diagnosis and management of hyperthyroidism, a rational approach kashif munir, m.d. assistant...
TRANSCRIPT

Diagnosis and Management of Hyperthyroidism, A Rational Approach
Kashif Munir, M.D.Assistant Professor of Medicine
Division of Endocrinology, Diabetes & NutritionUniversity of Maryland School of Medicine

Definitions
• Thyrotoxicosis - clinical state that results from inappropriately high thyroid hormone action in tissues generally due to inappropriately high tissue thyroid hormone levels
• Hyperthyroidism – a form of thyrotoxicosis due to inappropriately high synthesis and secretion of thyroid hormone(s) by the thyroid
Bahn et al. Hyperthyroidism and Other Causes of Thyrotoxicosis: Management Guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Thyroid, 2011 Jun;21(6):593-646 & Endocr Pract, 2011 May-Jun;17(3):456-520

Epidemiology/etiology
• Prevalence 1.2% (0.5% overt, 0.7% subclinical)• Graves’ disease• Toxic nodule/s• Subacute thyroiditis

Low TSH, High RAIUGrave’s disease Toxic MNGToxic AdenomaChorionic gonadotropin-inducedInherited non-immune hyperthyroidism (TSH receptor or G protein mutations)
Low TSH, Low RAIUIodine-induced hyperthyroidismAmiodarone-associated hyperthyroidism (due to excess iodine release)
Thyroiditis:Autoimmune
Lymphocytic thyroiditis (silent, painless, postpartum)Acute exacerbation of Hashimoto’s
Viral or post viralSubacute (granulomatous, painful, post viral)
Drug-inducedAmiodaroneLithium, interferon-α, IL-2, GM-CSF
Infectious (acute)Post-partum
Iatrogenic over-replacementThyrotoxicosis factitiaIngestion of natural products containing thyroid hormone
“Hamburger” thyrotoxicosisNatural foodstuffsThyromimetic compounds (e.g. Tiracol)
Occupational exposure to thyroid hormonePill manufacturingVeterinary occupations
Struma OvariiMetastatic functioning thyroid carcinomaNormal/Elevated TSH
TSH-secreting pituitary tumorsThyroid hormone resistance

Is low TSH enough to diagnose thyrotoxicosis?

Biochemical evaluation
• TSH has highest sensitivity and specificity• Diagnostic accuracy improves with measurement
of free T4• Free T4 gives baseline measurement of degree
of thyrotoxicosis– Important for monitoring success of initial treatment– Though not always related to severity of symptoms
• T3 toxicosis– Can be sign of early disease

Spencer et al. J Clin Endocrinol Metab. 1990 Feb;70(2):453-60.
TSH and free T4 have inverse log-linear relationship

• Thyrotoxicosis/Hyperthyroidism:– Low or suppressed TSH (< 0.1 mIU/L)– Elevated T4, elevated T3 or both
• Subclinical Hyperthyroidism– Low or suppressed TSH (< 0.4 mIU/L)– Normal T4 & T3

Subclinical hyperthyroidism
• Document by repeating TSH in 3-6 months– Can spontaneously resolve
• Increased rates of atrial fibrillation in the elderly
• Increased risk of osteoporosis/fracture• Possible increased risk of mortality

Subclinical hyperthyroidism
• Treat if TSH persistently < 0.1 mU/L in persons 65 years or older, postmenopausal women, patients with cardiac risk factors, osteoporosis, or symptoms of thyrotoxicosis
• Consider treating younger patients with symptoms and TSH < 0.1 mU/L
• Consider treating older patients with TSH ≥ 0.1 mU/L with cardiac disease or symptoms

Is ultrasound indicated in the work-up of thyrotoxicosis?

• Thyroid Ultrasound– Color Doppler Flow helpful in AIT 1 vs. AIT 2.– May reveal nodular disease or increased
vascularity (seen in Grave’s)• Thyroid Uptake & Scan– High uptake:• Graves’, toxic MNG, toxic adenoma
– Low uptake:• Thyroiditis, iodine-induced hyperthyroidism
ATA/AACE guidelines
“Ultrasonography does not generally contribute to the differential diagnosis of thyrotoxicosis”
• Radioiodine uptake should be done when clinical presentation not diagnostic of Graves’– Scan added in presence of nodularity

Toxic adenoma

Alzahrani et al. Endocrine Practice. 18(4): 567-578
Suggestion to add US to diagnostic algorithm for thyrotoxicosis• Cost effectiveness• Non-invasive• Detection of nodules• Avoidance of radiation
exposure

“Thyroid inferno” – seen in Graves’ disease (color doppler US)

Zuhur et al. Endocr Pract. 2013 Nov 18:1-36.

Zuhur et al. Endocr Pract. 2013 Nov 18:1-36.
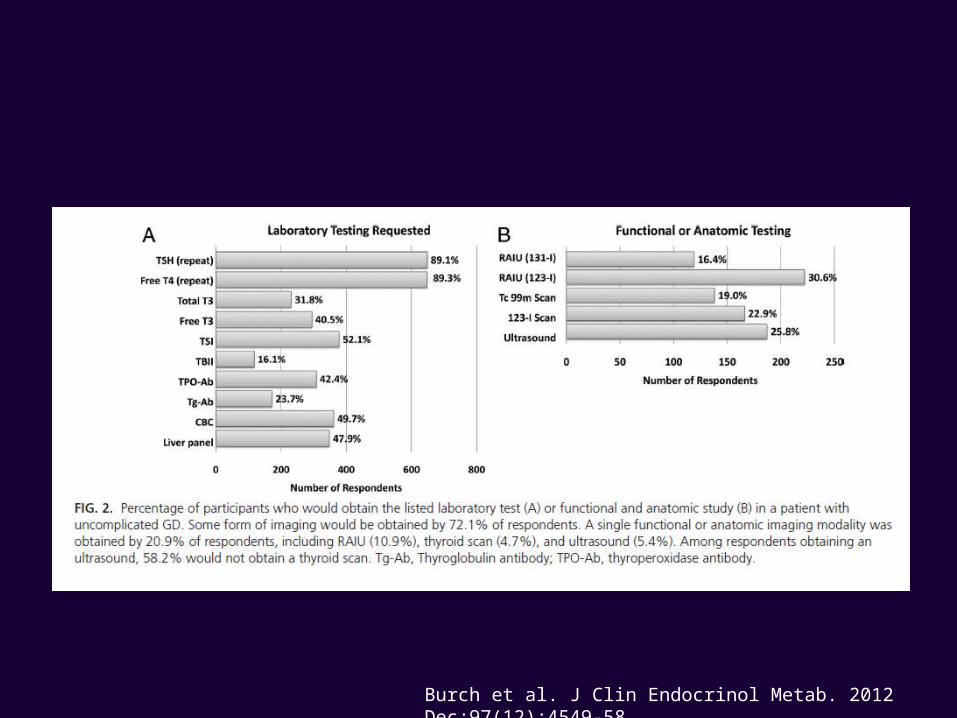
Burch et al. J Clin Endocrinol Metab. 2012 Dec;97(12):4549-58

How is hyperthyroidism best treated?

Treatment
• Goals:– Normalize serum TSH levels – Reverse\correct clinical signs & symptoms and
metabolic derangements.• Beta-blockers• Antithyroid medication• I-131• Surgery

Burch et al. J Clin Endocrinol Metab. 2012 Dec;97(12):4549-58

Burch et al. J Clin Endocrinol Metab. 2012 Dec;97(12):4549-58

Burch et al. J Clin Endocrinol Metab. 2012 Dec;97(12):4549-58

Medical therapy
Methimazole (MMI) – 5-30 mg daily Propylthiouracil (PTU) – 100-300 mg per day divided BID/TID
• Inhibit the synthesis of thyroid hormones– Interfere with iodination of tyrosine residues– Effects seen 1-2 weeks after initiation of therapy.
• Side effects:– Rash, arthralgias, nausea– Vasculitis– Liver function tests abnormalities (liver failure with PTU)– Agranulocytosis– Embryopathy Check baseline CBC/diff and LFT’s

PTU black box
Reserved for early pregnancy; thyroid storm; mild intolerance to methimazole in patients not wanting RAI or surgery

Andersen et al. J Clin Endocrinol Metab. 2013 Nov;98(11):4373-81

Methimazole
• Primarily used first line in Graves’– Not generally considered first line therapy for toxic nodular goiter
• Chance for ‘remission’ (euthyroid 1 year after treatment ceased)– More likely in smaller goiter, milder disease, lower antibody titer
• Pretreatment of patients awaiting RAI or surgery – stop 3-5 days prior to RAI
• Once daily dosing – 5 to 30 mg/day• Monitor labs every 4-6 weeks initially – free T4/T3
– TSH suppression can lag for months• Treat for 12-18 months

Methimazole
• Once daily dosing – 5 to 30 mg/day• Monitor labs every 4-6 weeks initially – free
T4/T3– TSH suppression can lag for months
• Treat for 12-18 months• Consider measuring thyroid receptor
antibodies to predict remission

Radioactive Iodine
• Beta-blockers often peri-therapy• Pregnancy- absolute contraindication• Graves’ disease – goal is hypothyroidism after
treatment – Fixed dose or calculation (weight [g] x 150 µCi/g x 1/24
hour uptake %)• Toxic MNG and Toxic Adenoma – can be eu-
thyroid following treatment• May repeat in 6 months if initial dose not effective

Surgery
– May need pre-op preparation with super-saturated potassium iodine (SSKI) to decrease vascularity of gland (Graves’ disease, large goiters).
– Continue anti-thyroid meds and beta blockers.– Levothyroxine replacement following surgery.– Total thyroidectomy for Graves’, partial possible
for toxic nodular goiter

Graves’ ophthalmopathy
• Up to 50% may have eye involvement• Can be euthyroid or hypothyroid in small minority
(< 10 %)• High dose steroids• Radiation• Surgery – orbital decompression• Selenium• Supportive therapies (lubricants, prisms, etc.)• Alternative therapies (e.g. rituximab, botox)

Stan et al. Med Clin N Am 96 (2012) 311–328

Bartalena L. J Clin Endocrinol Metab, March 2011, 96(3):592–599

Summary
• Thyrotoxicosis is a common condition encountered in practice
• Subclinical disease is more common than overt thyrotoxicosis
• TSH best for screening and free T4 for confirmation and monitoring treatment
• Radioiodine uptake and scan preferred imaging modality
• Treatment with methimazole or I-131 usually preferred