diatribe news final8 1 - nov_dec 2006.pdf · diatribe • research and product news for people with...
TRANSCRIPT
““
from the editor
SO HERE IT IS! The very first issue of diaTribe, and we hope it’s just the beginning. Here at Close Concerns, we are passionate about diabetes – understanding it, writing about it, not to mention managing it. (Many of us have it, some since we were children.)
As a patient-focused newsletter, diaTribe represents a new chapter for Close Concerns. Some readers may already know that we have an industry
newsletter called “Diabetes Close Up” (DCU), which covers new research, conferences, and product launches. We travel all over the world for the timeliest information, we have access to America’s leading diabetes’ researchers and clinicians, and we’ve developed unmatched expertise in the business of this disease. But until now, none of these efforts benefited the people who needed them most: the patients! With diaTribe, we intend to change that.
Our mission is to leverage our knowledge to give our readers the information they need. Unlike other newsletters, diaTribe is not just straight reporting, and it is not for everyone. As the name suggests, we are going to have an opinion. We might rant, we might rave, we might lament or celebrate, but we will always inform and enlighten. And we hope to reach that exquisite tribe of readers who are smart about diabetes, who believe in intensive management, and who are eager to learn more – for themselves, perhaps, or a loved one.
Diabetes is a large and complicated field – from multinational pharmaceutical companies to sprawling clinics, from prestigious academic centers to remote research labs. It is filled with exciting breakthroughs and heartbreaking disappointments, but ultimately it’s about patients – you and me – who want to live long, healthy lives. We believe diaTribe will help give you the information you need to live the life you want.
In every issue, we’ll bring you 1) Test Drive – our personal, no-holds-barred experience with new drugs and devices; 2) Logbook – a look at the human drama of diabetes by best-selling author James S. Hirsch; 3) Learning Curve – a closer look at the science behind the news; 4) Conference Pearls – what we consider the biggest news from major – and-under-the-radar-screen – conferences that we attend; 5) Diabetes Dialogue – excerpts of our conversations with key clinicians that we converse with regularly, who share with us lessons from their offices and labs; and 6) What We’re Reading – highlights of the top 5 percent of our monthly reading on diabetes (we review 25 magazines and journals per issue).
And because diaTribe is about you, please don’t hesitate to contact us with comments or suggestions at [email protected]. We’re all in this together, so we look forward to hearing from you.
Thank you for your time and support!
— Kelly L. Close
����������������������������������������������������������
VO L U M E 1 • I S S U E 1
From the Editor .............. 1Drumroll, please…
Test Drive ........................ 2Trying out DexCom’s continuous glucose monitor
Logbook .......................... 3Stem cells, George Bush, and a parent’s dream
Learning Curve ............... 4A closer look at incretins and Byetta
Conference Pearls .......... 6Get smart - Intelligence from your doctors’ recent diabetes meetings
Diabetes Dialogue ......... 8With educator extraordinaire Davida Kruger
What We’re Reading ...... 10Cutting through the information clutter
in this issue
We might rant, we
might rave, we might
lament or celebrate, but
we will always inform
and enlighten.
research and product news for people with diabetes
To subscribe to diaTribe, visit www.diaTribe.us.
diaTribe_NEWS_FINAL8.indd 1 11/8/06 12:14:38 PM
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
test driveTest Driving DexCom’s Short-Term Sensor (STS): A Look at Continuous Glucose Monitoring
Continuous glucose monitoring is one of the most eagerly anticipated diabetes products in recent history. So, shortly after its approval in March 2006, three of us at diaTribe ordered the DexCom Short-Term Sensor (STS). It was the first real-time continuous glucose monitor
to reach the market in a meaningful way. (Medtronic’s Guardian RT made a cameo in seven cities, but relatively few patients had access to it at the time of DexCom’s launch.)
The product is clearly valuable, specifically the trending data that allow us to catch extreme highs or lows; but we don’t see it replacing finger sticks for awhile. Inaccurate glucose values under-mine its reliability, and insurers don’t yet cover it, so its high cost makes it impractical for all but the wealthiest.
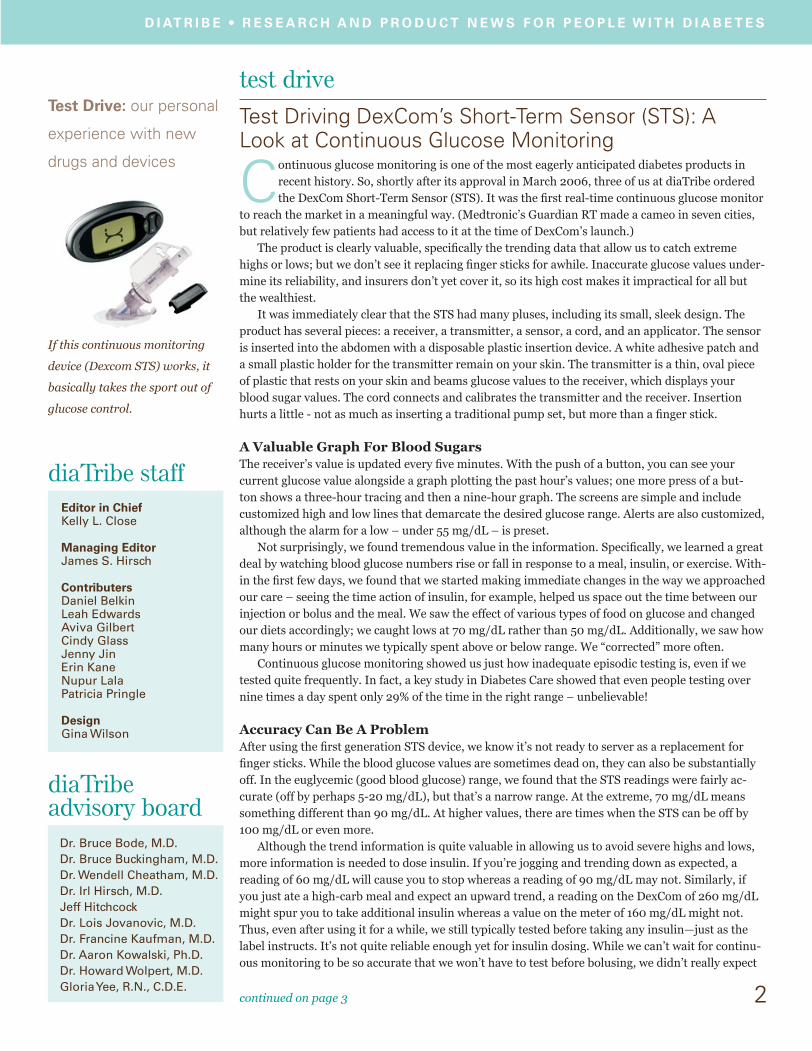
It was immediately clear that the STS had many pluses, including its small, sleek design. The product has several pieces: a receiver, a transmitter, a sensor, a cord, and an applicator. The sensor is inserted into the abdomen with a disposable plastic insertion device. A white adhesive patch and a small plastic holder for the transmitter remain on your skin. The transmitter is a thin, oval piece of plastic that rests on your skin and beams glucose values to the receiver, which displays your blood sugar values. The cord connects and calibrates the transmitter and the receiver. Insertion hurts a little - not as much as inserting a traditional pump set, but more than a finger stick.
A Valuable Graph For Blood SugarsThe receiver’s value is updated every five minutes. With the push of a button, you can see your current glucose value alongside a graph plotting the past hour’s values; one more press of a but-ton shows a three-hour tracing and then a nine-hour graph. The screens are simple and include customized high and low lines that demarcate the desired glucose range. Alerts are also customized, although the alarm for a low – under 55 mg/dL – is preset.
Not surprisingly, we found tremendous value in the information. Specifically, we learned a great deal by watching blood glucose numbers rise or fall in response to a meal, insulin, or exercise. With-in the first few days, we found that we started making immediate changes in the way we approached our care – seeing the time action of insulin, for example, helped us space out the time between our injection or bolus and the meal. We saw the effect of various types of food on glucose and changed our diets accordingly; we caught lows at 70 mg/dL rather than 50 mg/dL. Additionally, we saw how many hours or minutes we typically spent above or below range. We “corrected” more often.
Continuous glucose monitoring showed us just how inadequate episodic testing is, even if we tested quite frequently. In fact, a key study in Diabetes Care showed that even people testing over nine times a day spent only 29% of the time in the right range – unbelievable!
Accuracy Can Be A ProblemAfter using the first generation STS device, we know it’s not ready to server as a replacement for finger sticks. While the blood glucose values are sometimes dead on, they can also be substantially off. In the euglycemic (good blood glucose) range, we found that the STS readings were fairly ac-curate (off by perhaps 5-20 mg/dL), but that’s a narrow range. At the extreme, 70 mg/dL means something different than 90 mg/dL. At higher values, there are times when the STS can be off by 100 mg/dL or even more.
Although the trend information is quite valuable in allowing us to avoid severe highs and lows, more information is needed to dose insulin. If you’re jogging and trending down as expected, a reading of 60 mg/dL will cause you to stop whereas a reading of 90 mg/dL may not. Similarly, if you just ate a high-carb meal and expect an upward trend, a reading on the DexCom of 260 mg/dL might spur you to take additional insulin whereas a value on the meter of 160 mg/dL might not. Thus, even after using it for a while, we still typically tested before taking any insulin—just as the label instructs. It’s not quite reliable enough yet for insulin dosing. While we can’t wait for continu-ous monitoring to be so accurate that we won’t have to test before bolusing, we didn’t really expect
2
diaTribe staffEditor in ChiefKelly L. Close
Managing EditorJames S. Hirsch
ContributersDaniel BelkinLeah EdwardsAviva Gilbert Cindy GlassJenny JinErin KaneNupur LalaPatricia Pringle
DesignGina Wilson
continued on page 3
diaTribeadvisory board
Dr. Bruce Bode, M.D.Dr. Bruce Buckingham, M.D.Dr. Wendell Cheatham, M.D.Dr. Irl Hirsch, M.D. Jeff Hitchcock Dr. Lois Jovanovic, M.D.Dr. Francine Kaufman, M.D. Dr. Aaron Kowalski, Ph.D. Dr. Howard Wolpert, M.D. Gloria Yee, R.N., C.D.E.
Test Drive: our personal
experience with new
drugs and devices
If this continuous monitoring
device (Dexcom STS) works, it
basically takes the sport out of
glucose control.
diaTribe_NEWS_FINAL8.indd 2 11/8/06 12:14:38 PM

D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
3
it to happen on this first round. Although we hear a fair amount of complaints about accuracy, we find that accuracy isn’t really what we’re using it for. As Dr. Nancy Bohannon, an endocrinologist in San Francisco, says, “You’re using it for clinical utility – and you’re getting it!”
Even more frustrating than inaccurate numbers were no numbers at all. On at least two occa-sions, a morning fingerstick read low at 50 mg/dL even though STS had given no warning—because it had stopped reading four hours ago. Sometimes the readings would stop when glucose levels were rising or falling rapidly. If the number on the STS was very different from a meter reading (the STS works with the OneTouch Ultra only) and the two were in sync, the readings would abruptly stop. Until this device reads continuously with fewer interruptions, we wouldn’t consider it a fool-proof hypoglycemic alarm. We found several other negatives with the STS. First, a number of sensors failed to work at all. The good news is that the DexCom customer support line was very helpful. Then there is also the “high hassle factor” - wearing the STS requires carrying around the cable to connect the One Touch Ultra to the STS for calibration at least once every twelve hours, and wear-ing a shower patch since it isn’t yet waterproof.
High Cost Could Deter UseThe biggest negative, however, is the high cost of the system and the sensors. While we have insur-ance, this device isn’t covered yet. From what we know, your insurance probably won’t cover it ei-ther at this stage. The DexCom receiver and transmitter system costs $800 and each new sensor is $35. That’s over $250 per month for the sensors alone! Frankly, that makes the reliability problems even more unsettling.
But problems aside, we don’t want to give up the STS. The allure is still strong. What makes dia-betes, particularly type 1, so difficult is its unpredictability, and this product finally allows patients to better monitor the fluctuations and to respond accordingly. We are ultimately optimistic about STS as a first-generation product. We’ve had diabetes long enough to remember the first blood glu-cose monitors, with those giant blood drops, the painfully slow time, and the errors – wouldn’t you just cringe when you got those error codes!? Just as that technology got much better, this will too. In fact, Minimed has combined the pump and the monitor, and we start testing that system shortly. We’ll let you know how it goes. ■
logbookDoug Melton Ignores Threats, Political Hurdles in Hopes of Using Embryonic Stem Cells to Cure His Children
By James S. Hirsch
He’s been called the devil. He’s been told that God will send him to hell. His research has been compared to experiments conducted by the Nazis. Douglas Melton never expected such a critique when he began his career as a frog biologist, but his research – and life – took a very different turn in 1991 when his baby son, Sam, was diagnosed with diabetes. Determined to help, Melton redirected his Harvard lab toward creat-ing beta cells, but he also thrust himself into a bitter national debate about science, religion, and morality.
“It wasn’t something I expected,” Melton says. “I just wanted to find the cure.” President Bush’s veto of legislation in 2006 that would have expanded federally funded embry-
onic stem cell research has returned the issue to center stage. The legislative outcome could have a profound effect on researchers, none more than Doug Melton, who’s been hampered by restrictions imposed in 2001. But the debate could also put Melton himself back into the spotlight.
In many ways, he’s the ideal advocate. A lean figure with wire-rim glasses, graying hair, and a gentle voice, he projects middle-class decorum. That belies a fierce intellect and supreme self-con-fidence, which lead to biting criticism of his peers. (He describes experiments that show that beta cells can regenerate as “not just flawed but laughably flawed.”) But in any debate about stem cells, what gives him moral authority is not his scientific credentials but his personal motivation – a
continued on page 4
HIRSCH
““[My wife] will say, ‘You’ve
been working all this time,
and you haven’t cured the
disease.’ That’s a lot on my
mind.
““Determined to help,
Melton redirected his
Harvard lab toward
creating beta cells...
diaTribe_NEWS_FINAL8.indd 3 11/8/06 12:14:39 PM
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
4
parent’s primal urge to cure his son as well as his daughter. Ten years after his son was diagnosed, his 14-year-old daughter, Emma, also developed diabetes.
Melton is no stranger to the public square. In 1999 he testified before the U.S. Senate in support of stem cell research, noting that since Sam’s diagnosis, “I can’t recall a single night that we slept peacefully, free of worry.” After George W. Bush was inaugurated, he was summoned to the White House, where the president was mulling policy options. Melton told him that he should view stem cell research the way President Kennedy had contemplated going to the moon – as something bold and visionary that would define his presidency. “That could be your moon shot,” Melton said. “You could change the whole health care system.”
Bush, of course, ignored his advice. It didn’t matter that the actual fertilized eggs used by in-vestigators are surplus embryos from fertility clinics, which would otherwise be discarded, or that the research could benefit many diseases. The president announced on August 9, 2001, that federal funds could only be used for research on embryonic stem cell lines – or those derived from a single egg – created before that date, but not afterward.
The law itself made little sense. If a fertilized egg constitutes human life – as President Bush claims – why is it morally acceptable to destroy that “life” before August 9, 2001, but not after that date? More important, the restrictions severely limited the research, because there simply weren’t enough quality stem cell batches (about 20) that complied with the law. The regulations also forced Melton to take extraordinary steps to ensure that no federal money was spent on new cell lines that he lawfully obtained from a Boston IVF clinic. (He receives private money from the Howard Hughes Medical Institute, the JDRF, and other donors.) Melton had to create a separate lab that contained no equipment bought with government dollars, which meant the lab needed separate centrifuges, computers, even light bulbs. “It has slowed us down tremendously,” Melton says.
In 2004 Melton was named co-director of the Harvard Stem Cell Institute. The location of his cramped laboratory is kept secret for fear of protestors, and a special key card electronically checks the identity of anyone who enters. While the personal attacks are unpleasant, he actually enjoys the intellectual sparring.
Embryonic stem cells form in the embryo about four days after fertilization and can become vir-tually any cell in the body, giving them enormous curative potential. The research itself is relatively new, since human embryonic stem cells were not isolated until 1998. Melton’s goal – nurturing an insulin-producing beta cell from an undifferentiated embryonic stem cell – is nothing less than divining the mystery of life itself, but Melton argues that it’s necessary for curing diabetes.
Melton doesn’t need to understand every event that causes an embryonic cell to become a beta cell instead of, say, a bone cell or blood cell, but he needs to identify the few definitive genetic signals that produce one. That could make it possible to create beta cells for transplantation, using embryonic stem cells as a virtually unlimited source and thereby negating the supply problem that surgeons currently have with islets or pancreata.
But is such an outcome really possible? Melton says it is, but neither he nor any other stem-cell re-searcher is close; and after 15 years of work, his wife sometimes reminds him of this. “She’ll say, ‘You’ve been working all this time, and you haven’t cured the disease,’” he says. “That’s a lot on my mind.”
But so too are his children, and that’s why – regardless of personal threats or government road-blocks – he’s not about to stop. ■
— James S. Hirsch, the managing editor of diaTribe, is the author of “Cheating Destiny: Living with Diabetes, America’s Biggest Epidemic”.
learning curve Byetta Craze is First Salvo in Promising New Line of Drugs
W hat’s behind the Byetta craze?
For an industry that has often promised more than it’s delivered, Byetta is the first line of
a new class of drugs that could transform the therapeutic landscape for type 2 patients.
continued on page 5
Learning Curve:
a closer look at the
science behind the news
Look up Dr. Melton at
the Harvard Stem Cell
Institute-- www.stemcell.
harvard.edu
T2
T2This article may be of
particular interest to those
with type 2 diabetes.
diaTribe_NEWS_FINAL8.indd 4 11/8/06 12:14:39 PM

D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
5continued on page 6
Deadly Lizard Now Diabetics’ Favorite Reptile Byetta was approved by the FDA in April, 2005. In its first year on the market, more than 1 million
prescriptions were written by 50,000 doctors. Injected twice a day, Byetta helps patients maintain
normal blood sugars, but that alone wouldn’t cause a craze. After all, insulin does the same thing, even
better.
Byetta’s appeal is that it also helps people lose weight, a boon for type 2s. On chat boards, in sup-
port groups, and among friends, patients tell nearly miraculous stories of how the product caused
them to lose 20, 30, even 40 pounds.
Byetta, however, is not approved as a weight-loss drug, and it can have daunting (albeit temporary
for most) side effects, including nausea and vomiting.
The product has quirky origins: it’s derived from the saliva of the Gila monster, a deadly lizard
found in the American Southwest and now the diabetic community’s favorite reptile.
The frenzy Byetta had a spectacular launch, with more than 400,000 patients having taken Byetta as of late
2006. The biggest problem for the manufacturers – Amylin Pharmaceuticals and Eli Lilly –was, for a
short while, that they couldn’t meet demand. (They had to advise doctors for a couple of months last
summer not to write new prescriptions until they could make more cartridges.)
This frenzy was on display at the ADA’s annual meeting in June. At a Friday night symposium on
“incretin-based” therapies like Byetta, hundreds of attendees arrived an hour early at Washington’s
Grand Hyatt. Waiting outside the room, they crowded around an escalator and jostled for a place in
a line that extended down two floors and into a cocktail party. When the line finally advanced, many
were left outside. Some tried to sneak past guards at the door. Arguments ensued. One man cried.
Rock concerts have seen less excitement. So we think an explanation of Byetta is in order.
Byetta explained For starters, Byetta works for type 2 patients and can be seen as a kind of lifeline to an overworked
pancreas. Type 2 diabetes is thought to occur when the insulin-producing beta cells in the pancreas
become impaired. This breakdown often happens in overweight people whose body weight has made
them insulin resistant; their stressed-out beta cells can no longer fully compensate for their body’s
resistance to insulin. Simple aging can also impair beta cell function.
But relatively obscure “gut hormone peptides,” called incretins, play a role in maintaining normal
blood sugars. Specifically, natural incretins are secreted by the endocrine cells of the intestine after
meals. This normally enhances insulin release from the beta cells while suppressing glucagon release
from the alpha cells, which also lie in the pancreas.
One for the GIP Two incretins are crucial to improving beta cell function: glucose insulinotropic polypeptide (GIP) and
glucagon-like peptide-1 (GLP-1). GIP does not appear to be, alone, a promising treatment. But GLP-1
does affect the beta cells in diabetic patients and therefore has been the focus of research.
One problem is that GLP-1’s half-life in the blood is only one to two minutes, because it is quickly
broken down by the enzyme DPP-4. However, researchers have found two solutions: development of
GLP-1 analogs, which have a very similar structure to natural GLP-1 and provide all the same benefits
without being broken down by DPP-4, and the development of DPP-4 inhibitors, which are drugs that
prevent the enzyme from degrading natural GLP-1.
In non-diabetic individuals, glucagon is only released from the pancreas when blood sugar levels
are low, and glucagon secretion is shut off after meals by insulin and by GLP-1. In those of us with
diabetes, however, GLP-1 and insulin levels are low, which results in high glucagon levels.
This combination of hormonal signals mistakenly tells the body that it is starving when it really is
not. Thus, the liver continues to pump out glucose, even after a meal, and this is thought to be a major
cause of post-prandial (after-meal) hyperglycemia in diabetes.
Researchers also believe that when a person grows (whether during childhood or through weight
“
“Byetta had been
available for just a year;
more than 1 million
prescriptions had been
written, and the biggest
problem, at least for
a while, was that the
company couldn’t meet
demand. But now, more
than 400,000 patients
have taken Byetta, and
the drug should be
available soon in
Europe.
diaTribe_NEWS_FINAL8.indd 5 11/8/06 12:14:39 PM

D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
6continued on page 7
gain), the beta cells grow to meet that person’s increased metabolic needs. Some individuals are able
to maintain normal blood sugar even in the most extreme cases of obesity; thus, diabetes only occurs
when beta cells cannot maintain the appropriate mass. It is not known why beta cell mass diminishes,
and it is still debated whether decreased mass is due to increased apoptosis (cell death), decreased cell
replication (growth), or a mixture of both.
Regardless, GLP-1 therapy’s effect on beta cell mass could have profound implications. Research-
ers know that this treatment preserves or increases beta cell mass in rats and mice. Unfortunately, it
has been difficult to determine the effects of GLP-1 treatment on human beta cell mass, because it is
hard to measure directly how many beta cells we have without taking out some of the pancreas. Ad-
ditional research is needed to determine if this therapy could actually protect or regenerate beta cells.
Two different treatments For now, two different treatments can enhance GLP-1 function. The first is direct stimulation of GLP-1
receptors by GLP-1 analogs such as Byetta. These GLP-1 receptor agonists (molecules that activate a
receptor are called agonists) are small protein fragments. Since small proteins like insulin and GLP-1
are rapidly degraded by our digestive systems, we have to inject these drugs like insulin.
While Byetta’s injection was initially seen as a commercial deterrent, consumers have been won
over by the drug’s powerful benefits: it significantly increases insulin secretion, lowers A1c levels,
causes substantial weight loss, and may even promote beta cell growth.
The other strategy on the market to enhance GLP-1 function is the inhibition of DPP-4. Since the
DPP-4 enzyme naturally breaks down GLP-1 very quickly, DPP-4 inhibitor drugs prevent the break-
down of natural GLP-1 in the body.
Names to watch: Januvia and GalvusThe FDA recently approved the first DPP-4 inhibitor, called Januvia, and the agency is expected to
approve a second one, Galvus, later this year. DPP-4 inhibitors are taken once or twice a day. In some
ways DPP-4 inhibitors have an advantage over the injectable GLP-1 analogs because they are well-tol-
erated, oral drugs; however, they do not lower A1c levels as much as GLP-1 analogs and they lack the
weight loss benefits of GLP-1 analogs – two big benefits in our view.
Byetta and its caveats A few caveats about Byetta. You might need insulin as well, and a combination of insulin and Byetta
is not yet approved. First, if your A1c is over 8, this drug may not be enough – alone – to help you
achieve the ADA’s A1c goal of 7.0 or the AACE’s goal of 6.5 or lower. Plus, it sounds like targets maybe
going even lower – we look for a reduction in 2007!
You might need insulin first, and a combination of insulin and Byetta isn’t yet approved, although
we expect it to be in the next year or so. You can ask your healthcare team what will work best for you,
if the drug sounds intriguing.
Also, you need insurance to get it, because the product is expensive (about $7-8 a day, depending
on the dose), though most insurers are covering it (for more than 70% of patients, a normal co-pay of
$15 applies).
We’ll be watching, and we’ll report back, so please stay tuned. ■
conference pearlsThe annual American Diabetes Conference (Washington D.C., June 9-12) The Byetta LAR trial releases highly favorable results. Byetta LAR is the long-release form of Byetta that would only require weekly injections – a huge improvement, obviously, from the twice-daily insulin therapy many type 2 patients follow today. The results of the LAR trial released at ADA were very positive: 45 patients receiving 2.0 mg
“
“It is not known why beta
cell mass diminishes,
and it is still debated
whether decreased
mass is due to increased
apoptosis (cell death),
decreased cell replication
(growth), or a mixture
of both.
T2
diaTribe_NEWS_FINAL8.indd 6 11/8/06 12:14:39 PM

D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
7continued on page 8
doses of the drug for 15 weeks showed an average A1c drop of 2% and an average weight loss of 8.4 pounds, “with no evidence of plateau.” No plateau means huge therapeutic gains are possible with LAR: longer treatment may only mean more glycemic improvement and weight loss. By the end of the trial, a whopping 86% of subjects achieved a target A1c of fewer than 7%. There were no safety issues, and we hear anecdotally that “real world” patients may fare even better than patients in the trials if the Byetta experience offers any clues.
We expect Byetta LAR to be available by 2009, and we believe that about half of the patients on Byetta “classic” will convert to Byetta LAR in the first year alone.
DPP-4 inhibitors, one of which has received FDA approval, generate excitement for type 2 patients.Incretins are gut hormones that stimulate insulin secretion after meals, and DPP-4 is a natural enzyme that degrades those incretins. So researchers are trying to develop DPP-4 inhibitors that prevent this destructive process in diabetics.
The big two DPP-4 inhibitors that received the most attention at ADA were Januvia and Galvus; Januvia has since received FDA approval, and the same is expected for Galvus later this year.
Our impression is that these drugs won’t offer the same kind of weight loss as Byetta, which may be a bit of a disappointment. But they also don’t promote weight gain, which puts them a cut above traditional TZDs (Avandia and Actos) and sulfonylureas (Glucotrol and Amyryl, for example). The biggest excitement over DPP-4 inhibitors is the possibility that they may preserve or even regener-ate beta cells. Novartis’s GLORIOUS mega-trial on Galvus will shed light on this question.
For a complete discussion of the incretin craze, please see our Learning Curve column.
Continuous Glucose Monitoring (CGM) remains a focal point. In terms of excitement, CGM was second only to incretins at the conference. We expected noth-ing less. CGM is another step down the road to an artificial pancreas, and several models are now available. DexCom’s small and sleek STS (see page 2), Medtronic’s Minimed, and Abbott’s coming Navigator are the frontrunners. At the conference, new data suggested that the Navigator looks like the most accurate – but the Paradigm Real-Time 522/722 is still the only integrated device, which makes it closest to the artificial pancreas. We’ve heard about the artificial pancreas for years upon years and know you have too – we think we’re actually getting closer, especially since JDRF has added some very important funding recently.
Verdict is still out on inhaled insulin. Exubera, which finally started shipping to patients in September, got a lot of hype, but some physicians would like to see some more years of safety. Sure, Pfizer’s four-year trials indicate that side effects on lung function are too small to matter in patients without pre-existing pulmonary conditions. But, truthfully, we’d like to see a 20-year trial before we start lining up. Although physi-cians mobbed the booth, we think that, in this respect, seeing is different from believing, buying, and prescribing. In fact, besides the safety issue, just seeing the product was a little disappointing due to its cumbersome size: much larger than a dainty asthma inhaler.
Look out for a faster-acting insulin. The drug company Biodel may have developed an even faster insulin than Novolog, Humalog, and Apidra. Early data at the meeting showed that Viaject worked faster than rapid acting analogs in patients. It was only a few minutes faster, mind you, but time is money! The company is going to test this new drug in 66 centers across the United States. See www.clinicaltrials.gov for more info.
Bad lows may not damage cognitive function. Researchers have long feared that recurrent episodes of hypoglycemia can impair a patient’s cogni-tive function. But Dr. Alan Jacobson from the Joslin Diabetes Center has been following up with patients from the DCCT for an average of 18 years, and his results show that recurrent severe hy-poglycemic episodes had no effect on cognitive function in any of the domains measured: problem
For a complete discussion
on the incretin craze, see
Learning Curve, p 4.
“
“
“
“
We’ve heard about the
artificial pancreas for years
and know you have too
– we think we’re actually
getting closer.
Truthfully, we’d like to see
a 20-year trial before we
start lining up [for inhaled
insulin...
T2
T2
diaTribe_NEWS_FINAL8.indd 7 11/8/06 12:14:40 PM
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
8continued on page 9
solving, learning, immediate memory, delayed recall, spatial information processing, attention, psychomotor efficiency, and motor speed. Phew! ■ what we’re reading
W e know it’s impossible to stay current with all the news in diabetes. The immense flow
of information can be contradictory, confusing, and just plain overwhelming. Who has
time to read it all?Well, we do. It’s not just our livelihood. For those of us with diabetes, it’s our life, so we look for articles that
are smart, useful, and surprising. We pore over every possible diabetes publication and, in this column, we identify our most
important discoveries from recent patient magazines and newsletters. (When possible, we will give you the direct link to the article.) We hope this saves you time, and we’re pleased to point out to you pieces you might otherwise miss! We also follow the professional scientific journals such as Dia-betes Care, JAMA, and the New England Journal of Medicine, and we will report on one diabetes research article each issue.
Our favorite patient articles for this issue:
● “The Benefits of Tight Control: No End in Sight,” Wayne Clark, Diabetes Self-Manage-ment, May/June 2006. (The site is www.diabetesselfmanagement.com, but the article itself is not available online.) This article presciently reviews what we know about tight control—how many people with diabetes in the U.S. are getting there, and what it means for complications. Clark recounts the details of the Diabetes Control and Complications Trial (DCCT), which proved the hy-pothesis that tight glucose management reduces the risk of complications. The study also famously proved that there is no “glycemic threshold,” or “point below which a lower HbA1c does not yield additional benefit.” The follow-up study to the DCCT, the Epidemiology of Diabetes Interventions and Complications (EDIC) trial, found that even years after the DCCT, when the A1c’s of the two patient groups converged, patients from the intensive management cohort still had fewer complica-tions. A similar study, the United Kingdom Prospective Diabetes Study (UKPDS) published in 1998, found that intensive control in type 2 diabetes reduced microvascular complications by 25%.
Despite these impressive studies—which collectively followed more than 6,500 patients—data show that less than one-third of patients today are reaching glucose targets. In the article, Clark reviews some barriers to tight control, including lack of insurance coverage, the progressive nature of type 2 diabetes, and the way in which medical care is delivered. On this last point, MaineHealth in Portland, Maine, has implemented a “Chronic Care Model” that tackles diabetes using electronic registries, automated reminders and notices, and multidisciplinary treatment teams. As part of this program, nurse specialists called “Chronic Illness Care Managers” are incorporated into primary care practices to provide patients with more intensive education and motivational support. The model has been successful; the percentage of people with A1c values under 7% jumped from 41% to 49%, while the percentage of people with an A1c higher than 8% decreased from 31% to 24%.
The bottom line: Despite the poor outcomes for many diabetic patients, the Chronic Care Model used in Maine shows that enlightened, rigorous treatment can benefit many people with the disease. The challenge is how to spread these efforts to other parts of the country.
● “Special Report: How to Save Your Heart,” Hope Warshaw, Diabetic Living, Summer 2006. (You can read this online at www.diabeticlivingonline.com.) We love articles with information that you can apply to your own life. In this article, you receive guidance on how to lower your risk of cardiovascular disease, the number one cause of death in people with diabetes. As Dr. Francine Kaufman of Children’s Hospital of Los Angeles says, “When you have diabetes, your risk of a heart attack is as high as it is for a person without diabetes who’s had a heart attack.” Near “
“When you have diabetes,
your risk of a heart attack is
as high as it is for a person
without diabetes who’s
had a heart attack.
“
“This article presciently
reviews what we know
about tight control—
what it means for
complications and how
many people with diabetes
in the U.S. are (and are
not) getting there.
T2
diaTribe_NEWS_FINAL8.indd 8 11/8/06 12:14:40 PM

9
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
normal glucose levels can reduce the risk of heart attack and stroke. In addition to what might be termed obvious tips - 1) slim down; 2) eat smart; 3) get moving; and 4) take your medication - other more actionable advice from Warshaw includes testing blood lipids once a year. Other tips from Warshaw include testing blood lipids once a year, possibly taking a daily low-dose aspirin (75 to 162 mg), choosing unsaturated over saturated or trans fats, and knowing the signs of heart attack or stroke. From a patient perspective, we found her ABC Goals most compelling: A1c (under 6.5% or 7%, depending on which organization you ask), blood pressure (under 130/80 mmHg), and blood cholesterol (LDL under 100 mg/dL, HDL above 40 mg/dL for men and 50 mg/ dL for women, tri-glycerides under 150 mg/L). If you know your goals and your test results, you can be sure that your glucose and lipids are at healthy levels.
The bottom line: People with diabetes often worry more about microvascular complications, but heart disease is a real threat. With specific tips on how to live a healthier lifestyle, this article would benefit anyone, but it’s especially important for people with diabetes who are at higher risk for cardiovascular disease.
● “Learning the ABC’s of Beta Cells,” Robert S. Dinsmoor, JDRF Countdown, Spring 2006. (www.jdrf.org.) Beta cell regeneration, dedifferentiation, redifferentiation, isolation, and encapsulation: this article reviews some of the leading curative research, profiling scientists who are furiously trying to replace beta cells as a therapy for type 1 diabetes. Dinsmoor writes about projects across the world. For instance, a group in Denmark is using fluorescent protein tags in mouse models to better understand gene expression in beta cell differentiation, while researchers at Mt. Sinai are looking at how to make endoderm from embryonic stem cells. (Endoderm is the embryonic tissue layer that generates beta cells.) Researchers are now focused on learning what causes beta cells to de-velop. While we know that endoderm, a type of embryonic tissue, becomes the pancreas and the beta cell, we do not understand how this happens. Understanding the signaling that transforms general-ized tissue into beta cells may help researchers create new beta cells for people with diabetes.
The bottom line: Although curative research seems at times to be agonizingly slow, progress is being made. Researchers now understand considerably more about the genetics of beta cell dif-ferentiation. That said, even when researchers understand how beta cells are created, more work needs to be done before we can engineer cells to replace beta cells. As Dinsmoor writes, “Real beta cells must be able to synthesize insulin, store it, and secrete it in a glucose-responsive manner.” That’s a tall order.
Diabetes Research Update In April 2006, Dr. Louis Monnier and colleagues published an article in JAMA that challenged the conventional wisdom about diabetes management and complications. The article suggests that complications can occur not only because of high blood glucose but also because of fluctuations in glucose.
Microvascular complications (like eye, kidney, and nerve problems) and macrovascular com-plications (like atherosclerosis and cardiovascular disease) have been linked to oxidative stress, a damaging cellular process. In the study, investigators compared the effects of chronic sustained hyperglycemia and acute glucose fluctuations on the activation of oxidative stress. Twenty-one sub-jects with type 2 diabetes were enrolled in the study along with 21 “controls,” or people without dia-betes. All subjects wore a continuous glucose monitor, the Minimed CGMS system, to measure their glucose levels over three consecutive days. As a gauge of oxidative stress, researchers measured the subjects’ urine excretion of 8-iso-prostaglandin (8-iso-PGF2a), a marker of free radical production.
The study compared the data collected on the mean urinary excretion rate of 8-iso-PGF2a to the standard measurements of glycemic control. The strongest positive correlation was found between the mean urinary excretion of 8-iso-PGF2 and MAGE, or Mean Amplitude of Glucose Excursion. MAGE is an average of the differences between consecutive peaks and valleys in a glucose trend (e.g., a measure of how much glucose levels are fluctuating).
Levels of free radical production were twice as high in subjects with diabetes than in the control group, and glucose fluctuation was strongly correlated with high free radical production. Su-per-
continued on page 10
““Although curative research
seems at times to be
agonizingly slow, progress
is being made.
T2
diaTribe_NEWS_FINAL8.indd 9 11/8/06 12:14:40 PM

oxide production also correlated strongly with postprandial instability. The authors concluded that “glucose fluctuations during postprandial periods and, more generally, during glucose swings exhibited a more specific triggering effect on oxidative stress than chronic sustained hyperglycemia” (1681).
The same issue of JAMA published an editorial about the findings. Drs. Michael Brownlee and Irl B. Hirsch, who are well known for their expertise in glycemic variability, wrote: “If confirmed in larger studies, [these findings] have enormous clinical implications.” Previous work has suggested that excursions are damaging, even in patients with low glucose levels overall. Dr. Brownlee saw the impact of MAGE in his currently unpublished research on the activity of the endothelial cell enzyme, prostacyclin synthase, which inhibits atherosclerosis. When patients experienced induced hyperglycemic excursions with special hyperglycemic clamps, they saw a dramatic free-radical in-duced decrease in prostacyclin synthase. Both authors view the work of Monnier as further confir-mation that patients with type 2 diabetes should be more strongly encouraged to test frequently.
The bottom line: Dr. Monnier’s work challenges the standards of treatment, adopted since the DCCT, that have made A1c scores the gold standard of care. The focus on A1c may be too narrow, downplaying the possible damage caused by glucose excursions. We believe that devices like con-tinuous glucose monitors and drugs like Byetta and Symlin can diminish glycemic instability and can minimize excursions. They could play a much larger role in diabetes care if and when this latest research gains more adherents. If nothing else, this research reinforces the imperative of intensive management. ■
(Monnier D. et al. “Activation of Oxidative Stress by Acute Glucose Fluctuations Compared With Sustained Chronic Hyperglycemia in Patients With Type 2 Diabetes.” JAMA April 2006. 295 (14): 1681-1687. Saudek, Christopher, et al. “Assessing Glycemia in Diabetes Using Self-monitor-ing Blood Glucose and Hemoglobin A1c.” JAMA. 12 Apr 2006. 295(14):1688-1697.)
diabetes dialogueDavida Kruger
Davida Kruger, a certified nurse practitioner in diabetes, works in the Henry Ford Health System in Detroit. She spoke to us recently about the imperative of education, about patients’ enthusiastic response to new drugs, and about the chal-lenge of adherence.
diaTribe: Let’s start off with something basic! What do you recommend for type 1 and type 2 patients to achieve their blood glucose goals?
Kruger: It is very individualized, but we do say to the patients, “Look. We know if your fasting blood sugar is over 126 on a regular basis, you’re setting yourself up for retinopathy and other com-plications.” But if we can safely keep their blood glucose levels between 80 and 120, we’d love to do that.
diaTribe: Actually it seems like you emphasize the cause and effect more than other people. You make it very tangible to patients. Is that deliberate?
Kruger: Absolutely. Because the thing is, I don’t go home with them at night. What I can do is offer them information, but ultimately the patient is her own expert on her own diabetes. So I may say to you, “I really think you need to get your fasting blood sugars under 100.” But I put it in terms of best practices, because this is what we know.
I try to take the research and put it into layman’s terms. It’s not that I want you to be on a statin just because I said you should be on a statin, but let me tell you why I think you should be on a statin even if your LDL is good. Here’s how it will affect what’s happening in your heart. If there’s a blockage, I’m not going to know about it until you have chest pain. If I give you a statin, I might prevent that blockage from happening in the first place. Your greatest risk with diabetes is heart
10
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
continued on page 11
“
“[Michael Brownlee and
Irl B. Hirsch] saw the work
of Monnier as further
confirmation that patients
with type 2 diabetes
should be more strongly
encouraged to test
frequently.
“
“I don’t go home with
[patients] at night.
What I can do is offer
them information, but
ultimately the patient
is her own expert
on diabetes.
diaTribe_NEWS_FINAL8.indd 10 11/8/06 12:14:43 PM

D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
11continued on page 12
disease. How am I going to protect you from that greatest risk? What can you do with nutrition? What can you do with physical activity?
Instead of saying, “You will do it because I tell you to do it,” you get them to buy into it. It has to be their decision if they want to do it.
diaTribe: But why are some patients reluctant?
Kruger: The workload from diabetes is phenomenal. If patients can’t do it for a month at a time, you can’t beat them up over it or make them scared -- or say, “Oh, my God, you’re going to die.” It’s just, “Let’s get you back on the bandwagon. What happened so we can learn from the last month?”
I’m on the road right now, and I know I’ve gained weight not because of what I’m eating, but because I can’t exercise. There’s no time in my day. I’d be exercising right now if I weren’t talking to you. Seriously. I was on a four and a half hour flight yesterday. I’m going to be on a four and a half hour flight tomorrow. I’ve got meetings today and phone calls tonight. Where do I put exercise in my schedule? And I know that at 52 years old, if I don’t exercise, I get fat. The reality is some months I’m going to be fatter than other months.
diaTribe: Education is important for every disease, but what makes diabetes different?
Kruger: The reality is that educated patients have better outcomes, but it’s more than just A1c’s. It’s how do they control their life with diabetes. Education allows you to make better decisions.When you look at nutrition and think about how patients eat fast food all the time, they have no clue what they’re putting in their body. They may know it’s not great for them, but do they know how many calories are in a Big Mac? They might know if someone educated them. We’re all over these parents for obese kids, but has anybody ever said to them, “Do you know what you’re feeding your kids? Do you know what’s in it?” How many parents read the labels? If you had those kinds of classes for people on a regular basis and access to this kind of information, would people make bet-ter decisions? I think they would.
diaTribe: Where do most patients learn about diabetes?
Kruger: Ninety-nine percent of the information patients get is from each other. They’re out there blogging every day. That’s where they’re getting most of their information. They’re also very savvy about good Web sites, and I send them to good ones all the time.
diaTribe: Let’s talk about new products starting with technology. Are a lot of people coming in and asking about continuous monitoring?
Kruger: “When is it ready? When is it ready?”
diaTribe: Really?
Kruger: Really.
diaTribe: We’re disappointed that our insurance doesn’t pay for it yet.
Kruger: Oh, you’re not alone. A lot of patients could afford the meter but not the durables. That’s what we’re running into. They’ll put out for the meter, but if they don’t have insurance, they can’t afford the durables on a regular basis.
diaTribe: What else are you hearing from patients who are using some of these new drugs and devices?
Kruger: On Symlin, it’s the first time in their life they’ve ever been able to follow a meal plan be- cause they’re not hungry. (Editor’s note: Test Drive in diaTribe #2 will focus on Symlin.) So now we have to go back and provide an opportunity for patients to really learn the nutrition plan; whether it be Weight Watchers or ADA approved, whatever. It’s the first time that they’ve had control of their food intake, so let’s go back and provide the support and education in medical nutrition. Patients are thrilled with how flat their blood glucoses are after meals as well.
“
“On Symlin, it’s the first
time in their life they’ve
ever been able to follow
a meal plan because
they’re not hungry.
Patients are thrilled
with how flat their
blood glucoses are
after meals as well.
diaTribe_NEWS_FINAL8.indd 11 11/8/06 12:14:44 PM

D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
diaTribe: We’ve heard that the outcomes in the field are actually better than they were in the clini-cal trials. Kruger: Yes, I would say that too. The outcome in the field is a hundred percent better.
diaTribe: Wow – why do you think that is?
Kruger: I’m constantly saying that we finally have a chance to take these drugs out for a real test drive, because when you have to hold to the letter of a protocol in a clinical trial, you can’t be your own clinician. You can be a safety guru to make sure that the patient is safe, and you can also make sure the protocol is followed to the letter, but you can’t individualize treatment. Now I get to sit in front of the individual patient and see how Symlin or Byetta best fits into their life. And I’ll tell you, the A1c lowering and the weight loss with both of these drugs are so much more dramatic than we ever saw in the clinical trials.
diaTribe: So what are you seeing? Are you actually seeing A1c drops of more than a point or so, from a lowish baseline?
Kruger: Yes. Yes. Yes. In fact, what I’m seeing is so dramatic, and I know I’m not the only one, that I keep trying to send these case studies to Amylin saying these are better than what you’re using for your training. And they keep saying, “We can’t use them because we have to stay within the guide-lines.” So, yes, I am seeing dramatic weight loss, and I am seeing dramatic lowering of A1cs way beyond what the FDA approval was based on.
diaTribe: Can you talk about how patients feel about the drugs now that they’ve been out for a year?
Kruger: Oh yes. You know, there are always naysayers in the world, but I’ll tell you that my patients do not turn away from three extra injections a day if they get the benefit of Symlin. And people with type 2 diabetes who are not on injections do not mind taking the two injections if they get to use Byetta. It’s a different thought process with Symlin. I am not minimizing the fact that there’s a whole psychology to taking injections. But we can lay out benefits to a patient—their A1c will be lower, their blood glucoses will be better, and they probably will lose weight and feel better. I do not hang my hat on the weight loss part because some patients aren’t going to lose weight, and I don’t want them to get discouraged from the improvement of the A1c because for them that’s still a major benefit, and that’s not a reason not to use a drug. But I’ll tell you, I don’t have patients that turn away from using Symlin or Byetta because those drugs are injectables. I just don’t.
diaTribe: Why do you think adherence is such a problem?
Kruger: Well, I think what you have to remember is that life is really ... busy. I think if you look at any of us – I have hypertension, I have elevated lipids, and I have all of these other issues that I am personally dealing with. I understand what the ramifications are if I don’t take care of them. Do I al-ways eat well? And when I’m on the road, how do I compensate for all of that and how do I manage to get all of that done and still live my life? Then you think about people who have all those diseases I just mentioned, and they have diabetes on top 0f that. That’s typical. And I’m saying to them, “I want you to exercise. I want you to follow a diet. I want you to take six blood glucoses a day. I want you to wear an insulin pump. I want you to take Symlin and I want you to call me every three days.” So, tell me, would you have time to have a life? So is the issue adherence, or is it life? ■
Why not subscribe to diaTribe? Then you can
receive the latest information from the cutting edge
of diabetes research and product innovation. For
more information, visit www.diatribe.us����������������������������������������������������������
“
“So I’m saying to you, I
want you to exercise.
I want you to follow a
diet. I want you to take
six blood glucoses a
day. I want you to wear
an insulin pump. I want
you to take Symlin and
I want you to call me
every three days. So, tell
me, would you have time
to have a life? So is the
issue adherence, or is
it life?
diaTribe publishes information about diabetes products and research. This information is not a substitute for medical advice and should not be used to change treatment or therapy. diaTribe urges readers to consult with professional care providers in all matters relating to their health.
diaTribe_NEWS_FINAL8.indd 12 11/8/06 12:14:44 PM