different impact of changes in left ventricular ejection
TRANSCRIPT

Circulation Journal Vol.83, March 2019
584 YAMAMOTO M et al.Circulation JournalCirc J 2019; 83: 584 – 594doi: 10.1253/circj.CJ-18-0881
gression or with treatment. Improvement in LVEF with β-blocker treatment was associated with a better prognosis in a HFrEF cohort,9 and recent studies reported that patients with HFrEF and improved LVEF had a differ-ent clinical course compared with patients with HFpEF and HFrEF in whom reduced LVEF was persistent.10,11 Therefore, the change in LVEF, rather than a one-off measurement, may provide more important information for assessment of clinical outcomes in patients with HF. However, there have been no prospective observational studies regarding changes in LVEF over the clinical course, including the acute phase. Therefore, the optimal timing of LVEF measurement to determine the HF type has not been clarified because LVEF measurements are not performed
C lassification of heart failure (HF) is based on the left ventricular ejection fraction (LVEF) and includes HF with preserved ejection fraction
(HFpEF) and HF with reduced ejection fraction (HFrEF). In addition, HF with mid-range ejection fraction (HFm-rEF) has been proposed in the European Society of Cardi-ology guidelines as a novel classification when the LVEF falls between HFrEF and HFpEF.1–4 As previous studies have reported that there are no significant differences in prognosis between HFpEF and HFrEF, LVEF itself may have lost clinical value as an absolute predictor for risk in patients with HF, and may be a landmark for classifying the type of HF.5–8
In contrast, the LVEF can be changed by disease pro-
Received August 2, 2018; revised manuscript received November 11, 2018; accepted December 5, 2018; J-STAGE Advance Publication released online January 23, 2019 Time for primary review: 33 days
Department of Cardiology, Faculty of Medicine (M.Y., Y.S., T.I., T.M.-O., K.S., T.N., K.A., M.I.), Department of Cardiology, Graduate School of Comprehensive Human Sciences (Y.H.-H., S.S.), University of Tsukuba, Tsukuba; Department of Cardiology, Tsuchiura Clinical Education and Training Center, Tsuchiura (I.N.); Cardiovascular Center, Tsuchiura Kyodo Hospital, Tsuchiura (A.S.); Department of Cardiology, Ibaraki Prefectural Central Hospital, Kasama (M.B.); and Division of Cardiology, Ryugasaki Saiseikai General Hospital, Ryugasaki (K.O.), Japan
Mailing address: Yoshihiro Seo, MD, PhD, Department of Cardiology, Faculty of Clinical Medicine, University of Tsukuba, 1-1-1 Tennodai, Tsukuba 305-8575, Japan. E-mail: [email protected]
ISSN-1346-9843 All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected]
Different Impact of Changes in Left Ventricular Ejection Fraction Between Heart Failure Classifications in
Patients With Acute Decompensated Heart Failure
Masayoshi Yamamoto, MD, PhD; Yoshihiro Seo, MD, PhD; Tomoko Ishizu, MD, PhD; Isao Nishi, MD, PhD; Yoshie Hamada-Harimura, MD; Tomoko Machino-Ohtsuka, MD, PhD;
Kimi Sato, MD, PhD; Seika Sai, MD; Tomofumi Nakatsukasa, MD; Akinori Sugano, MD, PhD; Masako Baba, MD; Kenichi Obara, MD; Kazutaka Aonuma, MD, PhD; Masaki Ieda, MD, PhD
Background: Left ventricular ejection fraction (LVEF) can dramatically change when the patient has acute decompensated heart failure (ADHF). We investigated the impact of LVEF and subsequent changes on prognosis in patients with ADHF through a prospec-tive study.
Methods and Results: A total of 516 hospitalized patients with ADHF were evaluated. Echocardiography was performed on admis-sion, prior to discharge, and 1 year after discharge. The primary endpoint was a composite of cardiovascular death and hospitaliza-tion. In heart failure with reduced EF (HFrEF; LVEF <40%), LVEF did not significantly improve during hospitalization (P=0.348); however, it improved after discharge (P<0.001). In contrast, LVEF improved during hospitalization (P<0.001) in HF with preserved EF (HFpEF; LVEF ≥50%). In HF with mid-range EF (HFmrEF; LVEF 40–49%), LVEF consistently improved throughout the observa-tion period (P<0.001). A multivariable Cox model showed that improved LVEF after discharge was associated with a better outcome in HFrEF (hazard ratio [HR]: 0.951; 95% confidence interval [CI]: 0.928–0.974; P<0.001), while improved LVEF during hospitalization was associated with a better outcome in HFpEF (HR: 0.969; 95% CI: 0.940–0.998; P=0.038).
Conclusions: Improved LVEF after discharge in HFrEF and during hospitalization in HFpEF was associated with a better prognosis in patients with ADHF. Longitudinal improvements in LVEF had different prognostic impact, depending on the HF type by LVEF measurement.
Key Words: Acute decompensated heart failure; Echocardiography; Ejection fraction; Prognosis
ORIGINAL ARTICLEHeart Failure

Circulation Journal Vol.83, March 2019
585Change in LVEF and Prognosis
tions were to be performed at 3 time points: on admission, prior to discharge, and at 1 year after discharge.13 The first echocardiogram was performed in the emergency depart-ment or echocardiographic laboratories before admission. Subsequent LVEF measurements were made when the patient was in a stable condition prior to discharge, and again after 1 year. A core laboratory (University of Tsukuba) was assigned to analyze the echocardiographic data without any knowledge of the clinical data. LVEF is preferentially assessed by the quantitative 2D biplane vol-umetric Simpson method from 4- and 2-chamber views. The final LVEF assessment is based on the echocardiogra-pher’s collation of multiple methods of EF measurement (quantitative 2D biplane volumetric Simpson method, M-mode or 2D echocardiography from the parasternal views, or by visual estimation). Patients were classified into 3 groups by their predischarge LVEF (HFpEF ≥50%, HFmrEF 40–49%, and HFrEF <40%). We calculated 2 types of change in LVEF: during hospitalization (LVEF at discharge – LVEF on admission), and after discharge (LVEF at 1 year – LVEF at discharge). Based on the change in LVEF in each period, patients were classified into 3 groups: worsening LVEF (decrease ≥5%), stable LVEF (change of −5 to +5%), and improving LVEF (>5% increase).
Statistical AnalysisThe results are expressed as number (%) or mean ± standard deviation, where appropriate. One-way analysis of vari-ance with the post-hoc Tukey-Kramer test was used to compare variables between the 3 groups. Categorical data were compared using chi-square or Fisher exact tests, as appropriate. To assess predictors of change in LVEF, we used univariate and multivariable linear regression models. The initial candidates for variable selection were the set of the covariates with a value of P<0.05 in the univariate linear regression analysis. Kaplan-Meier analyses were done to determine the influence of LVEF classification and change of LVEF groups on the endpoints. The risk of reaching a clinical endpoint was determined with Cox pro-
at predetermined times, and the clinical implications for assessment of changes in LVEF have not been well studied.
We hypothesized that evaluation of LVEF in patients with HF should target those who are hospitalized for acute decompensated HF (ADHF), as this condition can dra-matically change the LVEF and may provide useful infor-mation regarding the optimal timing of LVEF measurements to determine the HF type.
We focused on 2 points: (1) investigate whether there are differences in the prognostic effect of the 3 HF classifica-tions depending on when LVEF was measured, and (2) clarify whether assessing the changes in LVEF during hos-pitalization or at 1 year after discharge has clinical implica-tions beyond a one-off measurement of LVEF.
MethodsStudy Population and ProtocolThe study population was 838 patients who were hospi-talized for ADHF and enrolled in the Ibaraki Cardiac Assessment Study-Heart Failure registry, a prospective, observational, multicenter registry compiling data from 11 institutions. The registration period was June 2012 through March 2015. The diagnosis of HF was made according to the Framingham criteria.12 Patients were excluded if they were aged <20 years, did not provide informed consent, or had a limited life expectancy owing to malignant neoplasms. The primary endpoint was a composite of cardiovascular death and hospitalization, and the secondary endpoint was all-cause death. Death was considered of cardiovascular origin if it was caused by HF, sudden death, acute myocar-dial infarction, stroke, or other cardiovascular causes. The investigation conformed with the principles outlined in the Declaration of Helsinki. The institutional ethical commit-tee approved the protocol. Written informed consent was provided by all patients before enrolment.
Echocardiographic StudyStandard 2D transthoracic echocardiographic examina-
Figure 1. Flowchart of the study of changes in left ventricular ejection fraction in patients with acute decompensated heart failure.
Circulation Journal Vol.83, March 2019
586 YAMAMOTO M et al.
ResultsBaseline CharacteristicsAmong the 838 patients identified in the database, 81 were excluded: 13 patients had undergone hemodialysis, 40 patients did not have an echocardiogram predischarge, and 28 died while in the hospital. Therefore, the analysis included 757 patients (Figure 1). The median follow-up
portional hazard models with adjustment for age and sex. The univariate factors with a value of P<0.05 were entered into the multivariable model to assess the effect of the param-eters on the endpoints. A P-value <0.05 was considered to indicate statistical significance. All analyses were performed with SPSS version 24 (SPSS Inc., Chicago, IL, USA).
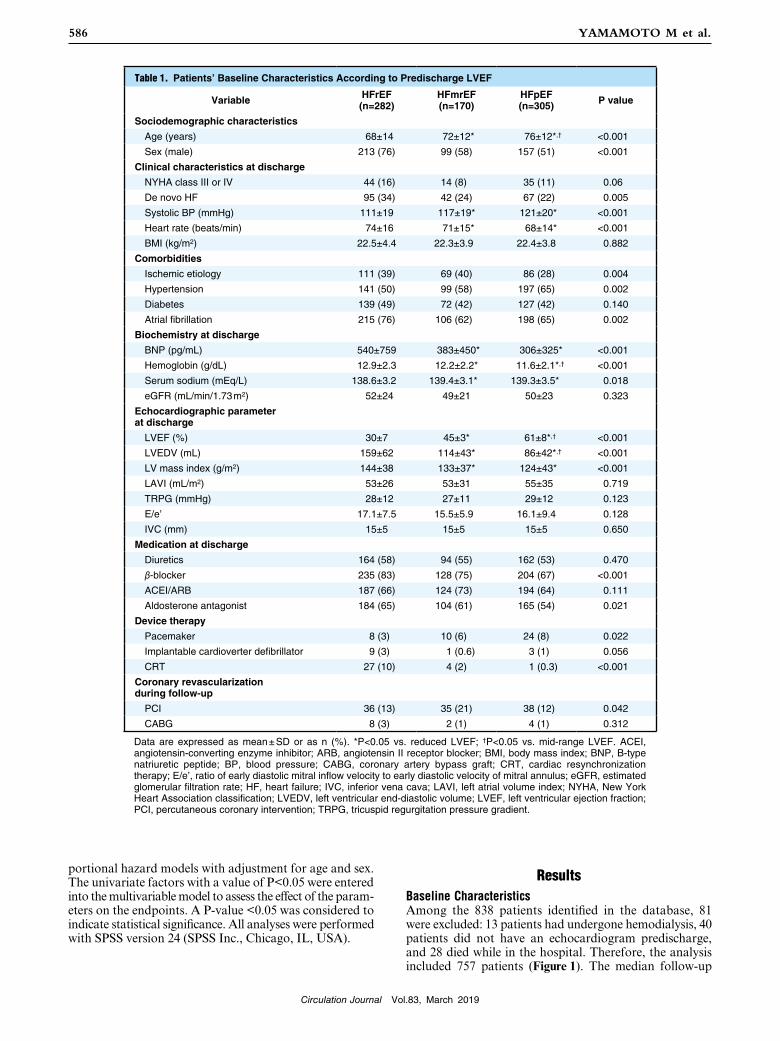
Table 1. Patients’ Baseline Characteristics According to Predischarge LVEF
Variable HFrEF (n=282)
HFmrEF (n=170)
HFpEF (n=305) P value
Sociodemographic characteristics
Age (years) 68±14 72±12* 76±12*,† <0.001 Sex (male) 213 (76) 99 (58) 157 (51) <0.001 Clinical characteristics at discharge
NYHA class III or IV 44 (16) 14 (8) 35 (11) 0.06 De novo HF 95 (34) 42 (24) 67 (22) 0.005
Systolic BP (mmHg) 111±19 117±19* 121±20* <0.001 Heart rate (beats/min) 74±16 71±15* 68±14* <0.001 BMI (kg/m2) 22.5±4.4 22.3±3.9 22.4±3.8 0.882
Comorbidities
Ischemic etiology 111 (39) 69 (40) 86 (28) 0.004
Hypertension 141 (50) 99 (58) 197 (65) 0.002
Diabetes 139 (49) 72 (42) 127 (42) 0.140
Atrial fibrillation 215 (76) 106 (62) 198 (65) 0.002
Biochemistry at discharge
BNP (pg/mL) 540±759 383±450* 306±325* <0.001 Hemoglobin (g/dL) 12.9±2.3 12.2±2.2* 11.6±2.1*,† <0.001 Serum sodium (mEq/L) 138.6±3.2 139.4±3.1* 139.3±3.5* 0.018
eGFR (mL/min/1.73 m2) 52±24 49±21 50±23 0.323
Echocardiographic parameter at discharge
LVEF (%) 30±7 45±3* 61±8*,† <0.001 LVEDV (mL) 159±62 114±43* 86±42*,† <0.001 LV mass index (g/m2) 144±38 133±37* 124±43* <0.001 LAVI (mL/m2) 53±26 53±31 55±35 0.719
TRPG (mmHg) 28±12 27±11 29±12 0.123
E/e’ 17.1±7.5 15.5±5.9 16.1±9.4 0.128
IVC (mm) 15±5 15±5 15±5 0.650
Medication at discharge
Diuretics 164 (58) 94 (55) 162 (53) 0.470
β-blocker 235 (83) 128 (75) 204 (67) <0.001 ACEI/ARB 187 (66) 124 (73) 194 (64) 0.111
Aldosterone antagonist 184 (65) 104 (61) 165 (54) 0.021
Device therapy
Pacemaker 8 (3) 10 (6) 24 (8) 0.022
Implantable cardioverter defibrillator 9 (3) 1 (0.6) 3 (1) 0.056
CRT 27 (10) 4 (2) 1 (0.3) <0.001 Coronary revascularization during follow-up
PCI 36 (13) 35 (21) 38 (12) 0.042
CABG 8 (3) 2 (1) 4 (1) 0.312
Data are expressed as mean ± SD or as n (%). *P<0.05 vs. reduced LVEF; †P<0.05 vs. mid-range LVEF. ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BMI, body mass index; BNP, B-type natriuretic peptide; BP, blood pressure; CABG, coronary artery bypass graft; CRT, cardiac resynchronization therapy; E/e’, ratio of early diastolic mitral inflow velocity to early diastolic velocity of mitral annulus; eGFR, estimated glomerular filtration rate; HF, heart failure; IVC, inferior vena cava; LAVI, left atrial volume index; NYHA, New York Heart Association classification; LVEDV, left ventricular end-diastolic volume; LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention; TRPG, tricuspid regurgitation pressure gradient.

Circulation Journal Vol.83, March 2019
587Change in LVEF and Prognosis
charge are summarized in Figure 2, as well as the classifica-tion by LVEF on admission. The rates for the composite endpoint (P=0.518) and all-cause death (P=0.524) did not differ among the 3 groups (Figure 2C,D).
Longitudinal Change in LVEFAmong the 757 patients evaluated, 68 (9.0%) died before the 1-year follow-up, and 173 (22.9%) did not undergo echocardiography within the defined period. Therefore, 516 patients were included in the longitudinal analysis of change in LVEF. Among these 516 patients, worsening LVEF occurred in 70 patients (13.6%), 183 patients had stable LVEF (35.4%), and 263 patients showed improve-ment in LVEF (51.0%). The baseline characteristics of each group are summarized in Table 2. The improving LVEF group consisted of the youngest subjects and had the high-est prevalence of new-onset HF, the highest heart rate, estimated glomerular filtration rate (eGFR), and hemoglo-bin, the lowest LVEF predischarge, and the lowest preva-lence of ischemic etiology, pacemaker and implantable cardioverter defibrillator implantation. There were no dif-ferences in the use of loop diuretics, renin-angiotensin system inhibitors, β-blockers, or aldosterone antagonists across the groups.
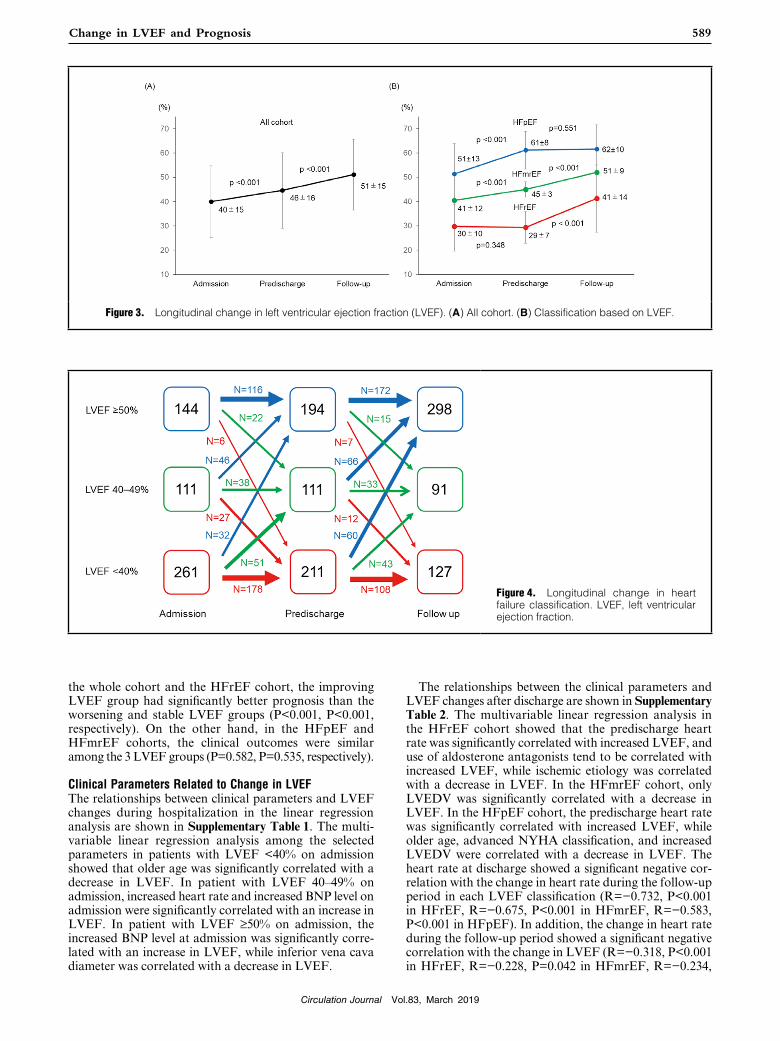
The longitudinal change in LVEF is shown in Figure 3. In all cohorts, LVEF consistently improved throughout the observation period (P<0.001) (Figure 3A). Figure 3B shows the sequential changes in LVEF in the 3 groups clas-sified by LVEF. In patients with HFrEF, LVEF did not significantly improve during hospitalization (P=0.348), but did improve after discharge (P<0.001). In contrast, LVEF improved during hospitalization (P<0.001), but did not change after discharge (P=0.551) in patients with HFpEF. In patients with HFmrEF, LVEF consistently improved throughout the observation period (P<0.001).
period was 534±309 days, and the maximum follow-up was 1,244 days. During follow-up, there were 126 (16.6%) deaths and 249 (32.9%) cardiovascular deaths or hospital-ization events. Patients were initially divided into HFrEF (n=282, 37.3%), HFmrEF (n=170, 22.5%), and HFpEF (n=305, 40.2%) based on the predischarge LVEF measure-ment. The baseline characteristics of the study groups clas-sified by predischarge LVEF are summarized in Table 1. Notably, the patients with HFpEF were older and predom-inantly women. Similarly, serum B-type natriuretic peptide (BNP) level was highest, and LV end-diastolic volume (LVEDV) was largest in the HFrEF group. The use of loop diuretics and renin-angiotensin system inhibitors was similar among the 3 groups, but the use of β-blockers and aldosterone antagonists was more frequent in the HFrEF group compared with HFmrEF and HFpEF. Regarding nonpharmacologic treatment, cardiac resynchronization therapy (CRT) was performed most frequently in HFrEF patients, whereas pacemaker implantation was performed most frequently in those with HFpEF. Percutaneous coro-nary intervention during follow-up was performed most frequently in the HFmrEF group.
Impact of LVEF on Admission and Predischarge on PrognosisIn the analysis of echocardiograms obtained on admission, 22 of the 757 patients (2.9%) were excluded because of inad-equate image quality, and of the remaining 735 patients, whose average LVEF was 41±15%, 354 had HFrEF (48.1%), 171 had HFmrEF (23.3%), and 210 had HFpEF (28.6%). Kaplan-Meier estimates of the time-to-endpoint based on the classification of LVEF on admission are shown in Figure 2; the rates for the composite endpoint (P=0.455) and all-cause death (P=0.672) were similar among the 3 groups (Figure 2A,B). Analyses based on LVEF predis-
Figure 2. Kaplan-Meier survival curves based on the left ventricular ejection fraction (LVEF) on admission and predischarge. (A) Composite endpoint (LVEF on admission). (B) All-cause death (LVEF on admission). (C) Composite endpoint (LVEF pre-discharge). (D) All-cause death (LVEF predischarge).

Circulation Journal Vol.83, March 2019
588 YAMAMOTO M et al.
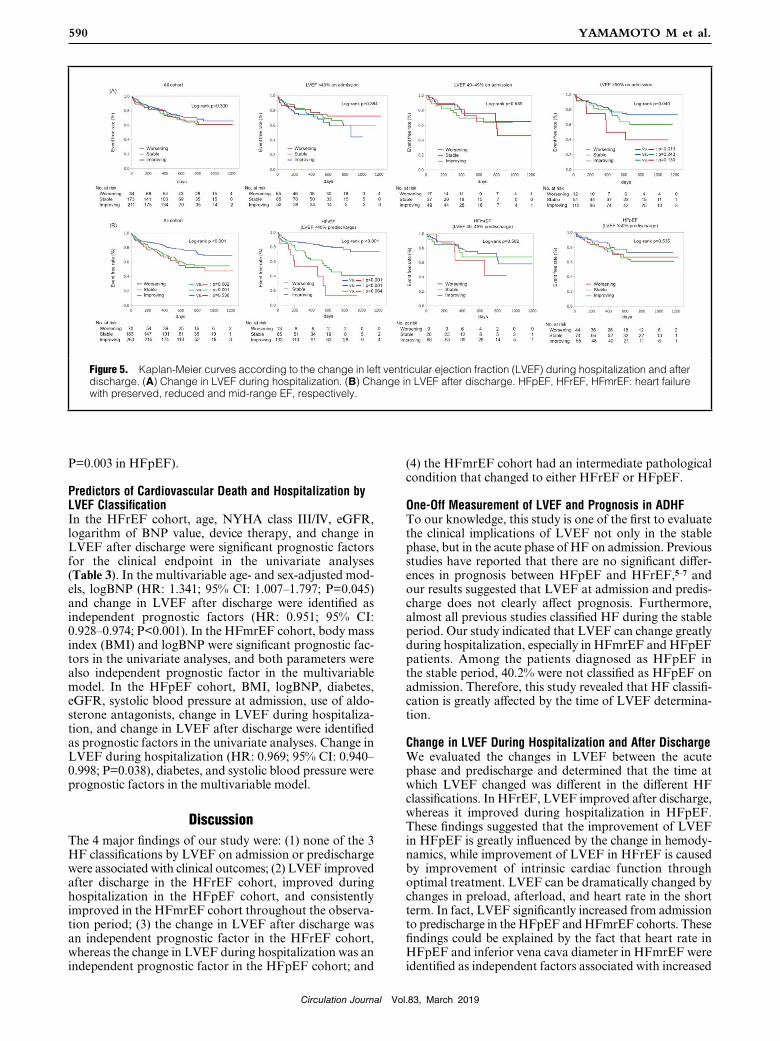
Change in LVEF and Clinical OutcomeKaplan-Meier estimates of the time-to-endpoint per the change in LVEF during hospitalization are shown in Figure 5A. In patient with LVEF <40% or 40–49% on admission, the clinical outcomes did not differ among the 3 LVEF groups (P=0.384, P=0.589, respectively). In patient with LVEF ≥50% on admission, the improving LVEF group had significantly better prognosis than the worsen-ing LVEF group (P=0.040).
Kaplan-Meier estimates of the time-to-endpoint per the change in LVEF after discharge are shown in Figure 5B. In
As illustrated in Figure 4, based on the predischarge LVEF, among 211 of the patients in the HFrEF group, 108 (51.2%) remained as HFrEF, and 43 (20.4%) and 60 (28.4%) changed to HFmrEF and HFpEF, respectively. Among 111 patients in the HFmrEF group, 33 (29.7%) remained as HFmrEF, and 12 (10.8%) and 66 (59.5%) changed to HFrEF and HFpEF, respectively. Among 194 patients in the HFpEF group, 172 (88.7%) remained as HFpEF, and 7 (3.6%) and 15 (7.7%) changed to HFmrEF and HFrEF, respectively.
Table 2. Patients’ Characteristics According to Change in LVEF After Discharge
Variable Worsening LVEF (n=70)
Stable LVEF (n=183)
Improving LVEF (n=263) P value
Sociodemographic characteristics
Age (years) 74±12 72±13 67±13*,† <0.001 Sex (male) 49 (70) 107 (59) 168 (64) 0.204
Clinical characteristics at discharge
NYHA class III or IV 9 (13) 24 (13) 21 (8) 0.170
De novo HF 26 (37) 60 (33) 48 (18) <0.001 Systolic BP(mmHg) 118±20 116±20 116±20 0.642
Heart rate (beats/min) 66±14 70±14 75±16*,† <0.001 BMI (kg/m2) 22.8±3.7 22.5±4.1 22.5±4.2 0.817
Comorbidities
Ischemic etiology 22 (31) 76 (42) 80 (30) 0.046
Hypertension 35 (50) 108 (59) 142 (54) 0.368
Diabetes 30 (43) 86 (47) 130 (49) 0.603
Atrial fibrillation 45 (64) 131 (72) 176 (67) 0.434
Biochemistry at discharge
BNP (pg/mL) 387±334 343±371 425±496 0.165
Hemoglobin (g/dL) 12.1±2.1 12.0±2.2 12.8±2.5† <0.001 Serum sodium (mEq/L) 140±3 139±3 139±3 0.467
eGFR (mL /min/1.73 m2) 46±20 50±22 55±23*,† 0.002
Echocardiographic parameter at discharge
LVEF (%) 56±15 48±16* 39±13*,† <0.001 LVEDV (mL) 119±67 120±64 124±55 0.707
LV mass index (g/m2) 136±48 128±40 134±39 0.233
LAVI (mL/m2) 60±29 57±37 51±30 0.066
TRPG (mmHg) 30±13 29±12 27±12 0.075
E/e’ 16.9±8.0 16.7±9.0 16.2±7.4 0.700
IVC (mm) 16±6 16±5 15±5 0.496
Medication at discharge
Diuretics 40 (57) 104 (57) 152 (58) 0.979
β-blocker 49 (70) 139 (76) 217 (83) 0.048
ACEI/ARB 46 (66) 117 (64) 184 (70) 0.394
Aldosterone antagonist 38 (54) 106 (58) 179 (68) 0.028
Device therapy
Pacemaker 13 (19) 9 (5) 5 (2) <0.001 Implantable cardioverter defibrillator 2 (3) 7 (4) 1 (0.4) 0.019
CRT 6 (9) 12 (7) 8 (3) 0.088
Coronary revascularization during follow-up
PCI 11 (16) 25 (14) 48 (18) 0.426
CABG 1 (1) 5 (3) 5 (2) 0.760
Data are expressed as mean ± SD or as n (%). *P<0.05 vs. Worsening LVEF; †P<0.05 vs. Stable LVEF. Abbrevia-tions as in Table 1.
Circulation Journal Vol.83, March 2019
589Change in LVEF and Prognosis
The relationships between the clinical parameters and LVEF changes after discharge are shown in Supplementary Table 2. The multivariable linear regression analysis in the HFrEF cohort showed that the predischarge heart rate was significantly correlated with increased LVEF, and use of aldosterone antagonists tend to be correlated with increased LVEF, while ischemic etiology was correlated with a decrease in LVEF. In the HFmrEF cohort, only LVEDV was significantly correlated with a decrease in LVEF. In the HFpEF cohort, the predischarge heart rate was significantly correlated with increased LVEF, while older age, advanced NYHA classification, and increased LVEDV were correlated with a decrease in LVEF. The heart rate at discharge showed a significant negative cor-relation with the change in heart rate during the follow-up period in each LVEF classification (R=−0.732, P<0.001 in HFrEF, R=−0.675, P<0.001 in HFmrEF, R=−0.583, P<0.001 in HFpEF). In addition, the change in heart rate during the follow-up period showed a significant negative correlation with the change in LVEF (R=−0.318, P<0.001 in HFrEF, R=−0.228, P=0.042 in HFmrEF, R=−0.234,
the whole cohort and the HFrEF cohort, the improving LVEF group had significantly better prognosis than the worsening and stable LVEF groups (P<0.001, P<0.001, respectively). On the other hand, in the HFpEF and HFmrEF cohorts, the clinical outcomes were similar among the 3 LVEF groups (P=0.582, P=0.535, respectively).
Clinical Parameters Related to Change in LVEFThe relationships between clinical parameters and LVEF changes during hospitalization in the linear regression analysis are shown in Supplementary Table 1. The multi-variable linear regression analysis among the selected parameters in patients with LVEF <40% on admission showed that older age was significantly correlated with a decrease in LVEF. In patient with LVEF 40–49% on admission, increased heart rate and increased BNP level on admission were significantly correlated with an increase in LVEF. In patient with LVEF ≥50% on admission, the increased BNP level at admission was significantly corre-lated with an increase in LVEF, while inferior vena cava diameter was correlated with a decrease in LVEF.
Figure 3. Longitudinal change in left ventricular ejection fraction (LVEF). (A) All cohort. (B) Classification based on LVEF.
Figure 4. Longitudinal change in heart failure classification. LVEF, left ventricular ejection fraction.
Circulation Journal Vol.83, March 2019
590 YAMAMOTO M et al.
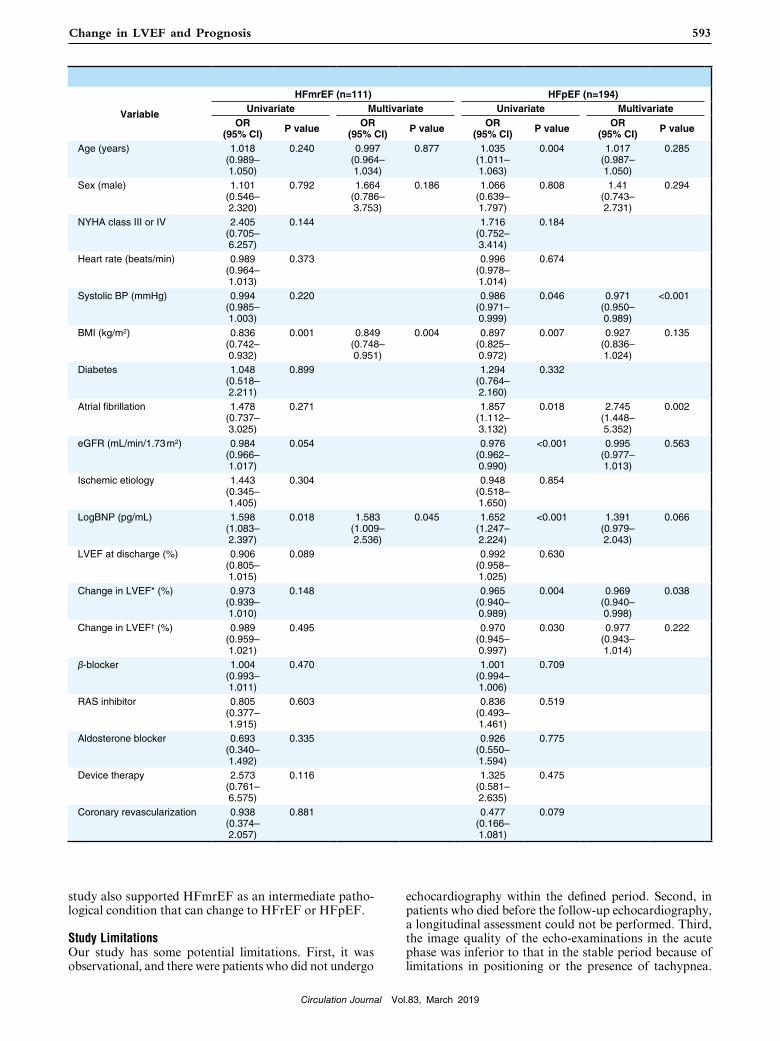
(4) the HFmrEF cohort had an intermediate pathological condition that changed to either HFrEF or HFpEF.
One-Off Measurement of LVEF and Prognosis in ADHFTo our knowledge, this study is one of the first to evaluate the clinical implications of LVEF not only in the stable phase, but in the acute phase of HF on admission. Previous studies have reported that there are no significant differ-ences in prognosis between HFpEF and HFrEF,5–7 and our results suggested that LVEF at admission and predis-charge does not clearly affect prognosis. Furthermore, almost all previous studies classified HF during the stable period. Our study indicated that LVEF can change greatly during hospitalization, especially in HFmrEF and HFpEF patients. Among the patients diagnosed as HFpEF in the stable period, 40.2% were not classified as HFpEF on admission. Therefore, this study revealed that HF classifi-cation is greatly affected by the time of LVEF determina-tion.
Change in LVEF During Hospitalization and After DischargeWe evaluated the changes in LVEF between the acute phase and predischarge and determined that the time at which LVEF changed was different in the different HF classifications. In HFrEF, LVEF improved after discharge, whereas it improved during hospitalization in HFpEF. These findings suggested that the improvement of LVEF in HFpEF is greatly influenced by the change in hemody-namics, while improvement of LVEF in HFrEF is caused by improvement of intrinsic cardiac function through optimal treatment. LVEF can be dramatically changed by changes in preload, afterload, and heart rate in the short term. In fact, LVEF significantly increased from admission to predischarge in the HFpEF and HFmrEF cohorts. These findings could be explained by the fact that heart rate in HFpEF and inferior vena cava diameter in HFmrEF were identified as independent factors associated with increased
P=0.003 in HFpEF).
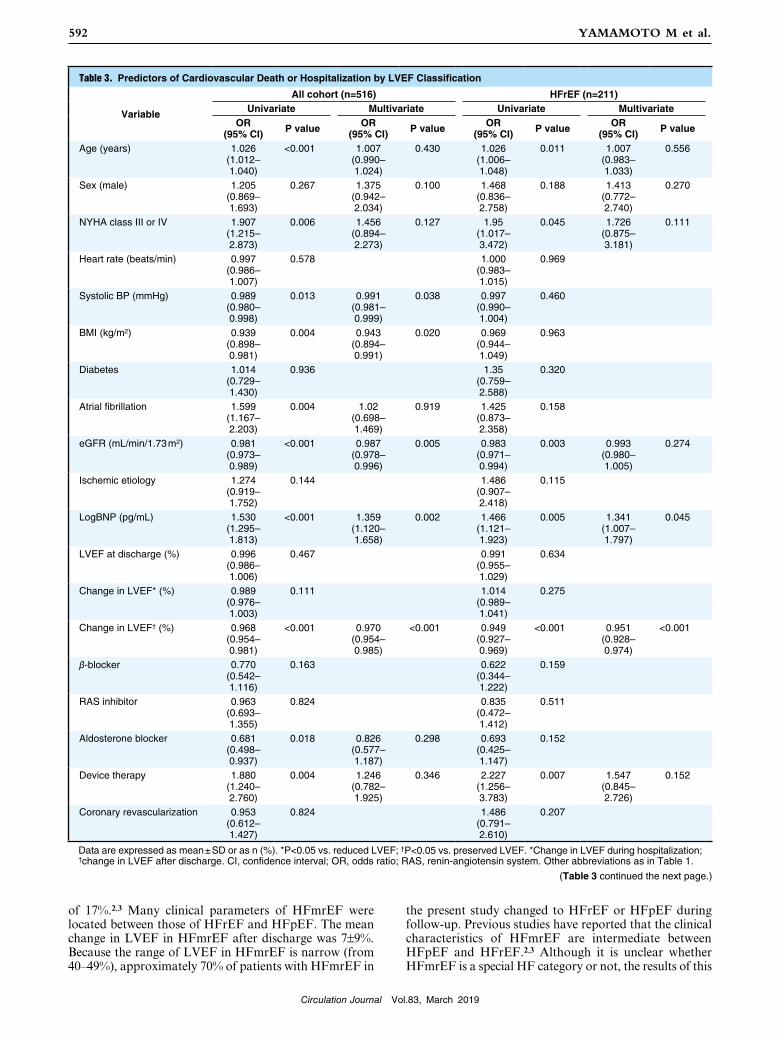
Predictors of Cardiovascular Death and Hospitalization by LVEF ClassificationIn the HFrEF cohort, age, NYHA class III/IV, eGFR, logarithm of BNP value, device therapy, and change in LVEF after discharge were significant prognostic factors for the clinical endpoint in the univariate analyses (Table 3). In the multivariable age- and sex-adjusted mod-els, logBNP (HR: 1.341; 95% CI: 1.007–1.797; P=0.045) and change in LVEF after discharge were identified as independent prognostic factors (HR: 0.951; 95% CI: 0.928–0.974; P<0.001). In the HFmrEF cohort, body mass index (BMI) and logBNP were significant prognostic fac-tors in the univariate analyses, and both parameters were also independent prognostic factor in the multivariable model. In the HFpEF cohort, BMI, logBNP, diabetes, eGFR, systolic blood pressure at admission, use of aldo-sterone antagonists, change in LVEF during hospitaliza-tion, and change in LVEF after discharge were identified as prognostic factors in the univariate analyses. Change in LVEF during hospitalization (HR: 0.969; 95% CI: 0.940–0.998; P=0.038), diabetes, and systolic blood pressure were prognostic factors in the multivariable model.
DiscussionThe 4 major findings of our study were: (1) none of the 3 HF classifications by LVEF on admission or predischarge were associated with clinical outcomes; (2) LVEF improved after discharge in the HFrEF cohort, improved during hospitalization in the HFpEF cohort, and consistently improved in the HFmrEF cohort throughout the observa-tion period; (3) the change in LVEF after discharge was an independent prognostic factor in the HFrEF cohort, whereas the change in LVEF during hospitalization was an independent prognostic factor in the HFpEF cohort; and
Figure 5. Kaplan-Meier curves according to the change in left ventricular ejection fraction (LVEF) during hospitalization and after discharge. (A) Change in LVEF during hospitalization. (B) Change in LVEF after discharge. HFpEF, HFrEF, HFmrEF: heart failure with preserved, reduced and mid-range EF, respectively.

Circulation Journal Vol.83, March 2019
591Change in LVEF and Prognosis
results of previous studies in which LVEDV and ischemic etiology were related parameters.2 Therefore, we conclude that less LV remodeling is related to improvement in LVEF in the chronic phase of HFmrEF.
Clinical Impact of Change in LVEFThis study showed that the change in LVEF after dis-charge is an independent prognostic factor in HFrEF, whereas a change during hospitalization is an independent prognostic factor in HFpEF. In all cohorts, the improving LVEF group had the lowest predischarge LVEF and a better prognosis compared with the stable and worsening LVEF groups. This result suggested that a change in LVEF is a strong predictor regardless of the baseline LVEF. Patients with HF and a recovered EF, currently defined as LVEF >40%22 or >45%11 or >50%,10 but previously documented lower LVEF than the cutoff value, have been reported to have a better clinical course than those with persistent HFpEF and HFrEF. We evaluated the changes in LVEF as a continuous variablesso that we could show a relationship between the change in LVEF and prognosis even if LVEF did not transition to another classification.
Breathett et al reported that LVEF improvement (≥5%) was associated with fewer clinical events in HFrEF patients treated with β-blockers, and that LVEF and serum creati-nine level were significant predictors.9 In our study, eGFR was not a strong predictor, but BNP and change in LVEF after discharge were independent predictors in HFrEF. Our population had a larger change in LVEF (11% vs. 4.5%), and the effect of this change on the prognosis was more apparent.
In HFpEF, not only the change in LVEF, but also some clinical parameters were independent prognostic factors. Previous studies have reported BNP level, age, diabetes status, systolic blood pressure, BMI, advanced NYHA classification, and renal function as prognostic factors in HFpEF.23,24 However, the clinical effect of changes in LVEF in HFpEF has been rarely evaluated. Most of these clinical indices, as well as a change in LVEF during hospi-talization, have been identified as related to prognosis in previous studies. HFpEF has also been reported to be potentially associated with systolic dysfunction.25 In cases in which LVEF improves more significantly in the acute phase, it seems to decrease because of elevated systolic blood pressure and tachycardia, but the intrinsic systolic function is maintained, which is thought to lead to an improvement in prognosis.
In HFmrEF, BMI and BNP level were independent prognostic factors. Previous studies have reported age, BNP level, and use of diuretics as being related to progno-sis, and HFmrEF patients had increased mortality when they progressed to HFrEF at 1 year.2 In this study, a signifi-cant effect of a change in LVEF on prognosis in HFmrEF was not observed. Our study registered patients at the time of admission for ADHF, whereas previous studies have included many outpatients, and the average BNP level in our study was almost twice that in the previous research (343 vs. 164 pg/mL), and more severe cases were included. Because the number of patients with HFmrEF in this study was small, further study with more patients with HFmrEF is needed.
Clinical Characteristics of HFmrEFIn this study, the prevalence of HFmrEF was 22.5%, which is slightly higher than the previously reported prevalence
LVEF. Previous studies have reported that patients with high blood pressure at hospitalization have a better prog-nosis and a larger LVEF during the stable period.14,15 Although no studies have evaluated the change in LVEF between the acute phase and stable phases, the results of this study suggested LVEF was more affected by heart rate and central venous pressure than by systolic blood pres-sure in the acute phase.
A previous study has reported that in patients with HFpEF, on average the LVEF decreased by 5.8% over 5 years, with greater declines in older individuals and those with coronary artery disease.16 Conversely, LVEF increased in patients with HFrEF (average increase 6.9% over 5 years). The follow-up period of our study was much shorter, but the improvement in LVEF was much larger in the HFrEF cohort, and decreases in LVEF were not observed in the HFpEF cohort. The prognosis for patients with reduced EF improves over time, but not for those with preserved EF.17 One explanation for the difference in these results is the improvement in the prognosis for HFrEF in recent years.
In the HFpEF group, results of this study showed a high heart rate was associated with increased LVEF after discharge, whereas advanced NYHA classification, large LVEDV, and older age were associated with a decrease in LVEF. These findings mean that a decline in preload because of tachycardia, and not advanced HF, without severe left ventricular remodeling is important for improve-ment of LVEF in HFpEF. Unlike in previous studies, the reason why decreases in LVEF were not observed in our study is unclear. A possible explanation is the shorter observation period and fewer cases of HF with an ischemic etiology, which is associated with smaller increases in LVEF, in our study population.
Although some HFrEF patients might have unique pathological conditions such as tachycardia-induced car-diomyopathy, a higher heart rate at discharge was related to an increase in LVEF, in common with HFrEF and HFpEF. One possible interpretation was that because sympathetic nervous activity was much higher in patients with a higher heart rate at discharge, treatment during the follow-up period more strongly suppressed sympathetic nerve activity, leading to a larger improvement in LVEF. LV myocardial viability is known to be an essential factor in recovery of LV systolic function, and the results of this study suggested that that parameter, which is related to LV myocardial viability, was different among the LVEF classifications. Non-ischemic etiology in HFrEF, mild LV remodeling, less advanced NYHA class and younger age in HFpEF were important factors related to the existence of LV myocardial viability.
Although a few clinical trials involving HFpEF suggest a possible benefit with regard to morbidity and other clin-ical parameters, no treatment has been identified to pro-vide a proven reduction in mortality.18–21 However, the effect of medical treatment on cardiac function in HFpEF is not fully elucidated. In the present study, there were no medical treatments associated with an increase in LVEF. Further research is needed to investigate not only the effect of medical treatment on prognosis, but also of cardiac function in HFpEF.
In HFmrEF, LVEDV, BNP, and heart rate were associ-ated with changes in LVEF during hospitalization, and these factors were also mainly associated with HFpEF. However, the only clinical parameter related to changes in LVEF after discharge was LVEDV, which agrees with the
Circulation Journal Vol.83, March 2019
592 YAMAMOTO M et al.
the present study changed to HFrEF or HFpEF during follow-up. Previous studies have reported that the clinical characteristics of HFmrEF are intermediate between HFpEF and HFrEF.2,3 Although it is unclear whether HFmrEF is a special HF category or not, the results of this
of 17%.2,3 Many clinical parameters of HFmrEF were located between those of HFrEF and HFpEF. The mean change in LVEF in HFmrEF after discharge was 7±9%. Because the range of LVEF in HFmrEF is narrow (from 40–49%), approximately 70% of patients with HFmrEF in
Table 3. Predictors of Cardiovascular Death or Hospitalization by LVEF Classification
Variable
All cohort (n=516) HFrEF (n=211)Univariate Multivariate Univariate Multivariate
OR (95% CI) P value OR
(95% CI) P value OR (95% CI) P value OR
(95% CI) P value
Age (years) 1.026 (1.012– 1.040)
<0.001 1.007 (0.990– 1.024)
0.430 1.026 (1.006– 1.048)
0.011 1.007 (0.983– 1.033)
0.556
Sex (male) 1.205 (0.869– 1.693)
0.267 1.375 (0.942– 2.034)
0.100 1.468 (0.836– 2.758)
0.188 1.413 (0.772– 2.740)
0.270
NYHA class III or IV 1.907 (1.215– 2.873)
0.006 1.456 (0.894– 2.273)
0.127 1.95 (1.017– 3.472)
0.045 1.726 (0.875– 3.181)
0.111
Heart rate (beats/min) 0.997 (0.986– 1.007)
0.578 1.000 (0.983– 1.015)
0.969
Systolic BP (mmHg) 0.989 (0.980– 0.998)
0.013 0.991 (0.981– 0.999)
0.038 0.997 (0.990– 1.004)
0.460
BMI (kg/m2) 0.939 (0.898– 0.981)
0.004 0.943 (0.894– 0.991)
0.020 0.969 (0.944– 1.049)
0.963
Diabetes 1.014 (0.729– 1.430)
0.936 1.35 (0.759– 2.588)
0.320
Atrial fibrillation 1.599 (1.167– 2.203)
0.004 1.02 (0.698– 1.469)
0.919 1.425 (0.873– 2.358)
0.158
eGFR (mL/min/1.73 m2) 0.981 (0.973– 0.989)
<0.001 0.987 (0.978– 0.996)
0.005 0.983 (0.971– 0.994)
0.003 0.993 (0.980– 1.005)
0.274
Ischemic etiology 1.274 (0.919– 1.752)
0.144 1.486 (0.907– 2.418)
0.115
LogBNP (pg/mL) 1.530 (1.295– 1.813)
<0.001 1.359 (1.120– 1.658)
0.002 1.466 (1.121– 1.923)
0.005 1.341 (1.007– 1.797)
0.045
LVEF at discharge (%) 0.996 (0.986– 1.006)
0.467 0.991 (0.955– 1.029)
0.634
Change in LVEF* (%) 0.989 (0.976– 1.003)
0.111 1.014 (0.989– 1.041)
0.275
Change in LVEF† (%) 0.968 (0.954– 0.981)
<0.001 0.970 (0.954– 0.985)
<0.001 0.949 (0.927– 0.969)
<0.001 0.951 (0.928– 0.974)
<0.001
β-blocker 0.770 (0.542– 1.116)
0.163 0.622 (0.344– 1.222)
0.159
RAS inhibitor 0.963 (0.693– 1.355)
0.824 0.835 (0.472– 1.412)
0.511
Aldosterone blocker 0.681 (0.498– 0.937)
0.018 0.826 (0.577– 1.187)
0.298 0.693 (0.425– 1.147)
0.152
Device therapy 1.880 (1.240– 2.760)
0.004 1.246 (0.782– 1.925)
0.346 2.227 (1.256– 3.783)
0.007 1.547 (0.845– 2.726)
0.152
Coronary revascularization 0.953 (0.612– 1.427)
0.824 1.486 (0.791– 2.610)
0.207
Data are expressed as mean ± SD or as n (%). *P<0.05 vs. reduced LVEF; †P<0.05 vs. preserved LVEF. *Change in LVEF during hospitalization; †change in LVEF after discharge. CI, confidence interval; OR, odds ratio; RAS, renin-angiotensin system. Other abbreviations as in Table 1.
(Table 3 continued the next page.)
Circulation Journal Vol.83, March 2019
593Change in LVEF and Prognosis
echocardiography within the defined period. Second, in patients who died before the follow-up echocardiography, a longitudinal assessment could not be performed. Third, the image quality of the echo-examinations in the acute phase was inferior to that in the stable period because of limitations in positioning or the presence of tachypnea.
study also supported HFmrEF as an intermediate patho-logical condition that can change to HFrEF or HFpEF.
Study LimitationsOur study has some potential limitations. First, it was observational, and there were patients who did not undergo
Variable
HFmrEF (n=111) HFpEF (n=194)Univariate Multivariate Univariate Multivariate
OR (95% CI) P value OR
(95% CI) P value OR (95% CI) P value OR
(95% CI) P value
Age (years) 1.018 (0.989– 1.050)
0.240 0.997 (0.964– 1.034)
0.877 1.035 (1.011– 1.063)
0.004 1.017 (0.987– 1.050)
0.285
Sex (male) 1.101 (0.546– 2.320)
0.792 1.664 (0.786– 3.753)
0.186 1.066 (0.639– 1.797)
0.808 1.41 (0.743– 2.731)
0.294
NYHA class III or IV 2.405 (0.705– 6.257)
0.144 1.716 (0.752– 3.414)
0.184
Heart rate (beats/min) 0.989 (0.964– 1.013)
0.373 0.996 (0.978– 1.014)
0.674
Systolic BP (mmHg) 0.994 (0.985– 1.003)
0.220 0.986 (0.971– 0.999)
0.046 0.971 (0.950– 0.989)
<0.001
BMI (kg/m2) 0.836 (0.742– 0.932)
0.001 0.849 (0.748– 0.951)
0.004 0.897 (0.825– 0.972)
0.007 0.927 (0.836– 1.024)
0.135
Diabetes 1.048 (0.518– 2.211)
0.899 1.294 (0.764– 2.160)
0.332
Atrial fibrillation 1.478 (0.737– 3.025)
0.271 1.857 (1.112– 3.132)
0.018 2.745 (1.448– 5.352)
0.002
eGFR (mL/min/1.73 m2) 0.984 (0.966– 1.017)
0.054 0.976 (0.962– 0.990)
<0.001 0.995 (0.977– 1.013)
0.563
Ischemic etiology 1.443 (0.345– 1.405)
0.304 0.948 (0.518– 1.650)
0.854
LogBNP (pg/mL) 1.598 (1.083– 2.397)
0.018 1.583 (1.009– 2.536)
0.045 1.652 (1.247– 2.224)
<0.001 1.391 (0.979– 2.043)
0.066
LVEF at discharge (%) 0.906 (0.805– 1.015)
0.089 0.992 (0.958– 1.025)
0.630
Change in LVEF* (%) 0.973 (0.939– 1.010)
0.148 0.965 (0.940– 0.989)
0.004 0.969 (0.940– 0.998)
0.038
Change in LVEF† (%) 0.989 (0.959– 1.021)
0.495 0.970 (0.945– 0.997)
0.030 0.977 (0.943– 1.014)
0.222
β-blocker 1.004 (0.993– 1.011)
0.470 1.001 (0.994– 1.006)
0.709
RAS inhibitor 0.805 (0.377– 1.915)
0.603 0.836 (0.493– 1.461)
0.519
Aldosterone blocker 0.693 (0.340– 1.492)
0.335 0.926 (0.550– 1.594)
0.775
Device therapy 2.573 (0.761– 6.575)
0.116 1.325 (0.581– 2.635)
0.475
Coronary revascularization 0.938 (0.374– 2.057)
0.881 0.477 (0.166– 1.081)
0.079
Circulation Journal Vol.83, March 2019
594 YAMAMOTO M et al.
tion, biomarkers, and outcomes. Circulation 2014; 129: 2380 – 2387.
11. Lupón J, Díez-López C, de Antonio M, Domingo M, Zamora E, Moliner P, et al. Recovered heart failure with reduced ejection fraction and outcomes: A prospective study. Eur J Heart Fail 2017; 19: 1615 – 1623.
12. McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history of congestive heart failure: The Framingham study. N Engl J Med 1971; 285: 1441 – 1446.
13. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quan-tification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2015; 28: 1 – 39.
14. Gheorghiade M, Abraham WT, Albert NM, Greenberg BH, O’Connor CM, She L, et al; OPTIMIZE-HF Investigators and Coordinators. Systolic blood pressure at admission, clinical char-acteristics, and outcomes in patients hospitalized with acute heart failure. JAMA 2006; 296: 2217 – 2226.
15. Ambrosy AP, Vaduganathan M, Mentz RJ, Greene SJ, Subačius H, Konstam MA, et al. Clinical profile and prognostic value of low systolic blood pressure in patients hospitalized for heart failure with reduced ejection fraction: Insights from the Efficacy of Vasopressin Antagonism in Heart Failure: Outcome Study with Tolvaptan (EVEREST) trial. Am Heart J 2013; 165: 216 – 225.
16. Dunlay SM, Roger VL, Weston SA, Jiang R, Redfield MM. Longitudinal changes in ejection fraction in heart failure patients with preserved and reduced ejection fraction. Circ Heart Fail 2012; 5: 720 – 726.
17. Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006; 355: 251 – 259.
18. Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJ, et al; CHARM Investigators and Committees. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: The CHARM-Preserved Trial. Lancet 2003; 362: 777 – 781.
19. Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B, et al; TOPCAT Investigators. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med 2014; 370: 1383 – 1392.
20. Fonarow GC, Stough WG, Abraham WT, Albert NM, Gheorghiade M, Greenberg BH, et al; OPTIMIZE-HF Investi-gators and Hospitals. Characteristics, treatments, and outcomes of patients with preserved systolic function hospitalized for heart failure: A report from the OPTIMIZE-HF Registry. J Am Coll Cardiol 2007; 50: 768 – 777.
21. Massie BM, Carson PE, McMurray JJ, Komajda M, McKelvie R, Zile MR, et al; I-PRESERVE Investigators. Irbesartan in patients with heart failure and preserved ejection fraction. N Engl J Med 2008; 359: 2456 – 2467.
22. Kalogeropoulos AP, Fonarow GC, Georgiopoulou V, Burkman G, Siwamogsatham S, Patel A, et al. Characteristics and out-comes of adult outpatients with heart failure and improved or recovered ejection fraction. JAMA Cardiol 2016; 1: 510 – 518.
23. Lee DS, Gona P, Vasan RS, Larson MG, Benjamin EJ, Wang TJ, et al. Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: Insights from the Framingham Heart Study of the National Heart, Lung, and Blood Institute. Circulation 2009; 119: 3070 – 3077.
24. Pocock SJ, Ariti CA, McMurray JJ, Maggioni A, Køber L, Squire IB, et al; Meta-Analysis Global Group in Chronic Heart Failure. Predicting survival in heart failure: A risk score based on 39372 patients from 30 studies. Eur Heart J 2013; 34: 1404 – 1413.
25. Kraigher-Krainer E, Shah AM, Gupta DK, Claggett B, Pieske B, Zile MR, et al; PARAMOUNT Investigators. Impaired sys-tolic function by strain imaging in heart failure with preserved ejection fraction. J Am Coll Cardiol 2014; 63: 447 – 456.
Supplementary Files
Please find supplementary file(s);http://dx.doi.org/10.1253/circj.CJ-18-0881
However, we were able to obtain adequate imaging from approximately 97% of the patients for the assessment of LVEF. Fourth, the LVEF classification strongly depends on the timing of its determination. Though patients were classified by LVEF at discharge, if classified by LVEF on admission, results were markedly different. However, this is a limitation and also an important fact that this study demonstrated. Last, though subsequent LVEF measure-ments were performed after 1 year from discharge accord-ing to the study protocol, clinical benefits are thought to be greater if prognosis is predicted earlier than 1 year.
ConclusionsIndependent of a one-off measurement of LVEF, the change in LVEF after discharge in HFrEF, and the change in LVEF during hospitalization in HFpEF, strongly affected prognosis. We believe that the findings of this study pro-vide a rationale for continuing intensive medical or inva-sive therapy in HF patients whose LVEF tends to decrease, or does not improve, and helps elucidate the pathophysi-ological differences in HF populations to guide optimal therapy.
Acknowledgments / Sources of FundingNone.
DisclosuresNone declared.
References 1. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG,
Coats AJ, et al. 2016 ESC Guidelines for the diagnosis and treat-ment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology. Eur J Heart Fail 2016; 18: 891 – 975.
2. Tsuji K, Sakata Y, Nochioka K, Miura M, Yamauchi T, Onose T, et al. Characterization of heart failure patients with mid-range left ventricular ejection fraction: A report from the CHART-2 Study. Eur J Heart Fail 2017; 19: 1258 – 1269.
3. Rickenbacher P, Kaufmann BA, Maeder MT, Bernheim A, Goetschalckx K, Pfister O, et al; TIME-CHF Investigators. Heart failure with mid-range ejection fraction: A distinct clinical entity? Insights from the Trial of Intensified versus standard Medical therapy in Elderly patients with Congestive Heart Failure. Eur J Heart Fail 2017; 19: 1586 – 1596.
4. Lam CS, Teng THK. Understanding heart failure with mid-range ejection fraction. JACC Heart Fail 2016; 4: 473 – 476.
5. Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med 2006; 355: 260 – 269.
6. Steinberg BA, Zhao X, Heidenreich PA, Peterson ED, Bhatt DL, Cannon CP, et al. Trends in patients hospitalized with heart failure and preserved left ventricular ejection fraction: Prevalence, therapies, and outcomes. Circulation 2012; 126: 65 – 75.
7. Bursi F, Weston SA, Redfield MM, Jacobsen SJ, Pakhomov S, Nkomo VT, et al. Systolic and diastolic heart failure in the com-munity. JAMA 2006; 296: 2209 – 2216.
8. Solomon SD, Anavekar N, Skali H, McMurray JJ, Swedberg K, Yusuf S, et al. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circula-tion 2005; 112: 3738 – 3744.
9. Breathett K, Allen LA, Udelson J, Davis G, Bristow M. Changes in left ventricular ejection fraction predict survival and hospital-ization in heart failure with reduced ejection fraction. Circ Heart Fail 2016; 9: pii: e002962.
10. Basuray A, French B, Ky B, Vorovich E, Olt C, Sweitzer NK, et al. Heart failure with recovered ejection fraction: Clinical descrip-