diagnos+cerrorinmedicineisamajorcauseofpaentharm,withtherateofclinical-reasoning.org/resources/pdfs/cr2-how-drs-think.pdf ·...
TRANSCRIPT

1

2

Diagnos+c error in medicine is a major cause of pa+ent harm, with the rate of missed, incorrect, or delayed diagnoses es+mated to be as high as 10%–15% in the ‘undifferen+ated special+es’. Autopsy studies have iden+fied major diagnos+c discrepancies in up to 20% of cases, sugges+ng that the working or final clinical diagnosis may be wrong in as many as one in five pa+ents overall.
85% of diagnos+c errors are considered preventable. Serious disability results in up to 50% of cases of diagnos+c error.
For every diagnos+c error there are a number of root causes, but errors in reasoning accounted for 2/3 of these in one study. Either available data was not adequately gathered, or available but not synthesised correctly.
Altho diagnos+c error is lower in radiology, es+mated to be around 4%, because medical imaging cons+tutes such a large component of modern clinical diagnosis, the problem of diagnos+c error is in part aPributable to errors in radiology. But error, as we will see, is a complicated maPer.
3

In medicine overall, studies of diagnos+c error assign three main categories: no fault errors, system failures, and human cogni+ve error. But if we look more closely at “human cogni+ve error” studies tend to find three things:
Knowledge gaps – eg Rigler’s sign Misinterpreta+on of diagnos+c tests – esp in neurological emergencies, when clinical exam can be more sens/spec than even MRI in first 24 hrs
Cog biases – like the “framing effect” (how something is handed over to you) and “search sa+sficing” – more of that later.
4

5
In teaching clinical reasoning to medical students we explain the different elements that make it up – what topics are in a clinical reasoning syllabus. One of the things we focus on a lot is that tests give test probabili+es, not real probabili+es. The pre-‐test (clinical) probability is vital, and that depends on good clinical skills (history and physical exam). Tests – whether blood results or radiological inves+ga+ons – have to be interpreted in the light of the clinical probability and that is something that is not necessarily explicitly taught in medical schools, certainly not prac+ced very well.

[read slide] This is important because as doctors we need to know how our thinking can be flawed so we can learn to be bePer thinkers and decision makers. Remember that most of the root causes of diagnos+c error are because of errors in reasoning, most commonly because the available data is not synthesised correctly.
6

Example of TYPE 1 thinking Which is the cat and which is the dog? It’s obvious! That’s because you have seen lots of different types of cats and lots of different types of dogs before -‐ you immediately (intui+vely) recognised the difference. And this is exactly what experienced GPs and consultants do in medicine. We dis+nguish diseases using paPern recogni+on, accessing a vast databank of experiences. Meanwhile the medical students are s+ll pondering: well they both have fur, they both have pointy ears, they both have wet noses, they both have four legs. Hang on, that one just meowed therefore it must be the cat. Medical students give lots of weight to single bits of informa+on (see the trees) – experts see the wood from the trees (see paPerns).
7

Let’s start with an experiment. Take a QUICK look at this problem and tell the person next to you the answer. Don’t think about it for too long. Now, intui+vely a number came to your mind – 10p. Most people come up with this answer. It is intui+ve – and wrong. What’s going on here?
8

Psychologists es+mate that we spend 95% of our daily lives engaged in Type 1 thinking – the intui+ve, fast, subconscious mode of decision-‐making. Imagine driving a car, for example – it would be impossible to func+on efficiently if every decision and movement was as deliberate, conscious, slow and efforrul as in our first driving lesson. With experience, complex procedures become automa+c, fast and effortless. The same applies to medical prac+ce. There is evidence that expert decision-‐making is well served by intui+ve thinking. The problem is that although intui+ve processing is highly efficient in many circumstances, in others it is prone to error.
9

And we use all of these in genera+ng a differen+al diagnosis and modifying our hypotheses … 1) Deduc+on moves from general rules to specific case: if the premise is true the conclusion
must also be true – e.g. troponin goes up in heart aPacks, therefore my pa+ent with a heart aPack will have a raised troponin.
2) Hypothe+co-‐deduc+ve is when we generate different hypotheses and arguments to test them. E.g. in disease A finding B is present. Finding B is absent, therefore Disease A is not the diagnosis.
3) However, in medicine we usually start with a specific case to reach a general conclusion (the opposite of deduc+on). This is called induc+on. We gather evidence in order to reach a conclusion. But the conclusions we reach are only probable, not certain. E.g. my pa+ent has a raised troponin, therefore he is having a heart aPack – not necessarily true (there are other causes of a raised troponin). People confuse deduc+on and induc+on.
4) Abduc+on is what doctors use most – working backwards from effects (symptoms/signs) to the most likely cause. What is the most likely diagnosis?
5) But then we also employ some other strategies: probabilis+c (what we did last +me) – thinking in terms of ‘likely’, ‘unsure’ or ‘unlikely’
6) We also use our knowledge of basic and clinical sciences to work things out in causal reasoning … e.g. in hyperthyroidism we would expect a low TSH and a high T4.
In genera+ng a differen+al diagnosis we use all of these types of reasoning, as well as ‘rules of thumb’ and paPern recogni+on (type 2 thinking). It’s a complicated blend of processes.
10

Clinicians use both Type 1 and Type 2 thinking, and both types are important in clinical decision-‐making. When encountering a problem that is familiar, clinicians employ paPern recogni+on and reach a working diagnosis or differen+al diagnosis quickly (Type 1 thinking). When encountering a problem that is more complicated, they use a slower, systema+c approach (Type 2 thinking). Both types of thinking interplay – they are not mutually exclusive in the diagnos+c process. Figure 1.6 illustrates the interplay between Type 1 and Type 2 thinking in clinical prac+ce.
Errors can occur in both Type 1 and Type 2 thinking – for example people can apply the wrong rules or make errors in their applica+on while using Type 2 thinking. However, it has been argued that the common cogni+ve biases encountered in medicine tend to occur when engaged in Type 1 thinking.
For example, imagine being asked to see a young woman who is drowsy. She is handed over to you as a ‘probable overdose’ because she has a history of depression and a packet of painkillers was found beside her at home. Her observa+ons show she has a Glasgow Coma Score of 10/15, heart rate 100 beats per minute, blood pressure 100/60 mmHg, respiratory rate 14 per minute, oxygen satura+ons 98% on air and temperature 37.5oC. Already your mind has reached a working diagnosis. It fits a paPern (Type 1 thinking). You think she has taken an overdose. At this point you can stop to think about your thinking (ra+onal override in Fig. 1.6). ‘What is the evidence for this diagnosis? What else could it be?’
On the other hand, imagine being asked to assess a pa+ent who has been admiPed with syncope. There are several different causes of syncope and a systema+c approach is required to get to a diagnosis (Type 2 thinking). However, you recently heard about a case of syncope due to a leaking abdominal aor+c aneurysm. At the end of your assessment, following evidence-‐based guidelines, it is clear the pa+ent can be discharged. Despite this, you decide to observe the pa+ent overnight ‘just in case’ (irra+onal override in Fig. 1.6). In this example, your intui+on is actually availability bias (when things are at the forefront of your mind) which has significantly distorted your es+mate of probability.
11

[read slide] Even highly skilled clinicians make errors because they are human. It is not a maPer of intelligence or memory – the human brain is wired to miss things that are obvious, see paPerns that do not exist, and jump to conclusions. In evolu+onary terms, speed of decision making was oten more important than accuracy. Clinicians are not exempt from these human characteris+cs. In his book Human Error (Cambridge University Press, 1990), psychologist James Reason argues that, ‘Our propensity for certain types of error is the price we pay for the brain’s remarkable ability to think and act intui+vely – to sit quickly through the sensory informa+on that constantly bombards us without was+ng +me trying to work through every situa+on anew.’ Even highly intelligent people fall in to the same cogni+ve traps or ‘cogni+ve biases’. Human thinking and decision making is in itself flawed.
12

This is an image from a CT scan of the thorax. Drew and colleagues from Harvard asked 23 consultant radiologists to look at CT scans of the thorax specifically to look for lung nodules. Unknown to the radiologists, the researchers inserted a matchbox-‐sized image of a gorilla in some of the scans. They found that 83% of the radiologists missed the gorilla, which was 45 +mes larger than the average lung nodule, even though they spent an average of 5.7 seconds looking at the gorilla-‐containing images and their eyes fixed briefly on the exact loca+on of the gorilla. This experiment highlights that we are only aware of a small part of our visual world at any one +me. We focus our aPen+on to filter out distrac+ons, but in focusing on what we are trying to see, we tend not to no+ce the unexpected.
13

14
Let’s try an experiment. If you have done this before, please keep quiet! Look at this sentence for a few moments -‐ how many ‘Fs’ are there?

15
How many people saw 2 Fs? 3? 4? 5? 6? (Usually there is a spread of answers across the group)

16
Here it is again.

17
There are 6 Fs – here they are highlighted. Now what is interes+ng about this experiment is that everyone in the room is smart. Everyone can read English. And we were all looking at the same thing. (If you got the correct answer, don’t be smug – something else will catch you out!)

Human factors is the science of the limita<ons of human performance. The fact is, the human brain is wired to jump to conclusions (like 10p), miss things that are obvious (like the F’s) and our es+mate of probability (in diagnos+c reasoning in my specialty) is poor. Recommend ‘the art of thinking clearly’ NYT bestseller, by Rolph Dobelli to find out more!
18

[tell story]
19

Cogni+ve biases fall in to 4 main groups: Social – peer pressure, ‘halo effect’ (when someone is good at one thing so you assume they are good at everything) Memory – hindsight bias (hindsight significantly impairs our ability to judge the quality of decision making that occurred in the past) Decision making – confirma+on bias and others in the hand out coming around now [HANDOUT] Probability/belief biases – e.g. Gambler’s fallacy, availability bias – more of that in a minute!
20
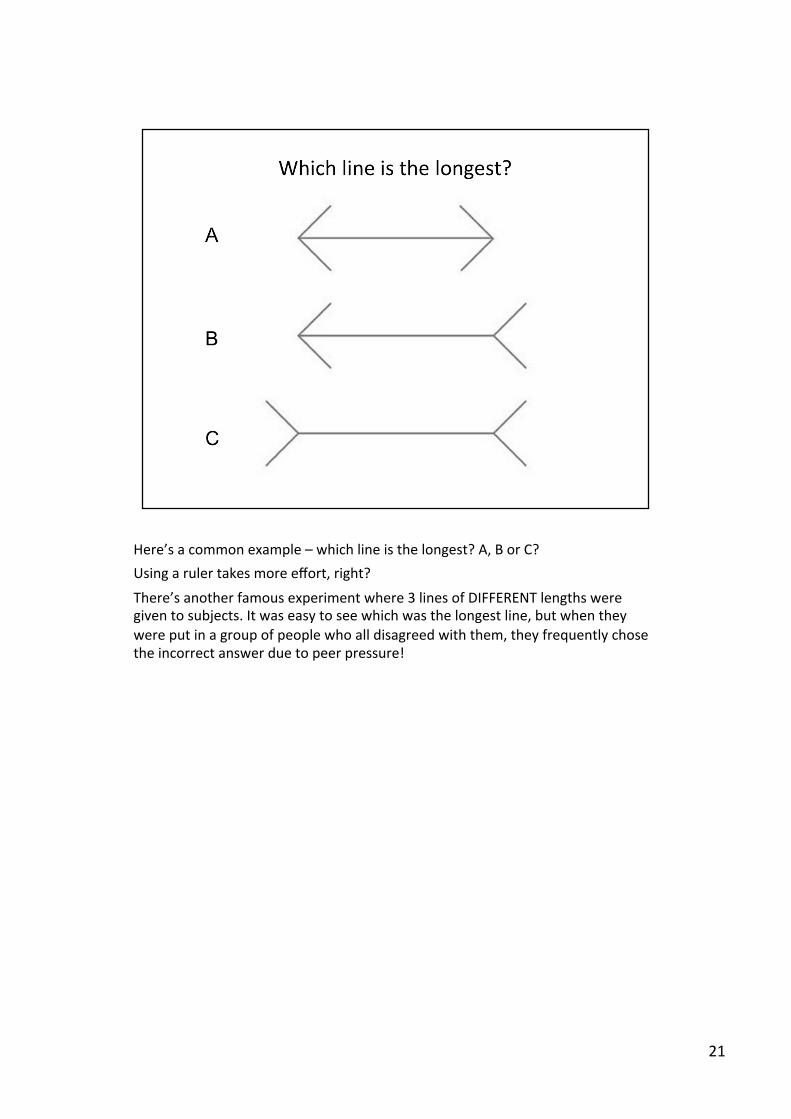
Here’s a common example – which line is the longest? A, B or C? Using a ruler takes more effort, right?
There’s another famous experiment where 3 lines of DIFFERENT lengths were given to subjects. It was easy to see which was the longest line, but when they were put in a group of people who all disagreed with them, they frequently chose the incorrect answer due to peer pressure!
21

Confirma+on bias is the tendency to look for confirming evidence to support a theory rather than looking for contradictory evidence to refute it, even if the laPer is clearly present. Confirma+on bias is common when you are seeing a pa+ent who has already been seen by another dr, who may be more senior than you. Actually, confirma+on bias is rife in everyday life: in general, people read newspapers that already support their views, browse internet sites that mirror their own values, and hang out with like minded people.
22
I like this one – fear of flying. Availability bias is when things are at the forefront of your mind because you have seen several cases recently or have been studying that condi+on in par+cular. There have been (what seems to be) a lot of airline crashes in the news recently. But neglect of probability (or base rate neglect) is the tendency to ignore the prevalence of something which then distorts our reasoning.
Of course, in life AND medicine, pure logic is some+mes NOT helpful when dealing with an anxious person!
23

[read slide]
24

25

26

Some of you may have been told about famous group think experiments where apparently normal intelligent people do really strange things because everyone else is doing it too.
Examples when I was a junior dr:
50 year old alcoholic man, abdo pain/vomi+ng, fever, ‘proteinuria’ = UTI (pancrea++s) 70 year old woman, CSF leak, immunosuppressed, new confusion = cons said ‘b cult if spikes temp’ (meningi+s)
27

28

Personality type and other individual characteris+cs influence decision making. Some people are naturally more confident (or over-‐confident) than others e.g. men vs women. Decisions are also made in context. My work environment is an accident wai+ng to happen: characterised by noise, interrup+ons, mul+-‐tasking and cogni+ve overload for example.
‘Comfortably numb’ we men+oned before – it refers to mindlessly adop+ng strategies to conserve thinking. This leads to problems: e.g. failure to do a thorough history and exam, blindly accep+ng informa+on from others, deferring to authority without ques+on, adop+ng a non-‐skep+cal approach … you must ques+on everything!
Healthcare providers cannot afford to be comfortably numb when pa+ent care is at stake.
29

[read slide] The areas of the brain required for Type 2 processes are most affected by sleep depriva+on and fa+gue … All factors combine to increase use of Type 1 processes and compromise func+on of Type 2 processes.
30

So no maPer how smart we are, our brains are wired to miss things and assume things … and make errors. So what can we do about it? [read slide]
31

James Reason is a well known psychologist who became famous for studying error in healthcare. He said this.
32

That’s it!
33

Cogni+ve biases should not be confused with ‘expert intui+on’ which is a common way experts make decisions – but only in their domain of exper+se. In 1973, two American psychologists took two groups of people – one consis+ng of chess masters and one consis+ng of novices – and showed them chessboards with 20-‐25 pieces on them, set up as if in the middle of a game. The subjects were shown the boards briefly and then asked to recall the posi+ons of the pieces. The chess masters were able to recall the posi+on of every piece on the board, but the novices could only recall four or five. The experiment was then repeated, but this +me the pieces were randomly distributed on the chess board. This +me, the chess masters were no bePer than the novices. Chess masters, with their years of experience, could look at the chess pieces in the middle of a game and see a paPern. The chess pieces were like lePers in a word, and like readers recognise whole words, chess masters are experts in the language of chess. But if they were asked to simply look at a jumble of lePers, they performed no bePer than everyone else.
Expert intui<on is really tacit knowledge. Although it involves intui+ve thinking, this is slightly different to the subconscious ‘assump+ons’ to which we are all prone, experts included. The apparent effortlessness is in fact not effortless at all -‐ 10,000+ purposeful prac+ce, feedback/coaching
34

You all know this word says “remember” because you recognise the word – you did not have to figure it out from the individual lePers. In the same way, expert chess players saw the pieces like lePers in a word, and expert clinicians see individual clinical features like lePers in a word – it seems effortless but the effort it took to get there is “hidden” from you. NOT the same as “jumping to conclusions” which we are going to discuss in more detail later.
35

Well, that has been a bit of a whirlwind tour of cogni+ve bias and human factors in radiology. I have e-‐mailed two pdf files to Cheika Kennedy, one is a good ar+cle covering errors in radiology and the other is common cogni+ve biases in medicine.
You might also find these websites useful – the first is the website for our GEM students and the other is the UK Clinical Reasoning in Medical Educa+on group website – they hold an annual conference. Both have a recommended reading list, popular, for students/teachers, and academic, if you want to know more. And there’s the TwiPer handles there. Well, thank you for listening and if there’s one thing I can say to console you – at least the error rate in Radiology is less than in Internal Medicine!!
36

So in your PBL sessions try and spot when you might be subconsciously filling in gaps/jumping to conclusions when really you don’t know.
37