dietary intake of specific carotenoids and vitamins a, c ... · abstract we determined whether...
TRANSCRIPT

Vol. 5, /47-153, Marc/i /96 Cancer Epidemiology, Biomarkers & Prevention 147
Dietary Intake of Specific Carotenoids and Vitamins A, C, and E, and
Prevalence of Colorectal Adenomas’
Shelley M. Enger,2 Matthew P. Longnecker,Miao-Jung Chen, Janice M. Harper, Eric R. Lee,Harold D. Frankl, and Robert W. Haile
Department of Preventive Medicine. University of Southern California School
of Medicine. Los Angeles. California 90033�l042 [S. M. E., J. M. H..
R. W. HI: Department of Epidemiology. University of California-Los Angeles
School of Public Health. Los Angeles. California 90024 IM. J. C.]: Divisionsof Gastroenterology. Belltlower IE. R. L.] and Sunset H D. F.J Kaiser
Permanente Medical Centers. Los Angeles. California 90027: and
Epidemiology Branch. National Institute of Environmental Health Sciences,
Research Triangle Park. North Carolina 277()9 IM. P. L.l
Abstract
We determined whether intakes of the main dietarycarotenoids (a-carotene, a-carotene, �-cryptoxanthin,lutein plus zeaxanthin, and lycopene) and of vitamins A,C, and E were associated with the prevalence ofcolorectal adenomas among male and female members ofa prepaid health plan in Los Angeles who underwent
sigmoidoscopy (n = 488 matched pairs). Participants,ages 50-74 years, completed a 126-item semiquantitative
food-frequency questionnaire and a nondietaryquestionnaire from 1991 to 1993. In the univariate-matched analysis, a-carotene, 1.3-carotene (with andwithout supplements), �.cryptoxanthin, lutein pluszeaxanthin, vitamin A (with and without supplements),and vitamin C (with and without supplements) wereassociated with a decreased prevalence of colorectaladenomas. After adjustment for intake of calories,saturated fat, folate, fiber, and alcohol, and for currentsmoking status, body mass index, race, physical activity,and use of nonsteroidal anti-inflammatory drugs, only
a-carotene including supplements was inverselyassociated with adenomas [odds ratio (OR), 0.6; 95%
confidence interval (CI), 0.4-1.1; trend, P = 0.04; ORscompare highest to lowest quartilesi; vitamin C showed aweaker inverse association (OR, 0.8; 95% CI, 0.5-1.5;
trend, P = 0.08); and the remaining compounds were nolonger clearly associated with risk. After including 13-carotene with supplements and vitamin C simultaneouslyin the multivariate model, the association of 13-carotenewith supplements with adenomas was weakened (OR, 0.8;95% CI, 0.5-1.3; trend P = 0.15), and vitamin C was nolonger associated with risk. These data provide only
modest support for a protective association of 13-carotenewith colorectal adenomatous polyps.
Introduction
The protective association of fruit and vegetable intake with therisk of colorectal polyps and cancer ( I - 8) may be due to
specific compounds found in those foods. Fruits and vegetables
are the main sources of vitamin C and carotenoids in the diet(9-1 1) and account for >20% of vitamin E intake in the UnitedStates ( 12). Preformed vitamin A is obtained from animalproducts, but provitamin A carotenoids, which contribute ap-
proximately one-third of total vitamin A intake, are derivedlargely from fruits and vegetables 13, 14). Although the pro-vitamin A carotenoids may have anticarcinogenic properties
through the conversion to vitamin A, these and the nonprovi-tamin A carotenoids also have antioxidant and other potentially
anticarcinogenic properties independent of conversion to vita-mm A (9). The carotenoids and vitamins C and E have anti-
oxidant, immunomodulation, and other properties that may
inhibit the development of carcinoma (9). Vitamin A also has
anticarcinogenic properties through its abilities to stimulate the
immune system and regulate cellular differentiation (15). De-spite the anticarcinogenic potential of these compounds, obser-
vational studies and randomized controlled trials evaluating the
effect of dietary carotenoids and vitamins A, C, and E on riskor recurrence of polyps have given inconsistent results (5-8,16-22), and no studies have investigated the role of specific
carotenoids other than f3-carotene on the prevalence of cob-rectal adenomas.
Until recently, an estimate of the 13-carotene content offoods was available, but not ofother specific carotenoids. Using
the newly available database for specific carotenoids (10), LeMarchand ci a!. (23) found that a-carotene and lutein pluszeaxanthin were inversely associated with the risk of lung
cancer. Their results support the need for investigation of theintake of specific carotenoids in relation to other neoplastic
processes.
Much evidence supports the concept that colorectab carci-noma may develop within an adenomatous polyp (24-28).Because diet may influence the occurrence of coborectab ade-
nomas, we examined the relationship of dietary intake of spe-cific carotenoids and vitamins A, C, and E with the prevalence
of adenomas in a group of men and women who underwentsigmoidoscopy.
Received 5/30/95: revised I 2/4/95: accepted I 2/5/95.
The costs of publication of this article were defrayed in part by the payment ofpage charges. This article must therefore be hereby marked advertisement in
accordance with I 8 U.S.C. Section 1734 solely to indicate this fact.I Support for this study was provided by National Cancer Institute Grants 1-ROl-
CA51923-OlAl and NCI Cancer Education Program Grant CA-49565.
2 To whom requests for reprints should be addressed, at University of Southern
California School of Medicine, Department of Preventive Medicine. 1420 SanPablo Street. PMB A202, Los Angeles. CA 90033.
Subjects and Methods
Subjects were eligible for the study if they underwent sigmoid-oscopy at either of two Southern California Kaiser Permanente
Medical Centers (Bellflower and Sunset) from January 1 , 1991,to August 25, 1993. Eligible men and women were ages 50-74years; were free of invasive cancer, inflammatory bowel dis-
ease, and familial polyposis: were fluent in English: had no
on March 3, 2020. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

148 Antioxidant Vitamins and Colorectal Polyps
previous bowel surgery or history of polyps; were residents of
metropolitan Los Angeles; and had no physical or mental
disability precluding an interview. In addition, subjects who
had severe gastrointestinal symptoms were excluded. Caseswere subjects diagnosed for the first time with one or more
histologically confirmed adenomatous polyps. Controls had no
polyps of any type at sigmoidoscopy, and were individually
matched to cases by gender, age (within 5-year category), date
of sigmoidoscopy (within 3-month category), and Kaiser
Center.During the accrual period, we identified 628 cases and 689
controls who were potentially eligible. Of these, 70 cases and
94 controls refused interview, and we were unable to contact 29
cases and 32 controls. Thus, we obtained interview data for 529
cases and 563 controls. The response rate (number interviewedl
number eligible) was 84% among cases and 82% among con-trols. If the control subject initially matched to a case was notinterviewed, a replacement control subject was identified.
Among interviewed subjects, the indications for sigmoid-
oscopy were routine for 45% of cases and 44% of controls,
referred to specific minor symptoms for I 6% of cases and 13%of controls, and were not given for 39% of cases and 43% of
controls. The average depth of penetration of the flexible sig-
moidoscope was 55 cm for cases [± I 1 (SD) cm; minimumdepth, 10 cm] and 59 cm for controls (± 5 cm; minimum depth,
34 cm). Fifteen cases had carcinoma in situ within an adeno-
matous polyp. The size and number of polyps were indicated on
a study form completed by the sigmoidoscopist. For 71% ofcases, the largest polyp was < 1 cm in diameter, and 79% of
cases had only one polyp. Colonoscopy reports were collectedfor all cases who underwent colonoscopy after sigmoidoscopy,but only polyps detected at sigmoidoscopy were included in the
analyses.
Participants provided data on smoking, therapeutic drug
use, physical activity, height, weight. family history of cancer,and other factors during a 45-mm in-person interview. The
interview was administered on average 5 months after sigmoid-
oscopy. Questions about exposure referred to the time before
sigmoidoscopy. The interviewer remained unaware of the case
or control status of the participant for 70% of cases and 87% of
controls.Five hundred nineteen cases and 556 controls completed a
126-item semiquantitative food-frequency questionnaire (29)
that inquired about diet in the year before sigmoidoscopy. This
analysis was restricted to matched pairs with complete dietary
data. Of 505 matched pairs, 488 pairs had complete dietary
data. Unmatched controls occurred when the case to whom thecontrol was matched was found not to speak English, or was
found to have invasive large bowel cancer at follow-upcolonoscopy. Unmatched cases occurred when we were unable
to interview a corresponding eligible control.
The self-administered food-frequency questionnaires were
collected and reviewed at the time of the interview. Standardmethods were used to calculate nutrient intakes (30). Specificfoods corresponding to items on the questionnaire were selected
based on the relative frequency of consumption among partic-
ipants in the 1988-1989 Nationwide Food Consumption Sur-vey (3 1 ), southwest region. Food carotenoid values were ob-
tamed from a nutrient database published recently by Mangels
ci a!. ( 10). For all other nutrients, the Nutrition Data System
(Ref. 32; nutrient database Ver. 21) was used as a nutrient
database for foods. Data on the gram weights for standardportions of items on the questionnaire and the nutrient content
of supplements were obtained from the Harvard School of
Public Health.3 For each subject, the reported frequency of
consumption of each item on the questionnaire was multipliedby the nutrient content of the corresponding amount of thespecified food, and total nutrient intake was obtained by sum-ming across foods the amount of nutrient contributed. Supple-
mental intakes of 13-carotene and vitamins A, C, and E weredetermined by summing intakes from multivitamins with in-
takes from single vitamin supplements.
Conditional logistic regression was used to estimatematched ORs4 and their 95% CIs. Covariates included in the
multivariate model results presented were race [four categories:white, black or Latino (black), nonblack Latino, and Asian or
Pacific Islander]; body mass index (two categories: <24 and�24 kg/rn2); current smoking status (three categories: non-
smoker, current smoker, and ex-smoker); vigorous leisure timeactivity (three categories: 0, >0 to <4, and �4 h/week); use ofnonsteroidal anti-inflammatory drugs (two categories: currentuser and current nonuser); and intakes of energy, saturated fat,alcohol, fiber, and folate (as continuous variables; Table 1).Saturated fat intake, rather than total fat intake, was used in the
model because preliminary analyses revealed that the OR foradenomas was greater among those with higher intakes of
saturated fat than among those with higher total fat intakes.Others (8, 33) observed similar findings. Subjects whose race
was “other” or missing (n = 19) were grouped with whites. One
subject with a missing body mass index was assigned to thelower category of the dichotomous variable. As a test for trendin effect across categories (quartiles) of intake, we used the
two-sided P value associated with a coefficient fit to the con-tinuous variable. Intake variables were transformed using loge
or square root to improve normality.
Results
The average age of the study participants was 62 years, one-third were female, and over one-half were white (Table 1).Nearly twice as many cases as controls were current smokers.On average, the cases were somewhat more overweight andexercised less than the controls. The controls drank less alcohol,ate less saturated fat, and ate more fruits and vegetables than thecases. Intakes of all micronutrients examined, except vitamin E
(not including supplements), were higher for controls than forcases.
In the univariate-matched analysis, a-carotene, 13-carotene(with and without supplements), 13-cryptoxanthin, lutein plus
zeaxanthin, vitamin A (with and without supplements), andvitamin C (with and without supplements) were inversely as-sociated with the prevalence of adenomas (Table 2). After
adjustment for current smoking status, body mass index, race,physical activity, use of nonsteroidal anti-inflammatory drugs,and intake of calories, saturated fat, folate, fiber, and alcohol,
only 13-carotene with supplements was clearly associated with
a decreased prevalence of adenomas. Vitamin C showed aweaker inverse association. The remaining compounds were nolonger clearly associated with risk. When fiber was not in-
cluded in the multivariate model, the results were unchanged.However, when folate was not included in the model, the resultsfor the carotenoids and vitamins resembled the results for theunivariate models (data not shown). After excluding subjectswith carcinoma in situ, the results were not changed. Adjustingfor family history of colorectal cancer, number of cigarettes
3 L. Sampson, personal communication.
4 The abbreviations used are: OR, odds ratio: CI, confidence interval.
on March 3, 2020. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Age (yr)
Sex (3 male)
Cancer Epidemiology, Blomarkers & Prevention 149
Table I Characteristics of the study population (n 488 matched pairs)
Variable
Race”
(3. White
% Black
% Latino. nonblack
% Asian or Pacific Islander
SmokingC/� Current smokers
Ck Nonsmokers
% Ex-smokers
Body mass index (kg/rn2)
% <27
(� �27
Vigorous physical activity (h/wk)”
c/i- 1-13
(;� �l4
Dietary variables
Total calories (kcallday)
Alcohol (g/day)
% 0-13
% >13
Fiber (g/day)
Saturated fat (g/day)
Folate (pg/day)
Fruits and vegetables
(servings/day)
ri-Carotene (pg/day)
/3-Carotene (�.LgIday)
n-Carotene with supplements
(�.tg/day)
f3-Cryptoxanthin (gglday)
Lutein plus zeaxanthin
(pg/day)
Lycopene (pg/day)
Vitamin A (lU/day)’
Vitamin A with supplements
(lU/day)
Vitamin C (mg/day)
Vitamin C with supplements
(mg/day)
Vitamin E (mg TE/day)
Vitamin E with supplements
(mg TE/day)
Cases
Mean (SD) Mean (SD)
61.9 (6.7) 61.8 (6.8)
66.6 66.6
55.3 53.9
15.8 17.8
17.2 17.6
11.7 10.7
19.7 11.3
34.4 42.6
45.9 46.1
51.0 58.3
49.0 41.7
76.4 67.4
14.3 18.0
9.2 14.5
2050 (841) 1921 (804)
Controls
44.7
34.6
20.7
18.9
25.2
312
5.5
(9.6)
(13.1)
(146)
(3.7)
46.9
36.7
16.4
20.0
22.2
336
6.2
(9.7)
(12.3)
(157)
(3.8)
915
4840
5110
(894)
(4290)
(4700)
1090
5550
6110
(1430)
(4650)
(5400)
66.7
3260
(95.9)
(2690)
73.4
3850
(81.8)
(3370)
4160
I 1.300
13,800
(3880)
(9500)
(10,700)
4380
12.500
15,100
(5350)
(10.600)
(11,600)
137
338
(99.3)
(385)
154
367
(104)
(392)
8.4
74.1
(4.1)
(139)
8.3
81.4
(4.2)
(151)
‘, Nineteen subjects with a race of “other” and four subjects with race missing
were included with whites.I, Vigorous physical activity was defined as any spare time activity with an MET
value (metabolic rate associated with given activity/resting metabolic rate) of at
least 4. performed at least 3 times/week.(. Total vitamin A (lU/day) was calculated as intake of retinol/0.333 + intake of
�3-carotene/0.6.
smoked, or daily servings of fruits and vegetables did notchange the results. After including 13-carotene with supple-ments and vitamin C in the same multivariate model, 13-caro-tene with supplements showed a weaker inverse associationwith an OR comparing the highest to lowest intake quartiles of0.8 (95% CI = 0.5-1.3; trend P = 0.15), and vitamin C intakewas less associated with risk (OR 0.9; 95% CI 0.5-1.7;
trend P = 0.28).
In a multivariate analysis that included only subjects un-dergoing routine sigmoidoscopy, 13-carotene with supplementsagain showed a weak inverse association with adenomas (OR =
0.5; 95% CI = 0.2-I .0; trend P = 0. 18), and vitamin C showedno association with adenomas (OR = 1.1; 95% CI = 0.5-2.6;trend P = 0.69).
When the data were analyzed separately for left colon
and rectal polyps, the multivariate results did not differ fromresults for left colon and rectal polyps combined (results not
shown). When the data were analyzed separately for small(<1 cm) and large (�1 cm) polyps, the multivariate resultswere not different from the results for all polyps combined
(results not shown).We also assessed the associations of 13-carotene and vita-
mm A, C, and E supplements (including multivitamin use, butnot including dietary intake) with prevalence of adenomas. The
association of 13-carotene supplements with adenomas appearedto be protective (OR = 0.6; 95% CI = 0.3-1.5), but theproportion of subjects taking 13-carotene supplements (2.3% ofcases and 3.6% of controls) was small. The proportions ofsubjects consuming vitamin A (40.1% of cases and 35.9% ofcontrols), vitamin C (49.5% of cases and 46.4% of controls),
and vitamin E (45.3% of cases and 41.2% of controls) supple-ments were sufficient to evaluate the associations, but none of
these supplemental intakes was associated with prevalence ofadenomas (results not shown).
The associations of f3-cryptoxanthin and vitamin E intakeswith adenomas varied by gender (test for the presence of
interaction, P < 0.20). In multivariate models among females,the ORs comparing highest to lowest quartiles of intake for13-cryptoxanthin were 0.4 (95% Cl = 0.2-1. 1; trend P = 0. 1 1),and for vitamin E were 0.4 (95% CI = 0.1-I .2; trend P = 0.06).Intakes of 13-cryptoxanthin and vitamin E were not associatedwith reduced prevalence of adenomas in males.
Discussion
We found that the intake of 13-carotene including supplements
and possibly of vitamin C were associated with reduced prey-alence of colorectal adenomas. After including both compoundsin the same model, however, the association of vitamin C wasno longer important, and the association of 13-carotene wasweakened.
Steinmetz and Potter (9) reported that there are dozens, ifnot hundreds, of classes of compounds in fruits and vegetables
that have anticarcinogenic properties. Because these com-pounds occur in many of the same foods, distinguishing amongtheir effects in epidemiological studies may be difficult orimpossible. However, even after we included folate, fiber, and
vitamin C in the model, the protective association of 13-caroteneincluding supplements was still evident, although the effect sizewas decreased.
Seven case-control studies and one nested case-controlstudy (5-8, 16-19) have evaluated the associations of carote-noid or vitamins A, C, or E intakes with occurrence of cob-
rectal polyps (Table 3), and the findings have varied greatly.
Only two of the studies included fiber intake in the models (17,18). In one of these studies (17), an inverse association with13-carotene intake was found for men only; in the other study(1 8), no associations of polyps with carotene or vitamins A, C,or E intakes were found. Among the other studies, a fewshowed inverse associations of carotene or vitamins A, C, or Eintakes with risk of polyps (5, 7, 8, 19), but the possibility existsthat confounding by other components of fruits and vegetables
accounts for these findings.
on March 3, 2020. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
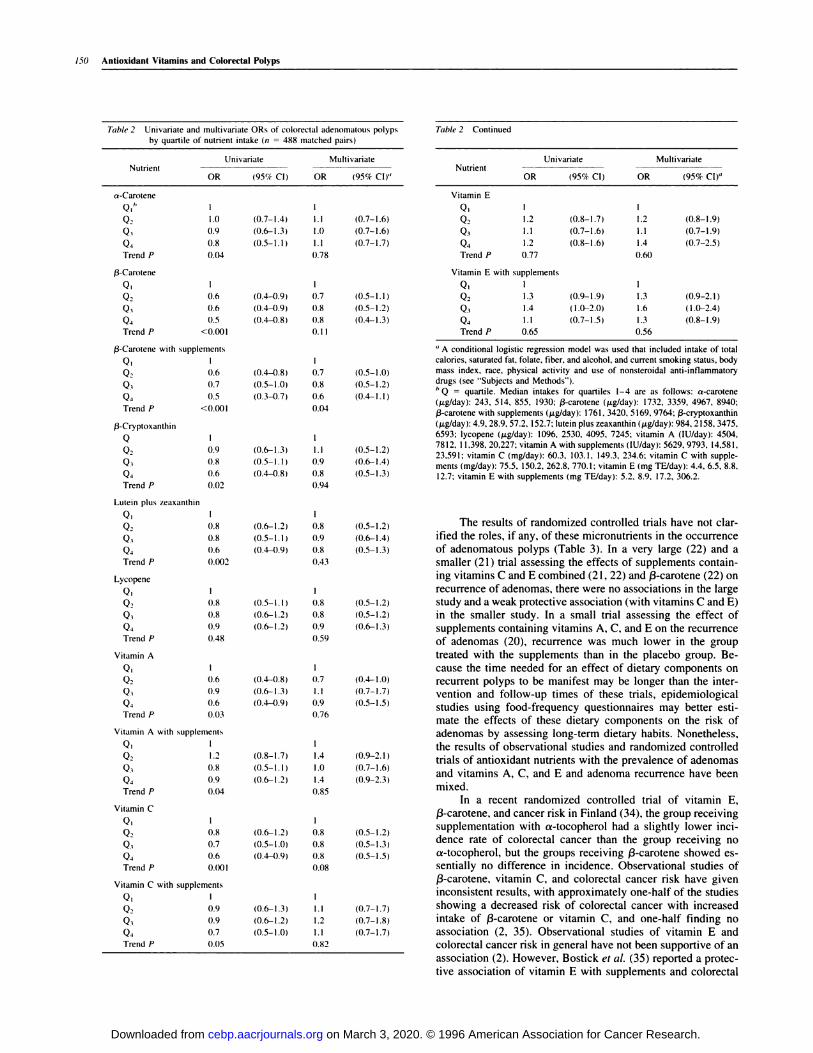
Table 2 Univariate and multivariate ORs of colorectal adenomatous polypsby quartile of nutrient intake (n = 488 matched pairs)
Univariate MultivariateNutrient
OR (95% Cl) OR (95% CI)”
Table 2 Continued
cs-Carotene
QI’,
Q2Q3Q4Trend P
/3-Carotene
QI
Q2Q3Q4Trend P
1.0
0.9
0.8
0.04
0.6
0.6
0.5
<0.001
UnivariateNutrient
OR (95% CI) OR
Multivariate
(95% CI)”
Vitamin E
Q1 I
Q2 1.2Q3 1.1
Q4 1.2
Trend P 0.77
(0.8-1.7)
(0.7-1.6)
(0.8-1.6)
I
1.2
1.1
1.4
0.60
(0.8-1.9)
(0.7-1.9)
(0.7-2.5)
Vitamin E with supplements
Q1 1
Q2 1.3
Q3 1.4
Q4 1.1
Trend P 0.65
(0.9-1.9)
(1.0-2W
(0.7-1.5)
1
1.3
1.6
1.3
0.56
(0.9-2.1)
(1.0-2.4)
(0.8-1.9)
/3-Carotene with supplements
Q1Q2 0.6
Q� 0.7
Q4 0.5
Trend P <0.001
/3-Cryptoxanthin
QQ2
Q4
Trend P
Lutein plus zeaxanthin
QI
Q2
Q4
Trend P
Lycopene
QI
Q2Q3Q4Trend P
Vitamin A
QI
Q2
Q4Trend P
0.9
0.8
0.6
0.02
0.8
0.8
0.6
0.002
0.8
0.8
0.9
0.48
0.6
0.9
0.6
0.03
(0.7-I .4)
(0.6-1.3)
(0.5-1.1)
(0.4-0.9)
(0.4-0.9)
(0.4-0.8)
(0.4-0.8)
(0.5-I .0)
(0.3-0.7)
(0.6-1.3)
(0.5-1.1)
(0.4-0.8)
(0.6-1.2)
(0.5-1.1)
(0.4-0.9)
(0.5-1.1)
(0.6- 1.2)
(0.6-1.2)
(0.4-4)8)
(0.6-I .3)
(0.4-0.9)
(0.8-I .7
(0.5-1.1)
(0.6- 1.2)
(0.6-1.2)
(0.5-1.0)
(0.4-0.9)
(0.6- 1.3)
(0.6- 1.2)
(0.5-1.0)
1.1
I .0
1.1
0.78
0.7
0.8
0.8
0. 1 1
0.7
0.8
0.6
0.04
1.1
0.9
0.8
0.94
0.8
0.9
0.8
0.43
0.8
0.8
0.9
0.59
0.7
1.1
0.9
0.76
I .4
I .0
I .4
0.85
0.8
0.8
0.8
0.08
1.1
I .2
1.1
0.82
(0.7-1.6)
(0.7-I .6)
(0.7-I .7)
(0.5-1.1)
(0.5-1.2)
(0.4-1.3)
(0.5-I .0)
(0.5-I .2)
(0.4-Il)
(0.5-1.2)
(0.6-1.4)
(0.5-1.3)
(0.5-I .2)
(0.6-1.4)
(0.5-1.3)
(0.5-1.2)
(0.5-I .2)
(0.6-I .3)
(0.4-I .0)
(0.7-I .7)
(0.5-IS)
(0.9-2.1)
(0.7-I .6)
(0.9-2.3)
(0.5-I .2)
(0.5-I .3)
(0.5-IS)
(0.7-I .7)
(0.7-I .8)
(0.7-I .7)
Vitamin A with supplements
QI 1
Q2 1.2
Q3 0.8
Q4 0.9
Trend P 0(34
(‘ A conditional logistic regression model was used that included intake of total
calories, saturated fat, folate, fiber, and alcohol, and current smoking status, body
mass index. race, physical activity and use of nonsteroidal anti-inflammatory
drugs (see “Subjects and Methods”).
h Q quartile. Median intakes for quartiles 1-4 are as follows: a-carotene
(j.cg/day): 243. 514, 855. 1930; /3-carotene (�.cg/day): 1732, 3359, 4967, 8940;
/3-carotene with supplements (�.cg/day): 1761. 3420, 5169. 9764; /3-cryptoxanthin
(�.tg/day): 4.9, 28.9, 57.2, 152.7; lutein plus zeaxanthin (pg/day): 984, 2158, 3475,
6593; lycopene (�.cg/day): 1096, 2530, 4095, 7245; vitamin A (lU/day): 4504,
7812, I 1,398, 20,227; vitamin A with supplements (lU/day): 5629, 9793, 14,581,
23,591; vitamin C (mg/day): 60.3. 103.1, 149.3. 234.6; vitamin C with supple-
ments (mg/day): 75.5, 150.2. 262.8, 770.1; vitamin E (mg TE/day): 4.4, 6.5, 8.8,
12.7; vitamin E with supplements (mg TE/day): 5.2. 8.9. 17.2, 306.2.
The results of randomized controlled trials have not clar-
ified the roles, if any, of these micronutrients in the occurrenceof adenomatous polyps (Table 3). In a very large (22) and asmaller (2 1 ) trial assessing the effects of supplements contain-ing vitamins C and E combined (21, 22) and 13-carotene (22) on
recurrence of adenomas, there were no associations in the largestudy and a weak protective association (with vitamins C and E)in the smaller study. In a small trial assessing the effect of
supplements containing vitamins A, C, and E on the recurrenceof adenomas (20), recurrence was much lower in the grouptreated with the supplements than in the placebo group. Be-
cause the time needed for an effect of dietary components onrecurrent polyps to be manifest may be longer than the inter-vention and follow-up times of these trials, epidemiologicalstudies using food-frequency questionnaires may better esti-
mate the effects of these dietary components on the risk ofadenomas by assessing long-term dietary habits. Nonetheless,the results of observational studies and randomized controlledtrials of antioxidant nutrients with the prevalence of adenomas
and vitamins A, C, and E and adenoma recurrence have beenmixed.
In a recent randomized controlled trial of vitamin E,13-carotene, and cancer risk in Finland (34), the group receivingsupplementation with a-tocopherol had a slightly lower mci-dence rate of colorectal cancer than the group receiving noa-tocopherol, but the groups receiving 13-carotene showed es-sentially no difference in incidence. Observational studies of13-carotene, vitamin C, and colorectal cancer risk have giveninconsistent results, with approximately one-half of the studiesshowing a decreased risk of coborectal cancer with increasedintake of 13-carotene or vitamin C, and one-half finding noassociation (2, 35). Observational studies of vitamin E and
colorectal cancer risk in general have not been supportive of an
association (2). However, Bostick et al. (35) reported a protec-tive association of vitamin E with supplements and coborectal
Vitamin C
QI
Q2Q3Q4Trend P
0.8
0.7
0.6
0(8)1
Vitamin C with supplements
QI
Q2Q3Q4Trend P
0.9
0.9
0.7
0.05
150 Antioxidant Vitamins and Colorectal Polyps
on March 3, 2020. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 151
Table 3 A summary of results from observational studies and randomized controlled trials that evaluated the associations of carotenoid or vitamins A, C, or E intake
and the risk of polyps
Study (ref.)Controls or no. in
Design” Cases” Cohort’ Nutrient Results
Giovannucci et a!.. 1993 (17) Nested C-C 331 9,490” /3-Carotene
Vitamin A
Vitamin C
Vitamin E
Inverse association for men (OR not given)
OR� = 0.9 1, CI 0.69- I . I 9
OR = 1.12, CI = 0.88-1.43
OR = 1.07, CI 0.84-1.36
Little et ill., 1993 ( 18) C-C 147 I53� Carotene
Vitamin A
Vitamin C
Vitamin E
No association
No association
No association
No association
Hoff ci al.. 1986 (5) C-C 78 77 Vitamin C Inverse association (P = 0.05, OR not given
Benito ci al.. 993 (7) C-C 101 242 Carotene
Vitamin A
Vitamin C
Vitamin E
OR 0.45, trend P < 0.05
OR = 0.52, trend P = ns5
OR = 0.37, trend P < 0.01
OR 0.53, trend P < 0.05
Neugut et a!.. 1993 (8) C-C 286 480 Carotene
Vitamin A
Vitamin C
No association
OR = 0.4, CI = 0.2-0.9 (women)
No association
Olsen et al.. 1994 (19) C-C 172 362 Vitamin A
Vitamin C
Vitamin E
OR 0.65, CI 0.4-1.1
OR = 0.86, CI = 0.5-1.4
OR = 0.48, CI 0.3-0.8
Kune el al. 1991 (6) C-C 49 727 Vitamin C OR 0.61. CI 0.27-1.36
Macquart-Moulin ci a!.
1987 (16)
C-C 185 238 Vitamin A
Vitamin C
Vitamin E
OR 1.52, trend P NS5
OR = 0.83, trend P NS
OR = 0.77, trend P = NS
Greenberg et a!.. 1994 (22) RCT 245 864 /3-Carotene
Vitamins C and E
OR = 1.01, CI = 0.85-1.20
OR = 1.08, CI 0.9 1-1.29
McKeown-Eyssen ci al.,
1988 (21)
RCT 63 185 Vitamins C and E OR 0.86. CI 0.5 1-1.45
Roncucci et al., 1993 (20) RCT 41 209 Vitamins A, C, and E 5.7% recurrence in treatment group compared to
35.9% in control group (P < 0.001)
“ Study design: C-C, case-control study; RCT, randomized controlled trial.F, For randomized controlled trials, number given is number with recurrent polyps.
‘. For randomized controlled trials, number given is total number in trial.
,1 The number of cases and cohort members shown are for males participating in the Health Professionals Follow-up Study; the paper also reported results for 564 femalecolorectal cancer cases among 15.984 women participating in the Nurses’ Health Study; the results are for all male and female subjects combined for the distal colon and
rectum.
� All ORs compare highest to lowest intake groups.I The number of controls shown are for fecal occult blood-negative controls; the paper also reported results for 176 fecal occult blood-positive controls.5. NS, not significant at an a level of 0.05.
cancer in their large cohort study of females, similar to theassociation of vitamin E intake in females only in this study. In
addition, in an analysis of pooled data from five cohort studies,Longnecker et a!. (36) reported a modest protective associationof serum a-tocopherol with risk of colorectal cancer.
In patients with coborectal adenomas, Cahill er a!. (37)demonstrated that dietary vitamin C supplements resulted in
decreased proliferation of cells throughout the crypt, and di-etary (3-carotene supplements resulted in decreased prolifera-
tion of cells in the base of the crypt. Dietary vitamin E sup-
plements had no effect on cell proliferation. Paganelli et a!. (38)found that dietary supplements of vitamins A, C, and E com-bined resulted in decreased rectal cell proliferation in the upperportion of the crypt in patients with colorectal adenomas. De-creasing proliferation of rectal crypt cells is a potential mech-
anism by which 13-carotene and vitamin C might reduce risk of
adenomas.The carotenoids and vitamins C and E have antioxidant
and other properties that may prevent polyps or cancer. Theprovitamin A carotenoids can be cleaved in the body to formvitamin A, a nutrient essential to cellular differentiation (39).
Carotenoids and vitamins C and E scavenge free radicals andinhibit lipid peroxidation (9, 39). The carotenoids and vitaminC also have immune-enhancing properties (9, 39, 40), andvitamins C and E can prevent the formation of carcinogenicagents from precursor compounds (9).
We observed interaction on the multiplicative scale of
gender and intakes of 13-cryptoxanthin and vitamin E withcoborectal adenomas. The inverse associations of 13-cryptoxan-thin and vitamin E with adenomas were observed only infemales. Although it is possible that there may be a real genderdifference, the results may also be due to chance. Therefore, theimportance of these findings will depend on their reproducibil-ity in other populations.
Certain limitations of this study may restrict our ability tomake inferences about colon and rectal polyp etiology. Mis-
on March 3, 2020. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

152 AntIoxidant Vitamins and Colorectal Polyps
classification of diet due to the use of a food-frequency ques-
tionnaire is a potentially important limitation. A concern withuse of the questionnaire is that it has been shown to overesti-mate intake of some foods considered healthful, such as certain
fruits and vegetables (41). However, Salvini et a!. (41) andFeskanich et a!. (42) demonstrated that the ranking of individ-uals by food intake, as assessed by the Willett questionnaire,was reasonably valid and reproducible. Another potentialsource of error related to the estimation of diet is the specific
carotenoid database published by Mangels et al. (10). Foodcarotenoid values were determined from existing informationon the carotenoid content of foods, as determined by variousresearch groups using different analytic techniques. The differ-ent techniques varied widely in quality, and the number ofsamples tested for each food item also varied. In addition, thecarotenoid content of fruits and vegetables often varies by
geographical region. Errors in the estimation of the carotenoidcontent of food items would likely result in an underestimationof an effect of carotenoids on the prevalence of adenomas.Despite these shortcomings, however, the estimates of specificcarotenoid intake using this carotenoid database were found to
be reasonably valid in this population (43), as well as in otherstudy populations using a similar food-frequency questionnaire
(44, 45).Because this is a sigmoidoscopy-based study, we were
able to evaluate only left-sided adenomas. If the data wereinterpreted as also applicable to risk of polyps of the entire largebowel, the results would likely be biased toward the null be-cause of nondifferential misclassification of disease status incontrols. Because the participants were informed of their polypstatus before completing the interview and dietary question-
naires, we cannot be certain that the diagnosis did not affecttheir responses. The possibility exists that gastrointestinalsymptoms may have prompted changes in the diets of some
subjects, but the proportion of symptomatic subjects was ap-proximately the same for both the case and control groups.Unlike many previous studies of diet and polyps, only subjectswith minor or no symptoms were eligible for the study, and all
of the subjects in this study had been examined for polyps usingan endoscopic procedure. Because the prevalence of adenomasin this age group is likely to be high (46), using screenedcontrols reduced the likelihood of misclassification. Becausethis study included prevalent rather than incident polyps, it is
not possible to discriminate between factors affecting the riskand the duration of polyps. However, determining factors thataffect duration may also be important, because larger polyps,and thus polyps of longer duration, may be more likely to
undergo malignant transformation (24, 46). In addition, theresponse rates were high for both the case and control groups.
With nearly 500 case-control pairs this is among the largeststudies of risk factors for colorectal polyps to date.
Overall, the data in epidemiological studies are mixedregarding the relationship of 13-carotene with occurrence ofadenomatous polyps of the large bowel. These results provideweak support for the hypothesis that 13-carotene protects againstthe occurrence of coborectal polyps. Although high intakes ofvitamin C also appeared to confer protection against colorectalpolyps, the effects may be due to other components of fruits andvegetables.
References
I . Steinmetz. K. A.. and Potter. J. D. Vegetables, fruit. and cancer. I. Epidemi-
ology. Cancer Causes & Control, 2: 325-357, 1991.
2. Potter. J. D., Slattery. M. L.. Bostick. R. M.. and Gapstur. S. M. Colon cancer:a review of the epidemiology. Epidemiol. Rev.. /5: 499-545. 1993.
3. Steinmetz, K. A., Kushi. L. H., Bostick. R. M.. Folsom, A. R., and Potter, J.D. Vegetables, fruit, and colon cancer in the Iowa Women’s Health Study. Am.
J. Epidemiol.. 139: 1-15, 1994.
4. Kono. S.. Shinchi, K., Ikeda. N.. Yanai. F.. and Imanishi, K. Physical activity.
dietary habits. and adenomatous polyps of the sigmoid colon: a study of self-
defense officials in Japan. J. Clin. Epidemiol., 44: 1255-1261, 1991.
5. Hoff, G., Moen, I. E., Trygg, K., Frolich. W.. Sauar, J.. Vatn, M., Gjone, E.,
and Larsen, S. Epidemiology of polyps in the rectum and sigmoid colon: eval-
uation of nutritional factors. Scand. J. Gastroenterol.. 21: 199-204, 1986.
6. Kune, G. A.. Kune, S., Read. A., MacGowan, K., Penfold, C., and Watson, L.
F. Colorectal polyps. diet. alcohol. and family history of colorectal cancer: a
case-control study. Nutr. Cancer, /6: 25-30. 1991.
7. Benito, E., Cabeza, E., Moreno, V., Obrador, A., and Bosch, F. X. Diet andcolorectal adenomas: a case-control study in Majorca. Int. J. Cancer. 55: 2 13-2 19.
1993.
8. Neugut. A. I., Garbowski, G. C., Lee. W. C., Murray. T.. Nieves, J. W., Forde,
K. A.. Treat, M. R., Waye, J. D.. and Fenoglio-Preiser, C. Dietary risk factors forthe incidence and recurrence of colorectal adenomatous polyps: a case-control
study. Ann. Intern. Med., 118: 91-95. 1993.
9. Steinmetz, K. A., and Potter. J. D. Vegetables, fruit, and cancer. II. Mecha-
nisms. Cancer Causes & Control, 2: 427-442, 1991.
10. Mangels, A. R., Holden. J. M., Beecher, 0. R.. Forman. M. R.. and Lanza.E. Carotenoid content of fruits and vegetables: an evaluation of analytic data.
J. Am. Diet Assoc., 93: 284-296, 1993.
I I . Block. G. Nutrient sources of provitamin A carotenoids in American diet.Am. J. Epidemiol., 139: 290-293, 1994.
12. Murphy, S. P., Subar, A. F., and Block. G. Vitamin E intakes and sources inthe United States. Am. J. Clin. Nutr., 52: 361-367, 1990.
13. Olson. J. A. Needs and sources ofcarotenoids and vitamin A. Nutr. Rev.. 52:
S67-S73. 1994.
14. Ross, A. C.. and Temus. M. E. Vitamin A as a hormone: recent advances inunderstanding the actions of retinol. retinoic acid. and /3 carotene. J. Am. Diet
Assoc., 93: 1285-1290, 1993.
15. Hill, D. L.. and Grubbs, C. J. Retinoids and cancer prevention. Annu. Rev.
Nutr.. 12: 161-181, 1992.
16. Macquart-Moulin, G., Riboli, E., Comee, J., Kaaks, R., and Berthezene, P.
Colorectal polyps and diet: a case-control study in Marseilles. Int. J. Cancer, 40:
179-188, 1987.
17. Giovannucci, E.. Stampfer. M. J.. Colditz, G.. Rimm, E. B., Trichopoulos. D..
Rosner. B. A.. Speizer. F. E., and Willett. W. C. Folate, methionine, and alcohol
intake and risk of colorectal adenoma. J. Natl. Cancer Inst.. 85: 875-884, 1993.
18. Little. i. Logan. R. F. A.. Hawtin, P. G., Hardcastle. J. D., and Turner, I. D.
Colorectal adenomas and diet: a case-control study of subjects participating in the
Nottingham faecal occult blood screening programme. Br. J. Cancer, 67:
177-184, 1993.
19. Olsen, J.. Kronborg, 0.. Lynggaard, J.. and Ewertz. M. Dietary risk factorsfor cancer and adenomas of the large intestine: a case-control study within a
screening trial in Denmark. Eur. J. Cancer, 30,4: 53-60, 1994.
20. Roncucci, L., Di Donato, P., Carati, L.. Ferrari, A., Perini. M.. Bertoni, G.,
Bedogni, G., Paris, B., Svanoni. F., Girola. M., and Ponz de Leon, M. Antioxidantvitamins or lactulose for the prevention of the recurrence of colorectal adenomas.
Dis. Colon Rectum, 36: 227-234, 1993.
21 . McKeown-Eyssen. 0., Holloway, C., Jazmaji. V.. Bright-See. E.. Dion. P.,
and Bruce, W. R. A randomized trial of vitamins C and E in the prevention of
recurrence of colorectal polyps. Cancer Res., 48: 4701-4705, 1988.
22. Greenberg. E. R., Baron, J. A., Tosteson, T. D., Freeman, D. H., Jr., Beck, G.
J.. Bond, J. H.. Colacchio. T. A., Coller, J. A., Frankl, H. D.. Haile, R. W.,Mandel, J. S.. Nierenberg. D. W., Rothstein. R., Snover, D. C.. Stevens, M. M.,Summers, R. W.. and van Stolk. R. U. for the Polyp Prevention Study Group. Aclinical trial of antioxidant vitamins to prevent colorectal adenoma. N. EngI. J.
Med., 33!: 141-147, 1994.
23. Le Marchand, L., Hankin, J. H., Kolonel, L. N.. Beecher, G. R., Wilkens, L.
R.. and Thao, L. P. Intake of specific carotenoids and lung cancer risk. CancerEpidemiol., Biomarkers & Prey.. 2: 183-187. 1993.
24. Enterline, H. T., Evans. G. W.. Mercudo-Lugo. R.. Miller, L., and Fitis, W.
T. Malignant potential of adenomas of colon and rectum. JAMA, I 79: 322-330.
I 962.
25. Stryker, S. J.. Wolff, B. G., CuIp, C. E., Libbe, S. D., llstrup, D. M., and
MacCarty. R. L. Natural history of untreated colonic polyps. Gastroenterology,
93: 1009-1013, 1987.
26. Jass. J. R. Do all colorectal carcinomas arise in preexisting adenomas? World
J. Surg., 13: 45-51, 1989.
27. Pollock, A. M., and Quirke, P. Adenoma screening and colorectal cancer
(Letter). Br. Med. J., 303: 3-4, 1991.
on March 3, 2020. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 153
28. Editorial. Colorectal cancer: new evidence for the adenoma/carcinoma se-quence. Lancet, 340: 210-21 I, 1992.
29. Rimm, E. B., Giovannucci, E. L., Stampfer, M. J., Colditz, 0. A., Litin, L.
B., and Willett, W. C. Reproducibility and validity of an expanded self-
administered semiquantitative food frequency questionnaire among male health
professionals. Am. J. Epidemiol., 135: 1 I 14-1 126, 1992.
30. Willett, W. C. Nutritional Epidemiology. pp. 83-84. New York: Oxford
University Press, 1990.
3 1 . Machine-Readable Data Sets on Composition of Foods and Results fromFood Consumption Surveys, Human Nutrition Information Service Administra-
tive Report No. 378. pp. 32. Hyattsville, MD: United States Department of
Agriculture Nutrition Monitoring Division, Survey Statistics Branch, 1991.
32. Schakel, S. F., Sievert, Y. A., and Buzzard, I. M. Sources of data fordeveloping and maintaining a nutrient database. J. Am. Diet Assoc., 88:
1268-1271, 1988.
33. Giovannucci, E., Stampfer, M. J., Colditz, G., Rimm, E. B., and Willeu, W.
C. Relationship of diet to risk of colorectal adenoma in men. J. Nail. Cancer Inst.,84: 91-98, 1992.
34. The Alpha Tocopherol. Beta Carotene Cancer Prevention Study Group. Theeffect of vitamin E and beta carotene on the incidence of lung cancer and other
cancers in male smokers. N. EngI. J. Med., 330: 1029-1035, 1994.
35. Bostick, R. M., Potter, J. D., McKenzie, D. R., Sellers, T. A., Kushi, L. H.,
Steinmetz, K. A., and Folsom, A. R. Reduced risk of colon cancer with high
intake of vitamin E: The Iowa Women’s Health Study. Cancer Res., 53:4230-4237. 1993.
36. Longnecker, M. P., Martin-Moreno, J. M., Knekt, P., Nomura, A. M. Y.,Schober, S. E., Stahelin, H. B., Wald, N. J., Gey, K. F., and Willett, W. C. Serum
a-tocopherol concentration in relation to subsequent colorectal cancer: pooled
data from five cohorts. J. NatI. Cancer Inst., 84: 430-435, 1992.
37. Cahill, R. J., O’Sullivan, K. R., Mathias, P. M., Beauie, S., Hamilton, H., and
O’Morain, C. Effects of vitamin antioxidant supplementation on cell kinetics ofpatients with adenomatous polyps. Gut, 34: 963-967, 1993.
38. Paganelli, G. M., Biasco, 0., Brand), G., Santucci, R., Gizzi, G., Villani. V.,Cianci, M., Miglioli, M., and Barbara, L. Effect of vitamin A, C, and E supple-mentation on rectal cell proliferation in patients with colorectal adenomas. J. Natl.
Cancer Inst., 84: 47-51. 1992.
39. Byers, T., and Perry, G. Dietary carotenes, vitamin C, and vitamin E as
protective antioxidants in human cancers. Annu. Rev. Nutr., 12: 139-159, 1992.
40. Bendich, A. Carotenoids and the immune response. J. Nutr., 119: 1 12-1 15,
1989.
41. Salvini, S., Hunter, D. J., Sampson, L.. Stampfer. M. J., Colditz, G. A.,Rosner, B., and Willen, W. C. Food-based validation of a dietary questionnaire:the effects of week-to-week variation in food composition. Int. J. Epidemiol., 18:858-867, 1989.
42. Feskanich, D., Rimm, E. B., Giovannucci. E. L., Colditz, G. A., Stampfer, M.
J., Litin, L. B., and Willett, W. C. Reproducibility and validity of food intake
measurements from a semiquantitative food frequency questionnaire. J. Am. DietAssoc., 93: 790-796, 1993.
43. Enger, S. M., Longnecker, M. P., Shikany. J. M., Swendseid, M. E., Chen, M.
J., Harper, J. M., and Haile, R. W. Questionnaire assessment of intake of specificcarotenoids. Cancer Epidemiol., Biomarkers & Prey., 4: 201-205, 1995.
44. Forman, M. R., Lanza, E., Yong, L-C.. Holden, J. M., Graubard, B. I.,Beecher, G. R., Melitz, M., Brown, E. D., and Smith, J. C. The correlation
between two dietary assessments of carotenoid intake and plasma carotenoid
concentrations: application of a carotenoid food-composition database. Am. J.
Clin. Nutr., 58: 519-524, 1993.
45. Yong, L-C., Forman, M. R., Beecher, G. R., Graubard, B. I., Campbell, W.
S., Reichman, M. E., Taylor, P. R., Lanza, E., Holden, J. M., and Judd, J. 1.Relationship between dietary intake and plasma concentrations of carotenoidsin premenopausal women: application of the USDA-NCI carotenoid food-
composition database. Am. J. Clin. Nutr., 60: 223-230, 1994.
46. Hoff, G. Colorectal polyps. Clinical implications: screening and cancer
prevention. Scand. J. Gastroenterol., 22: 769-775, 1987.
on March 3, 2020. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
1996;5:147-153. Cancer Epidemiol Biomarkers Prev S M Enger, M P Longnecker, M J Chen, et al. and prevalence of colorectal adenomas.Dietary intake of specific carotenoids and vitamins A, C, and E,
Updated version
http://cebp.aacrjournals.org/content/5/3/147
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/5/3/147To request permission to re-use all or part of this article, use this link
on March 3, 2020. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from