diabetic neuropathy - ncvh cardiovascular conference ncvh/5-27-wed/podiatry/1345_guy pupp.pdf ·...
TRANSCRIPT
Guy R. Pupp, DPM, FACFAS
Program Director
Podiatry Residency
Providence Hospital, Michigan
Diabetic Neuropathy

NO FINANCIAL DISCLOSURES

An estimated 285 million people worldwide had
diabetes in 2010, according to the International
Diabetes Federation. The federation predicts as
many as 438 million will have diabetes by 2030.
Nearly 110 million wounds! U.S… Yr. 2050: 48 Million DM, 9.6 Million Ulcers

Amputation secondary to NEUROPATHY and PAD

Misdiagnosed CLI
BKA associated with NEUROPATHY and PAD

Neuropathic Ulcers…B-K Amputation?
Diabetic Foot Ulcers One of the most common complications of diabetes
Annual incidence 1% to 4%1-2
Lifetime risk 15% to 25%3-4
~15% of diabetic foot ulcers result in lower extremity amputation3,5
~85% of lower limb amputations in patients with diabetes are proceeded by ulceration6-7
Peripheral neuropathy is a major contributing factor in diabetic foot ulcers1-7
Other factors: foot deformity, callus, trauma, and peripheral vascular disease
1. Reiber and Ledoux. In The Evidence Base for Diabetes Care. Williams et al, eds. Hoboken, NJ: John Wiley & Sons; 2002:641–665.
2. Boulton et al. NEJM. 2004;351:48.3. Sanders. J Am Podiatry Med Assoc. 1994;84:322.
4. Boulton et al. Lancet. 2005;366:1719.5. Ramsey et al. Diabetes Care 1999;22:382.6. Pecoraro et al. Diabetes Care. 1990;13:513.7. Apelqvist and Larsson. Diabetes Metab Res Rev. 2000:16:S75.
Diabetic Peripheral Neuropathy:
What is it?
• Nerve damage and dysfunction secondary to diabetes mellitus type 1 or 2
– Consensus definition: “the presence of an abnormality of nerve conduction and a symptom or symptoms or a sign or signs of neuropathy confirm Distal Symmetrical Polyneuropathy (DSPN). If nerve conduction is normal, a validated measure of small fiber neuropathy may be used.”
Tesfaye S, et al. Diabetes Care 2010;33:2285-2293..
Diabetic Neuropathy:
The Forgotten Complication
Results of the 2005 ADA National Survey
• Only one in four survey respondents who experience symptoms of diabetic neuropathy have been diagnosed with the condition.
• The majority of respondents who experience symptoms (56%) remain unaware of the term DIABETIC NEUROPATHY.
• 62% believe that their symptoms are associated with their diabetes, but only 42% have been told by their physician that diabetes is the cause.
• Approximately one in seven people who said they talked to their doctor about their symptoms and pain reported that no cause was mentioned.
May 10, 2005 /PR Newswire via COMTEX.

Neuropathy is Commonly Underdiagnosed
For every mistake made for not knowing, 10 are made
for not looking
Endocrinologists
Non-endocrinologists
Co
rre
ct
dia
gn
os
is (
%)
0
20
40
60
80
100
No neuropathy
(n=4628)Non-severeneuropathy
(n=2209)
Severeneuropathy
(n=541)
Herman et al. Diabetes Care. 2005;28:1480.Breathnach CS and Moynihan JB. Ulster Med J 2012;81(3):149-153.
- J.A. Lindsay
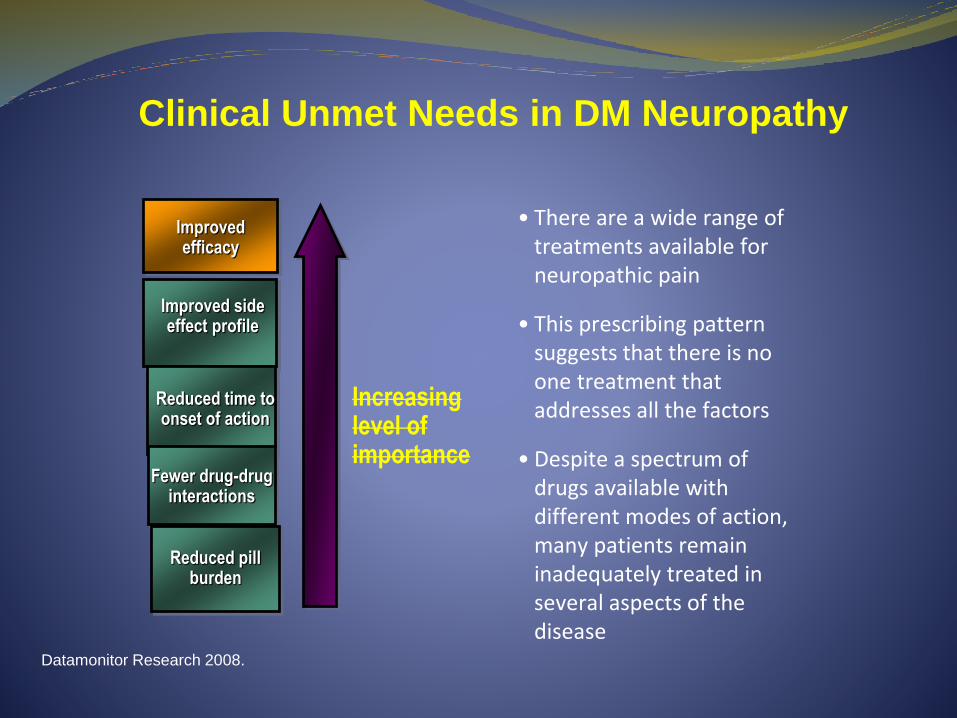
Clinical Unmet Needs in DM Neuropathy
• There are a wide range of treatments available forneuropathic pain
• This prescribing pattern suggests that there is no one treatment that addresses all the factors
• Despite a spectrum of drugs available with different modes of action, many patients remain inadequately treated in several aspects of the disease
Increasinglevel ofimportance
Improvedefficacy
Improved sideeffect profile
Reduced time toonset of action
Fewer drug-druginteractions
Reduced pillburden
Datamonitor Research 2008.

Clinical Impact of DPN Total Symptoms
DPN
Painfulneuropathicsymptoms
NeuropathicdeficitsImpairment
DisabilityHandicap
FootUlcers...Charcot
Infection(skin, bone)
Quality
of life
Surgery, Amputation96,000/y
AtaxiaWeakness
Falls
Mortality
Cost $37B
Fractures
Vinik, et al. Endo & Metab 2006;2(5):269-81.
Vinik, Aaron. Frontiers in Endocrinology 2012;3:1-3.
Vinik A, et al. Endocrinol Metab Clin N Am 2013;42:747-787.

NEUROPATHY…Charcot…Ulcer...Osteo…BKA

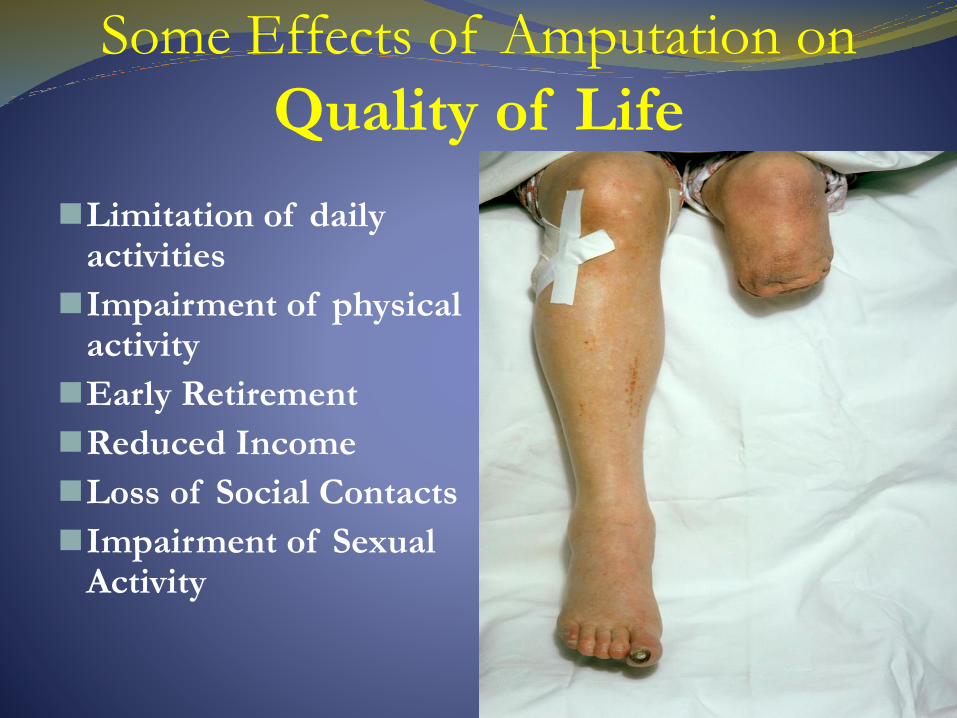
Some Effects of Amputation on
Quality of Life
Limitation of daily activities
Impairment of physical activity
Early Retirement
Reduced Income
Loss of Social Contacts
Impairment of Sexual Activity

Aging, Disease and Falls • Risk of falling typically increases when (age-related) diseases emerge
• One third of people >65y fall annually
• Each day in the US 63 people die from a fall- related injury
• An additional 1800 are hospitalized
• The commonest causes of falling are:
Hypertension
Diabetes
Polypharmacy
• Therefore we need to compensate for both age- and disease-related factors that can impact on balance and stability
Neuropathy in Diabetes
Tromp AM, et al. J Clin Epidemiol 2001;54:837-44.
Centers for Disease Control and Prevention website at http://www.cdc.gov/injury/wisqars

Reaction Time- Hand- Foot
Proprioception
Lower Limb Strength- Ankle dorsi-flexion- Knee flexion- Knee Extension
Sensation
Vision- Visual Acuity
- Contrast Sensitivity
Postural Sway
Clinical Tests

VisionSomatosensoryVestibular Auditory
Neurological
Perc
epti
on
Cognition
Pro
prio
ceptio
n
Strength
Motor
Balance & Mobility Cardiorespiratory
Polyp
harm
acy
Risk Factors for Falls

Distal Symmetric Diabetic Neuropathies
Subtypes:
Neuropathy
Large-fiber
MYELINATED SENSORY-MOTOR
Deep-seated pain (A- type)
Wasting and weakness
Numbness, pins and needles,
tingling & ataxia
Impaired vibration perception
Loss of position sense
Loss of reflexes
Impaired nerve conduction velocity
Interferes with normal life
Risk of falling and fractures
Small-fiber
UNMELINATED SENSORY ONLY
Superficial pain (C-fiber type)
Electric shock, burning, allodynia
Autonomic dysfunction
Thermal imperception
Normal strength and reflexes
Electrophysiogically silent
Quantitative sensory testing and
skin biopsies
Produces symptoms
Leads to morbidity and mortality
Vinik A, et al. Endo & Metab 2006;2(5):269-281.
Large Fiber NeuropathyCarry info regarding position and vibration
-weakness…<DTR, <Vib
-”numbness without pain”
Diagnosis: EMG, NCV

Simple Tests of Large-Fiber Function
Controls (n=11)Diabetic controls (n=8)Diabetic neuropathy (n=14)
0
20
40
60
80
100
120
140
160
180
2-minutewalk
Dis
tan
ce (
m)
*
30
0
5
10
15
20
25
Tandemstand
1- footstand
Balancewalk
Foottapping
Tim
e (
s) *
†
* *
Resnick et al. Muscle Nerve. 2002;25:43.
* P<0.05 vs nondiabetic controls; †P<0.01 vs nondiabetic controls

SMALL FIBER NEUROPATHY
Carry info regarding pain and temperature
-stocking/glove effect
-Electrical studies are WNL
Diagnosis: Clinical info
Skin biopsy

Differential Dx of Small Fiber Neuropathy
MS
Raynauds
FMS
RSD/CRPS
Restless Leg
Neuroma
Therapath Neuropathology Report, 2004.
CAUSES OF SMALL FIBER NEUROPATHY
AutoimmuneSarcoidSjogren’s SyndromeInflammatory Bowel DiseaseLyme DisEtOH abuseDrugs,ToxinsAmyloidosisLupusVasculitis
Bakkers M et al. J. Neurol 2010, 12: 2086-90

Small Fiber Neuropathy
– Pain is C-fiber type, burning, superficial, allodynia
– Early hyperesthesia and hyperalgesia, impaired neurovascular function
– late hypoesthesia and hypoalgesia
– Impaired warm thermal and pain thresholds, decreased IENF
– Decreased sweating
– Normal strength, reflexes and EMG!!!
Vinik, A.I., et al. Exp. Clin. Endocrinol Diabetes 2001;109(Suppl 2):S451-S473.
The Use of 1 and 10g Monofilament Test
DIABETIC NEUROPATHY

Diabetic Neuropathy: A Small Fiber Disease
Normal Skin
Biopsy
Small Fiber
Neuropathy Biopsy
Normal innervation with small nerve
fibers seen in the epidermis (arrows).
Skin biopsy specimens with protein
gene product 9.5 immunostaining.
A specimen from a patient with small
fiber neuropathy shows denervation
with no small nerve fibers seen in the
epidermis
Tavee J , Zhou L Cleveland Clinic Journal of Medicine 2009;76:297-305

Work-up for Peripheral Neuropathy:
A1c (Glycohemoglobin)
CBC
Chemistry Profile
TSH
B12, Folic Acid Level
Serum Protein Electrophoresis (SPEP)
Sedimentation Rate, ANA, RPR, RA
Heavy Metal Screen (Lead, Arsenic, Mercury)
*EMG/NCV
*Biopsy/CSF
*Genetic screening
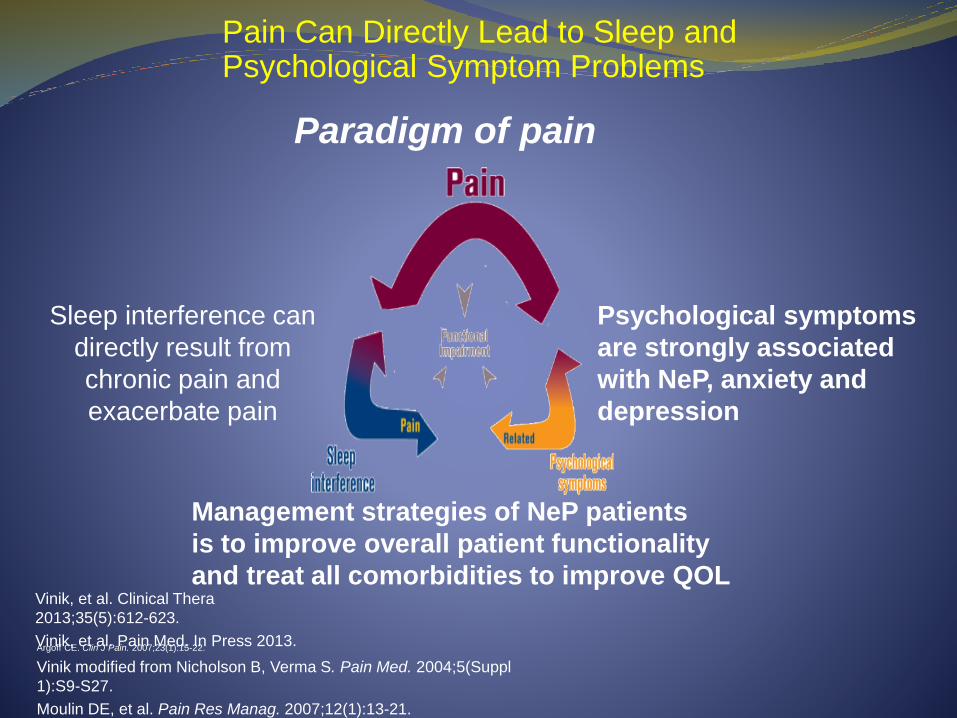
Pain Can Directly Lead to Sleep and Psychological Symptom Problems
Paradigm of pain
Sleep interference can
directly result from
chronic pain and
exacerbate pain
Psychological symptoms
are strongly associated
with NeP, anxiety and
depression
Management strategies of NeP patients
is to improve overall patient functionality
and treat all comorbidities to improve QOL
Argoff CE. Clin J Pain. 2007;23(1):15-22.
Vinik modified from Nicholson B, Verma S. Pain Med. 2004;5(Suppl
1):S9-S27.
Moulin DE, et al. Pain Res Manag. 2007;12(1):13-21.
Vinik, et al. Clinical Thera
2013;35(5):612-623.
Vinik, et al. Pain Med. In Press 2013.
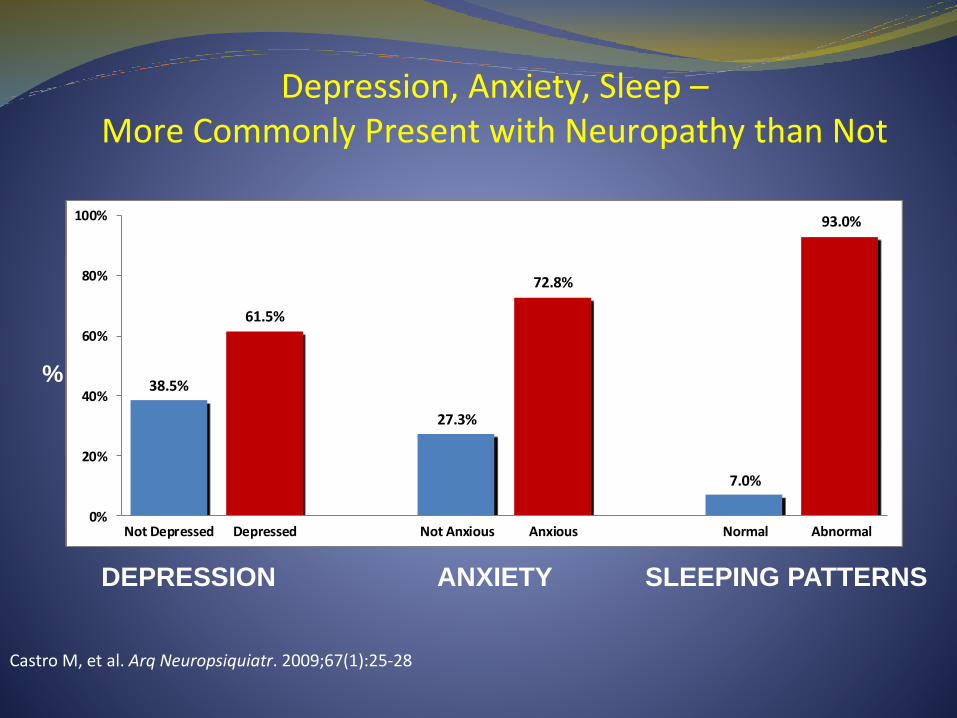
Depression, Anxiety, Sleep –More Commonly Present with Neuropathy than Not
Castro M, et al. Arq Neuropsiquiatr. 2009;67(1):25-28
38.5%
61.5%
27.3%
72.8%
7.0%
93.0%
0%
20%
40%
60%
80%
100%
Not Depressed Depressed Not Anxious Anxious Normal Abnormal
N=400
DEPRESSION ANXIETY SLEEPING PATTERNS
%

DNAssociation of Metformin and Clinically Worsened DPN
The Neuropathy Impairment Scale
has been designed in an effort to
maximize the measurement of
potential changes in all motor,
sensory and reflex activity in the
lower limbs. Total score ranges
from normal = 0 to maximum of
16.
n = 122
• A prospective study of 122 symptomatic DPN patients compared those who had >6 months of metformin to those without metformin
• Metformin-associated cobalamindeficiency may contribute to the clinical burden of DPN (P<0.001).
• The severity of DPN positively correlates to increases in the cumulative metformin dose (P<0.001)
Wile DJ, et al. Diabetes Care 2010;33:156-61.Bril, Vera. Eur Neurol 1999;41(Suppl 1):8-13.

Diabetic Neuropathy Treatment Options
TCAs, Pregabalin
Opioids
Gabapentin / Duloxetine
Pain Management
Glucose Management
Medical Foods (Metanx)
Vitamins (B12, Folic acid…)
Topical Compounds
Adapted from Tavakoli M and Malik R. Expert Opin Pharmacother. 2008;9(17):2969-2978..
Fonseca VA, et al. Am J Med 2013;126(2):141-149.
Interventional Tx-Regional N Blocks-Sympathetic Blocks-Spinal Cord Stimulators-Infusion Therapy
SURGERY-Tarsal Tunnel Deconpression
-Neurolysis

Metanx®-Methylfolate 3 mg
Methylcobalamin 2 mg
Pyridoxal 5’ –phosphate 35 mg
Nutritional support specifically modified for the management of the distinct nutrient needs that result from the disease or condition, as determined by medical evaluation.
Medical Food – Regulated by FDA
• Metanx® is dispensed by prescription under supervision of a HCP
• Metanx® addresses the underlying condition such as endothelial dysfunction / DPN
• Metanx® is scientifically recognized in peer-reviewed literature
U.S. Food and Drug Administration. Guidance for Industry: Frequently Asked Questions About Medical Foods. Available at:
http://www.fda.gov/Food/Guidanceregulation/GuidanceDocumentsRegulatoryInformation/Medical Foods/ucm054048.htm Accessed May 23, 2014.
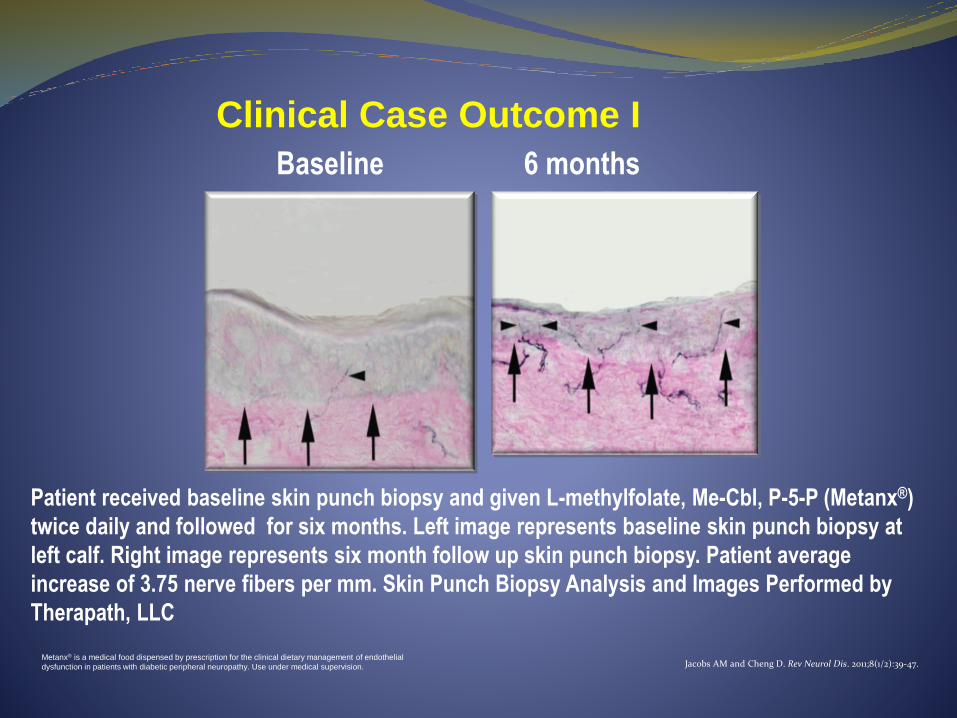
Clinical Case Outcome I
Baseline 6 months
Patient received baseline skin punch biopsy and given L-methylfolate, Me-Cbl, P-5-P (Metanx®)
twice daily and followed for six months. Left image represents baseline skin punch biopsy at
left calf. Right image represents six month follow up skin punch biopsy. Patient average
increase of 3.75 nerve fibers per mm. Skin Punch Biopsy Analysis and Images Performed by
Therapath, LLC
Metanx® is a medical food dispensed by prescription for the clinical dietary management of endothelial
dysfunction in patients with diabetic peripheral neuropathy. Use under medical supervision. Jacobs AM and Cheng D. Rev Neurol Dis. 2011;8(1/2):39-47.

Metanx® Administration to PregabalinPartial-Responders for Management of DPNP
Results from a 20 week, open label trial of Metanx® in 24 patients with a partial response to pregabalin.
After nutritional management with Metanx®:
The average absolute pain reduction after 20 weeks in the study group was 3.0 compared to .25 in the control group (P<0.001)
After 20 weeks, the study group experienced greater pain relief compared to the active control group, 87.5% vs. 25.0% reduction in NPS respectively (P=0.005)
Jacobs, AM, Cheng D. J Diabetes Mellit 2013;3(3):134-38.
0
-0.5
-1
-1.5
-2
-2.5
-3
-3.50 20
Weeks
Pai
n R
edu
ctio
n
P<0.001
Pregabalin
L-methylfolate,
Me-CBl, P-S-P/
Pregabalin
Significant Change in Neuropathic Pain
Summary and Conclusions: Diabetic Neuropathies
Diabetic neuropathies are a heterogeneous group of disorders that occur in about 50% of patients with diabetes. Approximately 40% are painful.
DPN is the most common form of neuropathy and is a mixed sensorimotor neuropathy involving small and large fibers, with each fiber having a different etiology and producing its own constellation of features.
The pathogenesis is being unraveled and therapy directed at oxidative/nitrosative stress and autonomic imbalance have lead to major breakthroughs in management with the ability to reduce cardiovascular events, regenerate nerves, stop falls and reduce foot ulceration. There are promising agents in the wings including gene therapy that address the core pathogenic mechanisms and are potential targets for therapy in the future.
Tesfaye S and Selvarajah D. Diabetes Metab Res Rev 2012;28(Suppl 1):8-14.Boulton AJM, et al. Diabetes Care 2005;28(4):956-962.
Vinik and Casellini. Diabetes, Metabolism Syndrome & Obesity 2013;6:57-78.


Guy R. Pupp, DPM, FACFAS
Program Director
Podiatry Residency
Providence Hospital, Michigan
Diabetic Neuropathy