diagnosis and treatment of
TRANSCRIPT

Diagnosis and Treatment ofDiagnosis and Treatment of Hyperprolactinemia: yp p
N hid Shi i MD• Nahid Shirazian MD. • Internist, Endocrinologist

An Endocrine Society Clinical Practice Guideline(J Clin Endocrinol Metab 96: 273–288, 2011)
Strong recommendations use phrase “we recommend” & number 1number 1
Weak recommendations use the phrase “we suggest” & number 2.number 2.
Cross filled circles indicate quality of the evidence:Cross‐filled circles indicate quality of the evidence: ⊕ denotes very low quality evidence; ⊕⊕, low quality; , q y;⊕⊕⊕, moderate quality; ⊕⊕⊕⊕, high quality.
2

• Prolactin synthesis & secretion by pituitary lactotroph cells
• Prolactin acts to induce & maintain lactation of the primed breast.
3

Regulation ofRegulation of PRL Cycle

Regulation of hypothalamic‐pituitary‐prolactin axisprolactin axis
• predominant effect of hypothalamus is inhibitory, h di i i ll b b h h lthat mediate principally by tuberohypophysealdopaminergic neuron system & dopamine D2
l hreceptors on lactotrophs.
• dopamine neurons;stimulated by acetylcholine (ACh) & glutamatestimulated by acetylcholine (ACh) & glutamate inhibited by histamine & opioid peptides.

Regulation of hypothalamic‐pituitary‐prolactin axisprolactin axis
• One or more prolactin‐releasing factors (PRFs) probably mediate acute release of PRL ( i kli d i t )mediate acute release of PRL (e.g., in suckling, during stress).
Th l did PRF• There are several candidate PRFs;thyrotropin‐releasing hormone (TRH), vasoactive intestinal polypeptide (VIP),
oxytocin.
• PRF neurons are activated by serotonin (5‐HT).
• Estrogen sensitizes pituitary to release PRL.

Regulation of hypothalamic‐pituitary‐prolactin axis‐prolactin axis
• ultra short‐loop feedback; Prolactin on pituitary regulate its own secretion
• Prolactin also influences gonadotropin secretion by suppressingProlactin also influences gonadotropin secretion by suppressing release of luteinizing hormone–releasing hormone (LHRH).
• Short‐loop feedback; mediated indirectly by PRL receptor regulation of hypothalamic dopamine synthesis, secretion, & turnover.
• CNS, central nervous system; GABA, γ‐aminobutyric acid.


prolactin levels in women prolactin levels in men
25 µg/l~ ng/ml 20 µg/l~ ng/ml 25 µg/l ng/ml µg g

• To establish diagnosis of hyperprolactinemia, we recommend a single measurement of serum gprolactin;
• A level above upper limit of normal confirms diagnosis as long as serum sample was obtained g g pwithout excessive venipuncture stress.
• We recommend against dynamic testing of prolactinsecretion for diagnosis of hyperprolactinemiag yp p(1 ⊕⊕⊕⊕).
10
D i t t f l ti ti i• Dynamic tests of prolactin secretion using;
TRHTRH, L‐dopa, if inomifensine,
Domperidone
are not superior to measuring a single serum prolactin sample
for diagnosis of hyperprolactinemia.
11

• Men & non‐pregnant women will normally have only small amounts of prolactin in their blood.
• Prolactin levels do, however, need to be evaluated based on the time of day that they are collected.
• The levels will vary over a 24‐hour period, rising during sleep & peaking in morning.
• Ideally, a person's blood sample should usually beIdeally, a person s blood sample should usually be drawn shortly after waking, preferably after person has been resting quietly for 30 minutes, although a doctor may have his own reasons for doing them at other times.

• Initial determination of serum prolactinpshould avoid excessive venipuncture stress & can be drawn at any time of day.
• When in doubt, sampling can be repeated on a different day at 15 to 20 min intervals toa different day at 15‐ to 20‐min intervals to account for possible prolactin pulsatility.

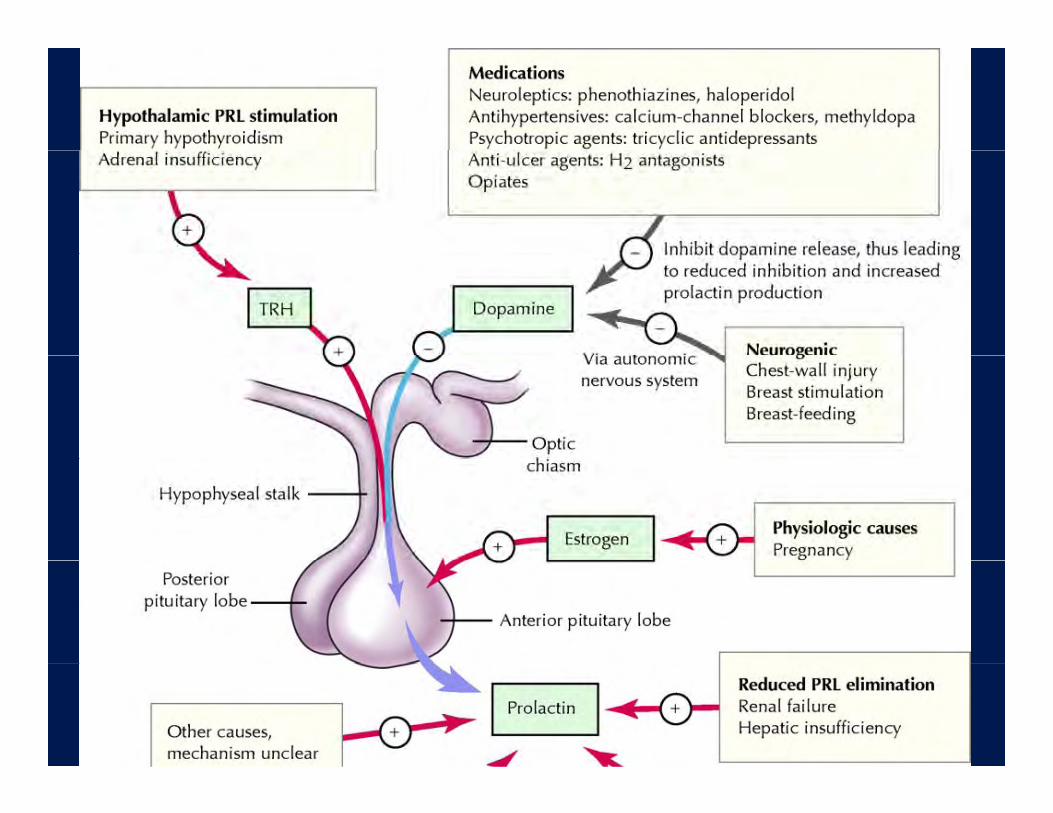
Causes ofhyperprolactinemiayp p
Copyright ©2003 Canadian Medical Association or its licensors
Serri, O. et al. CMAJ 2003;169:575‐581


Cause of hyperprolactinemia1 Physiologic hypersecretion1. Physiologic hypersecretion
PregnancyLactation Chest wall stimulation
5. Hypothalamic–pituitary stalk damageTumorsChest wall stimulation
SleepStress
CraniopharyngiomaSuprasellar pituitary mass extension
2. Pituitary hypersecretionProlactinomaAcromegaly
MeningiomaDysgerminomaMetastasesEmpty sellaAcromegaly
3. Systemic disordersChronic renal failure
Empty sellaLymphocytic hypophysitisAdenoma with stalk compressionGranulomasChronic renal failure
HypothyroidismCirrhosisEpileptic seizures
GranulomasIrradiationTraumaPituitary stalk sectionEpileptic seizures
4. Drug‐induced hypersecretion
ySuprasellar surgery

Serum prolactin concentrations increase duringpregnancypregnancy

Serum prolacin & suckling

Ranges of serum prolactin concentrations in several causes ofhyperprolactinemiayp p

• We recommend excluding;
medication use, renal failure,
hypothyroidism, &
parasellar tumorsparasellar tumors
in patients with symptomatic nonphysiologicalhyperprolactinemia (1 ⊕⊕⊕⊕). 21

• Prolactin level > 500 g/lit is diagnostic of aProlactin level > 500 g/lit is diagnostic of a macroprolactinoma.
• Although a prolactin level > 250 g/lit usually indicates presence of prolactinoma, selected drugs, i l di i id & l idincluding risperidone & metoclopramide, may cause prolactin elevations > 200g/lit in patients without evidence of adenoma.evidence of adenoma.
• Even minimal prolactin elevations may beEven minimal prolactin elevations may be consistent with presence of a prolactinoma, but a non‐prolactin‐secreting mass should first be
id dconsidered.22
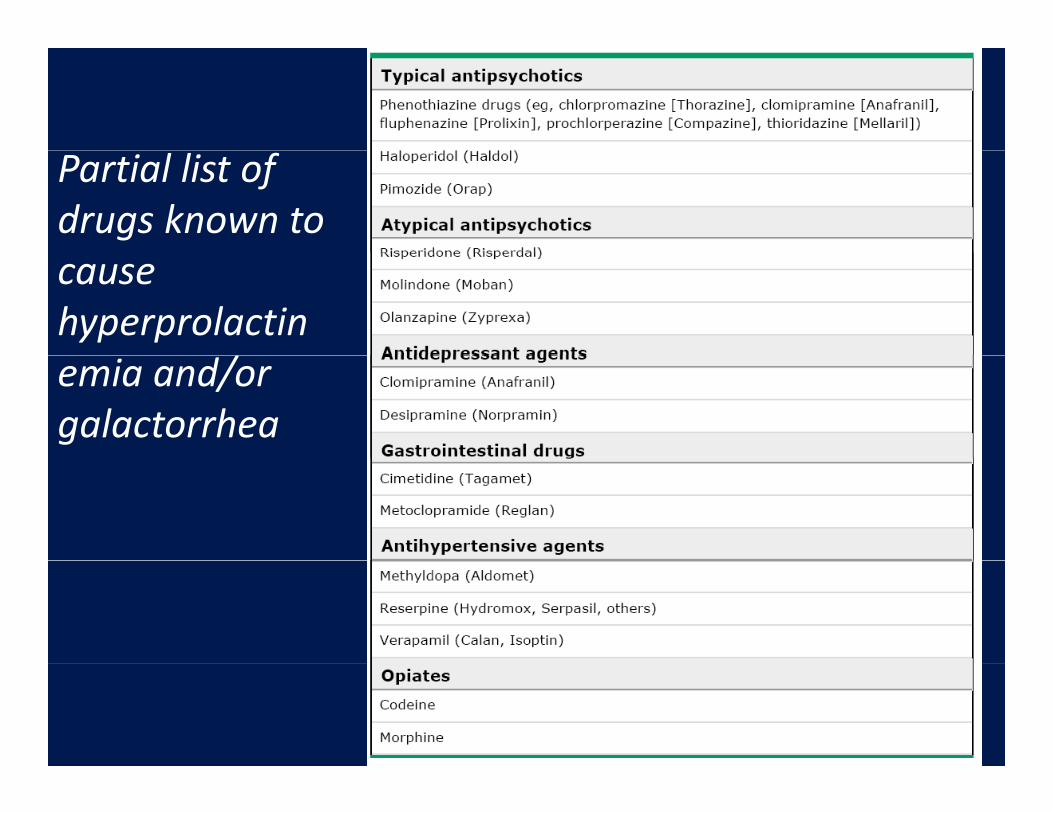
Partial list of drugs known to cause hyperprolactinemia and/or galactorrhea

Symptom of Hyperprolactinemie
• hypogonadism, low LH, low FSH, low stradiol
• infertility, li h h• oligomenorrhea, amenorrhea
• less often by galactorrhea• less often by galactorrhea.• Low BMDLow BMD

MenMen• hypogonadotropic hypogonadism in men, • decreased libidodecreased libido,• decreased energy & libido, • decreased muscle massdecreased muscle mass, • body hair, • osteoporosis• osteoporosis. • impotence, • infertility• infertility, • gynecomastia, • rarely galactorrhea• rarely galactorrhea• Erectile dysfunction

Case 1female 26y amenorrhea LMP; 3 months agofemale, 26y amenorrhea. LMP; 3 months ago, 3 home pregnancy tests ; negative. Takes no medications.M h 12 t l l l til 3 thMenarche ; age 12 years, menstrual cycles regular until 3 months ago. Weekly headaches, Occasional induced galactorrhea. Physical examination; normal. Serum prolactin level; 1665 ng/mL(1665 mg/L)
Which of the following is the most likely cause of thisWhich of the following is the most likely cause of this patient's hyperprolactinemia?
A PA. PregnancyB. CirrhosisC. Primary hypothyroidD. Prolactin‐producing pituitary tumor


Tumor size correlates positively withTumor size correlates positively with serum PRL levels
PRL level > 100 ng/mLis strongly indicative of a
PRL-secreting pituitary tumorPRL-secreting pituitary tumor


Adenomas <1 cm Adenomas1‐2 cm Adenomas>2 cm
below 200 ng/mL 200‐1000 ng/mL above 1000 ng/mL

A "giant" prolactinoma

Case 2Case 2
• Female 45y, Headachey,• Lab: prolactin 56 ng/ml, p gE2 < 10 pg/ml, FSH 8.3 mIU/ml, LH 2.8 mIU/ml, T4 5.54, TSH 2.57 uIU/ml, Cortisol 8 AM 7.49 ug/dl
next step?

• CT scan of brain:CT scan of brain:Sphenoid sinus mass (2 cm) / i i i h i i iR/o pituitary tumor with intra‐sinus extension

Diagnosis of ProlactinomasDiagnosis of Prolactinomas
• Prolactin is secreted episodicallyProlactin is secreted episodically• Nonsecreting tumor causing modest prolactin elevations (usually < 150 ng/ml)elevations (usually < 150 ng/ml)
• Prolactin‐secreting macroadenoma (prolactin l l ll 250 / l)levels usually > 250 ng/ml)
• MRI with gadolinium enhancement

If tumor size not correlation with serum PRL levels :with serum PRL levels :
1. Hook effect
2. Necrosis or cystic of tumor
3. Mass effect (other adenoma)
4. IGF-1

two‐site immunoradiometricassayassay

Hook Effect
• In immunometric assays, it is also important that a large excess of capture antibody be usedlarge excess of capture antibody be used.
A h i i h h ff i• As the antigen concentration approaches the effective binding capacity of the capture antibody system, the signal no longer increasessignal no longer increases.
• If the antigen concentration exceeds binding capacity of capture antibody, the signal may actually decrease.

• second (signaling) antibody binds directly to excess prolactin remaining in solution &, therefore, is less available to prolactin already bound to firstavailable to prolactin already bound to first (coupling) antibody.
• the assay should be repeated after a 1:100 serum sample dilution to overcome a potential hook effect.p p
• We recommend that this artifact be excluded in patients who have pituitary macroadenomas &
tl l ildl l t d l tiapparently normal or mildly elevated prolactinlevels.
38

Hook Effecct;

Hook Effect
• This is a potentially dangerous phenomenon, because the same values might be measured with very high & lower concentrations.
• we recommend serial dilution of serum samples to eliminate an artifact that can occur with someeliminate an artifact that can occur with some immunoradiometric assays leading to a falsely low prolactin value (“hook effect”). (1 ⊕⊕⊕⊕).
• If measured value for diluted specimen is higher than original result,
a high‐dose hook effect probably is present.

Hook Effect• Most manufacturers are aware of this potential problem & configure• Most manufacturers are aware of this potential problem & configure
assays with relatively large amounts of capture antibody; however, some patients produce high concentrations of hormones or antigens that may exceed assay limits.
• Laboratories can detect this phenomenon by analyzing specimens at 2 dilutions, but this practice generally is not cost‐effective.
• Therefore, feedback to laboratory about results that are inconsistent with clinical findings is essentialare inconsistent with clinical findings is essential.

Goals of therapyGoals of therapy
The goals of therapy are :The goals of therapy are : • to normalize prolactin, • to restore fertilityto restore fertility, • to reduce tumor size, • to ameliorate the symptoms of hypogonadism• to ameliorate the symptoms of hypogonadism.
• All patients with macroadenomas & most patients with• All patients with macroadenomas & most patients with microprolactinoma require treatment.

Prolactinoma
prolactinomas are more amenable toprolactinomas are more amenable to pharmacologic treatment
than any other kind of pituitary adenoma because of availability of dopamine agonists,
decrease both secretion &&
size of these tumors.

Shrinkage of prolactinoma after bromocriptine



Pharmacological options:
Dopamine agonist
1. Bromocriptine2 Cabergoline2. Cabergoline3. Pergolide4. Quinoglideg
l l l lNormalize prolactin levels.Reduce the volume of the tumor.

In all cases treatment withIn all cases, treatment with any dopamine agonist should useany dopamine agonist should use
lowest dose &
shortest duration possible.
Big & Big Big Prolactin:
• 85% of circulating prolactin is imonomeric (23.5 kDa),
• serum also contains a covalently bound dimer(polimerization), “big prolactin,”
• a much larger polymeric form(tetramer), g p y ( )“big‐big prolactin.”
• Antiprolactin autoantibodies may also be associated with macroprolactinemia.49


Big & Big Big Prolactin:
• macroprolactinemia denotes situation in which a preponderance of the circulatingwhich a preponderance of the circulating prolactin consists of these larger molecules.
• These polymers have a lower bioactivity &slower clearance than monomeric form.

In patients withIn patients with asymptomatic hyperprolactinemia, weasymptomatic hyperprolactinemia, we suggest assessing for macroprolactin
(2 ⊕⊕)(2 ⊕⊕).
52

Big & Big Big Prolactin:
• Retrospective analyses of patients with hyperprolactinemia ; ~ 40% have macroprolactinemia 40% have macroprolactinemia.
• a smaller proportion of patientsi h l i iwith macroprolactinemia
has signs & symptoms of hyperprolactinemia, l h i i 20%galactorrhea is present in 20%, oligo/amenorrhea in 45%,
& i i d i 20%& pituitary adenomas in 20%.53

Big & Big Big Prolactin:
• Polyethylene glycol precipitation is an y y g y p pinexpensive way to detect presence of
macroprolactin in serum.p
54

macroprolactin
• High concentrations of polyethylene glycol (PEG) precipitate macroprolactin from serumprecipitate macroprolactin from serum.
• Mean recovery of PRL from serum containing only monomeric PRL as 86% (ran e 71 106%)monomeric PRL was 86% (range, 71–106%).
• Macroprolactin can be detected by low PRL recovery after precipitation with PEG, & recovery allows an estimate of monomeric PRL.
• A cutoff of 50% has been used and validated with the Delfia assay to identify presence of macroprolactin.

Thanks For Your Att tiAttention