diabetic foot exam - southern kentucky ahecsoahec.org/wp-content/uploads/2019/10/ann-davis.pdf ·...
TRANSCRIPT

Diabetic Foot ExamANN DAVIS, DPM
Learning Objectives➢Understand the comprehensive diabetic foot exam and its components
➢Understand pertinent positives of the exam that increase the risk for foot problems
➢Identify patients at risk for foot ulceration and amputation
➢Identify ways to prevent diabetic foot complications

Scope of the ProblemLifetime risk of a person with diabetes developing an ulceration as high as 25%
◦ Singh N, Armstrong DG, Lipsky BA: Preventing foot ulcers in patients with diabetes. JAMA 293:217–228, 2005
108,000 lower extremity amputations performed secondary to diabetes complications in 2014. This is the most common cause of non-traumatic lower extremity amputations.
◦ 2017 CDC National Diabetes Statistics Report
Diabetic patients with foot ulcers have 34% hospital readmission rates
◦ Burden of Infected Diabetic Foot Ulcers on Hospital Admissions and Costs. Ann Vasc Surg 2016 May; 33:149-158

Scope of the Problem3-year survival rate after one major lower extremity amputation is only 50%
Diabetics with amputations have a 50% chance of amputation to the contralateral limb within 5 years
◦ Team approach toward lower extremity amputation prevention in diabetes. Frykburg et al. J Am Pod Med. 1997; 87:7.

Economic Burden of Diabetic Foot Complications
Foot ulcers account for at least 33% of costs related to the treatment of diabetes related complications.
The cost of care for patient with a foot ulcer is 5.4 times higher in the first year compared to diabetics without foot ulcers.
◦ The costs of diabetic foot: the economic case for the limb salvage team. Driver et at. Journal of Vasc Surg2010 Sept; 52:3S
Foot ulcers and amputations cost the U.S. health care system an estimated $29 billion in 2007
◦ Rogers LC, Lavery LA, Armstrong DG. The right to bear legs—An amendment to healthcare; how preventing amputations can save billions to the US health-care system. J Am Podiatr Med Assoc 2008;98: 166-8.

Ulceration and Amputation Risk
Increased in people who have the following risk factors◦ Previous amputation◦ Past foot ulcer◦ Peripheral neuropathy◦ Foot deformity◦ Peripheral vascular disease◦ Visual impairment◦ Diabetic nephropathy◦ Poor glycemic control◦ Cigarette smoking
Boulton AJ, Armstrong DG, Albert SF, et al.; American Diabetes Association; American Association of Clinical Endocrinologists. Comprehensive foot examination and risk assessment: a report of the task force of the foot care interest group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists. Diabetes Care 2008;31:1679–1685

Comprehensive Diabetic Foot Exam
History
Vascular
Neurologic
Musculoskeletal
Dermatologic

History
Boulton AJ, Armstrong DG, Albert SF, et al.; American Diabetes Association; American Association of Clinical Endocrinologists. Comprehensive foot examination and risk assessment: a report of the task force of the foot care interest group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists. Diabetes Care 2008;31:1679–1685

FootwearAre these shoes appropriate for these feet?
Inappropriate shoes◦ Excessively worn
◦ Too small
◦ Resulting in rubbing creating erythema, blister, or callus formation
Vascular Exam

Arterial Anatomy: Lower Extremity

Arterial Anatomy: Lower Extremity

Peripheral arterial disease is the cause or major contributing factor in at least one-third of non-healing diabetic foot ulcerations.
Early recognition and prompt referral to vascular surgery is vital to decrease amputation rates.
Toe and flow: essential components and structure of the amputation prevention team. Rogers et al. Jour Vasc Surg. Sept 2010. Vol 52; 12S.

Dorsalis PedisPosterior Tibial
Pedal Pulses
0 Absent1 Diminished2 Palpable3 Full4 Bounding

Capillary Refill Time
▪Place foot at heart level
▪Completely compress blood from plantar aspect of great toe with thumb
▪Time it takes to completely refill the area of pallor
▪Normal: <3 sec
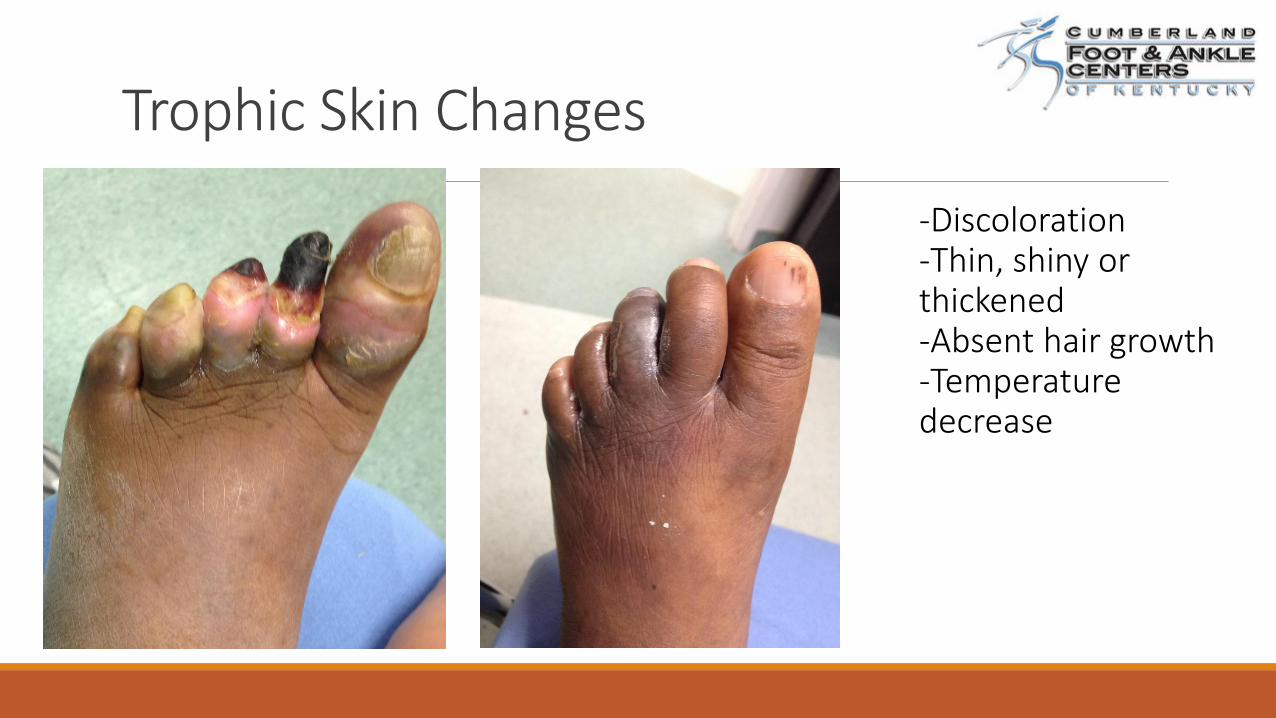
Trophic Skin Changes
-Discoloration-Thin, shiny or thickened-Absent hair growth-Temperature decrease

Ankle-Brachial Index
2016 AHA/ACC Guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease
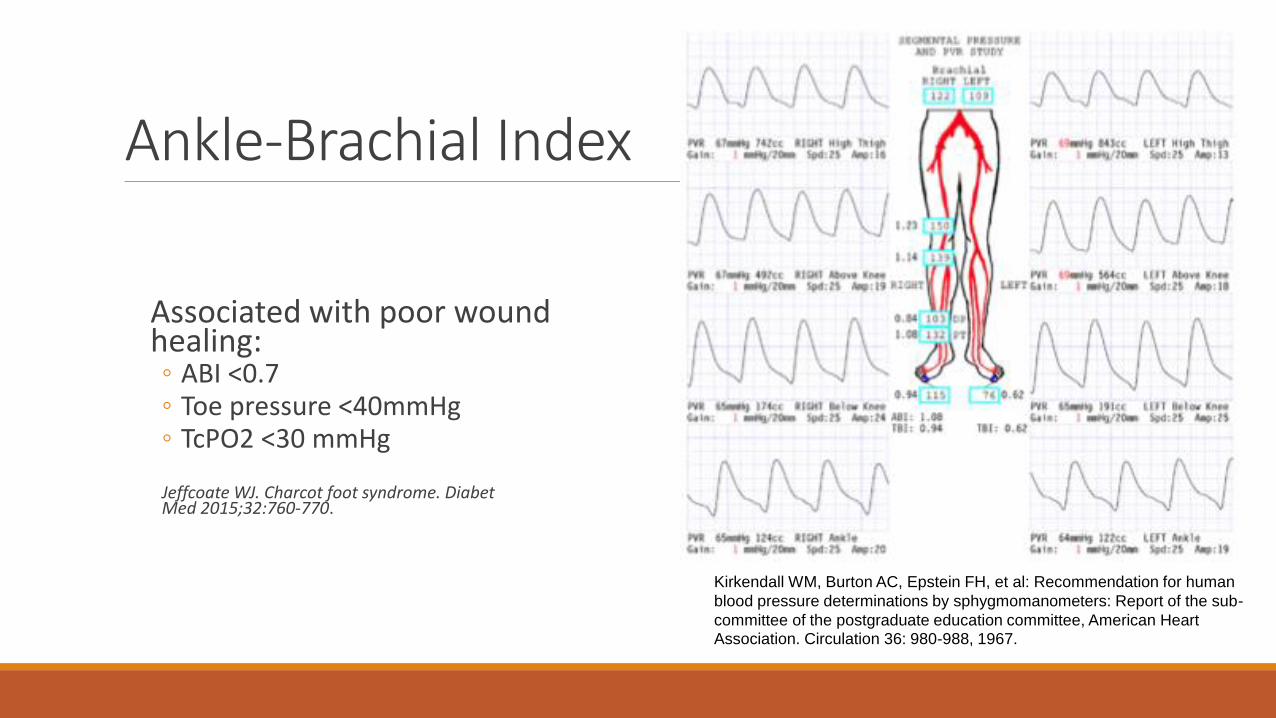
Ankle-Brachial Index
Associated with poor wound healing:◦ ABI <0.7◦ Toe pressure <40mmHg◦ TcPO2 <30 mmHg
Jeffcoate WJ. Charcot foot syndrome. DiabetMed 2015;32:760-770.
Kirkendall WM, Burton AC, Epstein FH, et al: Recommendation for human
blood pressure determinations by sphygmomanometers: Report of the sub-
committee of the postgraduate education committee, American Heart Association. Circulation 36: 980-988, 1967.

Arterial Calcifications

Neurologic Exam

Diabetic Peripheral Neuropathy▪Length dependent
▪Distal symmetric polyneuropathy
▪Primarily affects sensory and autonomic fibers, motor late stage
Diabetic neuropathy → loss of protective sensation → patient is unable to feel minor, repetitive trauma → callus
→ ulcer → amputation

Diabetic Peripheral NeuropathyDistal symmetric polyneuropathy occurs in 58-62% of patients with >5 years diabetes
Present in >82% of patients with foot wounds
Loss of 10-g monofilament perception and reduced vibration perception predict foot ulcers
◦ Boulton AJ, Vinik AI, Arezzo JC, et al.; American Diabetes Association. Diabetic neuropathies: a statement by the American Diabetes Association. Diabetes Care 2005;28:956–962

Subjective FindingsTingling, numbness, burning
Socks feel “bunched up”
Excessively cold or hot sensations
Heaviness
Balance deficits
Allodynia/Hyperalgesia

5.07 (10g) Semmes-Weinstein MonofilamentTest for the loss of protective sensation
o Perpendicular to the skino Enough pressure to cause monofilament to
buckle for one secondo Release
o Failure to sense the monofilament means the test site is insensate

5.07 (10g) Semmes-Weinstein Monofilament
Yes Responses/10 each foot
Score of <8/10 = LOPS
Yes Responses/5 each foot
Score of <3/5 = LOPS

•Number of test sites and the threshold for the definition of loss of protective sensation varies• Loss of protective sensation = 8/10 or 3/5 or 2/3
•Highly predictive of foot ulceration and lower extremity amputation
•Patients identified as having loss of protective sensation with the SWM have 2.5 to 5 times higher risk of developing an ulceration than patients with normal sensation
5.07 (10g) Semmes-Weinstein Monofilament
The Semmes Weinstein monofilament examination is a significant predictor of the risk of foot ulceration and amputation in patients with diabetes mellitus. Feng et al. Journal of Vascular Surgery. Jan 2011; 53:1.

Vibratory Sensationo128 hZ tuning fork
oApplied to the bony prominence of the big toe
oIf impaired, proceed to proximal bony prominences: medial malleolus, patella
oTests integrity of large fiber nerves
Loss of ProprioceptionWide base of gait
Loss of balance, especially with the eyes closed
Unsteady gait

Proprioception▪Hold the distal phalanx of the great toe by its sides
▪Demonstrate movement of the toe “up” and “down”
▪Have the patient close their eyes and tell you which direction you are moving the toe
▪Failure to identify the correct direction indicates a loss of proprioception

ReflexesAchilles Reflex
◦ Foot is dorsiflexed at the ankle
◦ Hammer strikes the stretched Achilles tendon just proximal to the calcaneus
◦ Normal elicits a small amount of plantarflexion
Patellar Reflex◦ Knee hangs with gravity flexion off table
◦ Hammer strikes patellar tendon between patella and tibial tuberosity
◦ Normal elicits knee extension

Autonomic Neuropathy
Denervation of dermal structures leads to decreased sweating causing dry skin, cracking, thick and brittle toenails, dysregulation of temperature
Musculoskeletal

Structural Deformity and Limited Joint MobilityLead to focal areas of high pressure
Abnormal pressure + loss of protective sensation → ulceration

Muscle Wasting – “Intrinsic Minus Foot”Foot deformities are more common in diabetic patients due to atrophy of the intrinsic musculature responsible for stabilizing the toes
Guttering between metatarsals
Peripheral Neuropathy and the Diabetic Foot. Sunshein, Samouilov. Diabetes Care March 2017.

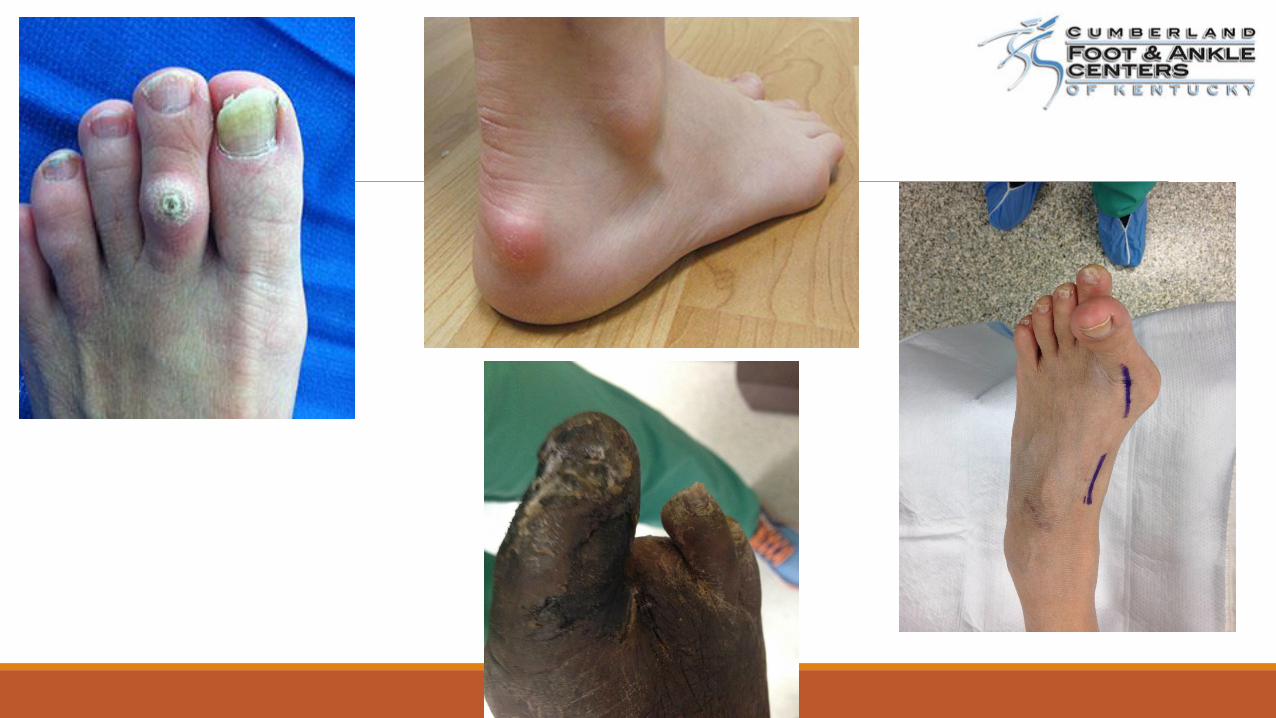
Deformities
CharcotBunion & Hammertoes
Dermatologic

General InspectionNail dystrophy
Elongated or ingrowing toenails
Dry or cracking skin
Interdigital changes
Callus
Ulceration

Onychomycosis

Fissures and Dry Skin

Interdigital Maceration
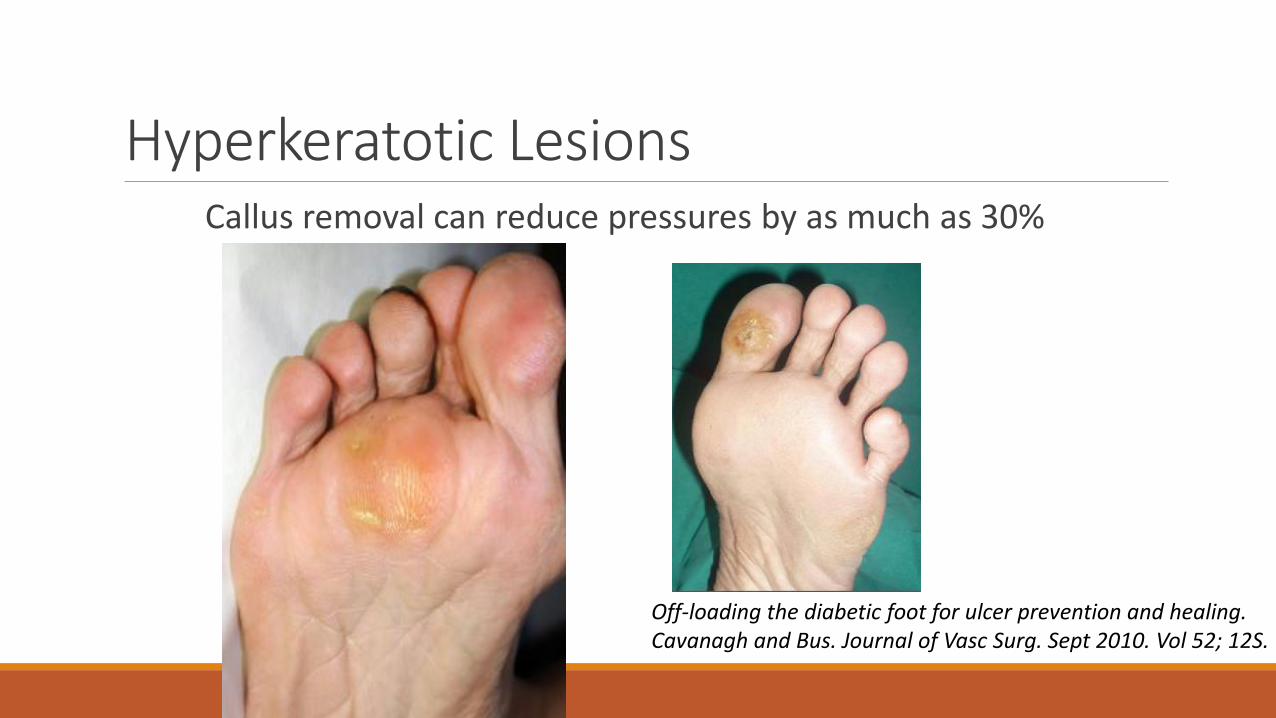
Hyperkeratotic LesionsCallus removal can reduce pressures by as much as 30%
Off-loading the diabetic foot for ulcer prevention and healing. Cavanagh and Bus. Journal of Vasc Surg. Sept 2010. Vol 52; 12S.
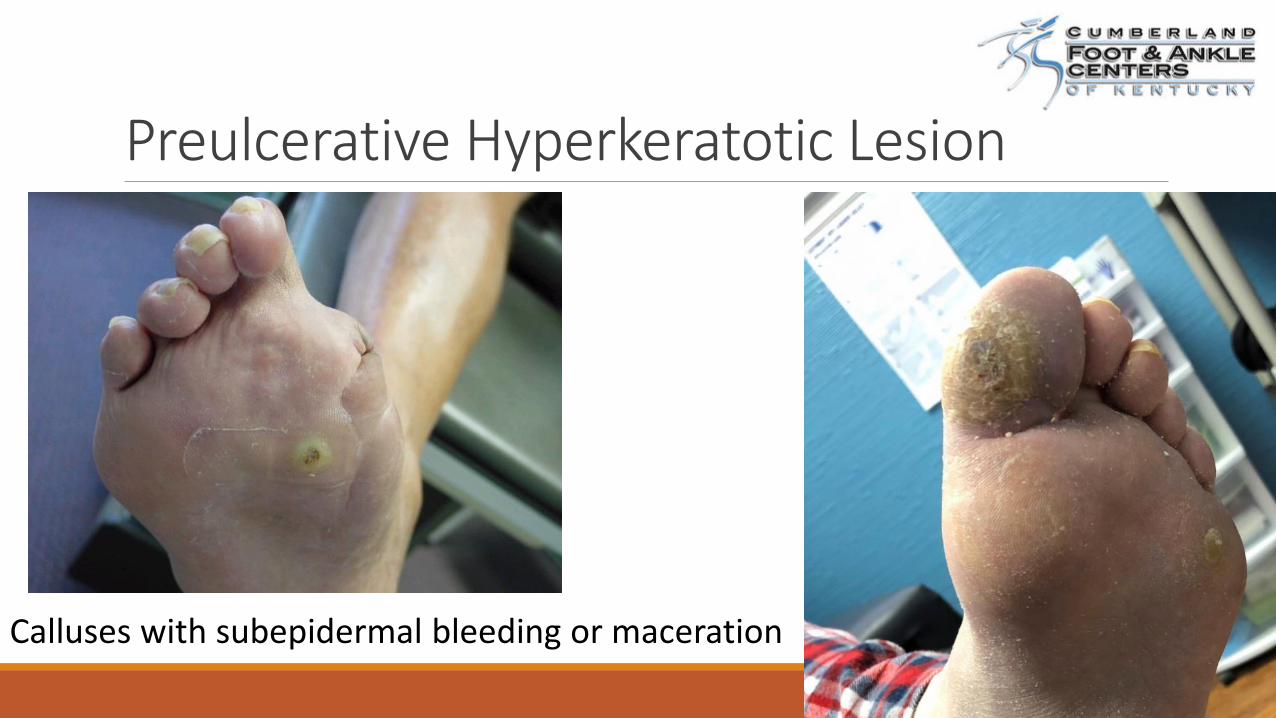
Preulcerative Hyperkeratotic Lesion
Calluses with subepidermal bleeding or maceration

Diabetic Foot Ulceration

Diabetic Foot UlcerationTypically painless due to neuropathy – few subjective complaints
Most common sites: ◦ Plantar metatarsal heads◦ Toes◦ Heel
Diabetic ulcers precede more than 80% of non-traumatic lower extremity amputations
Jain A. A simple new classification for diabetic foot ulcers. Med-Sci 2015;4:2109

Diabetic Foot Ulcer: #1 Offload!
Lack of protective sensation combined with unaccommodated foot deformities exposes patients to undue sudden or repetitive stress that leads to callus and eventual ulcer formation
Off-loading the diabetic foot for ulcer prevention and healing. Cavanagh and Bus. Journal of Vasc Surg. Sept 2010. Vol 52; 12S.

Diabetic Foot Ulcer: #1 Offload!
Continued unabated pressure may lead to fat exposure and exposure of bone
Peripheral Neuropathy and the Diabetic Foot. Sunshein, Samouilov. Diabetes Care March 2017.
Gold Standard: Non-weight bearing

Diabetic Foot Ulceration: DebridementNormal physiology of acute wound healing: inflammation→proliferation→maturation
Chronic wounds are arrested in the inflammatory stage◦ ↑metalloproteases produced by necrotic tissue
and bacteria
◦ ↓chemotactants, growth factors, mitogens
◦ Presence of senescent cells and biofilm
Debridement of the noninfected wound. Cornell et al. Journ Vasc Surg Sept 2010. Vol 52; 12S.
Diabetic Foot Ulceration: RecurrenceAfter an ulcer is healed, the risk of recurrence is high. This demonstrates the
importance of continuous offloading with appropriate diabetic shoes and inserts.
40% recurrence rate of diabetic foot ulcers in a median of 4 monthsPound N, Chipchase S, Treece K, Game F, Jeffcoate W. Ulcer-free survival following management of foot ulcers in diabetes. Diabet Med 2005;22:1306-9.

Infected or Contaminated?•>60% of chronic wounds contain biofilm
•Cultures may show colonization of multiple bacteria, but not all are causing infection
•Gram positive are the most common infectious pathogen
•Periwound erythema, edema, warmth, purulent drainage are used to guide antibiotic timing
Debridement of the noninfected wound. Cornell et al. Journ Vasc Surg Sept 2010. Vol 52; 12S.
Peripheral Neuropathy and the Diabetic Foot. Sunshein, Samouilov. Diabetes Care March 2017.
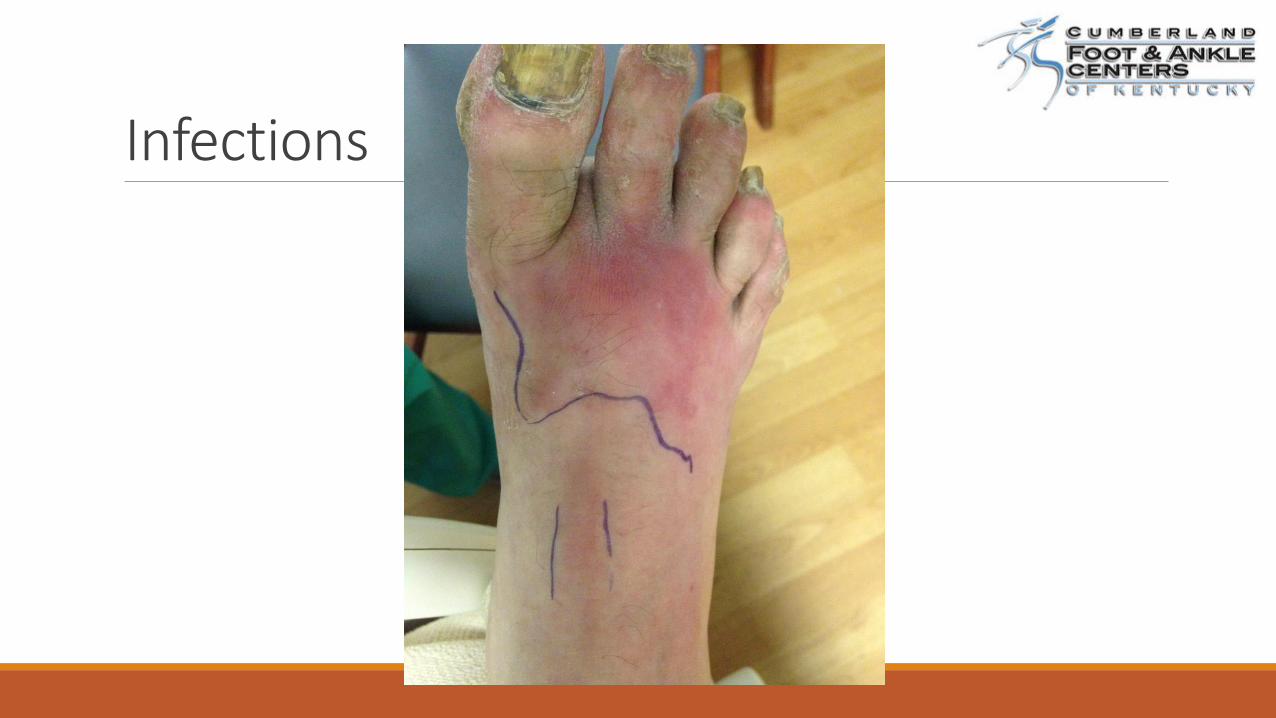
Infections


Charcot NeuroarthropathyNeuropathic patients presenting with erythema, edema, warmth
Often misdiagnosed: Cellulitis, gout, DVT, osteomyelitis
Average Patient:
-55-60 years old
-80% have been diabetic >10 years

Eichenholtz Classification (1966)
Stage 0: (addition by Shibata et al. 1990)◦ Primarily Exam: red, hot, swollen
◦ Minimal/No osseous destruction visible on plain radiographs
Stage I: Destruction◦ Capsular distention, osseous fragmentation,
peri-articular debris formation, subluxations, fracture
Stage II: Coalescence◦ Osseous resorption, consolidation
Stage III: Reconstruction◦ Maturation of bone consolidation
Stages of Charcot
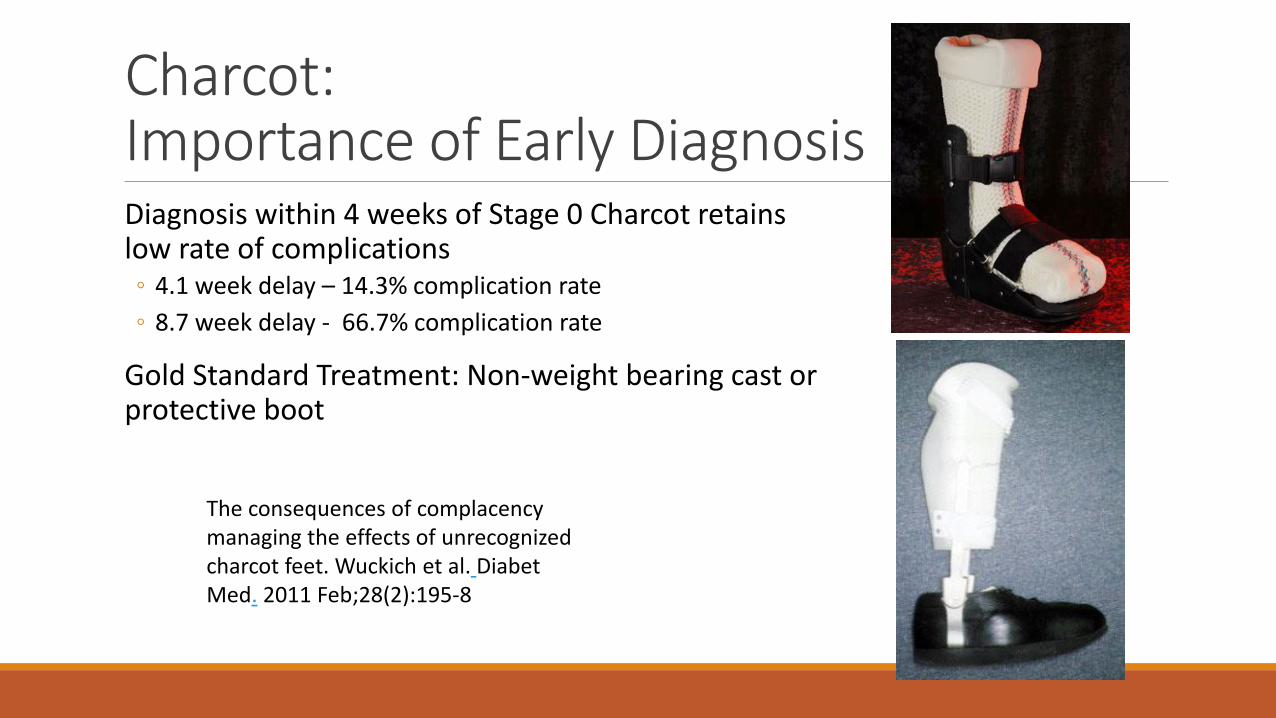
Charcot: Importance of Early DiagnosisDiagnosis within 4 weeks of Stage 0 Charcot retains low rate of complications◦ 4.1 week delay – 14.3% complication rate
◦ 8.7 week delay - 66.7% complication rate
Gold Standard Treatment: Non-weight bearing cast or protective boot
The consequences of complacency managing the effects of unrecognized charcot feet. Wuckich et al. Diabet Med. 2011 Feb;28(2):195-8

Charcot Complications7% of Charcot patients will eventually have an amputation
28% of Charcot patients with an ulceration will eventually have an amputation
◦ Saltzman Clin Ortho Rel Res 2005

Risk Stratification and Prevention

American Diabetic Association Foot Risk Classification
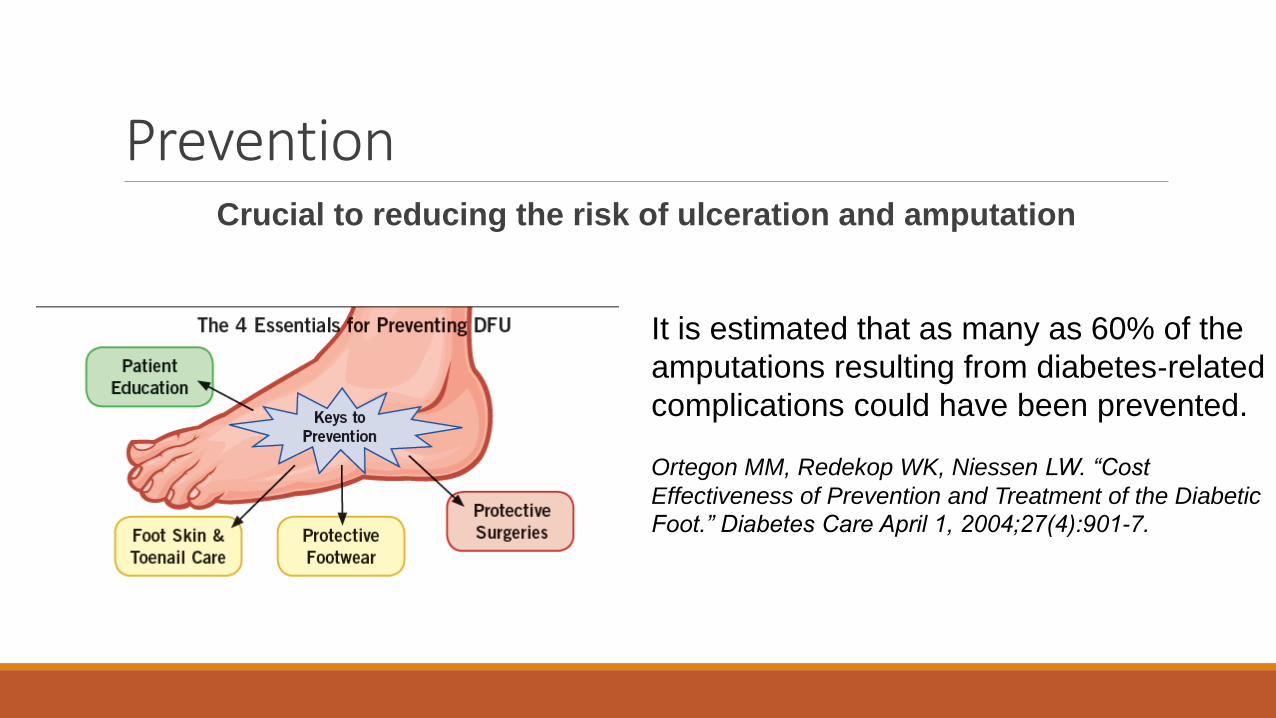
PreventionCrucial to reducing the risk of ulceration and amputation
It is estimated that as many as 60% of the
amputations resulting from diabetes‐related
complications could have been prevented.
Ortegon MM, Redekop WK, Niessen LW. “Cost
Effectiveness of Prevention and Treatment of the Diabetic
Foot.” Diabetes Care April 1, 2004;27(4):901-7.
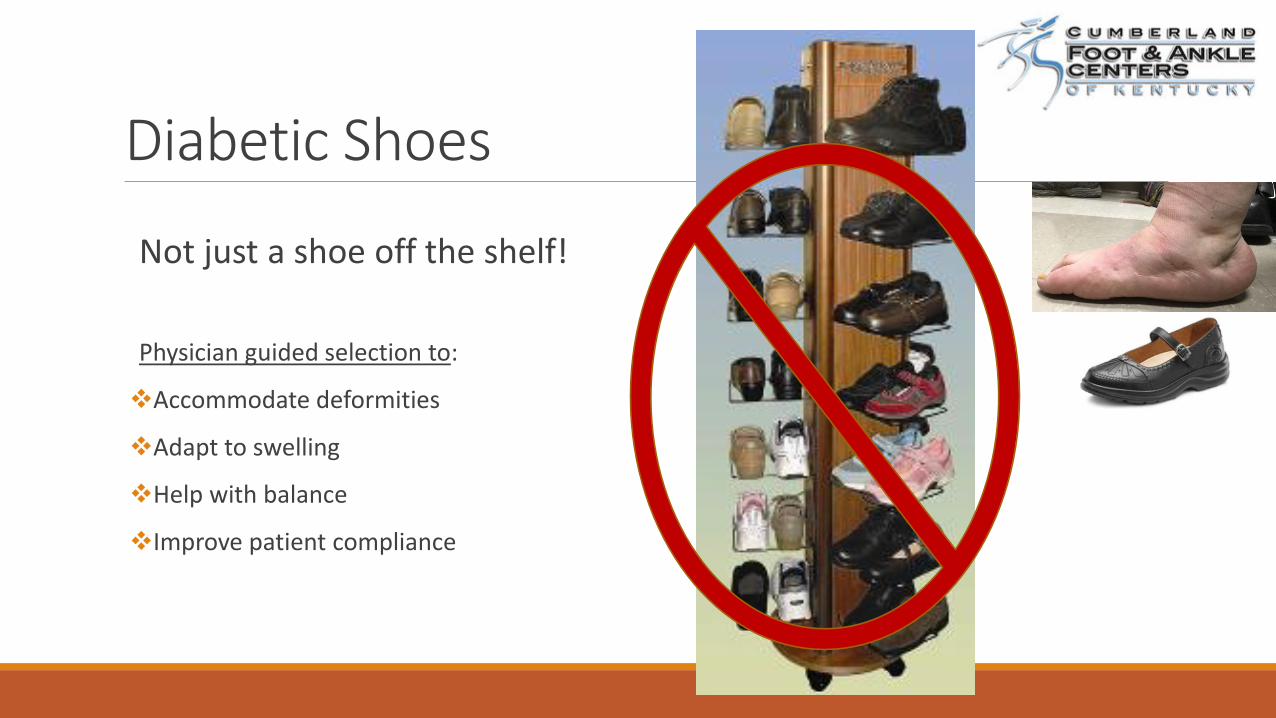
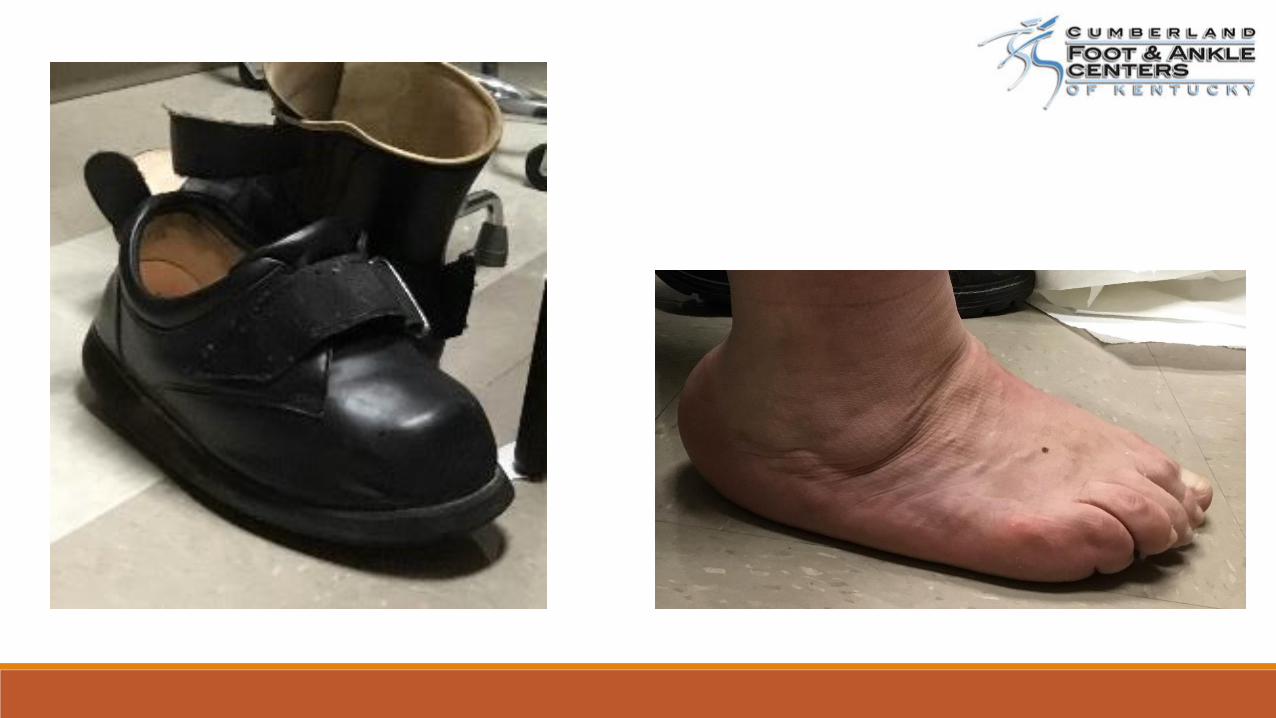
Diabetic Shoes
Not just a shoe off the shelf!
Physician guided selection to:
❖Accommodate deformities
❖Adapt to swelling
❖Help with balance
❖Improve patient compliance

Diabetic Shoes

Amputation PreventionPatient
Daily foot inspection
Gentle cleansing with soap and water
Application of topical moisturizers
Proper footwear
Avoid temperature extremes
PractitionerCareful objective diabetic foot
exams
A1C control
Peripheral vascular testing
Diabetic shoes

Amputation Prevention: Multidisciplinary Approach
Primary Care
Hospitalists
Endocrinology
Infectious Disease
Radiology
Podiatry
General Surgery
Orthopedic Surgery
Plastic Surgery
Vascular Surgery
Nursing
Nutrition
Diabetes Educators
Physical Therapy
Orthotists
Social Services
Implementation of the team approach to manage diabetic foot ulcers within a given region or health care system has been reported to reduce long term amputation rates from 82% to 62%
The costs of diabetic foot: the economic case for the limb salvage team. Driver et at. Journal of Vasc Surg 2010 Sept; 52:3S

Summary