diabetes medicationsdiabetes medications and insurance companies •every insurance company has a...
TRANSCRIPT
Diabetes Medications
Transforming Diabetes Care –
Changes and Choices
April 18, 20151

Objective
Discuss New diabetes medications and their role in
treatment
Conflict of InterestI have no conflict of Interest
2

Diabetes
• 40-50% of the US Population is expected to
develop Diabetes in their lifetime.
• If type 2 diabetes were a country it would be
the 3rd largest in the world.
• 90% of the tasks of diabetes management are
done at home by the patient – we better do a
good job of education. 3

Diabetes Medications and
Insurance Companies
• Every Insurance Company has a Formulary
• Tells you what medications they will pay for.
• And they all have this statement “this list of medications may change at any moment without warning or notice”.
• Be alert for the patient who has just changed insurance companies
• They usually don’t know what the new company (or their current insurance company) will pay for. Meters, test strips, meds, pumps, type of insulin.
4

The 1st Line Treatment for
Diabetes
• Lifestyle changes• Decrease weight
• Recommend to lose 7-10% of current weight, if overweight
• Increase exercise
• Recommend 150 minutes per week
• Maintain the first two.
5

6

7
8
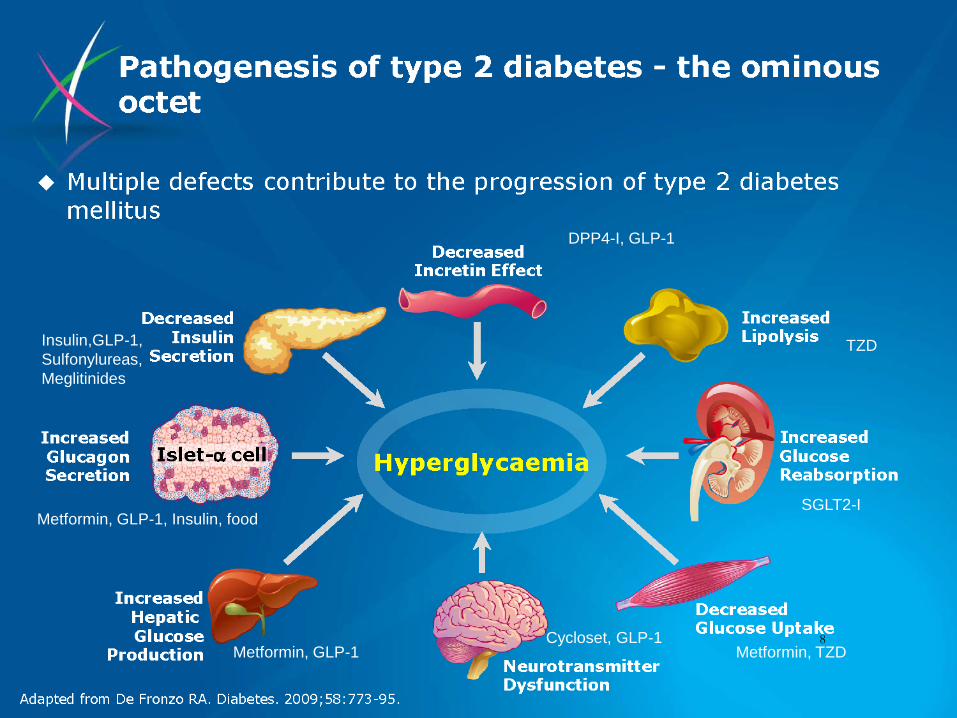
DPP4-I, GLP-1
TZD
SGLT2-I
Metformin, TZDCycloset, GLP-1
Metformin, GLP-1
Metformin, GLP-1, Insulin, food
Insulin,GLP-1,
Sulfonylureas,
Meglitinides

Stimulates production of Insulin
Sulfonylurea
• Glipizide, Glyburide, Glimipride
• Glucotrol, Glynase, Diabeta, Micronase, Glucotrol XL,
• $4 / Month pill
• Low blood sugar
• Nausea / vomiting
• Hypoglycemia is the biggest concern.
9

Insulin Sensitizer/Decreases
effect of Glucagon - Metformin
Biguanide• Glucophage, Glucophage XR, Fortamet, Riomet
• Decreases the liver’s glucose production – from inappropriate glucagon release
• Opens the cell and allows the body to use the insulin more efficiently – increases sensitivity.
• GI upset, diarrhea, gas - 30% of people will have this, of that 30% will have to stop the pill. Formulation change?
• Check the Creatinine >1.4 in women & >1.5 in men.
• Stop 24 hours before & after dye test. The most important is after the dye. 12 hour half life.
10

Insulin Sensitizer - Metformin
• Use with caution in people with liver or kidney
problems.
• Take the pill with food to help decrease Gas and
decrease irritation to stomach.
• Used in PCOS to break the insulin resistance along
with lifestyle changes. .
• $4 / month pill
11

Insulin Sensitizer -Thiazolidinedione
TZD
• Actos (Pioglitazone), Avandia (Rosiglitazone)
• Works at peripheral cells to help open the cells
and allow the body to use the insulin more
efficiently
• Watch for edema, weight gain (sodium shift)
12

Insulin Sensitizer TZD’s
• Also may be used in PCOS.
• Might be effective in diabetes prevention
• Big controversy with Avandia so you won’t see this used much. It is on the market.
13

Insulin Stimulator
Meglitinade Insulin Secretagogue
• Prandin (Repaglinide), Starlix (Nagletinide)
• Take at the beginning of each meal
• Works for 2 hours after taken
• Low blood sugar
• The problem with these pills is you have to take them at the beginning of the meal, since it works for 2 hours. People would forget.
14

Alpha Glucosidase Inhibitor
• Precose, Glyset
• These drugs work in the intestines to slow the digestion of some carbs so that after meal blood sugar peaks are not so high.
• Take at the START of each meals
• GI upset, GAS, abdominal pain very common
• Hypoglycemia must be treated with pure glucose tabs, gel or milk as food absorption is delayed.
• You have to take this with the first bite of food –patients always forgot.
15

DPP-4 Inhibitors
• Blocks the DPP4 enzyme so native GLP-s is not degraded, allows GLP-1 to stimulate insulin producation
• Does not interfere with any other medications or foods. This is an enzyme
• Caution using in patients with history of pancreatitis or medulary thyroid cancer
• New study found this has not happened.
16

DPP-4
• Januvia (Sitagliptin)
• Onglyza (Saxagliptin)
• Tradgenta (Linagliptin)
• Nesina (Alogliptin)
17

SGLT – 2 Inhibitor
• Normally the kidney
reabsorb glucose primarily
via SGLT2, sodium-glucose
co-transporter 2,
protein located in the proximal
tubule of the nephron.
• By inhibiting SGLT2,
these medications block
reabsorption of glucose thereby
increasing urinary glucose excretion.
18

Selective Sodium-Glucose
Transporter
• The patient excretes more glucose through the kidneys out the urinary tract
• Will be glucosuria
• Patient may lose 300 calories/day, may decrease BP
• Side effects
• Vaginal infections,
• UTI
• Volume depletion19

SGLT – 2 Inhibitor
• Invokana (canagliflozin)
• Farxiga (dapagliflozin)
• Jardiance (empagliflozin)
20

SGLT-2 Inhibitors and Kidney
Function
• Estimated Glomerular Filtration Rate/Kidney
Disease
• GFR > 60 – Great, no problem using the pills
• GFR 45 to 60 – Use the lower dose
• GFR < 45 – Avoid the meds (although some company’s
will say “use with caution” consider a safer alternative.
• If GFR down to 30’s need a nephrologist.
21

Medications
Some pills are in combination
• ActoPlus Met – Actos and Metformin
• Avandamet – Avandia & Metformin
• Avandaryl - Avandia and Amaryl
• Duetact – Actos and Glimepiride
• Glucovance – Glyburide & Metformin
• Metaglip – Glipizide & Metformin
• Prandimet – Prandin and Metformin 22

Newer Combination Pills
• Janumet – Januvia and Metformin IR and ER
• Kombiglyze – Onglyza and Metformin ER
• Jentadueto – Tradjenta and Metformin
• Kazano – Alogliptin and Metformin
• Oseni – Alogliptin and Metformin
• Invokamet – Invokana and Metformin
• Xigduo XR – Farxiga and Metformin ER
• Glyxambi – Jardiance and Tradjenta 23

Amylin Symlin
• Symlin – (Pramlintide)
• Amylin is a hormone made in the beta cells.
• Amylin deficiency can make it harder to control glucose levels after meals.
• Reduces fluctuations of blood sugar
• Used with type 1 or 2 at every meal.
• Must eat 250 calories or 30 grams of carbs
• Watch for hypoglycemia
• Problem: Cost and so many shots24

Glucose Like Peptide – 1
GLP-1
• Replaces the GLP-1 hormone that is not being made or used. Responsible for the “incretin effect” 50-70% of insulin release with a meal
• Decreases glucagon release
• Slows gastric emptying
• “Satiety” hormone, helps people feel full faster
• People feel full longer, decrease food intake
• Nausea – transient, or with high fat meal25

GLP-1 - Replaces/Enhances
GLP-1
• Byetta (Exenatide) -Twice a day (2005)
• Victoza (Liraglutide) - Once a day
• Bydureon (Exenatide XR) - Once a week
• Tanzeum (Albiglatide) - Once a week
• Trulicity (Dulaglutide) - Once a week
26

Insulin
Replaces what the body
can not make enough of
or does not use properly
27

Cost of Insulin
• Sometimes this is the barrier for patients
• Insulin can cost $435 or more/vial
• NPH / Regular / Reli-On Brand cost $25-35/vial
• Sometimes skipping medications is cost related –
always ask them.
• Patient Assistant Programs
• Use of Free or Reduced Drug Cards
28

Medications - Insulin
• Insulin is divided into four categories
1. Long Acting – Lantus, Levemir
2. Intermediate Acting – NPH (cloudy insulin)
3. Short Acting - Regular
4. Very Short Acting – Humalog / Novolog / Apidera
• All Insulin is now made in laboratories, not from animals
29

Rapid Acting
Humalog / Novolog / Apidra
• Onset 5 to 15 minutes.
• Given at the meal to “cover” the food at the
meal.
• Peak action is 1 hour.
• Duration is 2-3 hours.
30

Rapid Acting
Humalog / Novolog / Apidra
• Is Used in the Insulin Pump.
• Is used in the V-GO
31

Inhaled Insulin Afrezza
• A rapid acting inhaled insulin
Inhaled powder delivered using a small, discreet and easy to use inhaler – looks like a whistle.
• Administer at the start of the meal.
• Afrezza disolves instantly upon inhalation to the deep lung and delivers to blood stream – OK to use if you have a cold, allergies. Lung clearance very good.
• Peak insulin levels are achieved within 12 to 15 minutes of administration, and decline to baseline by approximately 180 minutes.
• Must be used in combination with a long acting insulin.
• Must have Baseline Spirometry before starting this medication.32

Fast Acting
Regular
• Onset 30 minutes, so should be given 30 minutes before a meal.
• Peak action is 1 – 3 hours.
• Duration is 5 to 6 hours.
• Main uses • Patient with Gastroparesis
• Patient with 24 hour tube feedings
• IV Insulin – 5 minute half life
33

Intermediate Acting
NPH
• Onset 1-1 ½ hours
• Peak is 6 – 10 hours
• Duration is 12 – 16 hours
• Generally given at breakfast and bedtime
• Cloudy insulin – Be sure to mix thoroughly.
• May be used in pregnancy – generally at HS to control early morning blood sugars.
34

Long Acting
Lantus (Glargine)/Levemir (Detemir)
• Onset in 1 – 1 ½ hours
• Duration is 24 hours
• Needs to be given at a consistent time
• Generally given at bedtime or morning
• Some may need twice a day shots
• May burn at the injection site
• Can Not be mixed with any other insulin
35

New
Toujeo (Lantus) U300
• The large insulin molecule (lantus) is shrunk to a
smaller molecule so you have smaller surface area
which releases more consistently
• 1/3 Less volume
• 6 hours to reach peak (if there is a peak)
• 5 days to steady state
• More consistent duration of 24-36 hours – should
not need BID dosing. 36

When to give the Long Acting
Insulin
• At Bedtime
• If there is a peak, it will peak early morning.
• Many people have early morning high blood sugars.
• Judge if this is a good dose by the FBS
• At Breakfast
• If there is a peak it will peak in the evening
• May have a better weight loss with morning shot
• Check blood sugar before bed to determine if this is a good dose.
37

Concentrated Insulin
• Regular U500 Insulin
• Is 5X more concentrated than insulin.
• 5 units of U500 is 25 units of U100 insulin
• Comes in 20 mL vials
• Generally given 3 times a day, with the three meals
• Try to spread the meals apart 6+ hours.
38

Combination Insulin
• 70/30 – 70% NPH & 30% Regular
• 75/25 – 75% NPH & 30% Humalog
• 50/50 – 50% NPH & 50% Humalog
• Novolog Mix 70/30 – 70% NPH & 30% Novolog
Insulin with the name Novolin or Humulin is usually NPH mixed with regular
39

What may be new?
• IDegLira
• Injectable medication that combines Victoza and
an Ultralong acting Basal Insulin degludec (a 42
hour insulin).
• Brand name will be Xultophy
• Fixed dose of GLP-1 and Insulin.
• Cost expected to be high
40

What may be new?
• Long Acting DPP4
• All DPP4’s last 24 hours, but they are working on
a once week version.
• Omarigliptin 25 mg, lowers Alc 0.71 mg in a 12
week study.
41

FDA approved Liraglutide for Weight
Loss
• Liraglutide (Victoza) now called Saxenda has been
approved as a treatment for chronic weight management
along with reduced calorie diet and physical activity
• Saxenda is a GLP-1 and can not be used with any other
GLP-1.
• Victoza doses is 0.6, 1.2 or 1.8 mg and Saxenda is 3 mg
• Concern will be nausea
42

Step wise approach to
Type 2 Treatment1. Lifestyle changes
2. Inititate Metformin (lower Alc by 1-2%)
3. If Alc > 7% after 3 months... (not in any order)
1. Add sulfonylurea (lower Alc by 1-2%)
2. TZD (lower Alc by 0.5 – 1.4%)
3. DPP4-I (lower Alc by 0.7-1.2%)
4. GLP-1 (lower Alc by 0.5 – 1%)
5. SGLT-2-I (lower Alc by 0.7-1.5%)
6. Basal insulin (lower Alc by 1.5%)
7. Mealtime (bolus) insulin (1 or more meals)43

Step wise approach to
Type 2 TreatmentDecision on what medications to use
Based on ADA/EASD Recommendations 2012
Individualized decisions based on 7 factors
Patient attitude and expected treatment effort
Hypoglycemia and other risks
Disease duration
Life expectancy
Comorbidities
44

continued
Established vascular complications
Resources, support system
Every medication regimen should be specifically designed for
that person
45

Questions
• Rebecca Newberry APRN MS CDE
Diabetes Education Center of the Midlands
Omaha, Nebraska 68124
46

47