diabetes and vascular disease: from mechanisms to ... · prognosis in type 2 diabetes davide...
TRANSCRIPT

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 1
Ferrarotto Hospital University of Catania
Coronary Atherosclerotic Burden And
Prognosis In Type 2 Diabetes
Davide Capodanno, MD, PhD Ferrarotto Hospital, University of Catania, Italy
Diabetes and vascular disease: from mechanisms to treatment

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 2
Ferrarotto Hospital University of Catania
Disclosure of Financial Interest
• I, Davide Capodanno, DO NOT have a financial
interest/arrangement or affiliation with one or more
organizations that could be perceived as a real or
apparent conflict of interest in the context of the
subject of this presentation.

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 3
Ferrarotto Hospital University of Catania
Questions Surrounding Revascularization For
Coronary Artery Disease in Type 2 Diabetes
What are the contemporary outcomes of patients with coronary artery disease and diabetes?
Does the coronary atherosclerotic burden impact on prognosis in diabetes?
Does diabetes independently weigh into decision making for revascularization by PCI or CABG?
1
2
3

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 4
Ferrarotto Hospital University of Catania
Questions Surrounding Revascularization For
Coronary Artery Disease in Type 2 Diabetes
What are the contemporary outcomes of patients with coronary artery disease and diabetes?
Does the coronary atherosclerotic burden impact on prognosis in diabetes?
Does diabetes independently weigh into decision making for revascularization by PCI or CABG?
1
2
3

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 5
Ferrarotto Hospital University of Catania
Questions Surrounding Revascularization For
Coronary Artery Disease in Type 2 Diabetes
What are the contemporary outcomes of patients with coronary artery disease and diabetes?
Does the coronary atherosclerotic burden impact on prognosis in diabetes?
Does diabetes independently weigh into decision making for revascularization by PCI or CABG?
1

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 6
Ferrarotto Hospital University of Catania
Revascularization versus Medical Therapy 5-Year Outcomes of the BARI-2D Trial (2,368 with T2DM and CAD)
BARI 2D Study Group. N Engl J Med 2009;360:2503-15
12,2
22,8
11,7
24,1
0
10
20
30
40
50
60
Death Death/MI/stroke
Patients
(%
)
Revasc. OMT
P=0.97 P=0.70
10,8
23
10,2
21,1
0
20
40
60
Death Death/MI/stroke
PCI OMT
P=0.92 P=0.70
13,6
22,4 16,4
30,5
0
20
40
60
Death Death/MI/stroke
CABG
P=0.33 P=0.01
PC
I Stra
tum
C
AB
G S
tratu
m

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 7
Ferrarotto Hospital University of Catania
• BARI
• EAST
• RITA
• CABRI
POBA versus CABG
• ERACI II
• ARTS
• SoS
• MASS II
• AWESOME
BMS versus CABG
• CARDIa
• SYNTAX
• FREEDOM
1° Gen. DES versus CABG
• VA CARDS
1°/2° Gen. DES versus CABG
2006-2010 2002-2010 1996-2000 Pre-Stent era
POBA/PCI versus CABG Overview of Trials and Post-Hoc Analyses With Focus on Diabetes

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 8
Ferrarotto Hospital University of Catania
Farkouh ME, et al. N Eng J Med 2012;367:2375-84
Kappetein AP et al. Eur J Cardiothorac Surg. 2013;43:1006-13
SYNTAX DM FREEDOM
Study type Subgroup analysis RCT
Patients, n 452 1,900
Follow up 5 years 5 years
DES PES SES/PES
Age 65.4±9.2 63.1±9.1
Insulin treated Diabetes 40% 32%
Haemoglobin A1c ≥7.0% 57% 64%
Chronic kidney disease 3% 5%
Acute coronary syndromes 30% 31%
EuroSCORE 4 (mean) 1.9 (median)
Coronary lesions 4.6±1.8 5.7±2.2
Left main 29% Excluded
3VD 83% 83%

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 9
Ferrarotto Hospital University of Catania
SYNTAX Trial: Impact of Diabetes at 5 Years All Interaction Terms For Diabetes Status By Treatment Arm = NS
Kappetein AP et al. Eur J Cardiothorac Surg. 2013;43:1006-13
10,9 4,9 3,4 3,5
13,4 15,9 26,3
12,0 7,7 9,9 2,2
22,8 19,8
34,1
0
20
40
60
80
All Death Cardiac Death MI Stroke Revasc. All Death/MI/CVA MACCE
Patients
(%
)
CABG (n=676) TAXUS (n=672)
P=0.48 P=0.035 P<0.001 P=0.15 P<0.001 P=0.069 P=0.002
12,9 6,5 5,4 4,7
14,6 19,1 29,0
19,5 12,7 9,0
3,0
35,3 23,9
46,5
0
20
40
60
80
All Death Cardiac Death MI Stroke Revasc. All Death/MI/CVA MACCE
Patients
(%
)
CABG (n=221) TAXUS (n=231)
P=0.065 P=0.034 P=0.20 P=0.34 P<0.001 P=0.26 P<0.001
Diabetes
Non Diabetes

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 10
Ferrarotto Hospital University of Catania
Farkouh ME, et al. N Eng J Med 2012;367:2375-84
FREEDOM Trial: 5-Year Outcomes Death and MI increased with PCI; 5-Year stroke increased with CABG
PCI CABG P value
All
Death 16.3% 10.9% 0.049
CV
Death 10.9% 6.8% 0.12
MI 13.9% 6.0% <0.001
Stroke 2.4% 5.2% 0.03
18,7
26,5
0
10
20
30
40
CABG PCI
Patients
(%
)
Death/MI/Stroke
P=0.005

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 11
Ferrarotto Hospital University of Catania
FREEDOM Trial: 5-Year Outcomes No Interactions With Insulin Treatment
Dangas G. et al. Presented at TCT 2013
9,3
14,1
4,8
8,6
4,3
7,5
13,5
19
11,9
17,7
1,7 3,7
0
5
10
15
20
25
30
Non Insulin Treated
Insulin Treated Non Insulin Treated
Insulin Treated Non Insulin Treated
Insulin Treated
Pati
en
ts (
%)
CABG PCI
All Death (Pint=0.78) MI (Pint=0.37) Stroke (Pint=0.77)
D +5.2% D +5.1% D +7.1% D +9.1% D -2.6% D -3.8%

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 12
Ferrarotto Hospital University of Catania
Meta-Analysis of CABG vs DES in Patients With Diabetes
2,588 Patients From 4 RCTs
CABG
Events/N
DES
Events/N
CARDIa
FREEDOM
Combined (Random effects)
32/248 37/254
83/761 114/699
146/1308 216/1280
Heterogeneity: Χ2=5.89, df=3, P=0.12, I2=49%
Test for overall effect: P=0.008
Relative Risk
[95% CI]
0.65 [0.48-0.90]
RR [95% CI]
CABG:PCI
1 Favors CABG Favors DES
5-Year (or longest FU) Mortality
SYNTAX DM
VA CARDS (2 year)
26/202 44/226
5/97 21/101
0.89 [0.57-1.37]
0.67 [0.51-0.87]
0.66 [0.42-1.03]
0.25 [0.10-0.63]
Verma et al. Lancet Diabetes 2013 Ahead of Print
DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 13
Ferrarotto Hospital University of Catania
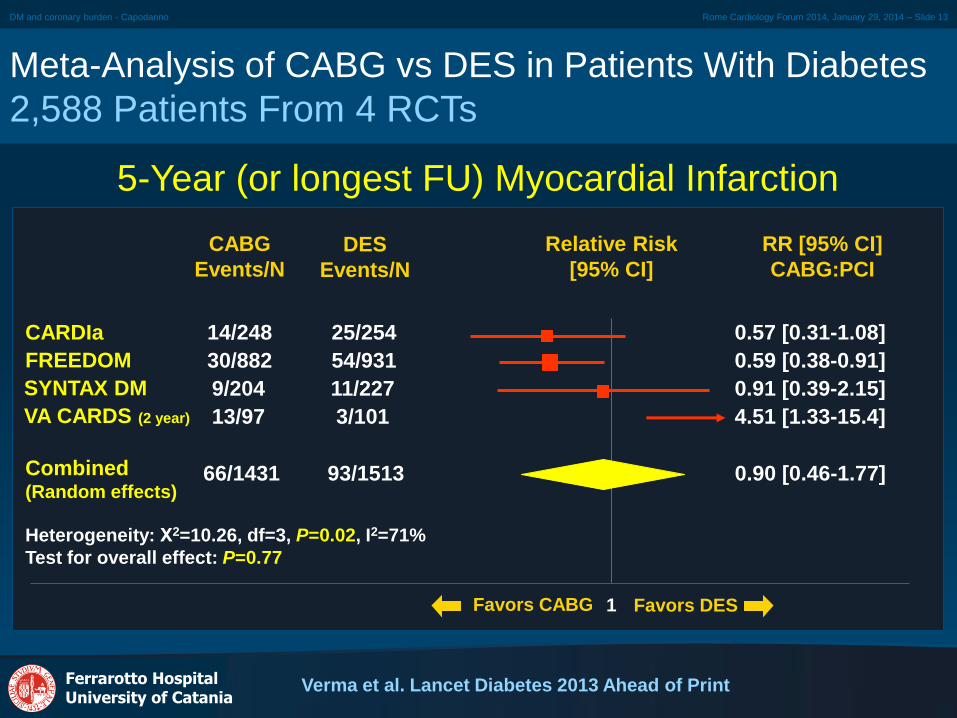
Meta-Analysis of CABG vs DES in Patients With Diabetes
2,588 Patients From 4 RCTs
CABG
Events/N
DES
Events/N
CARDIa
FREEDOM
Combined (Random effects)
14/248 25/254
30/882 54/931
66/1431 93/1513
Heterogeneity: Χ2=10.26, df=3, P=0.02, I2=71%
Test for overall effect: P=0.77
Relative Risk
[95% CI]
0.90 [0.46-1.77]
RR [95% CI]
CABG:PCI
Favors DES
5-Year (or longest FU) Myocardial Infarction
SYNTAX DM
VA CARDS (2 year)
9/204 11/227
13/97 3/101
0.57 [0.31-1.08]
0.59 [0.38-0.91]
0.91 [0.39-2.15]
4.51 [1.33-15.4]
Verma et al. Lancet Diabetes 2013 Ahead of Print
1 Favors CABG
DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 14
Ferrarotto Hospital University of Catania
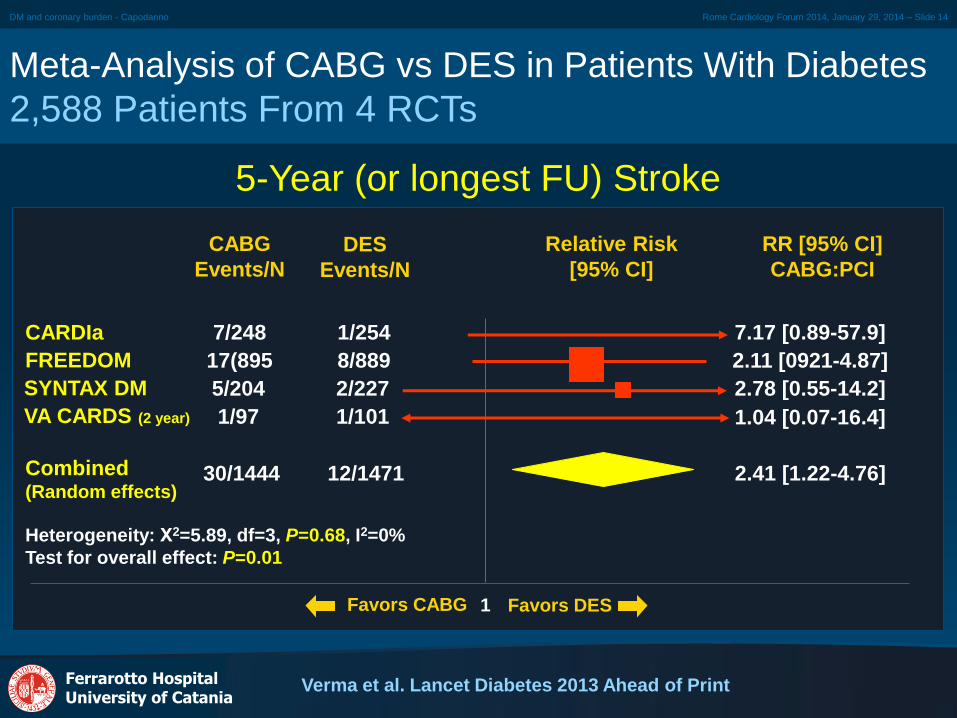
Meta-Analysis of CABG vs DES in Patients With Diabetes
2,588 Patients From 4 RCTs
CABG
Events/N
DES
Events/N
CARDIa
FREEDOM
Combined (Random effects)
7/248 1/254
17(895 8/889
30/1444 12/1471
Heterogeneity: Χ2=5.89, df=3, P=0.68, I2=0%
Test for overall effect: P=0.01
2.41 [1.22-4.76]
RR [95% CI]
CABG:PCI
1 Favors CABG Favors DES
5-Year (or longest FU) Stroke
SYNTAX DM
VA CARDS (2 year)
5/204 2/227
1/97 1/101
7.17 [0.89-57.9]
2.11 [0921-4.87]
2.78 [0.55-14.2]
1.04 [0.07-16.4]
Verma et al. Lancet Diabetes 2013 Ahead of Print
Relative Risk
[95% CI]

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 15
Ferrarotto Hospital University of Catania
Meta-Analysis of CABG vs DES in Patients With Diabetes
2,588 Patients From 4 RCTs
CABG
Events/N
DES
Events/N
CARDIa
FREEDOM
Combined (Random effects)
5/248 30/254
42/875 117/699
71/1424 205/1511
Heterogeneity: Χ2=8.75, df=3, P=0.03, I2=66%
Test for overall effect: P=0.003
Relative Risk
[95% CI]
0.38 [0.23-0.65]
RR [95% CI]
CABG:PCI
Favors DES
5-Year (or longest FU) Revascularization
SYNTAX DM
VA CARDS (2 year)
13/204 46/226
11/97 12/101
0.17 [0.07-0.43]
0.38 [0.27-0.54]
0.31 [0.18-0.56]
0.95 [0.44-2.06]
Verma et al. Lancet Diabetes 2013 Ahead of Print
1 Favors CABG

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 16
Ferrarotto Hospital University of Catania
Why Does CABG Outperforms PCI,
Especially in Diabetes?
Taggart D. Lancet. 2013;381:605-7
• During CABG placing bypass grafts to the mid coronary
vessel has two effects:
1. It makes complexity of culprit lesion irrelevant
2. Over the long term, CABG offers prophylaxis against future culprit
lesions by protecting whole zones of vulnerable proximal
myocardium in diffusely unstable coronary endothelium (especially
diabetes)
• In contrast, PCI with stents only treats suitable localised
proximal culprit lesions but has no prophylactic benefit
against new disease (proximal to, within or distal to the
stent)

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 17
Ferrarotto Hospital University of Catania
Questions Surrounding Revascularization For
Coronary Artery Disease in Type 2 Diabetes
What are the contemporary outcomes of patients with coronary artery disease and diabetes?
Does the coronary atherosclerotic burden impact on prognosis in diabetes?
Does diabetes independently weigh into decision making for revascularization by PCI or CABG?
2

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 18
Ferrarotto Hospital University of Catania
Does the Coronary Burden Modify The
Outcomes of Revascularization? 1. Revascularization versus Medical Therapy
Brooks MM, et al. Circulation. 2012;126:2115-2124
MED
Rate
REV
Rate
Low Risk*
High Risk*
18.3% 20.8%
29.9% 29.7%
Hazard ratio
[95% CI]
Favors REV 1 Favors MED
Death/MI/Stroke MED
N
REV
N
610 694
195 203
Interaction
P value
0.16 PCI Stratum
Low Risk*
High Risk*
25.1% 19.8%
36.8% 24.8%
205 177
180 201
0.26 CABG Stratum
*Based on BARI 2D Angiographic Risk Score

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 19
Ferrarotto Hospital University of Catania
The SYNTAX Score
1 2 3 4 5
6 7 8 9 10
Diameter
reduction
Total
Occlusion
Trifurcation Bifurcations
Severe
tortuosity
Long lesion Heavy
calcification Thrombus
Aorto-ostial
stenosis
Diffuse
disease

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 20
Ferrarotto Hospital University of Catania
The SYNTAX Score
Diameter
reduction
Total
Occlusion
Trifurcation Bifurcations
Severe
tortuosity
Long lesion Heavy
calcification Thrombus
Aorto-ostial
stenosis
Diffuse
disease
• Age >3 months +1
• Blunt stump +1
• Bridging +1
• First segment visible
beyond TO +1/seg.
• SB <1.5mm +1
• SB < & ≥ 1.5mm +1
• 1 segment +3
• 2 segments +4
• 3 segments +5
• 4 segments +6
• Type A,B,C +1
• Type D,E,F,G +2
• Angulation <70 +1
• Total occlusion x5
• Significant lesion
(50-99%) x2
• Aorto-ostial +1
• Aorto-ostial +1 • Severe tortuosity +2 • Length >20mm +1 • Heavy calcification
+1
• Thrombus +1

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 21
Ferrarotto Hospital University of Catania
The SYNTAX Score Forces The
Heart Team To Focus on Anatomy
www.syntaxscore.com
LAD
D1
Ramus
OM1
RCA
L1
(Segment 7): 2.5x2 5
Medina 0,1,0 1
Angulation <70° 1
L2 (Segment 7): 2.5x2 5
Length >20 mm 1
L3 (Segment 9): 1x2 2
Length >20 mm 1
L4 (Segment 12): 1x2 2
Medina 0,0,1 2
L5 (Segment 12a): 1x2 2
Medina 0,0,1 2
L6 (Segment 2): 1x2 2
Total Lesion 1 7
Total Lesion 2 6
Total Lesion 3 3
Total Lesion 4 4
Total Lesion 5 4
Total Lesion 6 2
SYNTAX
Score 26

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 22
Ferrarotto Hospital University of Catania
Risk Stratification By SYNTAX Score
30,6 35,5
34,6
44,7
34,8 19,8
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
SYNTAX DM FREEDOM
Pati
en
ts (
%)
Score 0-22 Score 23-32 Score ≥33
29.0±11.2 26.2 ± 8.6

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 23
Ferrarotto Hospital University of Catania
Does the Coronary Burden Modify The
Outcomes of Revascularization? 2. PCI versus CABG
17,5
22,6 18,2
26,4
21
30,9
0
15
30
45
60
CABG PCI
Pati
en
ts (
%)
Score
0-22
Score
23-32
Score
≥33
Score
0-22
Score
23-32
Score
≥33
Capodanno D. et al. Submitted
5-Year Death/MI/Stroke in Pooled analyses of FREEDOM and SYNTAX DM
P=0.50 P=0.04

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 24
Ferrarotto Hospital University of Catania
Meta-Analysis of PCI vs CABG in LM/MVD And Diabetes
5-Year Risk of Death/MI/CVA
CABG
Events/N
1° Gen DES
Events/N
SYNTAX DM
FREEDOM
Combined (Random effects)
12/74 23/74
44/192 56/182
56/266 79/256
Heterogeneity: Cochran’s Q = 0.98, P=0.32, I2=0%
Test for overall effect: P=0.01
Odds Ratio
[95% CI]
0.52 [0.28-0.97]
0.74 [0.53-1.05]
0.69 [0.51-0.92]
OR [95% CI]
CABG:PCI
1 Favors CABG Favors PCI
High SYNTAX Score (≥33)
Capodanno D. et al. Submitted

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 25
Ferrarotto Hospital University of Catania
Meta-Analysis of PCI vs CABG in LM/MVD And Diabetes
5-Year Risk of Death/MI/CVA
CABG
Events/N
1° Gen DES
Events/N
SYNTAX DM
FREEDOM
Combined (Random effects)
15/70 17/77
72/406 119/438
87/476 136/515
Heterogeneity: Cochran’s Q = 1.36, P=0.24, I2=26%
Test for overall effect: P=0.05
Odds Ratio
[95% CI]
0.97 [0.53-1.79]
0.65 [0.50-0.85]
0.72 [0.51-1.00]
OR [95% CI]
CABG:PCI
1 Favors CABG Favors PCI
Intermediate SYNTAX Score (23-32)
Capodanno D. et al. Submitted

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 26
Ferrarotto Hospital University of Catania
Meta-Analysis of PCI vs CABG in LM/MVD And Diabetes
5-Year Risk of Death/MI/CVA
CABG
Events/N
1° Gen DES
Events/N
SYNTAX DM
FREEDOM
Combined (Random effects)
12/60 14/74
58/340 76/329
70/400 90/403
Heterogeneity: Cochran’s Q = 0.86, P=0.35, I2=0%
Test for overall effect: P=0.09
Odds Ratio
[95% CI]
1.06 [0.53-2.11]
0.74 [0.54-1.00]
0.78 [0.59-1.04]
OR [95% CI]
CABG:PCI
1 Favors CABG Favors PCI
Low SYNTAX Score (0-22)
Capodanno D. et al. Submitted

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 27
Ferrarotto Hospital University of Catania
Questions Surrounding Revascularization For
Coronary Artery Disease in Type 2 Diabetes
What are the contemporary outcomes of patients with coronary artery disease and diabetes?
Does the coronary atherosclerotic burden impact on prognosis in diabetes?
Does diabetes independently weigh into decision making for revascularization by PCI or CABG? 3

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 28
Ferrarotto Hospital University of Catania
Does Diabetes Independently Weigh Into the CABG:PCI
Equation? Treatment Interactions in SYNTAX
Farooq V et al. Lancet. 2013;381:639-50
2
1
0
-1
-2
0 20 40 60
PCI
CABG 2
1
0
-1
-2
No Yes
PCI
CABG
Lo
g H
R
Lo
g H
R
SYNTAX Score Diabetes

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 29
Ferrarotto Hospital University of Catania
The SYNTAX Score II - No Role for Diabetes
Farooq V et al. Lancet. 2013;381:639-50
1 2 3 4
5 6 7 8
SYNTAX
Score
Age Gender Creatinine
clearance
Left main
disease
Chronic
obstructive
pulmonary
disease
Peripheral
artery disease
Left Ventricular
Ejection fraction

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 30
Ferrarotto Hospital University of Catania
1. If I have a patient with diabetes and complex
coronary artery disease, is it useful to calculate the
SYNTAX score for prognostic stratification?
Yes: In pooled analyses of diabetic patients from
SYNTAX and FREEDOM, there was a 8% absolute
risk reduction in death/MI/stroke with PCI and a 4%
absolute risk reduction with CABG between
patients in the highest and lowest angiographic risk
groups.
Diabetes, Coronary Complexity And
Decision-making

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 31
Ferrarotto Hospital University of Catania
2. If I have a patient with diabetes and complex
coronary artery disease, is it useful to calculate the
SYNTAX score II for decision making?
Unknown: SYNTAX included only 452 patients with
diabetes, while the score was derived on a
population that included 75% of patients with no
diabetes. Further validation of the SYNTAX score II
in patients with diabetes from the FREEDOM trial is
ongoing.
Diabetes, Coronary Complexity And
Decision-making

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 32
Ferrarotto Hospital University of Catania
2013 ESC Guidelines On Diabetes, Pre-diabetes
And Cardiovascular Diseases
Rydén L et al. Eur Heart J. 2013;34:3035-87
Optimal medical treatment should be considered as
preferred treatment in patients with stable CAD and
DM unless there are large areas of ischemia or
significant left main or proximal LAD lesions.
IIa B
CABG is recommended in patients with DM and
multivessel or complex (SYNTAX Score >22) CAD to
improve survival free from major cardiovascular
events.
I A
PCI for symptom control may be considered as an
alternative to CABG in patients with DM and less
complex multivessel CAD (SYNTAX score ≤22) in
need of revascularization.
IIb B

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 33
Ferrarotto Hospital University of Catania
Coronary Atherosclerotic Burden And Prognosis
In Type 2 Diabetes: Closing Remarks / 1
1. A quarter of procedures for coronary artery
disease are performed in patients with diabetes
and long-term mortality in these patients is
higher than in patients without diabetes.
2. In patients with stable coronary artery disease
and diabetes, routine revascularization does
not improve survival over first-line medical
treatment, with the exception of CABG in
patients with extensive atherosclerosis.

DM and coronary burden - Capodanno Rome Cardiology Forum 2014, January 29, 2014 – Slide 34
Ferrarotto Hospital University of Catania
Coronary Atherosclerotic Burden And Prognosis
In Type 2 Diabetes: Closing Remarks / 2
3. In patients with MVD and diabetes, revascularization by
CABG rather than PCI is associated with:
A large (-35%) reduction in mortality at long-term
Reduced risk of revascularization at early and long-term
Increased early risk of stroke
4. This benefit seems irrespective of coronary burden and
insulin status.
5. In diabetics who need revascularization, the SYNTAX score
maintains some value in prognostic risk stratification,
especially for PCI, but its utility in decision making between
PCI and CABG is marginal. Whether the SYNTAX Score II
may overcome this limitation is under investigation.