diabetes complications: screening and...
TRANSCRIPT

2015 International Diabetes Center
Diabetes Complications: Screening
and Management
Gregg Simonson, PhD
Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department of Family Practice
Complications Associated with Diabetes
2015 International Diabetes Center
� CVD death 2–4 times higher
� Stroke risk 2–4 times higher
� Hypertension risk 2–3 times higher (present in 75–80%)
� PAD 2 times higher
� Type 2 diabetes is closely linked to obesity (although in some not obvious due to excess central adiposity, i.e. ‛‛metabolically obese, normal weight” [MONW])
Cardiovascular Disease in Type 2 Diabetes
CDC, National Diabetes Fact Sheet, 2011; ADA Web Site
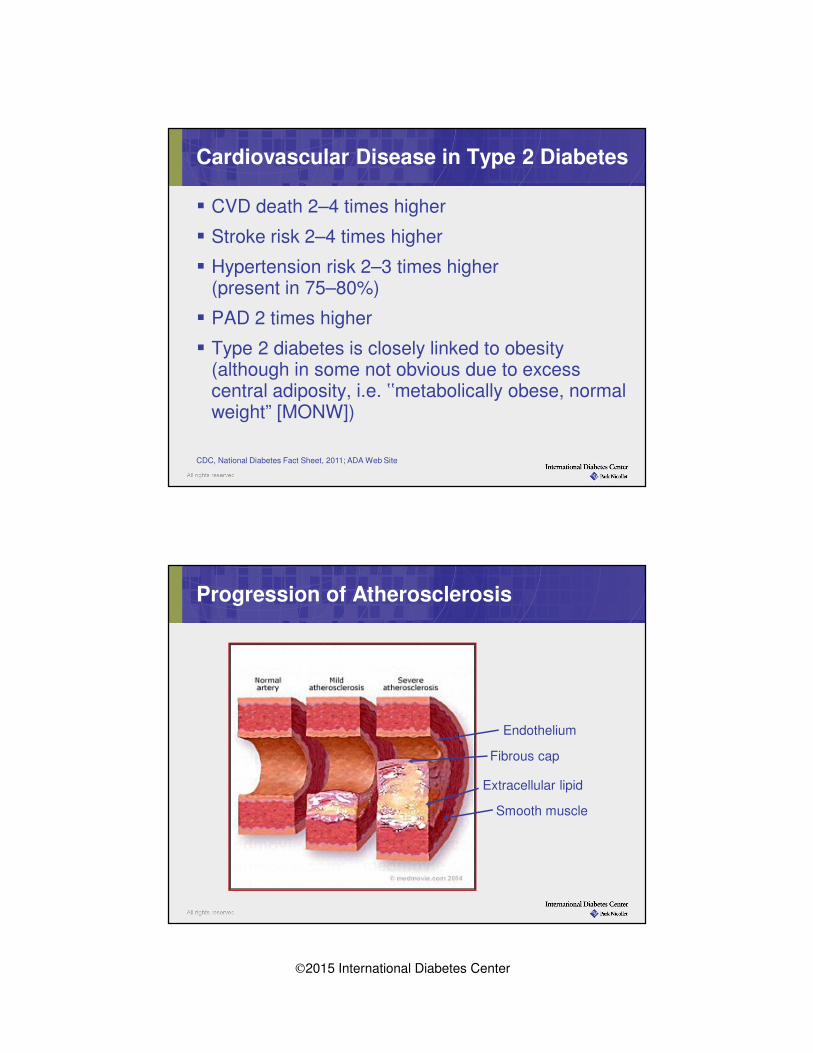
Progression of Atherosclerosis
Endothelium
Smooth muscle
Extracellular lipid
Fibrous cap

2015 International Diabetes Center
Priorities of Care for Adults with Diabetes
Macrovascular ComplicationsMacrovascular ComplicationsASA, tobacco, ACEI/ARB, statin
© 2015 International Diabetes Center.
Diagnosis–PreventionDx A1C ≥6.5%, fasting glucose ≥126 casual ≥ 200 + symptoms
prevent pre-diabetes (IFG-IGT) & metabolic syndrome
Self-Management Knowledge and SkillMonitoring Medication Problem solving Food plan & nutrition
Risk reduction Living & coping Physical activity
Hemoglobin A1C
Target < 7.0%
SMBG
Pre 70-130 mg/dL
Post <180 mg/dL
(~ 50% of readings)
Blood Pressure
(every visit)
Dx and Rx < 140/90
Annual Lipid Profile
LDL < 100
HDL > 40
Trigs < 150
DM + CVD
LDL < 70
Annual Screening
NephropathyMicroalbumin screening
Calculated GFR
RetinopathyDilated retinal exam
NeuropathyNeuro and foot exam
Sexual health
Hospital care
Foot care
Dental care
Immunizations
Glucose HypertensionLipidsMicrovascularcomplicationsMicrovascularcomplications
Other essentialsOther essentialsof care
?
ADA LDL Cholesterol Targets 2014 vs. 2015
ADA Clinical Practice Recommendations, Diabetes Care 2014; 37
Suppl 1.; ADA Standards of Medical Care. Diab Care 2015; 38 Suppl 1
LDL-C<100 mg/dL
LDL-C<70 mg/dL
LDL-C Goal Diabetes
LDL-C Goal Diabetes + CVD
2014
No target
No target
LDL-C Goal Diabetes
LDL-C Goal Diabetes + CVD
2015

2015 International Diabetes Center
Rationale
� Statin therapy benefits most diabetes patients
� No LDL targets, consistent with 2013 AHA/ACC recommendations
2015 ADA Dyslipidemia Management Recommendations
ADA Standards of Medical Care. Diab Care 2015; 38 Supplement 1
Statins are Expectant Therapy in Diabetes
� Rosuvastatin (Crestor), Atorvastatin (Lipitor), Simvastatin (Zocor), Pravastatin (Pravachol), Lovastatin, Pitavastatin (Livalo), Fluvastatin
� Most powerful LDL lowering agents
– 50% + reduction from baseline
� Increases HDL ~5-15% and lowers triglycerides ~15-25%
� May cause muscle pain (myopathy)
� Associated with modest increased risk for diabetes (10-25%), yet CV benefit outweighs risk
Ridker et al., Lancet. 2012;380:565-571.
2015 International Diabetes Center
1. Individuals with clinical ASCVD (ACS, MI, angina, revascularization, stroke, TIA, PAD)
2. Individuals with LDL-C ≥190 mg/dL
3. Individuals 40-75 years of age with diabetes and LDL-C 70-189 mg/dL
4. Individuals without clinical ASCVD or diabeteswho are 40-75 years of age and LDL-C 70-189 mg/dL and 10 year ASCVD risk ≥ 7.5%
4 Statin Benefit Groups
Stone et al, Circulation 2013: Published Online Stone et al., Circulation. 2013; Nov Online.

2015 International Diabetes Center
Source: S. E. Nissen et al. , JAMA 2004; 291:1071-80.
Can statins reverse atherosclerosis?
Intravascular Ultrasound Images at Baseline and Follow-up
Answer: Yes in some patients and stops progression in others.Results of the Reversal of Atherosclerosis with Aggressive Lipid Lowering (REVERSAL) study
Combination Therapy for Dyslipidemia
Rationale
�ACCORD trial showed the addition of fenofibrate to statin therapy did not reduce CV events compared to statin therapy alone
�AIM-High trial was stopped early due to lack of CV benefit of adding niacin to statin therapy vs. placebo
ADA Standards of Medical Care. Diab Care 2015; 38 Supplement 1

2015 International Diabetes Center
Priorities of Care for Adults with Diabetes
Macrovascular ComplicationsMacrovascular ComplicationsASA, tobacco, ACEI/ARB, statin
© 2015 International Diabetes Center.
Diagnosis–PreventionDx A1C ≥6.5%, fasting glucose ≥126 casual ≥ 200 + symptoms
prevent pre-diabetes (IFG-IGT) & metabolic syndrome
Self-Management Knowledge and SkillMonitoring Medication Problem solving Food plan & nutrition
Risk reduction Living & coping Physical activity
Hemoglobin A1C
Target < 7.0%
SMBG
Pre 70-130 mg/dL
Post <180 mg/dL
(~ 50% of readings)
Blood Pressure
(every visit)
Dx and Rx < 140/90
Annual Lipid Profile
LDL < 100
HDL > 40
Trigs < 150
DM + CVD
LDL < 70
Annual Screening
NephropathyMicroalbumin screening
Calculated GFR
RetinopathyDilated retinal exam
NeuropathyNeuro and foot exam
Sexual health
Hospital care
Foot care
Dental care
Immunizations
Glucose HypertensionLipidsMicrovascularcomplicationsMicrovascularcomplications
Other essentialsOther essentialsof care
?
Measure
Blood
Pressures
Accurately
What’s wrong with
this picture?
2015 International Diabetes Center
American Diabetes Association HTN Management Recommendations
� Systolic BP treatment target of <140 mmHg
– Lower systolic BP target of <130 mmHg for certain individuals (e.g. younger patients without undue treatment burden)
� Diastolic BP target <80 mmHg
� Treatment recommendations:
– Lifestyle changes including weight loss, DASH diet, reduced sodium, increased physical activity
– ACE inhibitor or ARB as first-line therapy
– Multiple medications often needed to achieve BP target, administer one or more at bedtime
ADA Clinical Practice Recommendations. Diabetes Care, 2014; 37:Suppl.1.
JNC 8 Guidelines are not without controversy
1. Not endorsed by any large professional association (e.g. ACC/AHA)
2. Not all panel members agreed with raising SBP >150 mmHg in
individuals ≥60 years
3. May cause initiation of pharmacotherapy too early in “low risk”
individuals

2015 International Diabetes Center
JNC 8 Recommendations for Individuals with Diabetes
� In individuals ≥18 years, initiate pharmacologic treatment when BP ≥140/90 mmHg and treat to goal BP <140/90 mmHg
� In the general nonblack population initial pharmacotherapy treatment should be:
– Thiazide diuretic
– Calcium channel blocker
– ACE-I or ARB
� In the general black population initial pharmacotherapy treatment should be:
– Thiazide diuretic or calcium channel blocker
James et al. JAMA, 2013; Published Online Dec 18th.
Role of Intensive BP Control in DiabetesResults of the ACCORD BP Study
ACCORD Study Group, N Engl J Med. 2010.
•Average 3.4 antihypertensive medications in intensive vs. 2.2 in standard care
•Serious adverse events occurred 3.3% intensive vs. 1.3% standard care
•What is the appropriate BP target in type 2 diabetes???
119 mmHg
133.5 mmHg
2015 International Diabetes Center
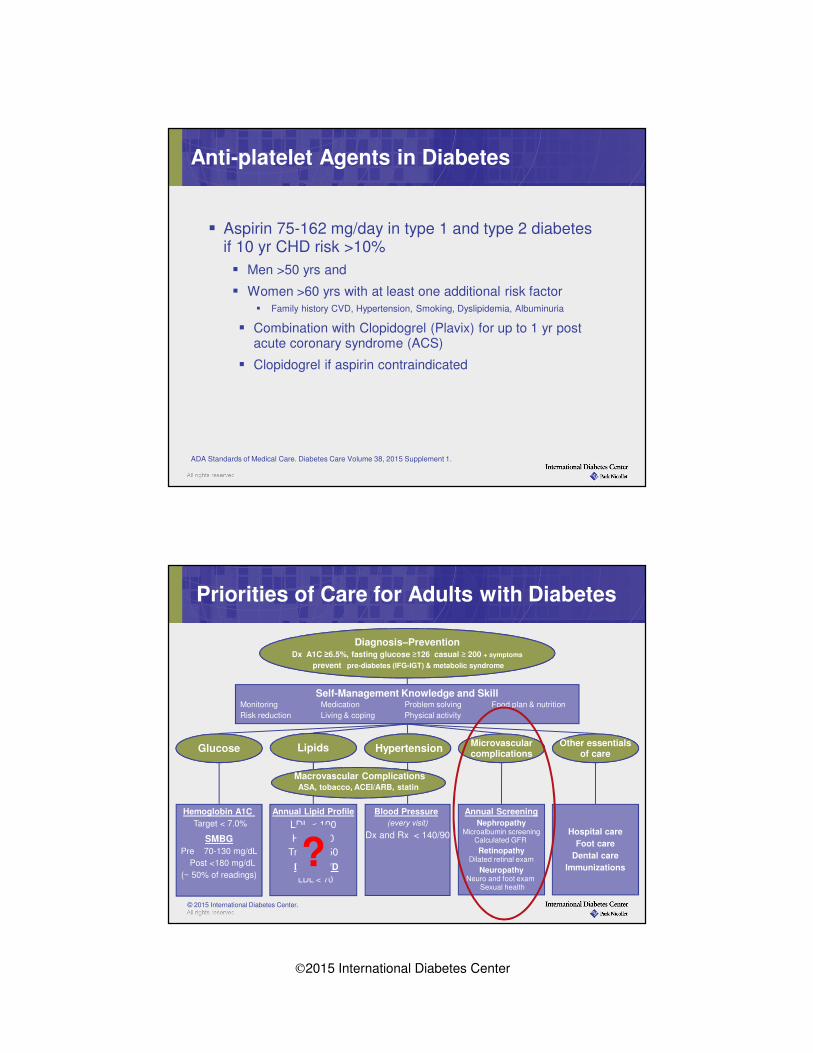
Anti-platelet Agents in Diabetes
� Aspirin 75-162 mg/day in type 1 and type 2 diabetes if 10 yr CHD risk >10%
� Men >50 yrs and
� Women >60 yrs with at least one additional risk factor
� Family history CVD, Hypertension, Smoking, Dyslipidemia, Albuminuria
� Combination with Clopidogrel (Plavix) for up to 1 yr post acute coronary syndrome (ACS)
� Clopidogrel if aspirin contraindicated
ADA Standards of Medical Care. Diabetes Care Volume 38, 2015 Supplement 1.
Priorities of Care for Adults with Diabetes
Macrovascular ComplicationsMacrovascular ComplicationsASA, tobacco, ACEI/ARB, statin
© 2015 International Diabetes Center.
Diagnosis–PreventionDx A1C ≥6.5%, fasting glucose ≥126 casual ≥ 200 + symptoms
prevent pre-diabetes (IFG-IGT) & metabolic syndrome
Self-Management Knowledge and SkillMonitoring Medication Problem solving Food plan & nutrition
Risk reduction Living & coping Physical activity
Hemoglobin A1C
Target < 7.0%
SMBG
Pre 70-130 mg/dL
Post <180 mg/dL
(~ 50% of readings)
Blood Pressure
(every visit)
Dx and Rx < 140/90
Annual Lipid Profile
LDL < 100
HDL > 40
Trigs < 150
DM + CVD
LDL < 70
Annual Screening
NephropathyMicroalbumin screening
Calculated GFR
RetinopathyDilated retinal exam
NeuropathyNeuro and foot exam
Sexual health
Hospital care
Foot care
Dental care
Immunizations
Glucose HypertensionLipidsMicrovascularcomplicationsMicrovascularcomplications
Other essentialsOther essentialsof care
?

2015 International Diabetes Center
Microvascular Complications of Diabetes:From Head to Toe
Eye�Retinopathy�Cataracts�Glaucoma�Visual Impairment
KidneyNephropathy� Microalbuminuria� Macroalbuminuria� Renal insufficiency/failure
Nerves Neuropathy� Peripheral/Central� Autonomic
Complications Risk in Diabetes
0
2
4
6
8
6 7 8 9 10 11 12A1C (%)
Rel
ati
ve
Ris
k
of
Co
mp
lica
tio
ns
Adapted from: Skyler JS. Endocrinol Metab Clin North Am. 1996 Jun;25(2):243-54.
DCCT Study Group. N Engl J Med 329:977, 1993
UKPDS 35. Stratton IM. BMJ 321:405-412, 2000.
120 150 180 210 240 270 300Average Glucose
Lowering blood glucose significantly
reduces the risk of microvascular
complications
In both Type 1 and Type 2 diabetes
2015 International Diabetes Center
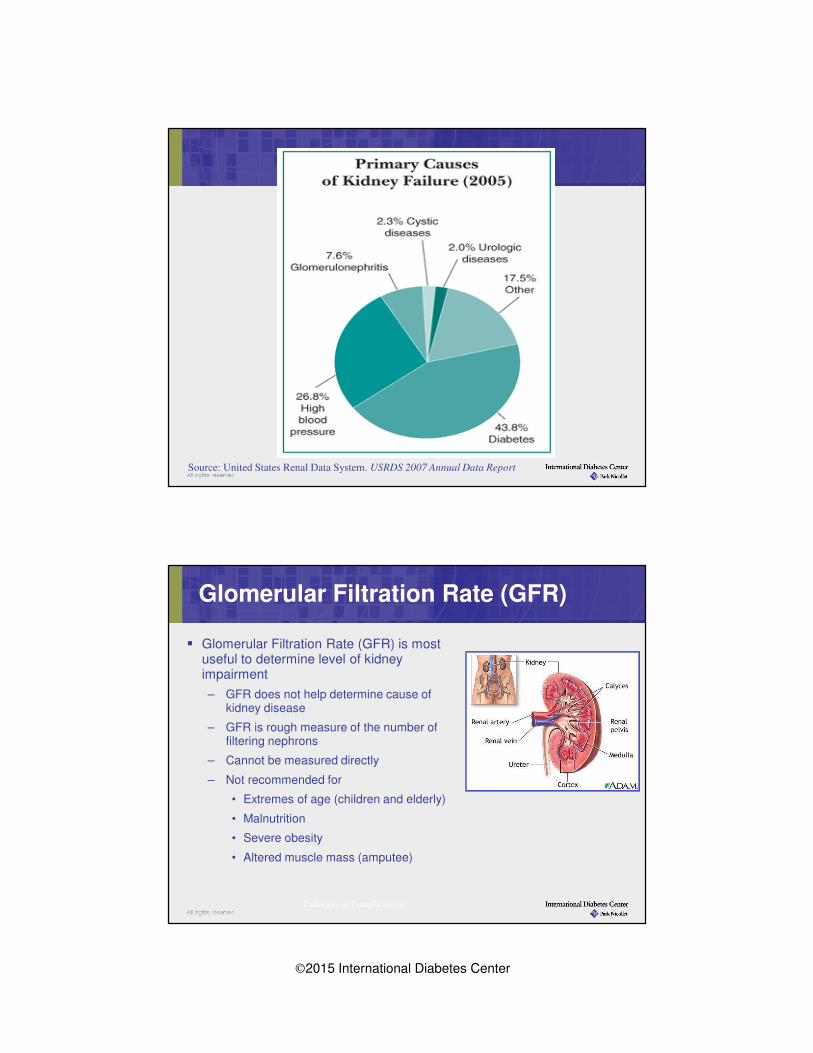
Source: United States Renal Data System. USRDS 2007 Annual Data Report
Glomerular Filtration Rate (GFR)
� Glomerular Filtration Rate (GFR) is most useful to determine level of kidney impairment
– GFR does not help determine cause of kidney disease
– GFR is rough measure of the number of filtering nephrons
– Cannot be measured directly
– Not recommended for
• Extremes of age (children and elderly)
• Malnutrition
• Severe obesity
• Altered muscle mass (amputee)
Pathways to Complications

2015 International Diabetes Center
Stages of Chronic Kidney Disease (CKD)
Stage eGFR
(ml/min/1.73 m2)
Description Action
1 >90 Normal or higher
GFR w. evidence of
kidney disease
Dx and Rx of co-
morbidities
2 60-89 Mild decrease in
GFR
Monitor progress and
Rx co-morbidities
3
3a
3b
30-59
45-59
30-44
Moderate decrease
in GFR
Monitor progress and
Rx co-morbidities and
consider referral
4 15-29 Severe decrease in
GFR
Pre ESKD, prepare pt.
for dialysis
5 <15 Kidney failure Dialysis or
replacement
Am J Kid Dis 2002 39:S1-266
CKD defined as Stage 3 or higher for 3 months or more
CKD
Bakris, GL Mayo Clin Proc 2011 86:444-456
Screening Recommendations
Nephropathy
� Annual microalbuminuria screen
� Albumin/creatinine (A/C) ratio preferred
� Annual serum creatinine/calculate eGFR
Type 1 Diabetes
� After 5 years duration; annually thereafter
Type 2 Diabetes
� At diagnosis; annually thereafter
American Diabetes Association Clinical Practice Recommendations. Diabetes Care 2011; Suppl 1.
2015 International Diabetes Center
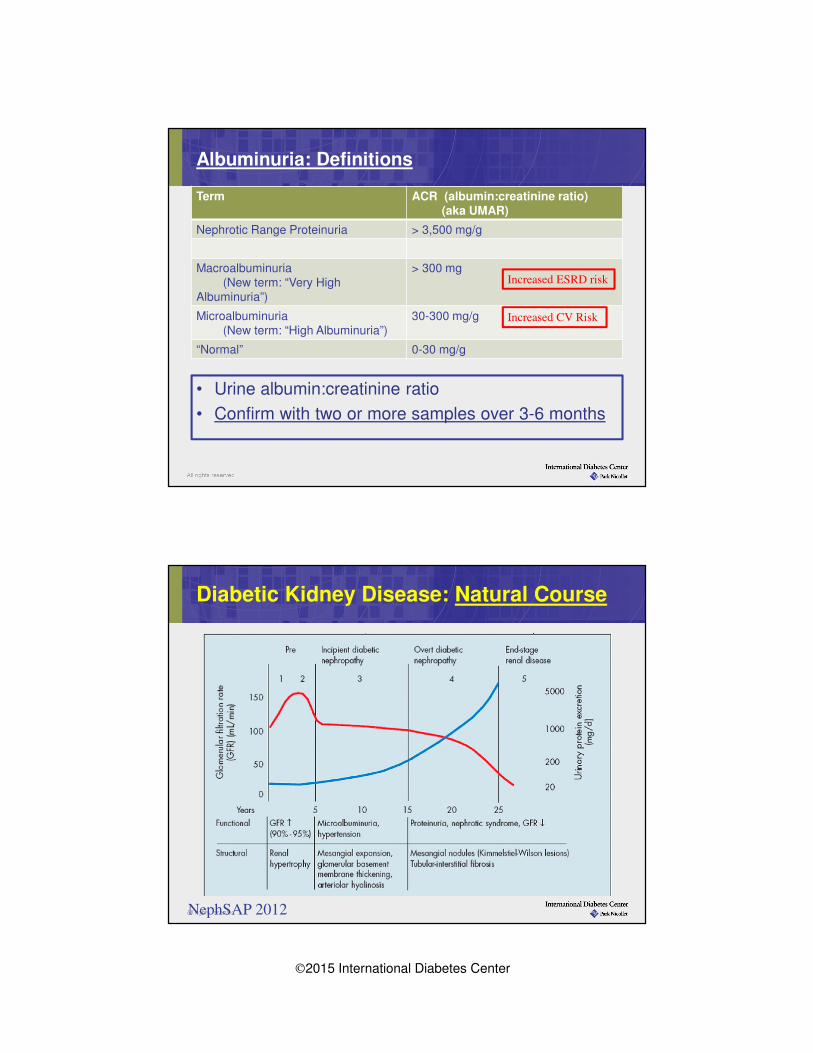
Albuminuria: Definitions
Term ACR (albumin:creatinine ratio)(aka UMAR)
Nephrotic Range Proteinuria > 3,500 mg/g
Macroalbuminuria(New term: “Very High
Albuminuria”)
> 300 mg
Microalbuminuria(New term: “High Albuminuria”)
30-300 mg/g
“Normal” 0-30 mg/g
Increased CV Risk
Increased ESRD risk
• Urine albumin:creatinine ratio
• Confirm with two or more samples over 3-6 months
Diabetic Kidney Disease: Natural Course
NephSAP 2012

2015 International Diabetes Center
Treatment of Diabetic Nephropathy
� Glucose control
� A1C <7% delays onset of albuminuria- individualize target for pt safety
� Smoking cessation
� Low protein diet (0.8 g/kg/day)
� Improves renal function (e.g. slows increase in albumin level, decline in GFR, and occurrence of ESRD)
� Results conflicting, might be considered in patients whose nephropathy is progressing despite optimal glucose and BP control
� ASA/Lipids
� All patients with persistent albuminuria should be Rx with ASA and statins
� Consider ASA and statins in all patients with eGFR <60 ml/min
� Fenofibrate may further reduce albuminuria (ACCORD-LIPID) but can increase serum creatinine
Treatment of Diabetic Nephropathy
Blood pressure control:
� <140/90 mmHg
� Can consider lower target e.g. <130/80 mmHg if significant proteinuria
� Start ACE Inhibitor(ACE-I) or Angiotensin II Receptor
Blocker (ARB) � Baseline creatinine and K+, repeat in 1-2 weeks
� Titrate dose to maximum approved hypertension dose if can be achieved safely
� Monitor A/C ratio to assess response to therapy and progression of disease
� Similar BP control and kidney protection actions
� May need multiple BP medications to reach goal
� UKPDS 30% pts with 3 or more drugs

2015 International Diabetes Center
Scope of Diabetic Retinopathy (DR)
� After 20 years of diabetes-Evidence of retinopathy in almost all patients with type 1 DM, 60-85% with type 2 DM
� Leading cause of new cases of blindness among adults aged 20-74 years
� Detecting and treating diabetic eye disease with laser can reduce the development of severe vision loss by 50-60%
National Diabetes Fact Sheet, US 2011
Bressler etal. NEJM 2011: 365; 1520-1526
Non-Proliferative DR Diabetic Macular Edema Proliferative DR
Microvascular damage• Chronic, occurring over years
• Typically no significant vision loss,
but progresses to DME and/or PDR
• Similar damage occurs in other
end-organ vascular beds
Swelling in central retina• Accounts for most vision loss
• Clinically significant ME (CSME)
involves or threatens the fovea
• Co-exists with any level of DR
End stage• Neovascularization of retina
• High risk of severe visual loss
Classification of Diabetic Retinopathy
More common
Less severeLess common
More severe

2015 International Diabetes Center
Normal RetinaEarly Nonproliferative
Retinopathy
Proliferative Retinopathy
Optic nerve
Macula
Hard exudates
Hemorrhage
Neovascularization

2015 International Diabetes Center
American Academy of OphthalmologyRecommended Eye Examination Schedule for Patients with Diabetes Mellitus
• 40-50% do not receive recommended eye care (NCQA, 2009)
• Joslin study of patient self-awareness of DR (ARVO, 2011; n=3100)
• 93% of patients with DR and 63% with vision-threatening DR were unaware they had any DR
• 83% with vision-threatening DR had no scheduled follow-up eye exam
Diabetes Type Recommended Time
For First Examination
Recommended
Follow-up
Type 1 3-5 years after diagnosis Yearly
Type 2 At time of diagnosis Yearly
American Academy of Ophthalmology Retina Panel. Preferred Practice Pattern® Guidelines.
ARVO = The Association for Research in Vision and Ophthalmology ; NCQA = National Committee for Quality Assurance.
Retinopathy: What We Know & What We Are Learning
We Know – The following are critical:• Regular eye check ups
• Glucose control
• Blood pressure control
• Smoking cessation
• Laser treatment gold-standard Rx for PDR
• ASA safe in DR
• Women planning or pregnant should have prompt eye exam with follow-up
We Are Learning:• ACE/ARB’s may slow progression of retinopathy
• Fenofibrate may slow progression of retinopathy (30-40%) -FIELD and ACCORD-EYE
• VEGF inhibitors with prompt or deferred laser gold-standard Rx for diabetic macular edema (DME)

2015 International Diabetes Center
Classifications of Diabetic Neuropathy
� Diabetic Peripheral Neuropathy (DPN)
� Diabetic Autonomic Neuropathy (DAN)
– Cardiac
– Gastrointestinal (gastroparesis)
– Genitourinary (bladder and sexual dysfunction)
– Sudomotor and metabolic (hypoglycemia unawareness)
� Focal
– Cranial (i.e. Bell’s Palsy)
– Truncal /Limb Plexopathy or Mononeuropathy (i.e “foot drop”)
– Diabetic Amyotrophy or Lumbosacral Radiculopathy
– Nerve Entrapment syndromes (i.e. Carpal Tunnel)
Autonomic Nervous system
2015 International Diabetes Center
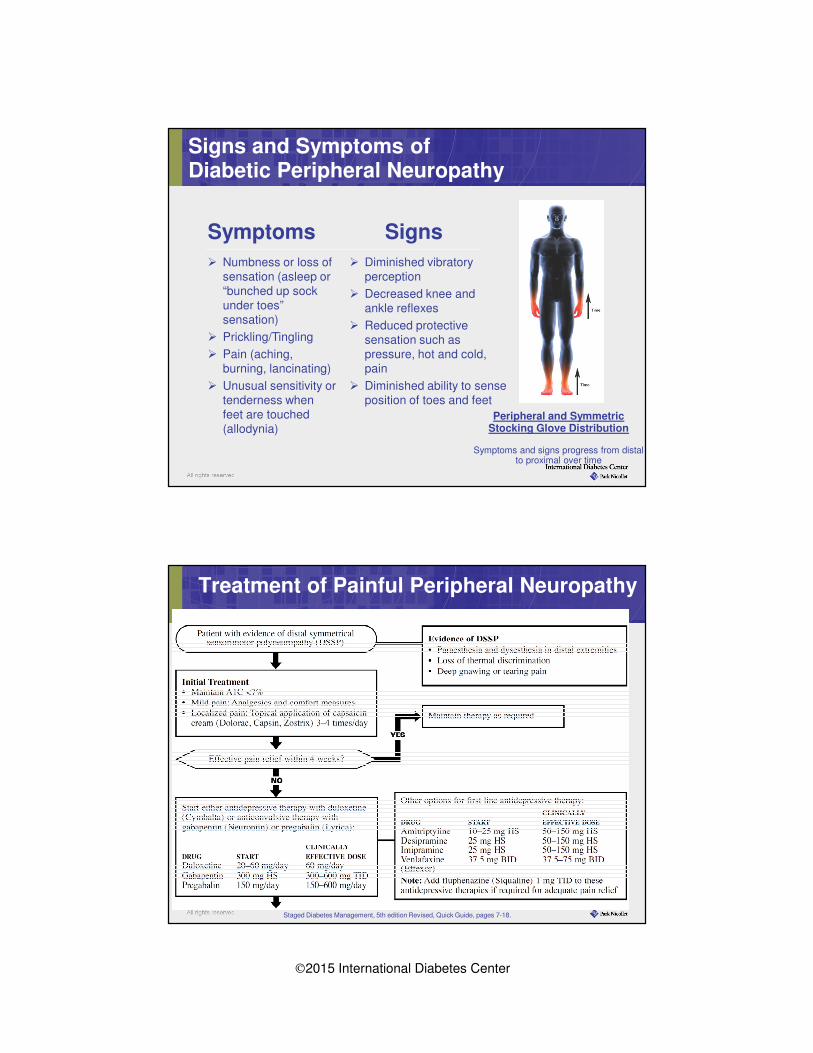
Signs and Symptoms ofDiabetic Peripheral Neuropathy
Symptoms
� Numbness or loss of sensation (asleep or “bunched up sock under toes” sensation)
� Prickling/Tingling
� Pain (aching, burning, lancinating)
� Unusual sensitivity or tenderness when feet are touched (allodynia)
Signs
� Diminished vibratory perception
� Decreased knee and ankle reflexes
� Reduced protective sensation such as pressure, hot and cold, pain
� Diminished ability to sense position of toes and feet
Peripheral and Symmetric Stocking Glove Distribution
Symptoms and signs progress from distal to proximal over time
Treatment of Painful Peripheral Neuropathy
Staged Diabetes Management, 5th edition Revised, Quick Guide, pages 7-18.

2015 International Diabetes Center
The Foot Examination
Careful inspection
� Skin, shoes, shape of foot
Vascular integrity
� Pulses
� Capillary refill
� Ankle-Brachial Pressure Index (ABI, if indicated)
Neurological examination and function
� Light touch (5.07/ 10g monofilament)
� Vibratory sensation (128-Hz tuning fork)
� Reflexes
Source: Staged Diabetes Management, 5th edition, Quick Guide, pages 7-26.
Standards of Care at Diagnosis & Annually
Foot Ulcer
2015 International Diabetes Center
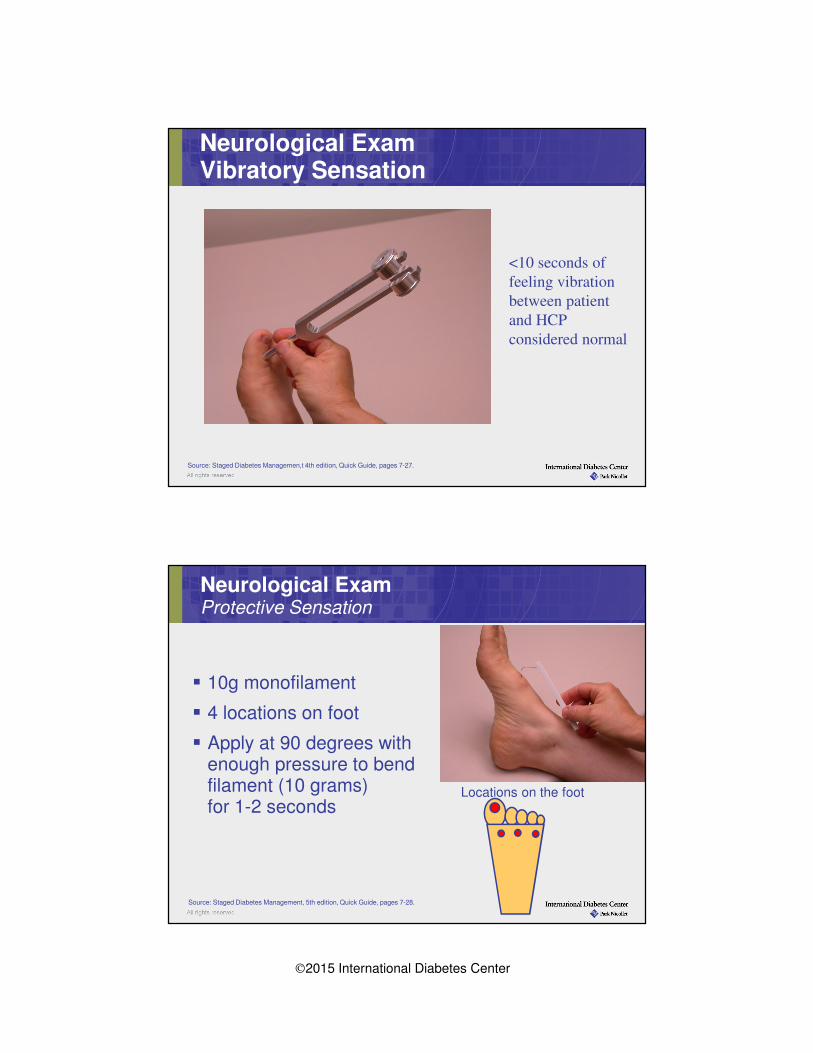
Source: Staged Diabetes Managemen,t 4th edition, Quick Guide, pages 7-27.
Neurological ExamVibratory Sensation
<10 seconds of
feeling vibration
between patient
and HCP
considered normal
Source: Staged Diabetes Management, 5th edition, Quick Guide, pages 7-28.
Neurological ExamProtective Sensation
� 10g monofilament
� 4 locations on foot
� Apply at 90 degrees with enough pressure to bend filament (10 grams) for 1-2 seconds
Locations on the foot