development and use of ambulatory adverse event trigger tools jonathan r. nebeker ahrq conference...
TRANSCRIPT

Development and Use of Ambulatory Adverse Event Trigger Tools
Jonathan R. Nebeker
AHRQ CONFERENCE SEPT. 29, 2010
BOSTON UNIVERSITY SCHOOL OF PUBLIC HEALTH, BOSTON, MA, VA CENTER FOR ORGANIZATION, LEADERSHIP AND MANAGEMENT RESEARCH (COLMR), BOSTON [email protected]

Acknowledgements
PI Amy Rosen, PhD Co-PI Jonathan Nebeker,
MD, MS Co-Investigators:
Stephan Gaehde, MD Haytham Kaafarani, MD,
MPH
Brenna Long, MA Hillary Mull, MPP Brian Nordberg, BS Steve Pickard, MS Peter Rivard, PhD Lucy Savitz, PhD, MBA Chris Shanahan, MD, MPH Stephanie Shimada, PhD
Sponsored by AHRQ Contract No. HHSA290200600012, Task Order Officer: Amy Helwig, MD
What’s new?
ADE Surveillance rules Complex to maximize PPV and Sensitivity Action-Oriented to make a difference for
patient Use input from system-based focus
groups and experts with practical experience
Study Flow
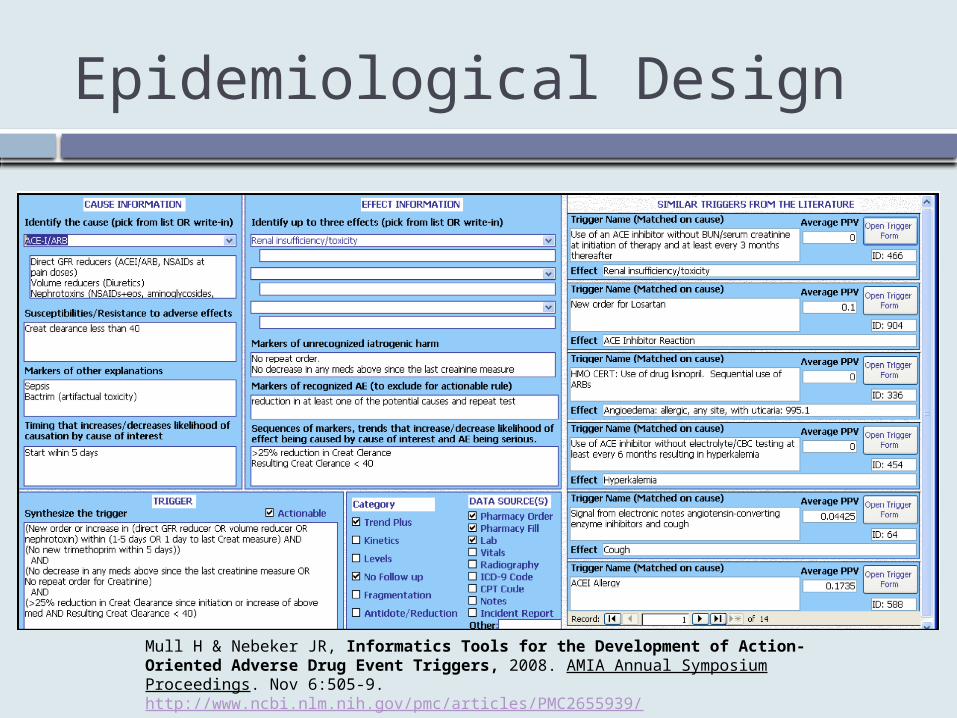
Epidemiological Design
Mull H & Nebeker JR, Informatics Tools for the Development of Action-Oriented Adverse Drug Event Triggers, 2008. AMIA Annual Symposium Proceedings. Nov 6:505-9. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2655939/

Example of Complex Trigger
[Dose change in GFR reducer or renal toxin and subsequent creatinine > 50% from average baseline creatinine value or > 33% from last post dose change creatinine value] AND (No new trimethoprim within 1 day prior to 7 days after creatinine lab value firing) AND (GFR Reducer or renal toxin used within 90 days prior to lab value)
Suppress If: Renal toxin or GFR reducer dose reduced 0-7 days after lab) OR ( new creatinine lab result within 1-6days of firing lab value)
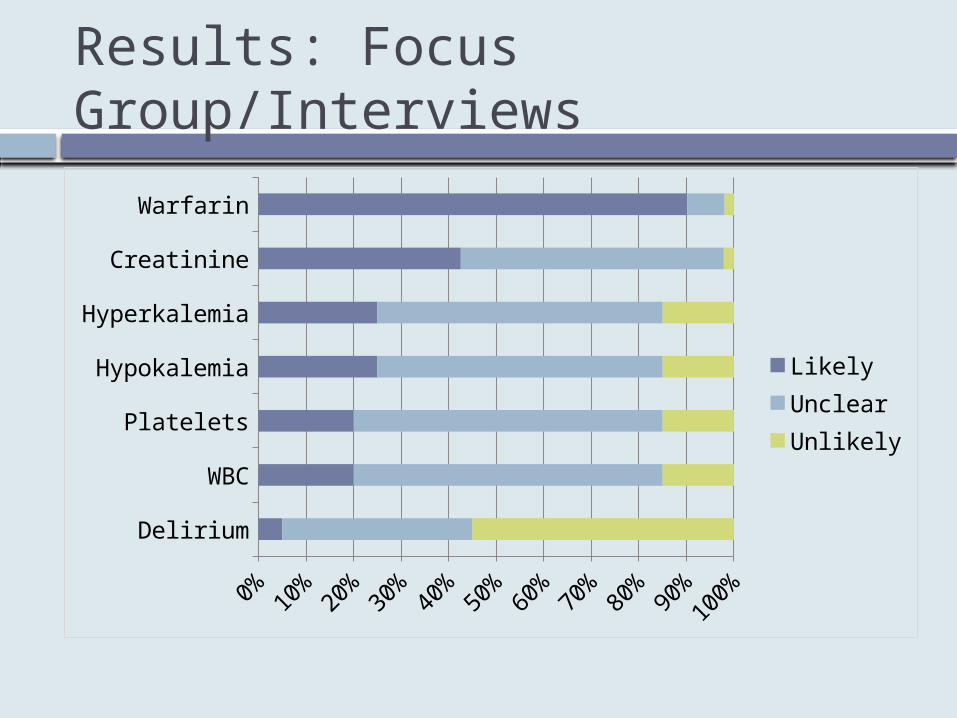
Results: Focus Group/Interviews
Delirium
WBC
Platelets
Hypokalemia
Hyperkalemia
Creatinine
Warfarin
0% 20% 40% 60% 80% 100%
LikelyUnclearUnlikely

Delphi Highlights
50% national experts, 50% local clinical leaders
Got perspectives that represented emphasis of research or clinical experience. ED doc liked delirium trigger
Various, contradictory input on thresholds
Helpful modifications Interesting insights on what would be
useful
Analysis
Sample Requested sets of 2,000 pts based on
exposure to target meds Got 1,059 to 9,339 -> IRB amendment Restricted to patients with 2 notes in 1 year
Analysis 1° PPV = number of patients with
AE/number of cases triggered 2° Sensitivity, if prevalence >5% (for 25%
CI width) (highest was 4%)

Ignore the CI behind the curtain
Nebeker JR, Stoddard GJ & Rosen AK, Considering Sensitivity and Positive Predictive Value in Comparing the Performance of Triggers Systems for Iatrogenic Adverse Events, Proceedings of the Trigger and TIDS Expert Meeting, Agency for Healthcare Research and Quality, June 2008. Bethesda, MD. http://www.ahrq.gov/QUAL/triggers/triggers2.htm

End Points
Harm PSO Harm scale WHO Causality criteria (certain or probable) Explicit criteria Lab values without symptoms are not harm
Change in care (useful) E.g., prevented additional lab draw

Trigger Performance
Trigger Reviewed/ Flagged
Harm PPV (CI)
Change PPV (CI)
Either PPV (CI)
Creatinine 40/57 0 60%(43-75%)
60%(43-75%)
WBC 0 - - -
Platelets 17/17 6%(0-29%)
53%(28-77%)
59%(33-82%)
Warfarin 96/677 13%(7-21%)
14%(7-22%)
19%(12-28%)
Hypokalemia
85/90 17%(9-26%)
42%(31-54%)
58%(46-68%)
Hyperkalemia
50/64 8%(2-19%)
28%(16-43%)
36%(23-51%)
Delirium 68/359 10%(4-20%)
10%(4-20%)
19%(11-31%)
Summary
Harm is in the eye of the beholder: less or more? Doomed to benchmarking apples with
oranges? Explicit criteria
Potential to affect practice Are complex trigger better?