development of periodontium 1
TRANSCRIPT

DEVELOPMENT OF PERIODONTIUM
“You never know where you are going unless you know where you came from”
DR. T.MADHAVI
PERIO PG
The periodontium is defined as those tissues supporting & investing the tooth,
comprising of
1. Cementum
2. Periodontal ligament
3. Bone lining the alveolus (socket)
4. That part of the gingiva facing the tooth
Following the development of the neural tube, the neural crest cells (NCC) migrate
from the dorsal midline region of the neural tube to invade the developing branchial
arches. Dye injected tracings have shown that neural crest cells from the posterior
midbrain, and to a lesser extent from the anterior hindbrain, form dental
ectomesenchyme. Subsets of cranial neural crest cells give rise to chondrocytes,
osteoblasts, periodontal ligament fibroblasts, cementoblasts and odontoblasts.
The failure of the normal migration of neural crest ectomesenchymal cells to
appropriate sites during craniofacial development leads to serious developmental
defects.
Dental lamina
Two or three weeks after the rupture of the buccopharyngeal membrane, when the
embryo is 6 weeks old, certain areas of basal cells of the oral ectoderm proliferate
more rapidly. This leads to formation of the dental lamina. It is a band of epithelium
that has invaded the underlying ectomesenchyme along each of the horseshoe- shaped

future dental arches. The dental laminae serve as the primordium for the ectodermal
portion of the deciduous teeth.
Tooth Development
The developmental history of a tooth is divided into several morphogenetic “stages”.
They are named after the shape of the epithelial part of the tooth germ and are called
Bud stage
Cap stage
Bell stage
Bud stage : Portions of epithelium in dental lamina, first begin to aggregate and
invaginate into underlying connective tissue
Cap stage: the enamel organ is in its earliest stage of development. The dental papilla
and dental follicle are formed by concentration of neural crest ectomesenchyme cells.
The interaction b/w cell surface syndecan and tenascin (extra cellular matrix adhesion
molecule) reduces migration and promotes aggregation of the ectomesenchymal cells
to form papilla & follicle.

Immediately underneath the epithelial cap, mesenchymal cells begin to proliferate and
form dental papilla. These cells further proliferate and encapsulate the enamel organ
to form dental sac.
(The syndecans: In the early 1990s a group of scientists discovered that a number of
components of the extra-cellular microenvironment had a high affinity for binding
with heparin. These extra-cellular components included growth factor peptides,
proteases, antiproteases and ECM molecules which, by binding to a cell, could
produce changes in cell shape, motility, adhesion, proliferation and differentiation.
They discovered that there is a family of integral membrane proteoglycans made up of
heparan and chondroitin sulphate, both structural analogues of heparin, which can
also bind to a wide variety of structural proteins and growth factors in the internal
and external cellular environment. They named these molecules the syndecans, from
the Greek ‘syndein’ which means ‘to bind together’. It has since been shown that by
binding to extra-cellular ligands, syndecans can mediate the activity of the ligands
and enable the cells to become more or less responsive to their microenvironment.
They are also involved in the maintenance of cell morphology. For example, if
syndecans are not expressed in epithelial cells, then the cells become rounded in
shape.
At present, four members of this family have been identified.
Syndecan-1, the most prevalent of the group, is expressed predominantly in epithelial
tissues.
Syndecan-2 predominates in tissues rich in endothelial cells.

Syndecan-3 is found primarily in neural tissues.
Syndecan-4 mainly in the liver and kidney.)
Bell Stage : enamel organ continues to enlarge and takes on a bell shaped appearance.
Four different types of cells can be distinguished on light microscopic examination.
Inner enamel epithelium – it consists of a single layer of cells that differentiate into
tall columnar ameloblasts. The cells of IEE exert an organizing influence on the
underlying mesenchymal cells in the dental papilla, which later differentiate into
odontoblasts.
Outer enamel epithelium – the cells are low cuboidal. During the formation of enamel,
the OEE is laid in folds. Between the folds, the adjacent mesenchyme of the dental sac
forms papillae that contain capillary loops and thus provide a rich nutritional supply
for the avascular enamel organ.
Stratum intermedium – a few layers of squamous cells between IEE and stellate
reticulum. Essential for enamel formation.
Stellate reticulum – the cells are star shaped with long processes and intercellular
fluid. The layer collapses before enamel formation to reduce the distance between
ameloblasts and the nutrient capillaries near OEE.
Advanced bell stage: formation of future DEJ – the boundary between the IEE and the
odontoblasts – membrana preformativa. The cervical loop of enamel organ gives rise
to HERS.

Development of periodontium
Mesenchyme deriving periodontium has two compartments:
1. Alveolar clade: fibroblasts, osteoblasts
2. Cement clade: fibroblasts, cementoblasts
Dental follicle (dental sac) gives rise to cementum, periodontal ligament and the
alveolar bone.
Dental follicle anatomically consists of dental follicle proper, perifollicular
mesenchyme.

Dental follicle proper: well defined band of cells juxtaposed to the dental papilla and
the convex outer surface
CEMENTUM
The cementum is a specialized mineralized tissue covering the root surfaces. After
enamel & dentin formation has reached the future CEJ, enamel organ forms the
Hertwig’s epithelial root sheath (HERS). HERS consists of the outer and inner enamel
epithelia. The structural continuity of HERS is lost once there is differentiation of
radicular cells into odontoblasts & first layer of root dentin is laid. The remnants of
HERS persist as cell rests of Malassez which are found in the periodontal ligament of
erupted teeth.
The intact epithelial sheath is located between the dental papilla and the dental follicle
proper. Cells of the dental follicle proper project cytoplasmic processes from their
leading edge towards and into the intercellular space between the root sheath cells.
These cells are identified as precementoblasts. The unidirectional migration of
precementoblasts towards the predentin surface appears to contribute to the breakup of
the root sheath and the formation of Sharpey’s fibres. Upon contact with the predentin
surface, the elongated precementoblasts become cuboidal in shape and differentiate
into cementoblasts.
Following a brief period of cementogenesis, the cementoblasts appear to detach from
the newly formed cementum surface and join the fibroblast population in the
periodontal ligament.
Primary cementum formation
Once differentiated, the cementoblasts deposit collagen fibrils at right angles to the
root surface so that the root has a series of fine collagen fibrils attached to it. The

cementoblasts then migrate away but continue to deposit collagen so that the fine fiber
bundles not only lengthen to maintain a fibrous fringe on the root surface, but also
thicken to form the fibrous matrix of acellular cementum. Cementoblasts also secrete
non collagenous proteins such as bone sialoprotein and osteocalcin.
This first formed cementum is acellular, as the cells that form it remain on its surface;
develops relatively slowly as the tooth is erupting; and covers atleast the coronal two
thirds of the root. First formed cementum thus consists of a mineralized layer with a
fibrous fringe attached to it. This continues until the forming periodontal ligament
fiber bundles become attached to the fibrous fringe. No surface layer of unmineralized
matrix is associated with acellular cementum.
Secondary cementum formation
Once the tooth is in occlusion, a more rapidly formed and less mineralized form of
cementum is deposited around the apical third of the root. Cementoblasts become
trapped in the matrix they are forming to occupy lacunae, and the cells become
cementocytes.
Five major types of cementum – Schroeder 1992
1. Acellular intrinsic fiber cementum
2. Acellular extrinsic fiber cementum
3. Cellular intrinsic fiber cementum
4. Cellular mixed fiber cementum
5. Acellular afibrillar cementum

Acellular intrinsic fiber cementum
First formed cementum as a result of cementoblastic activity and is elaborated before
the periodontal ligament forms, therefore the collagen is intrinsic. During
cementogenesis, osteopontin is prominent in intrinsic fiber cementum.
Acellular extrinsic fiber cementum
Once the PDL fiber bundles are formed and get connected to fibrous fringe bundles of
the acellular intrinsic fiber cementum, further deposition of mineral about and within
the bundles results in the formation of acellular extrinsic fiber cementum. It is made
up of a particular class of fibroblasts that are alkaline phosphatase positive.
Cellular intrinsic fiber cementum
The cells forming this cementum resemble the bone-forming cells. When first
deposited, the periodontal ligament is unorganized, the cementoblasts deposit the
organic matrix directly onto the root surface. No evidence of insertion of the sharpey’s
fibers. It is commonly associated with the healing of root fractures and repair of
resorptive defects.
Cellular mixed fiber cementum
It consists of intrinsic collagen fibers produced by the cementoblasts and some
extrinsic sharpey’s fibers.
Acellular afibrillar cementum
It is limited to the enamel surface and appears as cemental spurs or cemental islands
on the crowns of erupted teeth. It represents aberration where, a part of REE
disaggregates and the cells of dental follicle interact with the exposed enamel matrix,
leading to cementum deposition.

PERIODONTAL LIGAMENT
The development of periodontal ligament begins with root formation prior to tooth
eruption.
The mesenchymal cells of perifollicular region attain polarity, increased cellular
volume and synthetic activity. They become elongated. There is an increase in RER,
mitochondria and active golgi complex which synthesize collagen fibrils and
glycoprotein.
Principal fibers
The development of the major collagen bundles, the principle fibers of the periodontal
ligament, is closely related to root formation.
Fiber bundles originate at the surface of the newly formed root dentin in close relation
to elongated and highly polarized fibroblasts. The fringe fibers are tightly packed by
the action of cementoblasts. As the periodontal ligament matures, the fringe fibers
merge across the width of the ligament to form the principle fiber bundles. During the
development of the fringe fibers, fibroblasts exhibit cytoplasmic polarity towards the
root and alveolar bone surfaces. A specific cementum attachment protein favours the
PDL fibroblast attachment to the cementum surface.

With continued development of the root, the principle fibres are established as
continuous structures embedded as Sharpey’s fibers in bone and cementum.
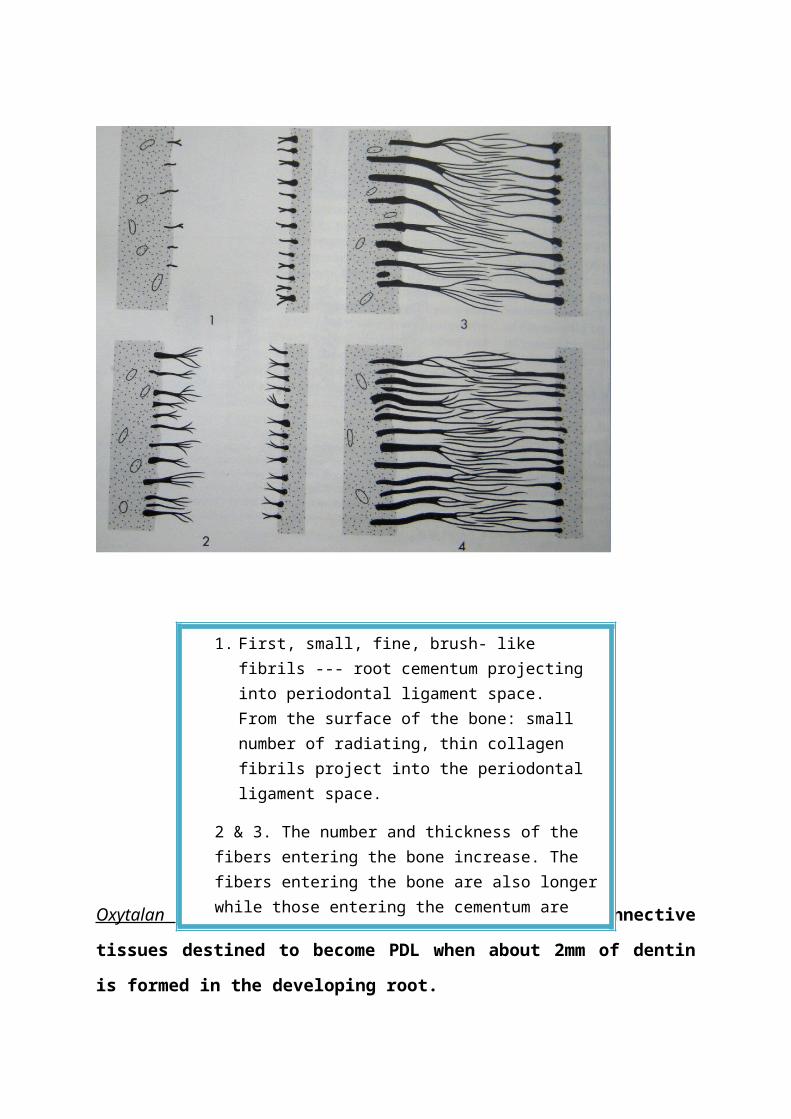
The figure illustrating the development of principle fibres of periodontal ligament.
Bone Cementumm
1. First, small, fine, brush- like fibrils --- root cementum projecting into periodontal ligament space. From the surface of the bone: small number of radiating, thin collagen fibrils project into the periodontal ligament space.
2 & 3. The number and thickness of the fibers entering the bone increase. The fibers entering the bone are also longer while those entering the cementum are still short.
4. The fibers entering the cementum increase in length and thickness and fuse with fibres originating from the alveolar bone in the periodontal ligament space.(intermediate zone)
Bone Cementumm

Oxytalan fibers: These are demonstrated in connective tissues destined to become
PDL when about 2mm of dentin is formed in the developing root.
They increase in size and rearrange themselves with further root development
Cells: The cells of the periodontal ligament are fibroblasts, osteoblasts, cementoblasts,
cementoclasts, and epithelial cells.
Viable cells are required for tooth movement.
1. Fibroblasts: These are the principle cells and most abundant cells in the
periodontal ligament and metabolize the extra cellular matrix components.
Fibroblasts help in remodelling: both synthesize & degrade collagen.
Subpopulation of osteoblast- like fibroblasts: these form bone cells &
cementoblasts, and are rich in alkaline phosphatase. They help in the
production of Acellular extrinsic fiber cementum.
2. Epithelial cells: Remnants of HERS, close to the cemental surface. These are
the Rests of Malassez.
3. The developing periodontal ligament consists of undifferentiated mesenchymal
cells or progenitor cells that retain the ability to differentiate into osteoblasts,
cementoblasts and fibroblasts.
4. Bone and cementum cells: Although technically situated in the PDL, bone and
cementum cells are properly associated with the hard tissues they form.
Development of neurovascular elements
In the early bell stage: rich innervation associated with small blood vessels is found in
the inner investing layer of dental follicle. As the root formation continues and the
tooth erupts, nerves grow into periodontal ligament. Vasculature is derived from the
networks associated with enamel organ & alveolar mucosa, vessels spread apically to
supply PDL.

GINGIVA
It is that part of the oral mucosa that covers the alveolar process of the jaws and
surrounds the necks of the teeth.
It comprises gingival epithelial and connective tissue. The epithelial component shows
regional morphological variations that include oral gingival epithelium, oral sulcular
epithelium and junctional epithelium.
The gingiva evolves as the crown enters the oral cavity by breaking through the oral
epithelium.
Development
The crown of the tooth is covered by a double layer of epithelial cells at the time it
begins its eruptive movements.
1. Those cells in contact with the enamel are the ameloblasts, which, having
completed their formative function, become firmly attached to the enamel
surface.
2. The outer layer consists of more flattened cells, the remnants of all the
remaining layers of the dental organ.
The above two layers of cells, together are called the reduced enamel epithelium.
Between the REE and the overlying oral epithelium is connective tissue that supports
both the REE and the oral epithelium.
When tooth eruption begins, this connective tissue breaks down. In response to the
degenerative changes occurring in the connective tissue, the cells of the outer layer of
the reduced enamel epithelium and the basal cells of the oral epithelium proliferate
and migrate into the degenerating connective tissue and eventually fuse to establish a
mass of epithelial cells over the erupting tooth. Cell death at the middle of this
epithelial plug leads to the formation of an epithelium- lined canal through which the
tooth erupts without hemorrhage.
REE

From this mass of epithelium, the epithelial cuff, together with the remaining REE, the
epithelial component of the dentogingival junction is established. Once the tip of the
cusp of the erupting tooth emerges into the oral cavity, oral epithelial cells begin to
migrate partially over the REE in an apical direction. The attachment of the gingival
epithelium to tooth is maintained through the reduced ameloblasts and their hemi
desmosomes and basal lamina adjacent to the enamel surface. This is the primary
epithelial attachment.
The REE transforms gradually to become Junctional epithelium. The reduced
ameloblasts change their morphology and are transformed into squamous epithelial
cells that retain their attachment to the enamel surface. The cells of the outer layer of
the REE retain their ability to divide continuously to become and function as basal
cells of the forming Junctional epithelium. The transformed ameloblasts are
eventually displaced by the mitotic activity of these basal cells.
Meanwhile, the cells of the epithelial cuff stratify separating the cells of transformed
dental epithelium from the nutritive supply, resulting in the degenerating of latter cells
creating a gingival sulcus. The final conversion of the REE to JE may not occur until
3- 4 years after the tooth has erupted. Thus the epithelial component of the
dentogingival junction is formed, the JE from REE and the sulcular epithelium from
epithelial cuff. The JE derived from dental epithelium is eventually replaced by JE
formed from oral epithelial cells.
Development of gingival connective tissue
Gingival connective tissue fibroblasts originate from perifollicular mesenchyme.
During normal development, gingival fibroblasts do not come into contact with the
tooth surface. Gingival collagen turns over more rapidly than that of skin and bone,
but slower than that of periodontal ligament. The collagen matrix of gingival
connective tissue is well organized into fiber bundles.
ALVEOLAR BONE
Alveolar bone proper
Late bell stage: bony septa, bony bridges- clearly outlined bony compartments
around tooth germs.
Bony compartments + tooth germ: bodily movements to adjust to growing jaws
– minor bone remodeling
Major changes: root development & eruption
Cells of dental follicle– osteoblasts – alveolar bone proper
Size and shape of individual tooth roots determine overall structure
Insertion of sharpey’s fibers
Rest of the bony structures: periosteal bone formation
Remodeling
At root formation: Alveolar process is over the occlusal plane of tooth.
Tooth eruption: remodeling
Gubernacular canal
New bone at base of bony crypt
EPITHELIAL MESENCHYMAL TISSUE INTERACTIONS

General features
Tissue morphology and phenotype are controlled by a complex interplay between
tissues of ectodermal and mesodermal origin. The interactions are controlled through
secreted products released from cells residing within both of these tissues and are
regulated via the genetic code of these cells.
Spemann (1938) demonstrated that for organogenesis to proceed, some form of
communication between the epithelial and mesenchymal tissues was required. This
interaction was called secondary embryonic induction and was shown to regulate
morphogenesis and cell differentiation.
The following are some examples that provide useful insight into the development of
teeth.
1. If epithelium from a developing tooth bud site is placed onto mesenchyme
distant from the dental arch, no tooth formation results.
2. If epithelium from a site that normally does not produce teeth is layered over
mesenchyme from the dental arch, then normal tooth bud formation occurs.
3. If epithelium from a developing tooth bud site is placed over the connective
tissue derived from the neural crest, then tooth development progresses.
These findings indicate that in undifferentiated tissues (such as neural crest cells)
the epithelium has an instructive component leading to the development of the
ectomesenchyme. Once this differentiation process has been initiated, the
ectomesenchyme adopts the dominant role in epithelial- mesenchymal interactions.
Once the enamel organ has formed during tooth development, the cells of the inner
enamel epithelium induce the adjacent cells in the dental papilla to differentiate
into odontoblasts: epithelium influencing mesenchyme.
Genetic features
The pathway of initiation, morphogenesis, and differentiation involves the production
of molecular signals via the initiation of gene expression.

Genetic codes for signaling mechanisms—instruct cells leading to organ development
E.g. transcription factors: these are nuclear proteins that bind to DNA and control the
expression of other genes.
Homeobox (Hox) genes: specify spatial location of future tooth germs.
Dlx-1 & 2 is noted in areas of epithelial thickening.
Molecular features
Following gene expression, locally secreted molecules control cell differentiation &
organ development.
Growth factors, cell surface glycoproteins, components of extracellular matrix appear
to be prime candidates for governing developmental processes. These exert their
influence on cells via specific cell surface receptors
During odontogenesis, BMPs, TGF- ß, FGF (fibroblast growth factor) have been
found to be differentially expressed according to the stage of development,
morphogenesis and cell differentiation.
Other growth factors including PDGF, EGF and growth hormone have been
associated with different stages of tooth development.
TGF- ß1 is first seen in the epithelial thickenings that dictate sites of developing teeth.
Shortly after this it is expressed in the underlying mesenchyme.
BMP-2, BMP-4 -- Budding epithelium....Mesenchyme.
FGF-3
FGF-4

Extracellular matrix
Components of extracellular matrix and cell surface--- instructional effect on cells
Initiated from mesenchymal cells---- influence ectodermal tissues
Tenascin : condensing mesenchyme of dental papilla
Tenascin, fibronectin --- bell stage --- odontoblast differentiation.
Syndecan – 1 --- early bud stage through cap stage --- condensing mesenchyme of
dental papilla
Decreases during transition from cap to bell
EGF – high in epithelium in bud stage, shifts to mesenchyme in bell stage.

Summary
The development of periodontal tissues involves both ectodermal and mesenchymal
tissues.
A good understanding of the principles of formation of periodontal structures is
essential for unraveling the mechanisms associated with tissue regeneration.
The clinical ramifications lie in the regulatory mechanisms governing the correct
expression of epithelial & connective tissue components during regeneration and r.
repair.