dies ist der titel der präsentation - mucosal immunology€¦ · 29 january 2015 prof. harry...
TRANSCRIPT

Gastroenterologie, Inselspital
29 January 2015 Prof. Harry Sokol, Paris
IBD Masterclass
Moderator: Pascal Juillerat, MD, MSc.
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 2
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Case 1
• Dr. med. A. Kugener

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 3
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
SM, female, 40yo • Fistulizing ileocolic Crohn's disease, montréal L3 B3 + P
03/2013: perforated appendicitis with suspicion of ileitis
Personal history
– Smoking
– Overweight BMI 27.5
– 2 sectio caesarea
• Family history: uneventful

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 4
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Past history / Crohn‘s disease diagnosis
• 02/2014 colonoscopy:
– ileal involvement, stenosis C. descendens & ileocaecal valve
– fistula: prox. anal canal, C.ascendens & ileocaecal valve
• MRI 02/2014: normal, no fistulas
• MRI 04/2014: wall thickening C.descendens & sigma
• Medication: Imurek 150mg/d, prednison (max. 50mg/d)

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 5
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Complications
• Iron deficiency anemia
• Vitamin B12-deficiency
• CT-scan 09/2014: jejunocolic fistula C. descendens & paracolic
abscess
Referred by GI-collegue from external hospital due to
complicated course 11/2014

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 6
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
CT scan 09/2014

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 7
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
1st presentation outpatient clinic, Inselspital Berne
• Stool frequency 2x/d, no mucus, no blood
• Weight loss 5kg and inappetence since second flare 09/2014
• Physical exam: leftsided flank pain, no fever or rash
• CRP 70->100mg/l under iv-antibiotics (ciprofloxacine &
metronidazole)
• CT-scan 04.11.2014: progredient paracolic abscess &
jejunocolic fistula

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 8
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
CT-scan 04.11.2014:
• progredient paracolic abscess & jejunocolic fistula
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 9
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
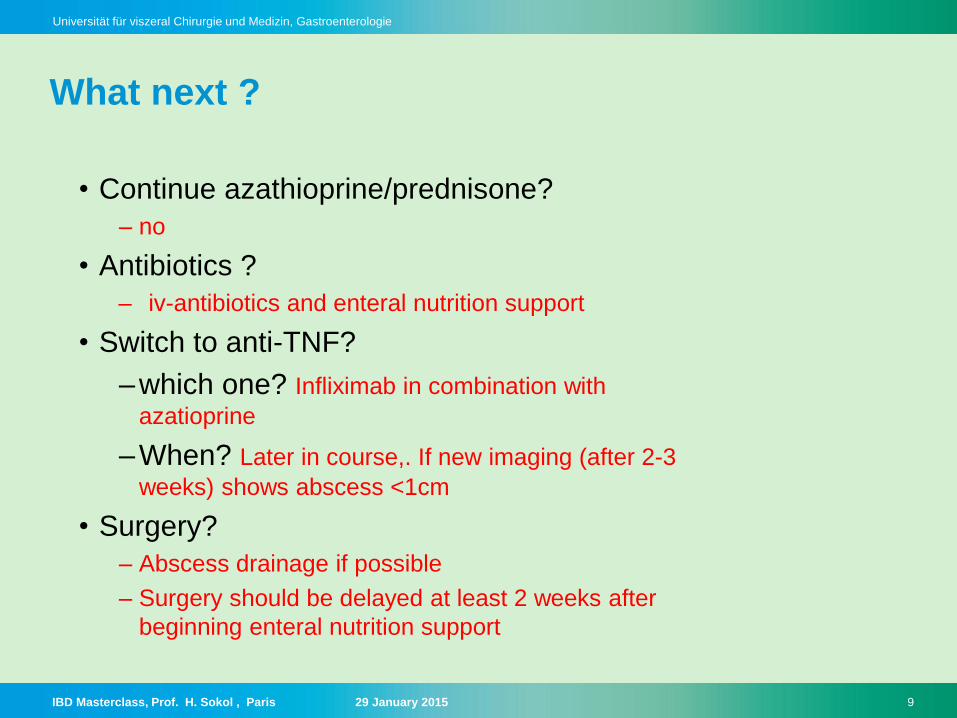
What next ?
• Continue azathioprine/prednisone?
– no
• Antibiotics ?
– iv-antibiotics and enteral nutrition support
• Switch to anti-TNF?
–which one? Infliximab in combination with
azatioprine
–When? Later in course,. If new imaging (after 2-3
weeks) shows abscess <1cm
• Surgery?
– Abscess drainage if possible
– Surgery should be delayed at least 2 weeks after
beginning enteral nutrition support

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 10
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
1st surgery and clincal course
• median laparotomie :
– with sigmaresection (10cm)
– small bowel resection (40cm distal Treitz)
– ileocaecal resection (30cm terminal ileum)
• Postoperative course without signs of abdominal pain, fever,
nausea or vomiting. But 4 kg weight loss
• Persistent elevated CRP ~170mg/l
• Sonography 2 weeks later due to suspicion of abdominal abscess

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 11
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
CT-scan 2.12.2014: • abdominal wall abscess, left lower
quadrant, paracolic
Percutaneous drainage & Tazobac
Microbiology: E.coli, S.milleri
• Metronidazole & ciprofloxacine -> switch
to Ceftriaxon & metronidazol (resistance)

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 12
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Colonoscopy 4.2.2014 • fistula of distal anastomosis,
• inflammation prox. Colon & ulceration,
• pseudopolyps

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 13
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
What to do next ?
• Conservative management? (ATB, drainage)
– No, surgical-related problem. End-to-end anastomosis in severe colitis
(1st surgery) not recommended due to high postoperative complicaton
rate -> revision of anastomosis & ileoprotectice stoma
• Start Immunosuppression with anti-TNFs / restart Imurek?
– No, no hint for Crohn relapse. Surgical problems not resolved
• Fistula resection?
– yes
• Protective ileostoma?
– yes

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 14
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
2nd surgery
• 09.12.2014: DIVERSION (Split-Stoma)
• Resection of ileotransversostomie, split-ileotransversostomie
• Sepsis after 5d, stool in wound drainage (anastomotic insufficiency?)
-> surgery: peritonitis and small bowel perforation
– Small bowel resection (10cm)
– Ileostomie & transversostomie
– VAC
• Tazobac

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 15
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Complicated course & 3rd surgery
• Pleural effusion, new fluid collection left upper abdomen
• Punction: E.feacium, candida
• Tazobac stop-> ceftriaxon, metronidazol, vancomycin, diflucan
• No percutaneous drainage possible
-> Revision laparotomy:
– abscess drainage
– peritonitis and small bowel perforation 10cm prox ileostomie
• Starting Entocort 9mg/d

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 16
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Rehab‘ period
• Psychic decompensation
• 13.1.2015: ileoscopy (45 cm ): no signs of inflammation
(macroscopic & microscopic) on Entocort .
• Following 3 weeks progressive improvement, discharged on
Jan. 20 2015
• Reevaluation in outpatient clinic february 2015
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 17
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
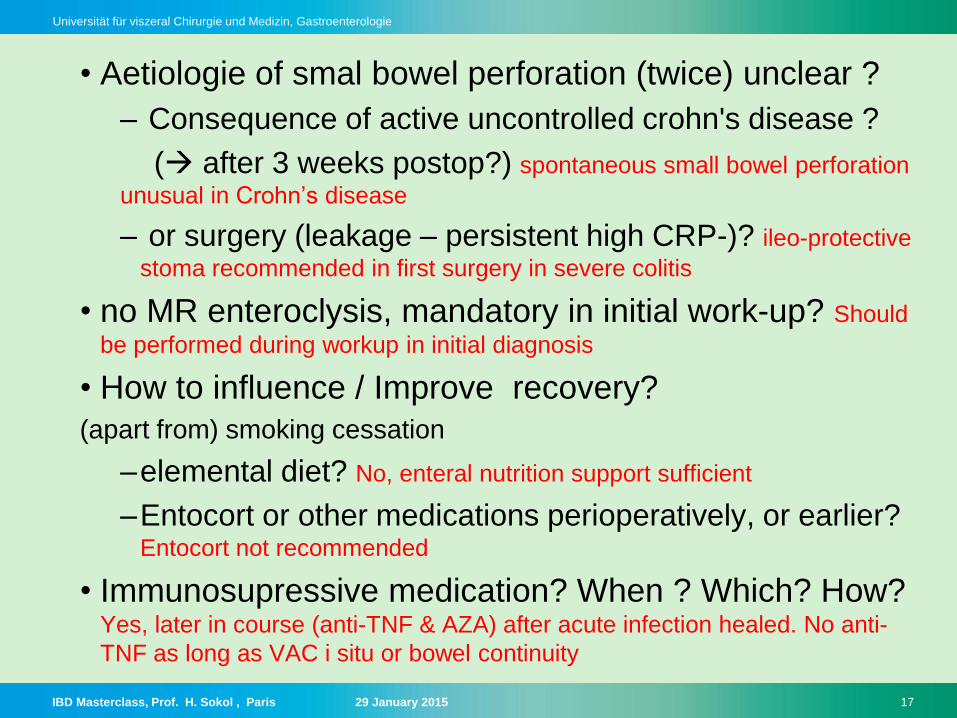
• Aetiologie of smal bowel perforation (twice) unclear ?
– Consequence of active uncontrolled crohn's disease ?
( after 3 weeks postop?) spontaneous small bowel perforation
unusual in Crohn’s disease
– or surgery (leakage – persistent high CRP-)? ileo-protective
stoma recommended in first surgery in severe colitis
• no MR enteroclysis, mandatory in initial work-up? Should
be performed during workup in initial diagnosis
• How to influence / Improve recovery?
(apart from) smoking cessation
–elemental diet? No, enteral nutrition support sufficient
–Entocort or other medications perioperatively, or earlier? Entocort not recommended
• Immunosupressive medication? When ? Which? How?
Yes, later in course (anti-TNF & AZA) after acute infection healed. No anti-
TNF as long as VAC i situ or bowel continuity

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 18
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Case 2
• Tobias Ernst

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 19
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease:
17 years old female patient
• Symptoms at initial presentation:
– chronic watery diarrhea up to 2x/d without blood in the stool
– lower abdominal pain
• laboratory values:
– hemoglobin (104 g/l), CRP 13 mg/l, ferritin 7 µg/l,
transferrin saturation 9%, fecal calprotectin 623 mg/kg,
neg. c-ANCA, neg. p-ANCA, pos. PAB
• examination:
– gastroduodenoscopy & colonoscopy aphthous lesions
in duodenal bulb and terminal ileum, no particular
histopathological findings
– abdomen MRI and no particular echographic findings
• therapy:
– initially Salofalk® 2x1 g per day because of a high
degree of psychological strain, additional iron replacement
– side effects: headache, nausea & symmetrical distal arm- and
leg disorder therefore therapy changed to 9 mg Budesonide
08/2012 – 1st flare

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 20
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease: 12/2012 – 2nd flare
• symptoms:
– after reduction and hold of Budesonide, patient complaints increase without
extraintestinal manifestations
• laboratory values:
– hemoglobin (132 g/l), CRP 3 mg/l, fecal calprotectin 1087 mg/kg
• therapy:
– Budesonide 9mg/d restarted
• procedure:
– Tapering of Budesonide and combination with Modulen®
• conclusion:
– at that stage: a functional component is considered because of negative results in
endoscopy, MRI and US begin with relaxation technique

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 21
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease: 05/2013 – 5 months later
• symptoms:
– patient feels well
• laboratory values:
– normal hemoglobin, CRP 4 mg/l, fecal calprotectin 144 mg/kg, normal values of
vitamin b12, 25-hydroxy-vit d3 and folic acid
no absorption disorder and decrease of inflammation
• therapy:
– Modulen® monotherapy
• procedure:
– next control in 6 months

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 22
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease: 09/2013 – 3rd flare
• symptoms:
– increase of abdominal pain and defecation frequency to 3x/d in the past 3 weeks
– but no pain and normal defecation frequency at the moment
• laboratory values:
– CRP 13 mg/l, fecal calprotectin 244 mg/kg
• therapy:
– Budesonide 9 mg per day by self medication since 3 weeks before
• procedure:
– begin with azathioprin (Imurek®) 50 mg
– To enable Entocort sparing
http://www.ibdetermined.org/ibd-information/ibd-treatment/ibd-
medication.aspx

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 23
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease: 05/2014 – 4th flare
• symptoms:
– relapse after stopping Budesonide despite therapy with azathioprin (Imurek®) 100 mg
– high stool frequence with bloody stool
– PCAI-score=20
• laboratory values:
– fecal calprotectin 600 mg/kg
• procedure:
– repeat ileocolonoscopy just minimal inflammation in the cecum without histopathological stigmata
based on symptoms and course of disease: Crohn’s disease A1 L1+L4 B1

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 24
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease: 09/2014 – 4 months later
• symptoms:
– normal stool frequency, no blood after an increase of azathioprin (Imurek®) 125 mg, but
still abdominal pain
– lactose-free diet without success
• laboratory values:
– fecal calprotectin 611 mg/kg
• examination:
– positive fructose breathing test
– DD: SIBO (small intestinal bowel overgrowth) therapy with metronidazol 2x500 mg/d
• procedure:
– testing of 6-thioguanine (6-TGN) and 6-mercaptopurine (6-MMP)

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 25
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease: 11/2014 – 2 months later
• symptoms:
– still abdominal pain
• laboratory values:
– still elevated fecal calprotectin
– 6TGN=314 pmol/8x108 (09/2014)
– 6-MMP=3134 pmol/8x108 (09/2014)
• procedure:
– dose escalation with azathioprin (Imurek®) 150 mg

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 26
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease: 12/2014 – 1 months later
• symptoms: – still abdominal pain and high stool frequency
• laboratory values:
– fecal calprotectin 91 mg/kg (improvement!) on Imurek 150 mg/d
What to do?

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 27
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease: 12/2014 – 1 months later
What to do?
• procedure:
– reduce azathioprin (Imurek®) to 75 mg – suspicion of AE
– Re-Test 6TG /6MMP
– ileo-colonoscopy and gastroscopy MRI enteroclysis: if lesion start Anti-TNF
results !!!!

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 28
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
• examination
– gastroduodenoscopy & colonoscopy without any signs of inflammation
– MRI: no lesions
• therapy:
– 25 mg azathioprin (Imurek®)
– 100 mg allopurinol
Course of disease: 12/2014 – 1 months later

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 29
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
• symptoms:
– patient feels well without any symptoms
• laboratory values:
– CRP 12 mg/l, ESR (erythrocyte sedimentation rate) 22 mm/h
Current situation 01/2015

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 30
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Summary
17 year old female patient with Crohn’s disease
• symptom onset 08/2012: elevated CRP, anemia and chronically watery
diarrhea without extraintestinal manifestations
• late diagnosis in 05/2014, after almost 4 flares
• 2 gastro-duodenoscopies /3 ileo-colonoscopies
• different doses of azathioprin (Imurek®) tried from 25 mg up to 150 mg
• present condition: asymptomatic after dose reduction of azathioprin
(Imurek®) and beginning of allopurinol therapy

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 31
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Discussion
• How do you distinguish between abdominal pain caused by Crohn’s disease and
abdominal pain caused azathioprin?
– It is very difficult to distinguish. Sometimes the time connection with the beginning of azathioprin
therapy may help you.
• How do you define a flare?
– An increase in subjective symptoms and increase in laboratory values.
• Should TPMN-activity be tested by default?
– If there are no problems with a therapy with azatioprin, you don’t have to test it. We don’t test it
by default.
• When should you check 6-TGN and 6-MMP?
– In our hospital we don’t measure these, but if unexplainable problems in context with a therapy
with azathioprin occur, you should test them.
• What increase is typical for this type of liver cytotoxicity (DD: EBV, Hepatitis)?
– You can’t differ between the cause by evaluating the elevated liver enzyms.
• When do you use allopurinol in this context and what are the most important side
effects?
– We don’t use allopurinol in this context, but there are the same side effects as in therapy of gout.
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 32
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
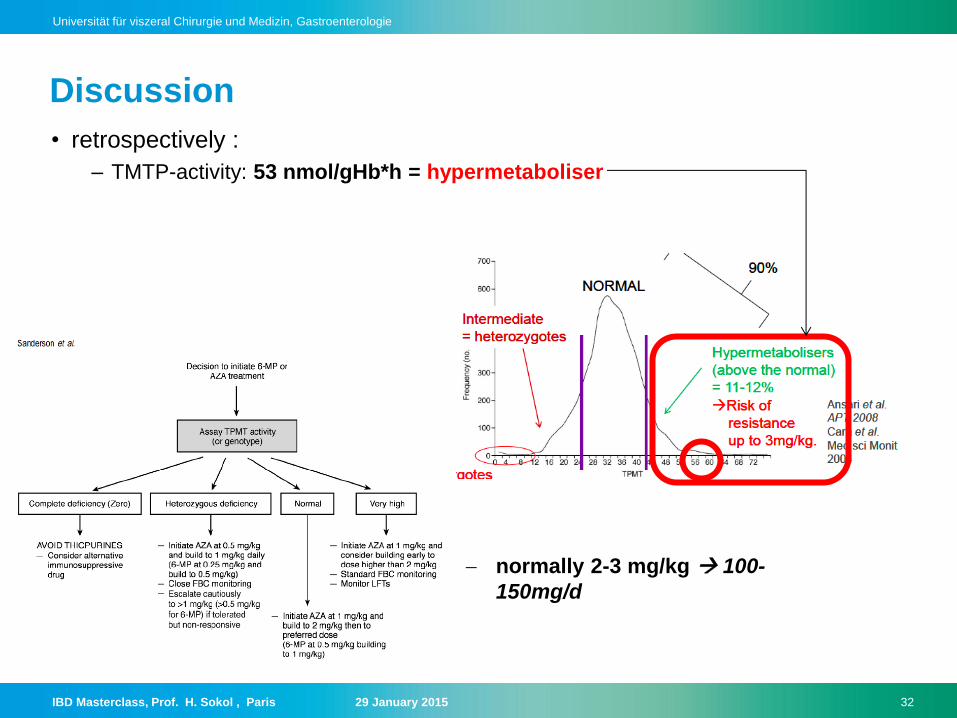
• retrospectively :
– TMTP-activity: 53 nmol/gHb*h = hypermetaboliser
Discussion
normally 2-3 mg/kg 100-
150mg/d
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 33
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
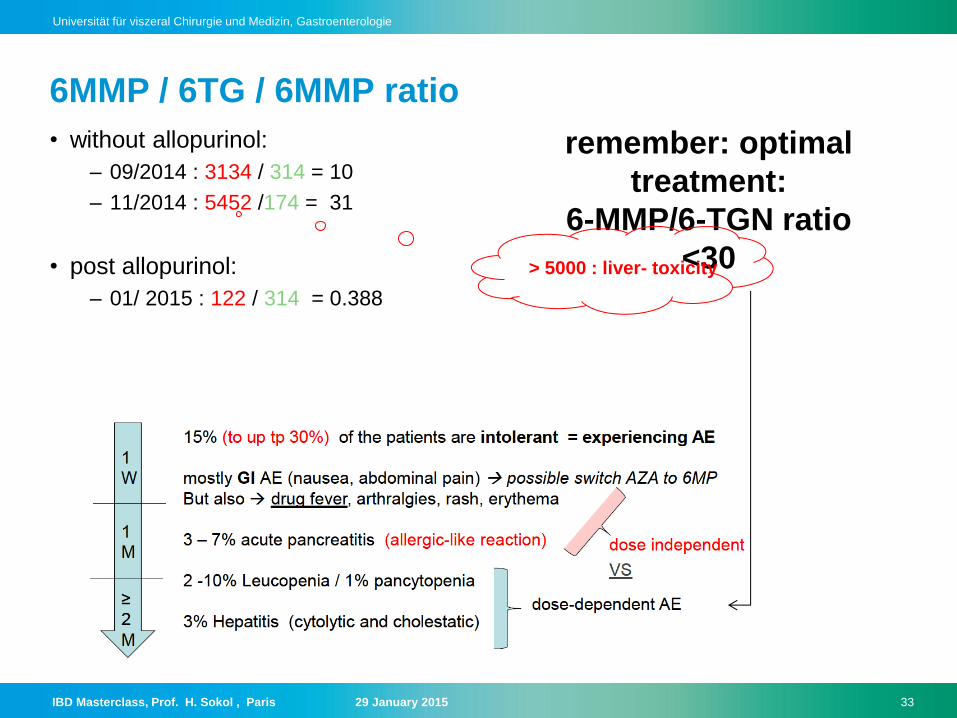
6MMP / 6TG / 6MMP ratio
• without allopurinol:
– 09/2014 : 3134 / 314 = 10
– 11/2014 : 5452 /174 = 31
• post allopurinol:
– 01/ 2015 : 122 / 314 = 0.388
remember: optimal
treatment:
6-MMP/6-TGN ratio
<30 > 5000 : liver- toxicity

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 34
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Discussion • consequences of increased TPMT activity
Bible Class on Thiopurine Use in IBD, February 6th, 2013, Dr med P. Juillerat,
M.Sc.

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 35
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Discussion • effects of adding allopurinol
Bible Class on Thiopurine Use in IBD, February 6th, 2013, Dr med P. Juillerat,
M.Sc.

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 36
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Case 3
• Roseline Ruetsch
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 37
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
38 years old patient, female
Colitis ulcerosa, diagnosed 2008
• Non-smoker status
• Family history: grandfather and one cousin affected by UC,
siblings with IBS
• Initial presentation: proctocolitis with segmental
presentation in colon descendens
• Extraintestinal manifestations:
- Axial and peripheral spondylarthropathy
- Recurrent episodes of iridozyklitidis (prior to
gastrointestinal manifestation !)

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 38
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
38 years old patient, female
Colitis ulcerosa, diagnosed 2008
• Initially steroid dependent course with glucocorticoid
treatment 12/2008-2012
severe osteopenia
• Azathioprin since 01/2009
• Infliximab 01/2011 -09/2011
• Adalimumab 01/2011 – 04/2013 (stopped due to extra-
intestinal symptoms – lupus-like and fever)
• 04/2014 salofalk 3g and azathioprin 100mg with clinically
remission

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 39
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
38 years old patient, female
New Flare 08/2014 – clinical presentation:
• Recurrent diarrhea with urgency, tenesmus and abdominal
cramps, bloody diarrhea (up to 20x day; 6x nights), fever
(38°C), weight loss: 5kg.
• NB: change of hormonal contraception just before new
flare (Gynera -Gestodenum, Ethinylestradiolum- / Cerazette Desogestrelum( Progesteron)

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 40
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
38 years old patient, female
New Flare 08/2014 2014 – treatment (extern):
• No response after 2 weeks prednison oral (50mg )
• Colonoscopy (extern) proctocolitis ulcerosa with segmental
pattern
• Infliximab 09/2014 (1 shot) without clinicial response
• 10/10/14 rectoscopy: progressive course with new
continious pattern rectum- 45cm ab ano
• Beginn Golimumab 16/10/14 100mg, 30/10 50mg
No response patient referred to University center.

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 41
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Colonoscopy 28/11/2014

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 42
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Pancolitis ulcerosa, macroscopically signs of moderate activity
(Mayo 2), with focal erosionen and fissur/ulceration (high
activity) with signs of reepithelialization (healing process)
up to to distal colon transversum.
Colonoscopy 28/11/2014

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 43
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Question
• 38 year old woman with complicated course of UC, already
treated with all anti TNF agents (1AE, 2 primary non
responder) in outpatient care
• Refered to universitary center from her gastroenterologist
• Endoscopically & histology: moderately active
What would you do at that point ??? GLM induction shema to low at the first time augmentation of the
dosage
Retry strategie induction with IFN was acceptable as 50% of patients reach
remission, BUT do not stop after just 1. shot
Prefer always combo therapy (better response / remission outcome)
GLM: if after a few days no acceptable response that possibility of 2. shot
after a few days for intensive induction
Contact surgery and discuss colectomy

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 44
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
• Treatment proposition at this time:
Hypothesis of inadequately conducted induction with
golimumab so:
New induction regimen with golimumab,
initially 200mg (19.11.2014), than 100mg
(30.11.2014)(26.12.2014) at outpatient clinic
38 years old patient, female
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 45
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
38 years old patient, female
• A few days later:
07.12.15: Beginn with Valcyte 900mg qid (until
06.01.15)
Valcyte: treat even if low PCR
copys, as an option to stop
any pro-inflammatory process
, cave offen with negativ
histology, even
immunohistochemistry !!! So
do not only trust histo
Cave, different if PCR in blood positive then of course treat with antiviral tt
but then reduce immunosuppression because sign an systemic infection !!
CMV+IBD colitis trigger for inflammation and inversely treat both (IS+antiviral)
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 46
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
38 years old patient, female
• Initial clinical improvement with clearly improvement of the
abdominal cramps, less diarrhea, less tenesmus.
• BUT, new pejoration after 3. Godulimab 23.12.2014
with high diarrhea frequency (20x), bloody bowel movement,
increased pain, important night symptoms
Lab values: hypoalbuminemia, high CRP

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 47
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
endoscopy 08.01.2015
Mayo endoscopic classification 3

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 48
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Question
What would you do at that point ???
So now situation of pancolitis pejoration of the situation
Refer to surgery for colectomy, also to reduce the neoplasia risk
secondary to continued high inflammatory activity by a patient with
disease history >8Y
Cyclosporin could be an option, as also Vedolizumab (but cave delayed
activity so perhaps not in these high acute situation with high
inflammation)
Hospitalization on the 08.01.2015 for intraveinous steroid
application

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 49
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
38 years old patient, female
CRP evolution
Albumin evolution
Calprotectin
evolution

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 50
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Campylobacter concisus facultative pathogenic germ,
mainly by IBD and immunosuppresion Cipro 500mg
2x/day 10 days

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 51
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Hospital course:
• Initial empiric antibiotic treatment with Metro/Cipro and
again trial with valcyte (08.01-12.01) by suspiscion of
superinfected colitis
• New antibiotical course (Campylobacter Consisius)
• IV steroid (Solumedrol 60mg 08.01 -22.01) Don’t stop the iv therapy to quikly, otherwise high risk for relapse, oral
form not so well absorbed, mainly because of the hypoalbuminemia (less
because of colitis) even if initial evolution very positive !!! Better
prolongate hospitalization with iv steroids
• Topical therapy with Salofalk 1gr und Budenofalk 2mg with
good tolerance and clinical response
• Azathioprine initiated, then stopped because of suspiscion
of induction of new pejoration

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 52
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Evolution
• After 3 weeks hospitalization clinical amelioration
• First contact with visceral surgery
• iv corticoids oral steroids
• Pejoration after adjunction of azathioprin stop actually
• Oral nutrition support with special nutrition drinks
• Last clinical evolution: 26/01/15 significant reduced pain,
bowel mouvement. Hypophosphatemia. Hypoalbuminemia.
• Patient discharged in good condition with oral prednisone
60mg/day
• Plan for further treatment: oral tapered steroid treatment,
start in a trial setting with anti-integrin agent

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 53
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Discussion
• Optimal time for hospitalization ?
• Which treatment ?

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 54
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Discussion
• When should we consider surgical treatment ? Should we
try again whith cyclosporine / tacrolimus ?
Remain delicate, especially in young patient, psychological acceptance with
this project needed, also difficult for the gastroenterologist to give up after a so
long trial with medical treatment
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 55
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Case 4
• Claudia Münger

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 56
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
55 year old female patient
• Crohn‘s disease, diagnosed in 2010:
isolated terminal ileitis
• Positive family history (sister died of the complications of
Crohn‘s disease, at age 39!)
Treatment
–5-ASA
–Systemic steroids
– Intolerance for multiple medications: Thiopurines stopped
because of nausea; budenoside…

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 57
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
• Patient wishes a stool transplantation
Colonoscopy 11/2013:
Known terminal ileitis with moderate activity over 2-3cm. No
stenosis.
application of donor stool during the colonoscopy

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 58
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
• Follow-up: clinical improvement for about 2 weeks, then
the comeback of the symptoms (abdominal pain)
• We suggested a second stool transplantation with a
different method: via jejunal tube

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 59
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
• Follow-up: only slight improvement of the bloating and
diarrhea.
• Calprotectin 525 mg/kg
Treatment with anti-TNF (Adalimumab)

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 60
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
• Follow-up under anti-TNF
– Improvement of the abdominal pain and of the diarrhea, stool
frequency 4-5x/d
–Normalisation of the CRP and calprotectin (47 mg/kg)

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 62
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Case 5
• Lorenzo Macchia

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 63
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Female, 78 years old
• Atrial fibrillation on anticoagulants
• Biological aortic valve replacement
many antibiotics in the past due to recurrent
cystitis and as prophylaxis before visiting the dentist at
least twice a year.
• Diverticulosis
History

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 64
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Female, 78 years old
December 2013: recurrent diarrhea
Diagnosis: Clostridium Difficile colitis
Therapy: Metronidazole, 2 per day for 7 days
Diarrhea stops
Initial presentation

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 65
Universität für viszeral Chirurgie und Medizin, Gastroenterologie

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 66
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
10 January 2014: patient brakes her wrist
Diarrhea starts again
Therapy: Metronidazole, for 9 days
Diarrhea stops
Previous
New episode

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 67
Universität für viszeral Chirurgie und Medizin, Gastroenterologie

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 68
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
24 January 2014: subdural hematoma
Diarrhea starts again
Therapy: Vancomycin, 4 per day until 10 March 2014
Diarrhea stops
Previous
New episode

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 69
Universität für viszeral Chirurgie und Medizin, Gastroenterologie

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 70
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
18 March 2014: 8 days after the end of the previous therapy cycle
Diarrhea starts again
Therapy: Vancomycin, tapering process
Diarrhea stops
Previous
New episode

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 71
Universität für viszeral Chirurgie und Medizin, Gastroenterologie

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 72
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
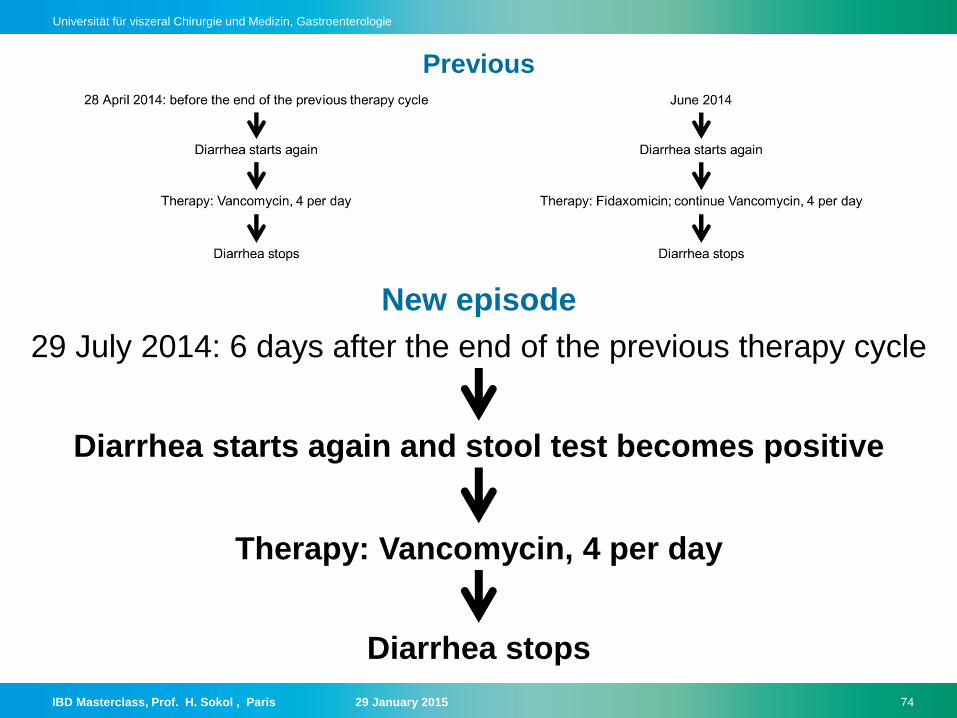
28 April 2014: before the end of the previous therapy cycle
Diarrhea starts again
Therapy: Vancomycin, 4 per day
Diarrhea stops and stool test becomes negative
Previous
New episode

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 73
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
June 2014
Diarrhea starts again
Therapy: Fidaxomicin; continue Vancomycin, 4 per day
Diarrhea stops
Previous
New episode
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 74
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
29 July 2014: 6 days after the end of the previous therapy cycle
Diarrhea starts again and stool test becomes positive
Therapy: Vancomycin, 4 per day
Diarrhea stops
Previous
New episode

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 75
Universität für viszeral Chirurgie und Medizin, Gastroenterologie

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 76
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
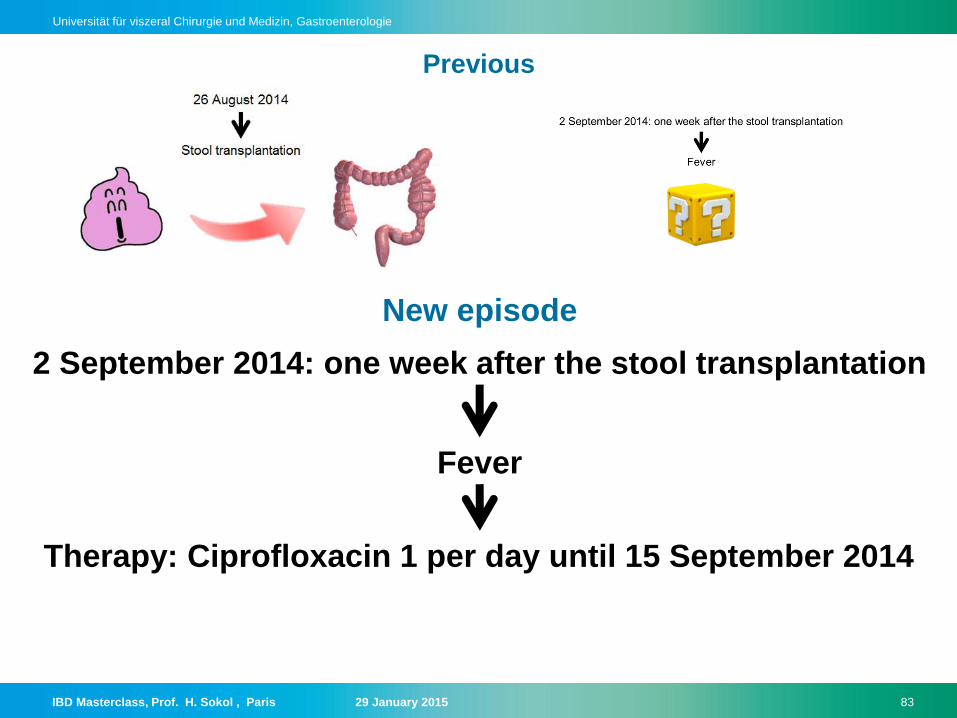
26 August 2014
Stool transplantation
Therapy

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 77
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
2 September 2014: one week after the stool transplantation
Fever
Previous
New episode

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 78
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Bacterial translocation?
Differential diagnosis
Port-a-cath infection?
Urinary tract infection?
Endocarditis?

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 79
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Positive for Proteus Mirabilis
Blood culture

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 80
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
No focus of infection
Abdomen CT scan

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 81
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
No focus of infection
Abdomen CT scan

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 82
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
No focus of infection or infiltration
Chest X-ray
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 83
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Therapy: Ciprofloxacin 1 per day until 15 September 2014
Previous
2 September 2014: one week after the stool transplantation
Fever
New episode

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 84
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
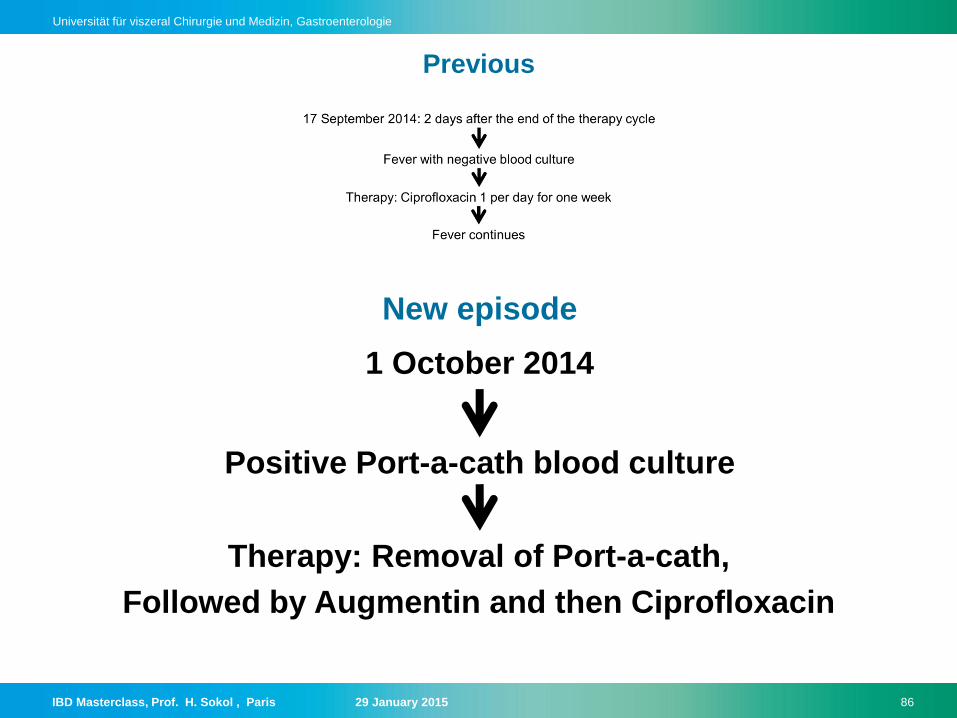
Therapy: Ciprofloxacin 1 per day for one week
Fever continues
Previous
17 September 2014: 2 days after the end of the therapy cycle
Fever with negative blood culture
New episode

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 85
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Persistent fever
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 86
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Therapy: Removal of Port-a-cath,
Followed by Augmentin and then Ciprofloxacin
Previous
1 October 2014
Positive Port-a-cath blood culture
New episode

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 87
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
The patient is finally better!
No recurrence of Clostridium Difficile
infection
Negative blood culture

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 88
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Questions
• Should the fecal transplantation have been considered
before? Once the recurrence of the infection had been seen, fecal
transplantation should have been considered
• Through which mechanisms does fecal transplantation
help in the treatment of recurrent colitis and IBD? It re-
establishes the balance between the bacteria populations thus creating a less
favorable environment for C. Difficile
• Are there other ways of re-establishing the balance in the
bacterial flora? There are a few possible alternatives which are being
studied and compared: one is Perenterol and the other one consists in 15
capsules containing treated fecal matter, to be given orally

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 89
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Questions
• What are the risks of fecal transplantation? Fecal transplantation
is a very safe procedure. Very few complications have been reported.
• Does this situation occur frequently in your experience? The
post-procedure complication in this patient were independent from the fecal
transplantation, which is very safe.
• What are the risks in patients with multiple morbidities? See
above (very safe procedure)
• Should we use another Stool transplantation method in
these patients? (e.g. enema) Prof. Sokol always uses the enema
method for all patients

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 90
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Case 6
• Markus Herzig

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 91
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
55 year old male patient
Ulcerative colitis E3
• First diagnosed 2003, pancolitis
• Initially diagnosed as Crohn’s disease due to granulomas
on histology, diagnosis changed to ulcerative colitis 2013
• ANCA, ASCA and PAB negative
• No extraintestinal manifestations

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 92
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease
• Flare 02/2004 despite steroids, start azathioprine
• Azathioprine intolerance: elevated transaminases,
lymphopenia, impaired renal function
• Start with MTX
• 1-2 flares/year, remission on steroids

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 93
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease
• 2007 only partial remission on steroids
• 2007-2011 4 doses of Infliximab and MTX, complete
remission
• Patient lost to follow up 2011-2013
• 2013 flare: bloody diarrhea, abdominal pain,
• Calprotectin >600mg/kg

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 94
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Colonoscopy 2013
Pancolitis, no CMV
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 95
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease
• Mesalazine granulate and enema no effect
• Prednisone 30 mg/d 4 weeks 6-7 bowel movements,
bloody stool
• MTX 15mg s.c. 1x/week 4 weeks no effect

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 96
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Sigmoidoscopy February 2014
Pancoltits, no CMV

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 97
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease
• Start Infliximab 07.02.2014: rapid response after first
infusion, MTX stopp
• 21.02.2014 second Infliximab-Infusion: anaphylaxis
(exanthema, bronchospasm, collapse)
• 6-7 bloody bowel movements daily

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 98
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Discussion
• WHAT TO DO ?
• Further combination of Metothrexate with an anti-TNF, p.e.
Adalimumab
• Alternative: switch to Golimumab

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 99
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Course of disease
• 20.03.2014 Start Adalimumab initial rapid
response
• after 4 weeks of Adalimumab: 5 bowel
movements, intermittent bloody stool
• 14.07.2014 colonoscopy: Colitis of rectum and
sigma

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 100
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
TL and ABs
• Adalimumab trough-level: <0.024ug/ml
• Adalimumab antibody: 218.2 UA/ml

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 101
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Discussion
• WHAT TO DO ?
• Switch to Golimumab as an option
• Combination with Metothrexate at least for 6 months.
• Premedication with corticosteroids not recommended
• If Golimumab fails: Vedolizumab in combination with
Metothrexate

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 102
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Answer
• Start Golimumab and MTX
• Patient in remission on Golimumab and MTX

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 103
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Summary
• Steroid dependent / refractory pancolitis ulcerosa
• Treatment failure with
–Mesalazine
–AZA
– Infliximab
–Adalimumab
• Response to Golimumab
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 104
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Discussion
• Continue MTX?
• Premedication with Prednisone, H2-Antagonist ?
• If Golimumab fails: Certolizumab? Vedolizumab?
• Tacrolimus?
• Cross-reaction between anti-TNF?
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 105
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Case 7
• Susanne Schibli
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 106
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Ulcerative Colitis and bugs
Susanne Schibli Pädiatrische Gastroenterologie, Hepatologie, Ernährung Medizinische Kinderklinik, Inselspital, Bern
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 107
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
L. ML 12 yo
• First presentation 2/2014
• Family holidays in South Africa 12/2013
• Not ill during 4wk trip
• After return, small amounts of fresh blood and
mucus in stool
• 3-4 BM/d, soft stool, once liquid
• Mild abdominal pain, not related to BM
• Normal activity
• Muscle pains in legs, no arthritis
• Previously healthy, normal growth (weight, height P
75)
• Mild asthma, multiple allergies (dust mites, birch)

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 108
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
L. ML 12 yo
• First presentation 2/2014
• Hb 129, MCV 82, Tc 282, Albumin 38, CRP<3, BSR 9
• Calprotectin >600
• Stool positive for
•Blastocystis hominis
•Endolimax nana cysts (reports of bloody diarrhea)
• No response to metronidazol

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 109
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
03/2014
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 110
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
L. ML 12 yo
• 3/2014
• Pancolitis ( - Colon transversum)
• Histology; lympho-plasmacellular infiltrates, mild
chronic changes (crypt distorsion, elongation)
• p-ANCA positive
• DD: infectious, UC
• 5-ASA: orally 2g, topically daily
• 5/2014
• Good response, clinical remission, PUCAI 0,
Calprotectin 58

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 111
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
L. ML 12 yo
• 6/2014
• Flare, bloody diarrhea, Calprotectin 600
• Stool cultures: Camplylobacter concisus
• Ciprofloxacin 2wks, 5-ASA po and enema
• Good response, resolution of bloody diarrhea
• 8-9/2014
• Flare, bloody diarrhea
• Stool cultures: Aeromonas caviae
• Entocort enema (partial response), Ciprofloxacin

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 112
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
L. ML 12 yo
• 10/2014
• 2 days after stop of Ciproxin, again bloody diarrhea
• Holidays in Germany
• Sigmoidoscopy with Pancolitis
• Prednison 50mg, partial response
• Tapering schedule: PDN 30mg, worsening of
diarrhea
• Stool cultures: Camplylobacter concisus
• 11/2014
• Colonoscopy under tx with PDN 30mg

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 113
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
11/2014

IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 114
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
L. ML 12 yo
• 11/2014
• Mainly nocturnal stools, incontinence, mild pains
• Almost normal daily activity
• Hb 139, MCV 82, Tc 282, Albumin 39, CRP<3, BSR 5
• Calprotectin 529
• Stool cultures: Camplylobacter concisus
• Tapering Prednison
• Ciprofloxacin, Metronidazol, Amoxicillin
• Start Mutaflor
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 115
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
L. ML 12 yo
• 12/2014
• Well under triple AB-therapy
• Few days after dc of AB, again soft stools, no blood
• C. diff positive
• Spontaneous improvement
• 1/2015
• Clinically well, PCDAI 15
• Calprotectin 250
• Treatment: Salofalk po and topically, Mutaflor
IBD Masterclass, Prof. H. Sokol , Paris 29 January 2015 116
Universität für viszeral Chirurgie und Medizin, Gastroenterologie
Discussion
• Ulcerative Colitis
• Campylobacter consicus
• Aeromonas, Endolimax, Blastocystis
• C.diff
• Steroid non-responder
• Treatment options?