genome [10]. devR is a well-characterized target for the detec-tion of M. tuberculosis . The devR – devS locus is pre-ceded by gene Rv3134c , which encodes a putative alanine – valine-rich protein. This locus is conserved in M. tuberculosis and Mycobacterium bovis bacille Calmette – Gu é rin (BCG), but not in other mycobac-teria. The devR – devS encodes a response regulator that has previously been identifi ed to be differentially expressed in the virulent strain of M. tuberculosis [11,12]. As the devR – devS 2-component regulatory system is found to be well conserved in M. tubercu-losis complex [13], and because IS6110 might be either missing or absent in Indian populations, we considered devR to be a suitable target for M-PCR along with IS6110 [14,15] for the detection of M. tuberculosis .
Materials and methods
Study population
A total of 500 consecutive patients – 300 highly sus-pected tuberculosis and 200 non-tubercular patients – who presented to the Pulmonary Medicine Department of the Postgraduate Institute of Medical Education and Research, Chandigarh, India (both as outpa-tients and inpatients) during a period of 2 y from April 2003 to March 2005 were prospectively enrolled in the study. These patients were categorized into 3 groups, as follows: (1) 200 confi rmed cases of tuberculosis with smear and/or culture positivity. Sixty-fi ve of these patients were on anti-tubercular treatment (ATT), and amongst the 65 cases, 21 were treatment failures; the remaining 135 patients denied any previous history of treatment. (2) One hundred patients with clinically/radiologically confi rmed tuberculosis, but smear- and culture-negative (sus-pected group). Out of the 100 clinically confi rmed cases, 33 patients were on ATT and an additional 17 patients had previously taken ATT; the remain-ing patients were not taking any treatment. (3) Two hundred non-tubercular patients suffering from respiratory diseases such as bronchial asthma, lung carcinoma, sarcoidosis, pneumonia, interstitial lung disease, chronic obstructive pulmonary disease (COPD), asthma, or other diseases of the lung, in whom tuberculosis was excluded on the basis of
clinical, radiological, and microbiological tests. Clin-ical parameters such as cough, fever, weight loss, breathlessness, chest pain, exudation, infi ltration, and cavitations were reported in confi rmed and sus-pected cases. Informed consent was obtained from all patients, and the institutional ethics committee approved the study.
Microscopy and culture
Smears were prepared from sputum samples and stained by Ziehl – Neelsen method. Samples were decontaminated by N-acetyl- L -cysteine sodium hydroxide (NALC – NaOH) method, cultured on Lowenstein – Jensen medium, and incubated at 37 ° C for 6 weeks. The isolates were identifi ed using stan-dard methods [16].
DNA extraction
Genomic DNA was extracted from clinical samples and from controls as per the standard protocol [17].
PCR and multiplex assay
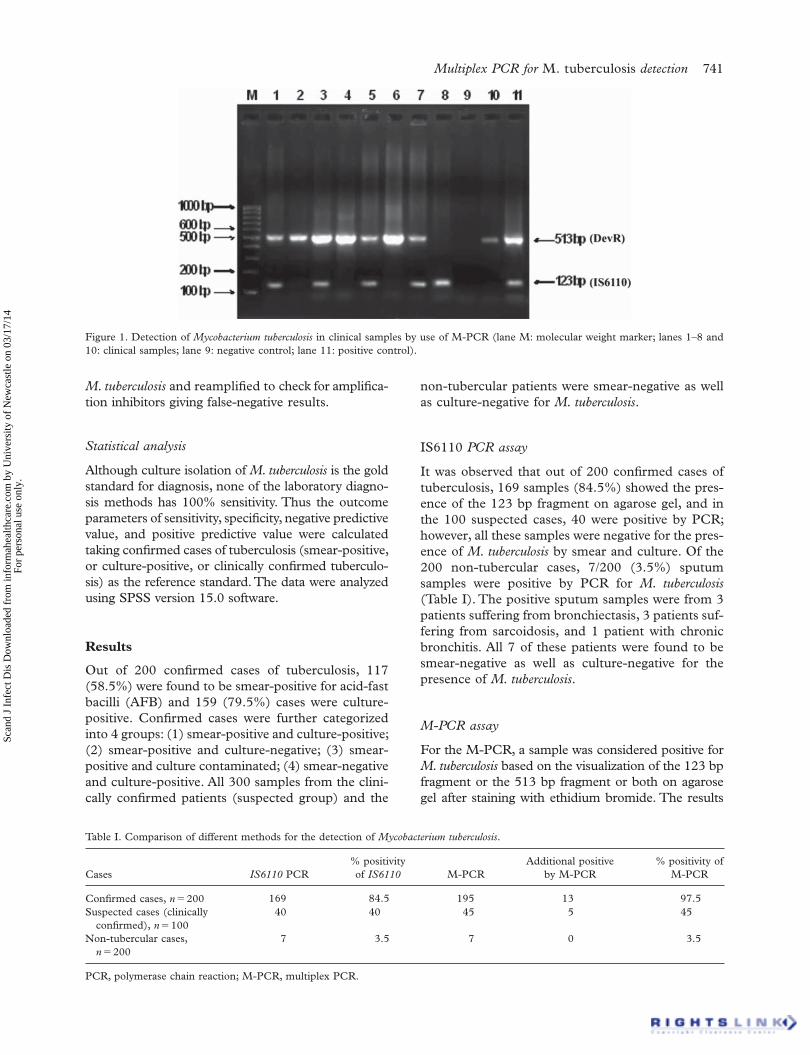
The PCR reaction was carried out using 1 set of primers specifi c for the amplifi cation of the IS6110 element present in M. tuberculosis [18]. The M-PCR reaction was carried out using 2 sets of primers spe-cifi c for the amplifi cation of M. tuberculosis , IS6110 [18] and devR [19]. The primer sequences used were as follows: IS1f (5 ′ CCT GCG AGC GTA GGC GTC GG 3 ′ ) and IS2r (5 ′ CTC GTC CAG CGC CGC TTC GG 3 ′ ), and devRf (5 ′ GGT GAG GCG GGT TCG GTC GC 3′ ) and devRr (5 ′ CGC GGC TTG CGT CCG ACG TTC 3 ′ ) (Bangalore Genei, India). The PCR was performed in 50- μ l reaction volumes using PCR buffer 10X (15 mM), dNTPs mix (10 mM), 10 pmol/ μ l each of IS1f and IS2r, 10 pmol/ μ l each of devRf and devRr, and 5 U/ μ l of Taq polymerase (Bangalore Genei, India). The ther-mal profi le used was 94 ° C for 5 min, denaturation at 94 ° C for 1.5 min, annealing at 65 ° C for 1.5 min, and extension at 72 ° C for 1 min, with a fi nal exten-sion at 72 ° C for 10 min. Thirty-fi ve amplifi cation cycles were performed. The amplifi ed products were stored at 4 ° C until the detection and were then sub-jected to 1.5% agarose gel electrophoresis. The stained gel was examined under UV light to look for the DNA bands of 123 bp and 513 bp correspond-ing to the IS6110 and dev genes, respectively, using a 100 bp ladder molecular weight marker (Figure 1). M. tuberculosis H37RV was used as positive con-trol. DNA from PCR-negative samples was spiked with 100 pg of DNA from an H37Rv strain of
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le o
n 03
/17/
14Fo
r pe
rson
al u
se o
nly.
Multiplex PCR for M. tuberculosis detection 741
M. tuberculosis and reamplifi ed to check for amplifi ca-tion inhibitors giving false-negative results.
Statistical analysis
Although culture isolation of M. tuberculosis is the gold standard for diagnosis, none of the laboratory diagno-sis methods has 100% sensitivity. Thus the outcome parameters of sensitivity, specifi city, negative predictive value, and positive predictive value were calculated taking confi rmed cases of tuberculosis (smear-positive, or culture-positive, or clinically confi rmed tuberculo-sis) as the reference standard. The data were analyzed using SPSS version 15.0 software.
Results
Out of 200 confi rmed cases of tuberculosis, 117 (58.5%) were found to be smear-positive for acid-fast bacilli (AFB) and 159 (79.5%) cases were culture-positive. Confi rmed cases were further categorized into 4 groups: (1) smear-positive and culture-positive; (2) smear-positive and culture-negative; (3) smear-positive and culture contaminated; (4) smear-negative and culture-positive. All 300 samples from the clini-cally confi rmed patients (suspected group) and the
non-tubercular patients were smear-negative as well as culture-negative for M. tuberculosis .
IS6110 PCR assay
It was observed that out of 200 confi rmed cases of tuberculosis, 169 samples (84.5%) showed the pres-ence of the 123 bp fragment on agarose gel, and in the 100 suspected cases, 40 were positive by PCR; however, all these samples were negative for the pres-ence of M. tuberculosis by smear and culture. Of the 200 non-tubercular cases, 7/200 (3.5%) sputum samples were positive by PCR for M. tuberculosis (Table I). The positive sputum samples were from 3 patients suffering from bronchiectasis, 3 patients suf-fering from sarcoidosis, and 1 patient with chronic bronchitis. All 7 of these patients were found to be smear-negative as well as culture-negative for the presence of M. tuberculosis .
M-PCR assay
For the M-PCR, a sample was considered positive for M. tuberculosis based on the visualization of the 123 bp fragment or the 513 bp fragment or both on agarose gel after staining with ethidium bromide. The results
Figure 1. Detection of Mycobacterium tuberculosis in clinical samples by use of M-PCR (lane M: molecular weight marker; lanes 1 – 8 and 10: clinical samples; lane 9: negative control; lane 11: positive control).
Table I. Comparison of different methods for the detection of Mycobacterium tuberculosis .
Cases IS6110 PCR% positivity of IS6110 M-PCR
Additional positive by M-PCR
% positivity of M-PCR
Confi rmed cases, n � 200 169 84.5 195 13 97.5Suspected cases (clinically
confi rmed), n � 10040 40 45 5 45
Non-tubercular cases, n � 200
7 3.5 7 0 3.5
PCR, polymerase chain reaction; M-PCR, multiplex PCR.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le o
n 03
/17/
14Fo
r pe
rson
al u
se o
nly.

742 S. K. Sharma et al.
were recorded as negative in the absence of the 123 bp and 513 bp fragments on the agarose gel (Figure 1).
M-PCR amplifi cation resulted in an increased detection of M. tuberculosis in the clinical samples. M-PCR was 97.5% successful in detecting the presence of M. tuberculosis in microbiologically con-fi rmed cases and 45% successful in clinically con-fi rmed cases, whereas PCR was 84.5% successful in microbiologically confi rmed cases and 40% success-ful in clinically confi rmed cases (Table I).
Comparison of PCR and M-PCR
For the 200 microbiologically confi rmed cases, the percentages of M. tuberculosis detection in sputum samples were as follows: smear 58.5%, culture 79.5%, PCR 84.5%, and M-PCR 97.5%. For the microbio-logically confi rmed and clinically confi rmed tuber-culosis cases, the sensitivity of M-PCR was found to be 80% that of IS6110 . The specifi cities of both PCR and M-PCR were found to be 96.5% (Table II). However, in 5 culture-positive patients, both IS6110 and M-PCR were negative.
For the clinically confi rmed cases, the number of M. tuberculosis -positive samples increased to 45% by the use of M-PCR (Table I). The sensitivity and spec-ifi city of these methods is shown in Table II. Of the 200 non-tubercular cases, 7 were found to positive by both PCR and M-PCR amplifi cation (Table I).
Discussion
The present study suggests that the M-PCR tech-nique is much more sensitive (84.5%) than IS6110 PCR. The increased sensitivity of PCR technology over other techniques has also been reported previ-ously [20,21]. In addition, 40% of suspected cases of tuberculosis (clinically and radiologically proven, but smear-negative and culture-negative) turned out to be PCR-positive for M. tuberculosis . This is in accordance with other studies [22,23], which have also reported M. tuberculosis positivity of 19 – 57% by PCR in clinical samples that were smear-negative as well as culture-negative for the presence of
M. tuberculosis . Although the detection of M. tubercu-losis in clinical samples by PCR was more sensitive than by routinely used techniques, the amplifi cation of an M. tuberculosis -specifi c DNA segment by 1 set of primers did not result in 100% M. tuberculosis detection. This could be due to the following reasons: (1) no biological property is 100% present in all the strains of a particular genus; it is possible that a few strains did not contain IS6110 elements in their genome; (2) the presence of inhibitors; and (3) a small amount of sample [24]. We confi rmed the PCR-negative/culture-positive samples by perform-ing IS6110 PCR on culture isolates, and all the iso-lates were found to be negative for IS6110 and positive for devR . This clearly shows that the IS6110 element was absent in these samples.
In order to increase the sensitivity of PCR, we included 2 sets of primers that were unrelated to each other. The target IS6110 has varying numbers of copies and might even be absent in up to 40% of Indian isolates. The devR locus is conserved in M. tuberculosis and M. bovis BCG, but not in other mycobacteria. The devR – devS encodes a response regulator that has been identifi ed previously as being differentially expressed in the virulent strain of M. tuberculosis . The combination has been shown to improve the sensitivity of detection, as shown in our study. By using these 2 sets of primers ( IS6110 and devR ), the detection of M. tuberculosis was increased from 84.5% (using 1 set of primers IS6110 ) to 97.5% by M-PCR in confi rmed cases. In suspected cases, M-PCR positivity was found to be 45%, although it has previously been demonstrated that the detection limit of IS6110 and devR PCR are the same and can detect 25 fg DNA [25]. There are a few reports on the use of M-PCR for the detection of M. tuberculosis from clinical samples. Boondireke et al. developed an M-PCR for M. tuberculosis and Pneumocystis jirovecii ; sensitivity was found to be 92.1% and specifi city 98.2% [26]. Other studies have used M-PCR IS6110 , MPB64 , and 65 kDa antigen in tuberculosis menin-gitis [27,28]. One group of authors used a combina-tion of IS6110 and protein antigen B (PAB) primers, which resulted in amplifi cation of 123 bp and 419 bp DNA fragments, respectively [29]. This report also
Table II. Sensitivity and specifi city of the different methods.
Parameter Smear Culture IS6110 PCR M-PCR
Sensitivity (95% CI) 39.0% (33.5 – 44.8) 53.0% (47.2 – 58.8) 72.0% (66.6 – 77.0) 82.3% (77.5 – 86.5)Specifi city (95% CI) 100.0% (98.1 – 100) 100.0% (98.2 – 100) 96.5% (92.9 – 98.6) 96.5% (92.9 – 98.6)PPV a (95% CI) 100.0% (96.9 – 100) 100.0% (97.7 – 100) 96.8% (93.6 – 98.7) 97.2% (94.4 – 98.9)NPV a (95% CI) 52.2% (33.5 – 44.8) 58.6% (47.2 – 58.8) 69.7% (63.9 – 75.0) 78.5% (72.8 – 83.4)
PCR, polymerase chain reaction; M-PCR, multiplex PCR; 95% CI, 95% confi dence interval; PPV, positive predictive value; NPV, negative predictive value. a PPV and NPV were calculated using SPSS software.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le o
n 03
/17/
14Fo
r pe
rson
al u
se o
nly.

Multiplex PCR for M. tuberculosis detection 743
favoured the use of M-PCR over simple PCR (using 1 set of primers), as the detection percentage increased to 87.5%. There are also reports on the use of M-PCR for the detection/differentiation of various species of mycobacteria from other clinical samples [30] and from mycobacterial isolates [31,32].
M. tuberculosis could not be isolated from 41 smear-positive cases; 6 cultures were contaminated with other microorganisms and M. tuberculosis could not be isolated in pure culture. Low culture positiv-ity was due to the fact that 33 samples were positive by IS6110 and 36 by M-PCR. This could be because these 30 patients were on ATT, as this has been reported previously [33]. It has been reported that most of the PCR-positive but culture-negative sam-ples were from patients who responded to ATT [21]. In the remaining 11 sputum samples, 3 were positive by PCR and 6 were positive by M-PCR. It is prob-able that mycobacteria failed to grow in these sam-ples because: (1) mycobacteria contained in these samples may have been in a non-cultivable state [24]; (2) our hospital is a referral hospital and the possibil-ity exists of some cases having received partial ATT and being unable to give a reliable treatment his-tory.
In the control group, 7 (3.5%) sputum samples were positive by PCR and M-PCR; 3 of the patients were suffering from sarcoidosis, 3 from bronchiecta-sis, and 1 from chronic bronchitis. Interestingly, we found that in the control group, 3 out of 26 (11.53%) sputum samples from patients with sarcoidosis were positive for M. tuberculosis DNA by IS6110 PCR and M-PCR techniques. The PCR technique used for the detection of M. tuberculosis in human clinical samples has been found to show positivity in patients suffer-ing from sarcoidosis. In the study of Beavis et al., M. tuberculosis DNA was detected by PCR in 50% of the bronchoalveolar lavage samples from patients with sarcoidosis [34]. Saboor et al. showed that M. tuberculosis DNA was detected in 12.5% of the tissue biopsies from patients with sarcoidosis [35]. Moreover the role of mycobacteria in sarcoidosis has been questioned on the basis of observations made by Bocard et al. [36]. The detection of M. tuberculosis DNA by PCR and M-PCR in 4 other patients with non-tubercular lung lesions in the present study was intriguing. It is unlikely that these positive results were due to amplicon carry-over contamination, as we had taken necessary precautions, used all the stringent conditions to avoid carry-over contamina-tion, and also included ample negative controls in all our test runs, as suggested by Cousins et al. [37]. None of the negative controls were ever positive in our PCR runs. In view of these fi ndings, we believe that our false-positivity was not due to sample con-tamination. Since tuberculosis is endemic in India, it
is likely that the patients with non-tubercular cases may have had primary M. tuberculosis complex in their lungs; many years later, after re-exposure to mycobac-teria present in the environment, a limited reactiva-tion of dormant foci of infection may occur in the lungs, which may be picked up by a sensitive tech-nique like PCR [38] but not by Ziehl – Neelsen stain-ing or culture. The sensitivity of Ziehl – Neelsen staining is 10 4 mycobacteria, whereas for positive cul-ture 10 2 mycobacteria are needed. We could not dem-onstrate evidence of disease or tuberculosis reactivation because of a lack of patient follow-up for the 7 cases in the control group who were positive for M. tuber-culosis by PCR and M-PCR.
Five sputum samples from confi rmed cases were found to be PCR-negative, which could be due to the presence of PCR inhibitors in the clinical sam-ples, as has been suggested previously [39,40]. The elimination of inhibitory factors continues to be a challenge in the use and acceptance of PCR assays in the clinical diagnostic setting. The present study suggests that the M-PCR developed in this study is more sensitive and accurate for the detection of M. tuberculosis in sputum samples of patients than IS6110 PCR and other microbiological tests, and could be applied in situations where tuberculosis is highly suspected and all others tests including IS6110 PCR are negative.
Declaration of interest: The authors report no confl icts of interest. The authors alone are respon-sible for the content and writing of the paper.
References
Bemer P, Palicova F, Rusch-Gerdes S, Drugeon HB, Pfyffer [1] GE. Multicentre evaluation of fully automatic BACTEC mycobacteria growth indicator tube 960 system for suscep-tibility testing of Mycobacterium tuberculosis. J Clin Micro-biol 2002;40:150 – 4. Brisson-No ë l A, Gicquel B, Lecossier D, L é vy-Fr é bault V, [2] Nassif X, Hance AJ. Rapid diagnosis of tuberculosis by amplifi cation of mycobacterial DNA in clinical samples. Lancet 1989;335:1069 – 71. Eiseniach KD, Cave MD, Bates JH, Crawford JT. Polymerase [3] chain reaction amplifi cation of repetitive DNA sequence specifi c for Mycobacterium tuberculosis. J Infect Dis 1990;161:977 – 81. Hermans PW, Schuitema AR, van Soolingen D, Verstynen [4] CP, Bik EM, Thole JE, et al. Specifi c detection of Mycobac-terium tuberculosis complex strains by polymerase chain reaction. J Clin Microbiol 1990;28:1204 – 13. Li H, Ulstrup JC, Jonassen TO, Melby K, Nagi S, Harboe M. [5] Evidence for absence of the MPB64 gene in some substrains of mycobacterium bovis BCG. Infect Immun 1993;61:1730 – 4. Henegariu O, Heerema NA, Dlouhy SR, Vance GH, Vogt PH. [6] Multiplex PCR: critical parameters and step-by-step protocol. Biotechniques 1997;23:504 – 11.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le o
n 03
/17/
14Fo
r pe
rson
al u
se o
nly.
744 S. K. Sharma et al.
Ballabio A, Ranier JE, Chamberlain JS, Zoolo M, Caskey CT. [7] Screening of steroid sulfatase (STS) gene deletions by multiplex DNA amplifi cation. Human Genet 1990;84:571 – 3. Bourque SN, Valero JR, Mercier JR, Mercier J, Lavioe MC, [8] Levesque RC. Multiplex polymerase chain reaction for detec-tion and differentiation of the microbial insecticide Bacillus thuringiensis. Appl Environ Microbiol 1993;59:523 – 7. Gibbs RA, Nguyen P, Edwards A, Civitello AB, Caskey CT. [9] Multiplex DNA deletion detection and exon sequencing of hypoxanthine phosphoribosyltransferase gene in Lesch – Nyhan families. Genomics 1990;7:235 – 44. Small PM, Van Embden JD. Molecular epidemiology of [10] tuberculosis. In: Bloom BR, editor. Washington, DC: Amer-ican Society for Microbiology; 1994. pp. 569 – 82. Kinger AK, Tyagi JS. Identifi cation and cloning of genes dif-[11] ferentially expressed in the virulent strain of Mycobacterium tuberculosis. Genes 1993;121:113 – 7. Dasgupta N, Kapur V, Singh KK, Das TK, Sachdeva S, [12] Jyothisri K, et al. Characterization of a two-component system, devR – devS , of Mycobacterium tuberculosis. Tuber Lung Dis 2000;80:141 – 59. Singh KK, Muralidhar M, Kumar A, Chattopadhyaya TK, [13] Kapila K, Singh MK, et al. Comparison of in house polymer-ase chain reaction with convention technique for the detec-tion of Mycobacterium tuberculosis DNA in granulomatous lymphadenopathy. J Clin Pathol 2000;53:355 – 61. Das S, Paramasivam CN, Lowerie DB, Praphakar R, Naray-[14] anan PR. IS6110 RFLP typing of clinical isolates of M. tuberculosis from patients with pulmonary tuberculosis in Madras, south India. Tuber Lung Dis 1995;76:550 – 4. Radhakrishanan I, Manju YK, Kumar RA, Mundayoor S. [15] Implication of low frequency of IS6110 in fi ngerprinting fi eld isolates of Mycobacterium tuberculosis from Kerala, India. J Clin Microbiol 2001;39:1683. Vestal AL. Procedure for isolation and identifi cation of [16] mycobacteria. Publication 77:8230. Atlanta, GA: Centers for Disease Control and Prevention; 1977. p. 159. Vestal AL. Procedure for isolation and identifi cation of [17] mycobacteria. Publication 77:8230. Atlanta, GA: Centers for Disease Control and Prevention; 1977. p. 1 – 135. van Soolingen D, Hermans PW, de Haas PE, Soll DR, van [18] Embden JD. Occurrence and stability of insertion sequences in Mycobacterium tuberculosis complex strains: evaluation of an insertion sequence-dependent DNA polymorphism as a tool in the epidemiology of tuberculosis. J Clin Microbiol 1991;29:2578 – 86. Rodrigues C, Nukala R, Menon S, Hakimiyan A, Mehta AP. [19] DNA amplifi cation of IS6110 in rapid detection of Myco-bacterium tuberculosis. Indian J Med Microbiol 1997;4:167 – 71. Singh KK, Nair MD, Radhakrishnan K, Tyagi JS. Utility of [20] PCR assay in diagnosis of en-plaque tuberculoma of the brain. J Clin Microbiol 1999;37:467 – 9. Clarridge JE, Shawar RM, Shinnick TM, Plikaytis BB. [21] Large scale use of polymerase chain reaction for detection of Mycobacterium tuberculosis in a routine mycobacteriology laboratory. J Clin Microbiol 1993;31:2049 – 56. Kolk AH, Schuitema AR, Kuijper S, Van Leeuwen J, Hermans [22] PW, Van Embden JD, et al. Detection of Mycobacterium tuberculosis in clinical samples by using polymerase chain reaction and a nonradioactive detection system. J Clin Micro-biol 1992;30:2567 – 75. Kocagoz T, Yilmaz E, Ozkara S, Kocagoz S, Hayran M, [23] Sachedeva M, Chamber HF. Detection of Mycobacterium tuberculosis in sputum samples by polymerase chain reaction using a simple fi eld procedure. J Clin Microbiol 1993;31:1435 – 8.
Warring FC, Sutramongkole U. Non-culturable acid-fast [24] forms in the sputum of patients with tuberculosis and chronic pulmonary disease. Am Rev Respir Dis 1970;102:714. Haldar S, Chakravorty S, Bhalla M, De Majumdar S, Tyagi [25] JS. Simplifi ed detection of Mycobacterium tuberculosis in sputum using smear microscopy and PCR with molecular beacons. J Med Microbiol 2007;56:1356 – 62. Boondireke S, Mungthin M, Tan-ariya P, Boonyongsunchai [26] P, Naaglor T, Wattanathum A, et al. Evaluation of sensitivity of multiplex PCR for detection of Mycobacterium tubercu-losis and Pneumocystis jirovecii in clinical samples. Clin Microbiol 2010;48:3165 – 8. Rafi W, Venkataswamy MM, Ravi V, Chandramuki A. Rapid [27] diagnosis of tuberculous meningitis: a comparative evalua-tion of in-house PCR assays involving three mycobacterial DNA sequences, IS6110 , MPB-64 , and 65 kDa antigen. J Neurol Sci 2007;252:163 – 8. Kusum S, Aman S, Pallab R, Kumar SS, Manish M, Sudesh [28] P, et al. Multiplex PCR for rapid diagnosis of tuberculous meningitis. J Neurol 2011;258:1781 – 7. Forbes BA, Hicks KE. Direct detection of Mycobacterium [29] tuberculosis in respiratory specimens in a clinical labora-tory by polymerase chain reaction. J Clin Microbiol 1993;31:1688 – 94. Kulski JK, Khinsoe C, Pryce T, Christiansen K. Use of mul-[30] tiplex PCR to detect and identify Mycobacterium avium and M. intracellulare in blood culture fl uids of AIDS patients. J Clin Microbiol 1995;33:668 – 74. Mustafa AS, Ahmed A, Abal AT, Chugh TD. Establishment [31] and evaluation of a multiplex polymerase chain reaction for detection of mycobacteria and specifi c identifi cation of Mycobacterium tuberculosis complex. Tuber Lung Dis 1995;76:336 – 43. Sinclair K, Challans JA, Kazwala RR, Hewinson RG, Sharp [32] JM. A multiplex polymerase chain reaction for distinguishing Mycobacterium tuberculosis from Mycobacterium tubercu-losis complex. Mol Cell Probes 1995;9:291 – 5. Tanaka II, Anno IS, Leite SR, Cooksey RC, Leite CQ. Com-[33] parison of multiplex PCR assay with mycolic acids analysis and conventional methods for the identifi cation of mycobac-teria. Microbiol Immunol 2003;47:307 – 12. Beavis KG, Lichty MB, Jungkind DL, Giger O. Evaluation [34] of Amplicor PCR for direct detection of Mycobacterium tuberculosis from sputum specimens. J Clin Microbiol 1995;33:2582 – 6. Saboor SA, Johanson NM, McFadden J. Detection of [35] mycobacterial DNA in sarcoidosis and tuberculosis with polymerase chain reaction. Lancet 1992;339:1012 – 5. Bocard D, Lecossier D, De Lassence A, Valeyre D, Battesti [36] JP, Hance AJ. A search for mycobacterial DNA in granu-lomatous tissues from patients with sarcoidosis using the polymerase chain reaction. Am Rev Respir Dis 1992;145:1142 – 8. Cousins DV, Wilton SD, Francis BR, Gow BL. Use of [37] polymerase chain reaction for rapid diagnosis of tuberculosis. J Clin Microbiol 1992;30:255 – 8. Richter E, Greinert KD, Rusch-Gerdes S, Schluter C, [38] Duchrow M, Galle J, et al. Assessment of mycobacterial DNA in cells and tissues of mycobacterial and sarcoid lesions. Am J Respir Crit Care Med 1996;153:375 – 80. Manjunath N, Shankar P, Rajan L, Bhargave A, Saluja S, [39] Shriniwas. Evaluation of a polymerase chain reaction for the diagnosis of tuberculosis. Tubercle 1991;72:21 – 7. Soni H, Skurnik M, Liippo K, Tal E, Vilganen MK. Detection [40] and identifi cation of mycobacteria by amplifi cation of a seg-ment of the gene coding for the 32-kilodalton protein. J Clin Microbiol 1992;30:2025 – 8.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
New
cast
le o
n 03
/17/
14Fo
r pe
rson
al u
se o
nly.