diaphragmatic hernia - pmj.bmj.com · to be a congenital diaphragmatic hernia, andnofurther action...
TRANSCRIPT
POSTGRAQ. MED. J. (I96I), 37, 191
DIAPHRAGMATIC HERNIAE. HOFFMAN, M.D., F.R.C.S.
Thoracic Surgeon to the Newcastle upon Tyne Regional Chest Surgery Service, Poole Hospital, Middlesbrough
DIAPHRAGMATIC HERNLZE are being recognizedwith increasing frequency. Herniation of ab-dominal contents into the thoracic cavity mayoccur through sites of embryological fusion,through the cesophageal hiatus, or followingtraumatic rupture of the diaphragm.
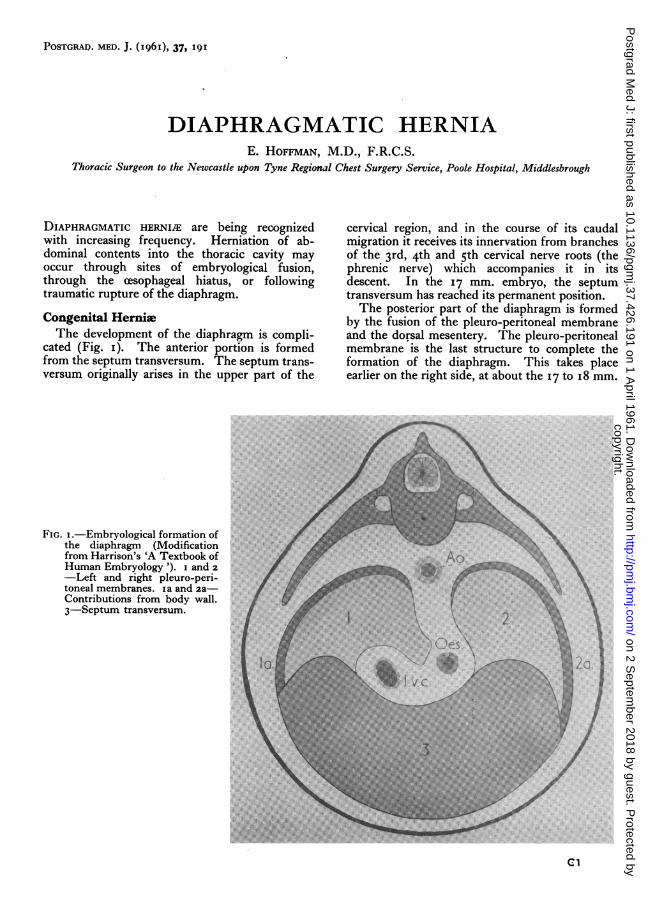
Congenital HerniaThe development of the diaphragm is compli-
cated (Fig. i). The anterior portion is formedfrom the septum transversum. The septum trans-versum originally arises in the upper part of the
cervical region, and in the course of its caudalmigration it receives its innervation from branchesof the 3rd, 4th and sth cervical nerve roots (thephrenic nerve) which accompanies it in itsdescent. In the 17 mm. embryo, the septumtransversum has reached its permanent position.The posterior part of the diaphragm is formed
by the fusion of the pleuro-peritoneal membraneand the dorsal mesentery. The pleuro-peritonealmembrane is the last structure to complete theformation of the diaphragm. This takes placeearlier on the right side, at about the 17 to i8 mm.
...
.... o...
0-R6IW1
FIG. I.-Embryological formation ofthe diaphragm (Modificationfrom Harrison's 'A Textbook ofHuman Embryology '). i and 2-Left and right pleuro-peri-toneal membranes. ia and 2a-Contributions from body wall.3-Septum transversum.
cl
copyright. on 2 S
eptember 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.426.191 on 1 April 1961. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
embryonic stage, and later on the left side at aboutthe 19 to 20 mm. stage. Before the formation ofthe pleuro-peritoneal membrane, there is a freecommunication between the pleural and peritonealcavities, the ' hiatus pleuro-peritonealis '. Inabout the ioth week of fuetal life, the herniatedintestines return from the umbilical cord to theabdominal cavity, and if the pleuro-peritonealcanal is still open, loops of bowel will herniate intothe pleural cavity (Bochdalek hernia). Embryo-logical sites of fusion of the diaphragm are sites ofpotential weakness and it is at these points thatcongenital hernia occur.The following cases are examples of these types
of hernia.
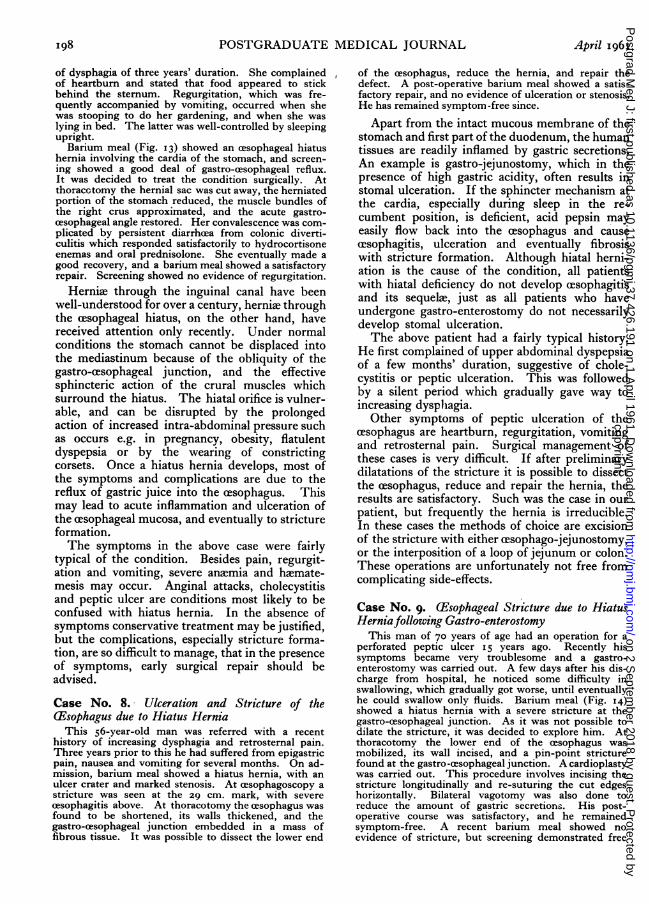
Case No. I. Congenital Diaphragmatic Hernia inthe Newborn (Bochdalek Hernia)
This baby was found to be dyspnreic and cyanosed atbirth. X-ray of the chest (Fig. 2) showed the right chestto be filled with intestines, which were displacing themediastinum to the left. At thoracotomy his chest wasfound to be filled with loops of small and large intestine.These were reduced, and the hernial orifice, which waslocated in the postero-lateral part of the diaphragm,was sutured. He made an uneventful recovery, and anX-ray showed satisfactory expansion of his lungs.
Herniae of the postero-lateral part of the dia-phragm (through the foramen of Bochdalek) arethe most common type of congenital diaphragmatichernia in the newborn. Surgical repair should becarried out preferably within the first 48 hours oflife. The operative mortality, unfortunately, ishigh, this being partly due to the frequent presenceof a hypoplastic lung, which does not inflate afterreduction of the contents of the hernia. Thistype of hernia contains no sac, and is therefore a' false ' hernia.
Case No. 2. Congenital Diaphragmatic Hernia(Bochdalek Hernia) in a Boy aged 2
This boy was referred for further investigation be-cause of failure to thrive, and attacks of abdominal colic.His chest X-ray (Fig. 3) showed gas-containing shadowssuggestive of intestines at the left base. However, it wasnot possible to assess whether these were above or belowthe diaphragm. Barium enema (Fig. 4) demonstratedcolon in the chest. A thoracotomy was carried out andherniated loops of small and large intestines were foundin the chest; there was no hernial sac present. Thesewere reduced, and the hemial orifice, which was foundto be at the site of the foramen of Bochdalek, was re-paired. His post-operative X-ray was satisfactory.The great majority of infants born with these
congenital defects, if untreated, die in the first fewhours or days. A few, however, may survive toadult life, and the hernia be discovered incidentallyat routine X-ray examination.
Case No. 3. Congenital Retrosternal (Parasternal)Diaphragmatic Hernia (Morgagni Hernia)
This 72-year-old man had had a productive cough with
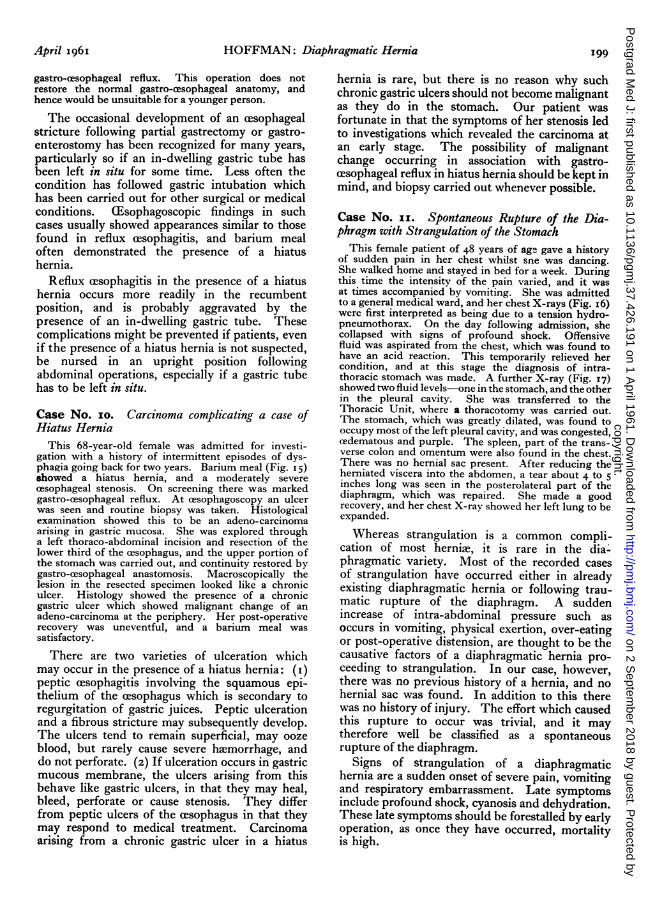
increasing dyspnea for 2 years. X-ray of his chest(Fig. 5) showed a rounded cystic opacity in the rightcardiophrenic angle. A lateral film showed that the air-containing opacity was situated retrosternally. Bariummeal showed the stomach and small intestine to benormal. Barium enema (Fig. 6) demonstrated part ofthe large bowel to be herniated into his chest. Furtherquestioning elicited the information that he had sufferedfrom flatulence for the past io years. A right thora-cotomy was carried out, the hernia reduced, and thehernial orifice repaired. His post-operative con-valescence was uneventful, and an X-ray of his chest wassatisfactory.
This type of congenital hernia is due to theabnormal development of that portion of thediaphragm which is formed from the fusion of theembryonal septum transversum, and the body wallcomponents. This hernia is probably not as rareas previously thought, since symptoms are presentin only a small proportion of patients. If thecontents of the hernial sac are extraperitoneal fator omentum, not adherent to the sac, symptomsare unlikely. If these structures become ad-herent, symptoms, particularly pain, may occurdue to traction. Transverse colon in the sacproduces symptoms which are predominantlyabdominal. The patients usually complain ofintermittent attacks of colic, bouts of abdominaldistension, and sometimes vomiting. If the con-tents of the hernia are extraperitoneal fat oromentum, then the shadow seen radiologically isopaque; if bowel is present, then the typical air-containing space is seen (Figs. 5 and 6).The majority of cases do not require surgery, as
they have no symptoms. When colon is present,however, operation should be carried out whethersymptoms are present or not, because of thedanger of strangulation.The following two cases demonstrate congenital
malformations of the diaphragm which may bemistaken for congenital diaphragmatic herniae.
Case No. 4. Eventration of the DiaphragmThis man of 49 years of age was admitted with a
io-year history of dyspepsia, which did not fit any typicalpattern, and was not related to meals. His X-rays(Figs. 7 and 8) showed an elevated left diaphragm, whichmoved sluggishly on screening. Barium meal (Fig. 9)showed no evidence of hiatus hernia, but the stomachwas inverted, giving the characteristic ' fish-hook 'appearance, recognized as being typical of an eventration.At thoracotomy the diaphragm was found to be thin,lax, and lying in folds; it was incised, overlapped andsutured. He made a good recovery, and was relieved ofhis symptoms.
Eventration is included here because it is easilyconfused with diaphragmatic hernia, as the symp-toms and radiological appearances are similar. Inits literal meaning, eventration should signifyactual herniation, but the accepted meaning of theterm is used to describe a condition of an abnormalelevation of the intact diaphragm. True eventra-
.Appril I96II92
copyright. on 2 S
eptember 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.426.191 on 1 April 1961. D
ownloaded from

HOFFMAN: Diaphragmatic Hernia
FIG. 2.FIG. 3.
FIG. 5.FIG. 4.
"April I96 I
,F.6.k.'.&
copyright. on 2 S
eptember 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.426.191 on 1 April 1961. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
FIC. 7.
FIG. 6.
FIG. 9.FIG. 8.
April I96II94copyright.
on 2 Septem
ber 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.426.191 on 1 A
pril 1961. Dow
nloaded from

April I96I HOFFMAN: Diaphragmatic Hernia
FIG. I0.
FIG. II.
:..,-.... aK,
3:..-*. ....s
..: ..;;.-*-'-
FIG. I2.
FIG. 13.
I
copyright. on 2 S
eptember 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.426.191 on 1 April 1961. D
ownloaded from

I96 POSTGRADUATE MEDICAL JOURNAL April I961
4FIG. 15.FIG. 14.
FIG. i6.
i
i
Tl--
FIr.. 17.
copyright. on 2 S
eptember 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.426.191 on 1 April 1961. D
ownloaded from

HOFFMAN: Diaphragmatic Hernia
tion is of congenital origin. The term eventrationshould not be used in conditions where there is anelevated diaphragm due to phrenic nerve paralysis.Eventration results when there is failure of muscledevelopment; whereas in phrenic nerve paralysis,the diaphragm shows a normally developed musclewhich is atrophic. In eventration movements ofthe affected leaf of the diaphragm may be greatlydiminished, but there is no paradoxical movementas when the phrenic nerve is paralysed.
In the majority of cases, treatment is un-necessary, but in people who have symptoms,surgery should be considered. Considerablerelief may be obtained by plication of the affecteddiaphragm.
Case No. 5. Partial Eventration of the RightDiaphragm. 'Herniation ' of the Liver into theChestThis 43-year-old man was admitted for investigation
of a large ovoid homogeneous opacity at the right base(Fig. io). Radiologically it was not possible to decideif the lesion was in the chest, in the abdomen or arisingfrom the diaphragm. He had a three years' history ofproductive cough and shortness of breath. Barium mealshowed no evidence of a diaphragmatic hernia. Adiagnostic pneumoperitoneum was therefore induced(Fig. i i). The lateral two-thirds of the lower surfaceof the right diaphragm was clearly outlined, but the airfailed to show the upper margin of the mass. From thisit was concluded that the opacity was formed by theliver. Pneumoperitoneum is not capable of differ-entiating between a diaphragmatic hernia and an even-tration, due to the fact that adhesions between thediaphragm and visceral pleura seal off the com-munication.At thoracotomy it was found that the liver was pro-
truding into the chest through the intact diaphragm,which was stretched over its upper surface, and adherentto it. There was no evidence of hernia or tear in thediaphragm. Nothing further was done and the chestwas closed.
The differential diagnosis which had to beconsidered in this case was a true hernia of theliver. A hernia of the liver usually follows severetrauma to the chest or abdomen. The injury hasoften taken place so many years ago that thepatient fails to recall it, or feels that it has noconnection with his present complaints, especiallyas the condition can be entirely asymptomatic, andmay be discovered only at routine X-ray exami-nation. Since these lesions eventually producesymptoms, and also because of the possibility ofmissing a tumour, it is necessary to explore allthese conditions.
Diaphragmatic Hernia ofTraumatic OriginThe diaphragm may be torn by compression
effects of crush injuries, or by stab or gunshotwounds.
Case No. 6. Traumatic Rupture of the Diaphragmdue to a Car Accident
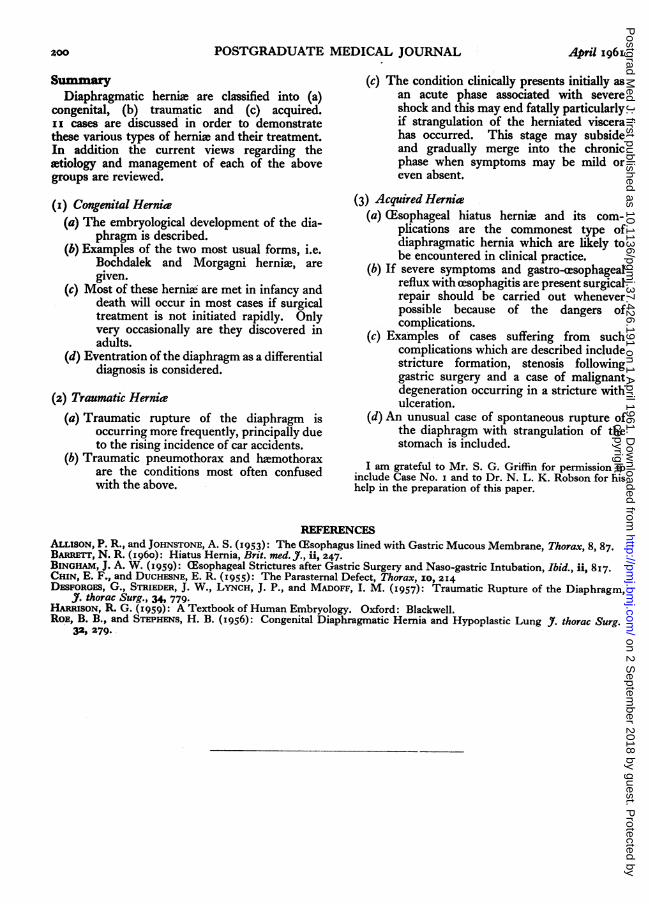
This 48-year-old man was admitted to a generalsurgical ward following a road accident. In the crashhe was thrown forward injuring the left side of hischest and abdomen on the steering wheel. On ad-mission he was slightly shocked and complained ofsevere pain in the left chest and abdomen. His abdomenwas tender with rigidity below the left costal margin. Adiagnosis of ruptured spleen was made and a laparotomycarried out. The spleen was, however, found to beuninjured, but the stomach was found to be protrudinginto the chest. The condition at the time was thoughtto be a congenital diaphragmatic hernia, and no furtheraction was taken. He was discharged home still com-plaining of dyspncea on exertion. A month later he wasreferred to the Thoracic Unit and his X-ray (Fig. I2)showed the left chest occupied by a large air space,absent lung markings, and the heart and mediastinumdisplaced to the right. At thoracotomy a grosslydistended stomach and the spleen were found to occupymost of his left chest. The herniated viscera werereduced, and a transverse tear in the diaphragm, about6 inches long, was repaired. His convalescence wasuneventful, and X-ray of his chest a fortnight laterwas satisfactory.
The diaphragm may be ruptured by trauma atany point. The left diaphragm is more frequentlyinjured than the right, because the right has theprotection of the liver. Traumatic herniae haveno hernial sac, and properly speaking this con-stitutes an evisceration of the abdominal contentsinto the thorax. The most common cause ofdiaphragmatic rupture is some severe form ofimpact such as occurs in automobile accidents.When the disruptive force is applied to the chestwall or upper abdomen, the diaphragm, being astructure of relative weakness, tears.
If following an accident, the victim is shocked,dyspn(ric and cyanosed, the possibility of rup-tured diaphragm should be borne in mind, andX-ray examination carried out. A pneumothoraxis the most likely condition to be considered as adifferential diagnosis. This may be ruled out bypassing a gastric tube, or getting the patient todrink some barium and observing it on an X-rayscreen. There is also an obvious irregularity orabsence of diaphragmatic continuity. The clinicalpicture of diaphragmatic rupture can be dividedinto an acute phase and a chronic phase. In thechronic phase the symptoms may be mild, orabsent. Once the diagnosis has been established,surgical repair should be carried out, and theresults are usually satisfactory.
Acquired Diaphragmatic HerniaThis group of cases deals with cesophageal
hiatus hernia, and its complications, and includesa case of spontaneous rupture of the diaphragm.
Case No. 7. (Esophageal Hiatus HerniaThis 59-year-old lady was admitted with a history
Aphril I96I 197copyright.
on 2 Septem
ber 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.426.191 on 1 A
pril 1961. Dow
nloaded from
POSTGRADUATE MEDICAL JOURNAL
of dysphagia of three years' duration. She complainedof heartburn and stated that food appeared to stickbehind the sternum. Regurgitation, which was fre-quently accompanied by vomiting, occurred when shewas stooping to do her gardening, and when she waslying in bed. The latter was well-controlled by sleepingupright.Barium meal (Fig. 13) showed an (esophageal hiatus
hernia involving the cardia of the stomach, and screen-ing showed a good deal of gastro-esophageal reflux.It was decided to treat the condition surgically. Atthoracotomy the hernial sac was cut away, the herniatedportion of the stomach reduced, the muscle bundles ofthe right crus approximated, and the acute gastro-esophageal angle restored. Her convalescence was com-plicated by persistent diarrhcea from colonic diverti-culitis which responded satisfactorily to hydrocortisoneenemas and oral prednisolone. She eventually made agood recovery, and a barium meal showed a satisfactoryrepair. Screening showed no evidence of regurgitation.
Herniax through the inguinal canal have beenwell-understood for over a century, hernixe throughthe cesophageal hiatus, on the other hand, havereceived attention only recently. Under normalconditions the stomach cannot be displaced intothe mediastinum because of the obliquity of thegastro-cesophageal junction, and the effectivesphincteric action of the crural muscles whichsurround the hiatus. The hiatal orifice is vulner-able, and can be disrupted by the prolongedaction of increased intra-abdominal pressure suchas occurs e.g. in pregnancy, obesity, flatulentdyspepsia or by the wearing of constrictingcorsets. Once a hiatus hernia develops, most ofthe symptoms and complications are due to thereflux of gastric juice into the cesophagus. Thismay lead to acute inflammation and ulceration ofthe (esophageal mucosa, and eventually to strictureformation.The symptoms in the above case were fairly
typical of the condition. Besides pain, regurgit-ation and vomiting, severe anamia and hemate-mesis may occur. Anginal attacks, cholecystitisand peptic ulcer are conditions most likely to beconfused with hiatus hernia. In the absence ofsymptoms conservative treatment may be justified,but the complications, especially stricture forma-tion, are so difficult to manage, that in the presenceof symptoms, early surgical repair should beadvised.
Case No. 8. Ulceration and Stricture of the(Esophagus due to Hiatus Hernia
This 56-year-old man was referred with a recenthistory of increasing dysphagia and retrosternal pain.Three years prior to this he had suffered from epigastricpain, nausea and vomiting for several months. On ad-mission, barium meal showed a hiatus hernia, with anulcer crater and marked stenosis. At cesophagoscopy astricture was seen at the 29 cm. mark, with severecesophagitis above. At thoracotomy the cesophagus wasfound to be shortened, its walls thickened, and thegastro-cesophageal junction embedded in a mass offibrous tissue. It was possible to dissect the lower end
of the (esophagus, reduce the hernia, and repair thedefect. A post-operative barium meal showed a satis-factory repair, and no evidence of ulceration or stenosis.He has remained symptom -free since.
Apart from the intact mucous membrane of thestomach and first part of the duodenum, the humantissues are readily inflamed by gastric secretions.An example is gastro-jejunostomy, which in thepresence of high gastric acidity, often results instomal ulceration. If the sphincter mechanism atthe cardia, especially during sleep in the re-cumbent position, is deficient, acid pepsin mayeasily flow back into the cesophagus and causecesophagitis, ulceration and eventually fibrosiswith stricture formation. Although hiatal herni-ation is the cause of the condition, all patientswith hiatal deficiency do not develop cesophagitisand its sequelx, just as all patients who haveundergone gastro-enterostomy do not necessarilydevelop stomal ulceration.The above patient had a fairly typical history.
He first complained of upper abdominal dyspepsiaof a few months' duration, suggestive of chole-cystitis or peptic ulceration. This was followedby a silent period which gradually gave way toincreasing dysphagia.
Other symptoms of peptic ulceration of thecesophagus are heartburn, regurgitation, vomitingand retrosternal pain. Surgical management ofthese cases is very difficult. If after preliminarydilatations of the stricture it is possible to dissectthe (esophagus, reduce and repair the hernia, theresults are satisfactory. Such was the case in ourpatient, but frequently the hernia is irreducible.In these cases the methods of choice are excisionof the stricture with either cesophago-jejunostomy,or the interposition of a loop of jejunum or colon.These operations are unfortunately not free fromcomplicating side-effects.
Case No. 9. (Esophageal Stricture due to HiatusHerniafollowing Gastro-enterostomy
This man of 70 years of age had an operation for aperforated peptic ulcer I 5 years ago. Recently hissymptoms became very troublesome and a gastro-enterostomy was carried out. A few days after his dis-charge from hospital, he noticed some difficulty inswallowing, which gradually got worse, until eventuallyhe could swallow only fluids. Barium meal (Fig. I4)showed a hiatus hernia with a severe stricture at thegastro-aesophageal junction. As it was not possible todilate the stricture, it was decided to explore him. Atthoracotomy the lower end of the (esophagus wasmobilized, its wall incised, and a pin-point stricturefound at the gastro-cesophageal junction. A cardioplastywas carried out. This procedure involves incising thestricture longitudinally and re-suturing the cut edgeshorizontally. Bilateral vagotomy was also done toreduce the amount of gastric secretions. His post-operative course was satisfactory, and he remainedsymptom-free. A recent barium meal showed noevidence of stricture, but screening demonstrated free
I98 -April I96 Icopyright.
on 2 Septem
ber 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.426.191 on 1 A
pril 1961. Dow
nloaded from
HOFFMAN: Diaphragmatic Hernia
gastro-cesophageal reflux. This operation does notrestore the normal gastro-cesophageal anatomy, andhence would be unsuitable for a younger person.The occasional development of an cesophageal
stricture following partial gastrectomy or gastro-enterostomy has been recognized for many years,particularly so if an in-dwelling gastric tube hasbeen left in situ for some time. Less often thecondition has followed gastric intubation whichhas been carried out for other surgical or medicalconditions. CEsophagoscopic findings in suchcases usually showed appearances similar to thosefound in reflux cesophagitis, and barium mealoften demonstrated the presence of a hiatushernia.
Reflux cesophagitis in the presence of a hiatushernia occurs more readily in the recumbentposition, and is probably aggravated by thepresence of an in-dwelling gastric tube. Thesecomplications might be prevented if patients, evenif the presence of a hiatus hernia is not suspected,be nursed in an upright position followingabdominal operations, especially if a gastric tubehas to be left in situ.
Case No. 1O. Carcinoma complicating a case ofHiatus Hernia
This 68-year-old female was admitted for investi-gation with a history of intermittent episodes of dys-phagia going back for two years. Barium meal (Fig. 15)showed a hiatus hernia, and a moderately severecesophageal stenosis. On screening there was markedgastro-cesophageal reflux. At cesophagoscopy an ulcerwas seen and routine biopsy was taken. Histologicalexamination showed this to be an adeno-carcinomaarising in gastric mucosa. She was explored througha left thoraco-abdominal incision and resection of thelower third of the cesophagus, and the upper portion ofthe stomach was carried out, and continuity restored bygastro-cesophageal anastomosis. Macroscopically thelesion in the resected specimen looked like a chroniculcer. Histology showed the presence of a chronicgastric ulcer which showed malignant change of anadeno-carcinoma at the periphery. Her post-operativerecovery was uneventful, and a barium meal wassatisfactory.There are two varieties of ulceration which
may occur in the presence of a hiatus hernia: (i)peptic cesophagitis involving the squamous epi-thelium of the cesophagus which is secondary toregurgitation of gastric juices. Peptic ulcerationand a fibrous stricture may subsequently develop.The ulcers tend to remain superficial, may oozeblood, but rarely cause severe himorrhage, anddo not perforate. (2) If ulceration occurs in gastricmucous membrane, the ulcers arising from thisbehave like gastric ulcers, in that they may heal,bleed, perforate or cause stenosis. They differfrom peptic ulcers of the cesophagus in that theymay respond to medical treatment. Carcinomaarising from a chronic gastric ulcer in a hiatus
hernia is rare, but there is no reason why suchchronic gastric ulcers should not become malignantas they do in the stomach. Our patient wasfortunate in that the symptoms of her stenosis ledto investigations which revealed the carcinoma atan early stage. The possibility of malignantchange occurrlng in association with gastro-cesophageal reflux in hiatus hernia should be kept inmind, and biopsy carried out whenever possible.
Case No. ii. Spontaneous Rupture of the Dia-phragm with Strangulation of the Stomach
This female patient of 48 years of age gave a historyof sudden pain in her chest whilst sne was dancing.She walked home and stayed in bed for a week. Duringthis time the intensity of the pain varied, and it wasat times accompanied by vomiting. She was admittedto a general medical ward, and her chest X-rays (Fig. i6)were first interpreted as being due to a tension hydro-pneumothorax. On the day following admission, shecollapsed with signs of profound shock. Offensivefluid was aspirated from the chest, which was found tohave an acid reaction. This temporarily relieved hercondition, and at this stage the diagnosis of intra-thoracic stomach was made. A further X-ray (Fig. 17)showed two fluid levels-one in the stomach, and the otherin the pleural cavity. She was transferred to theThoracic Unit, where a thoracotomy was carried out.The stomach, which was greatly dilated, was found tooccupy most of the left pleural cavity, and was congested,cedematous and purple. The spleen, part of the trans-verse colon and omentum were also found in the chest.There was no hernial sac present. After reducing theherniated viscera into the abdomen, a tear about 4 to 5inches long was seen in the posterolateral part of thediaphragm, which was repaired. She made a goodrecovery, and her chest X-ray showed her left lung to beexpanded.
Whereas strangulation is a common compli-cation of most herniae, it is rare in the dia-phragmatic variety. Most of the recorded casesof strangulation have occurred either in alreadyexisting diaphragmatic hernia or following trau-matic rupture of the diaphragm. A suddenincrease of intra-abdominal pressure such asoccurs in vomiting, physical exertion, over-eatingor post-operative distension, are thought to be thecausative factors of a diaphragmatic hernia pro-ceeding to strangulation. In our case, however,there was no previous history of a hernia, and nohernial sac was found. In addition to this therewas no history of injury. The effort which causedthis rupture to occur was trivial, and it maytherefore well be classified as a spontaneousrupture of the diaphragm.
Signs of strangulation of a diaphragmatichernia are a sudden onset of severe pain, vomitingand respiratory embarrassment. Late symptomsinclude profound shock, cyanosis and dehydration.These late symptoms should be forestalled by earlyoperation, as once they have occurred, mortalityis high.
April I 96 I 199
copyright. on 2 S
eptember 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.426.191 on 1 April 1961. D
ownloaded from
200 POSTGRADUATE MEDICAL JOURNAL April I96I
SummaryDiaphragmatic hernie are classified into (a)
congenital, (b) traumatic and (c) acquired.ii cases are discussed in order to demonstratethese various types of hernia and their treatment.In addition the current views regarding theetiology and management of each of the abovegroups are reviewed.
(I) Congenital Herniae(a) The embryological development of the dia-
phragm is described.(b) Examples of the two most usual forms, i.e.
Bochdalek and Morgagni hernia, aregiven.
(c) Most of these hernia are met in infancy anddeath will occur in most cases if surgicaltreatment is not initiated rapidly. Onlyvery occasionally are they discovered inadults.
(d) Eventration of the diaphragm as a differentialdiagnosis is considered.
(z) Traumatic Hernia(a) Traumatic rupture of the diaphragm is
occurring more frequently, principally dueto the rising incidence of car accidents.
(b) Traumatic pneumothorax and hlmothoraxare the conditions most often confusedwith the above.
(c) The condition clinically presents initially asan acute phase associated with severeshock and this may end fatally particularlyif strangulation of the herniated viscerahas occurred. This stage may subsideand gradually merge into the chronicphase when symptoms may be mild oreven absent.
(3) Acquired Herniae(a) (Esophageal hiatus hernke and its com-
plications are the commonest type ofdiaphragmatic hernia which are likely tobe encountered in clinical practice.
(b) If severe symptoms and gastro-cesophagealreflux with cesophagitis are present surgicalrepair should be carried out wheneverpossible because of the dangers ofcomplications.
(c) Examples of cases suffering from suchcomplications which are described includestricture formation, stenosis followinggastric surgery and a case of malignantdegeneration occurring in a stricture withulceration.
(d) An unusual case of spontaneous rupture ofthe diaphragm with strangulation of thestomach is included.
I am grateful to Mr. S. G. Griffin for permission toinclude Case No. i and to Dr. N. L. K. Robson for hishelp in the preparation of this paper.
REFERENCESALLIsON, P. R., and JOHNSTONE, A. S. (1953): The C1Esophagus lined with Gastric Mucous Membrane, Thorax, 8, 87.BARRErT, N. R. (I960): Hiatus Hemia, Brit. med. _., aU, 247.BINGHAM, J. A. W. (1959): CEsophageal Strictures after Gastric Surgery and Naso-gastric Intubation, Ibid., ii, 817.CHIN, E. F., and DUCHESNE, E. R. (1955): The Parastemal Defect, Thorax, IO, 214DESFORGES, G., STRIEDER, J. W., LYNCH, J. P., and MADOFF, I. M. (1957): Traumatic Rupture of the Diaphragm,
J. thorac Surg., 34, 779.HARRISON, R. G. (1959): A Textbook of Human Embryology. Oxford: Blackwell.ROE, B. B., and STEPHENS, H. B. (1956): Congenital Diaphragmatic Hernia and Hypoplastic Lung J3. thorac Surg.
32, 279.
copyright. on 2 S
eptember 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.426.191 on 1 April 1961. D
ownloaded from