direct and primary carotid endarterectomy for common carotid artery occlusion. report of 2 cases
TRANSCRIPT

Available online at www.sciencedirect.com
Surgical Neurolog
Imaging
Direct and primary carotid endarterectomy for common
carotid artery occlusion: Report of 2 cases
Tomohiro Inoue, MD, Kazuo Tsutsumi, MD4, Shinobu Adachi, MD,
Shota Tanaka, MD, Naoto Kunii, MD, Masahiro Indo, MDDepartment of Neurosurgery, Showa General Hospital, Kodaira-shi, Tokyo 187-8510, Japan
Received 18 July 2006; accepted 4 January 2007
www.surgicalneurology-online.com
Abstract Background: Cerebral ischemia associated with chronic CCA occlusion is a rare condition and
0090-3019/$ – see fro
doi:10.1016/j.surneu.2
Abbreviations: C
tomographic scan; EC
MCA, middle cerebral
magnetic resonance
posterior communicat
temporal artery; TIAs,
4 Corresponding a
E-mail address: k
raises strategic dilemma when the revascularization is needed.
Methods: Two patients with CCA occlusion presented with ischemic symptom associated with the
affected side. Both patients underwent vascular reconstruction by direct carotid endarterectomy to
achieve primary restoration of CCA to ICA flow.
Results: Successful reopening of the vessels was obtained in both patients without the evidence of
postsurgical ischemic event. Follow-up MRA was obtained at later than 6 months after surgery,
which demonstrated patent CCA-ICA in both patients.
Conclusions: Direct carotid endarterectomy of the occluded CCA can be safely performed if the
preoperative angiography suggest still patent vessels distal to carotid bifurcation and the substantial
bback flowQ is obtained from ICA during arteriotomy.
D 2008 Elsevier Inc. All rights reserved.
Keywords: Carotid endarterectomy; Common carotid artery occlusion; Ischemic cerebrovascular disease
1. Introduction
Chronic CCA occlusion is a rare condition and may be
associated with stroke, TIAs or chronic ischemia such as
vascular dementia. Several recent reports have discussed
the surgical revascularization of CCA mainly using
extracranial bypass procedure SA-ECA saphenous vein
interposition grafting with or without subsequent STA-
MCA bypass [1,3,5,6]. However, direct and primary carotid
endarterectomy for chronic CCA occlusion to reopen CCA-
ICA, CCA-ECA, or both has not been well discussed. We
report 2 patients who underwent carotid endarterectomy for
nt matter D 2008 Elsevier Inc. All rights reserved.
007.01.034
CA, common carotid artery; CT scan, computed
A, external carotid artery; ICA, internal carotid artery;
artery; MRA, magnetic resonance angiography; MRI,
imaging; PCA, posterior cerebral artery; PcomA,
ing artery; SA, subclavian artery; STA, superficial
transient ischemic attacks; VA, vertebral artery.
uthor: Tel.: +81 424 61 0052; fax: +81 424 64 7912.
[email protected] (K. Tsutsumi).
CCA occlusion. The details of the management are
presented and discussed.
2. Case reports
2.1. Case 1
The first subject is a 65-year-old man who presented to
another hospital with a complaint of left hemiparesis. His
medical history was significant for smoking and hyperlipid-
emia. Magnetic resonance imaging and MRA were per-
formed, which showed infarction of corona radiata and
watershed area of right cerebral hemisphere as well as right
ICA occlusion. He was referred to our department for
possible surgical revascularization. Neurologic examination
showed mental decline, left side neglect, as well as left
hemiparesis being worse in the upper extremity. Cerebral
angiography revealed right CCA occlusion with residual
stump opacified several centimeters from the origin at right
innominate artery. Collateral filling of right ECA back to the
origin of occipital artery was seen from vertebral injection
y 69 (2008) 620–626

T. Inoue et al. / Surgical Neurology 69 (2008) 620–626 621
through muscular branch, with only faint and delayed
opacification of right STA. Left carotid injection showed
moderate cross-flow toward right hemisphere and delayed
retrograde opacification of cavernous to petrous right ICA.
The right PCA area was also filled through this moderate
cross-flow because of atretic right P1 (Fig. 1). After
thorough discussion, we decided to try carotid endrater-
ectomy, expecting that the carotid bifurcation was still
open. In the operation, CCA was exposed proximally with
ligation and resection of omohyoideus muscle. We
observed that the ICA, ECA, as well as the CCA
appeared as externally normal vessels with enough vasa
vasorum, as usually seen in carotid endarterectomy. The
proximal portion of CCA and the distal portion of ICA
and ECA were soft on palpation. With CCA and ECA
clamped, arteriotomy was made along the CCA, showing
total occlusion of CCA just around the carotid bifurcation
by atheromatous plaque and retrograde extension of
organized thrombus. Then another small arteriotomy was
Fig. 1. Upper left: preoperative CT scan of the head showing infarction of coron
preoperative right carotid angiogram (anteroposterior view) showing CCA occlusio
artery. Upper right: collateral filling of right ECAwas seen from vertebral injectio
injection (anteroposterior view) showed moderate cross-flow toward right cerebra
right ICA.
made on ICA distal to the obvious atheromatous disease,
and moderate back flow was obtained. We extracted back
flow for a while to remove a possible small thrombus in
distal ICA, and then the distal ICA was clamped.
Atheromatous plaque was dissected in the usual manner.
The extent of plaque was within usual levels for ICA and
ECA, and could be cleaned out. On the CCA side, the
plaque was dissected as proximally as possible until it was
thin enough. After removal of plaque, the inner surface of
the vessels looked smooth with some oozing of blood
showing viable media. The arteriotomy was closed via
primary closure with 6-0 prolene. Postoperatively, to
reduce the risk of hyperperfusion, rigorous attention was
paid to keep the systolic blood pressure lower than 120
mm Hg for several days. Postoperative diffusion-weighted
MRIs did not show any new hyperintense spot compared
to preoperative ones (Fig. 2). Postoperative right carotid
angiogram showed patent cervical CCA-ICA, ECA, and
robust anterograde opacification of the whole right
a radiata and watershed area of the right cerebral hemisphere. Lower left:
n with residual stump several centimeters from the origin at right innominate
n (lateral view) through vertebral muscular branch. Lower right: left carotid
l hemisphere and delayed retrograde opacification of cavernous to petrous

Fig. 2. Left: postoperative right carotid angiogram (lateral view) showing patent cervical CCA-ICA and ECA. Upper right: right carotid angiogram (lateral
view) showing robust anterograde opacification of the whole right intracranial ICA area. Lower right: postoperative diffusion-weighted MRIs did not show any
new hyperintense spot compared to preoperative ones.
T. Inoue et al. / Surgical Neurology 69 (2008) 620–626622
intracranial ICA area (Fig. 2). The patient’s neurologic
status, especially mental decline and left side neglect, was
significantly improved. At 17 months follow-up after
surgery, MRI/MRA continued to show patent right CCA-
ICA without evidence of new ischemic lesions (Fig. 3).
The patient is walking and leading an almost independent
life although hemiparesis of the left upper extremity is
still present.
2.2. Case 2
This 75-year-old man presented to another hospital
complaining of recent mental decline and forgetfulness.
His medical history was significant for smoking, diabetes
mellitus, hypertension, and angina pectoris. Carotid ultra-
sonography was performed, and results suggested severe
right carotid stenosis. He was referred to our hospital for
possible surgical intervention. Neurologic examination
showed no focal deficit, although Wechsler Memory Scale
showed significantly impaired visual memory scale com-
pared to verbal memory scale, suggestive of obtunded right
cerebral hemisphere function. Magnetic resonance images
showed multiple lacunar infarctions with slight cerebral
atrophy compatible with his age. Cerebral angiography
demonstrated right CCA occlusion with residual stump
opacified several centimeters from the origin at right
innominate artery. Collateral filling of right ECA back to
the carotid bifurcation that led to very delayed and faint
anterograde filling of cervical ICA up to cavernous portion
was seen from vertebral injection through vertebral
muscular branch. In addition, vertebral injection showed
moderate flow toward the right ICA area through PcomA
(Fig. 4). After a thorough discussion, and considering that
carotid bifurcation is still open through vertebral collateral
in this patient, we decided to proceed with direct and
primary carotid endarterectomy to reopen the CCA-ICA
anterograde flow. Details of this surgical procedure are

Fig. 3. Cervical MRA (left) and intracranial MRA (upper right) obtained at 17 months follow-up (after surgery), showing still patent right CCA-ICA flow.
T. Inoue et al. / Surgical Neurology 69 (2008) 620–626 623
almost the same as in case 1 (Fig. 5). Postoperatively,
to reduce the risk of hyperperfusion, rigorous attention
was paid to keep the systolic blood pressure lower than
Fig. 4. Left: preoperative right carotid injection (anteroposterior view) showing C
origin at right innominate artery. Upper right: vertebral injection (lateral view, e
bifurcation through vertebral muscular branch. Moderate flow toward the right
(lateral view, late arterial phase) shows delayed and faint anterograde filling of cer
ICA collateral.
120 mm Hg for several days. Postoperative diffusion-
weighted MRIs were not performed because of contraindi-
cation (recent coronary stenting), although CT scan of the
CA occlusion with residual stump opacified several centimeters from the
arly arterial phase) showing collateral filling of right ECA back to carotid
ICA area through PcomA was also noted. Lower right: vertebral injection
vical ICA up to cavernous portion through vertebral muscular branch-ECA-
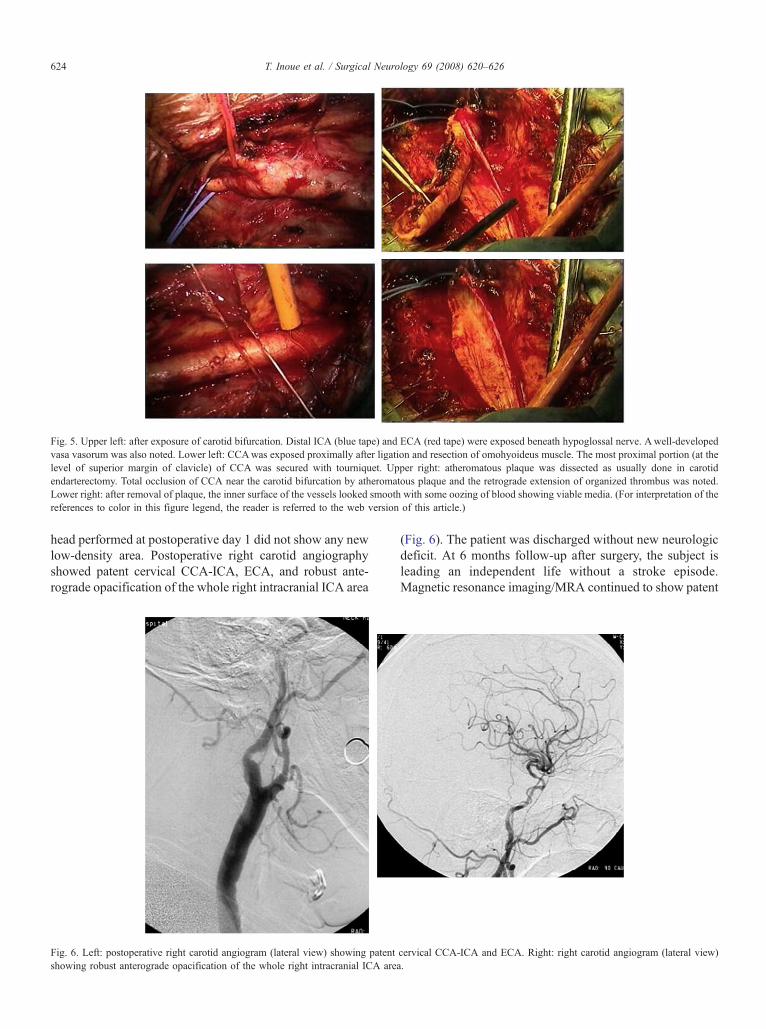
Fig. 5. Upper left: after exposure of carotid bifurcation. Distal ICA (blue tape) and ECA (red tape) were exposed beneath hypoglossal nerve. Awell-developed
vasa vasorum was also noted. Lower left: CCAwas exposed proximally after ligation and resection of omohyoideus muscle. The most proximal portion (at the
level of superior margin of clavicle) of CCA was secured with tourniquet. Upper right: atheromatous plaque was dissected as usually done in carotid
endarterectomy. Total occlusion of CCA near the carotid bifurcation by atheromatous plaque and the retrograde extension of organized thrombus was noted.
Lower right: after removal of plaque, the inner surface of the vessels looked smooth with some oozing of blood showing viable media. (For interpretation of the
references to color in this figure legend, the reader is referred to the web version of this article.)
T. Inoue et al. / Surgical Neurology 69 (2008) 620–626624
head performed at postoperative day 1 did not show any new
low-density area. Postoperative right carotid angiography
showed patent cervical CCA-ICA, ECA, and robust ante-
rograde opacification of the whole right intracranial ICA area
Fig. 6. Left: postoperative right carotid angiogram (lateral view) showing patent
showing robust anterograde opacification of the whole right intracranial ICA are
(Fig. 6). The patient was discharged without new neurologic
deficit. At 6 months follow-up after surgery, the subject is
leading an independent life without a stroke episode.
Magnetic resonance imaging/MRA continued to show patent
cervical CCA-ICA and ECA. Right: right carotid angiogram (lateral view)
a.

Fig. 7. Left and upper right: cervical MRA (left) and intracranial MRA (upper right) obtained at 6 months follow-up (after surgery) showing still patent right
CCA-ICA flow. Lower right: T2-weighted MRIs (6 months after the operation) showing no new ischemic lesion.
T. Inoue et al. / Surgical Neurology 69 (2008) 620–626 625
right CCA-ICA without the evidence of new ischemic
lesions (Fig. 7).
3. Discussion
Although the symptomatic CCA occlusion is a rare
condition, it is associated with poor prognosis due to very
restricted carotid collateral flow [2]. In the treatment of
progressive ischemia cases, the difficulty of using ipsilateral
ECA as surgical revascularization source raises a strategic
dilemma. Riles et al [7] have classified CCA occlusion into
4 types: type 1A, CCA occlusion with patent distal ICA and
ECA; type 1B, CCA occlusion with patent ECA only; type
1C, CCA occlusion with patent ICA only; type 2, complete
occlusion of the CCA-ICA-ECA. Various surgical revascu-
larizations for type 1 CCA occlusion have been reported,
mainly using extrathoracic-cervical bypass including SA to
ICA, SA (or transverse cervical artery, thyrocervical trunk)
to ECA with or without STA-MCA bypass [1,3,5,6].
However, direct carotid endarterectomy for CCA occlusion
to achieve primary restoration of CCA-ICA flow seems to
have been rarely performed and has not been well discussed.
If the conditions are well delineated, in which successful
restoration of primary CCA-ICA flow is safely achieved
with long-term patency, direct carotid endarterectomy would
be easier compared to previously mentioned complex
bypass procedures.
In these 2 cases, we noted 3 key issues to judge if the
primary carotid endarterectomy for CCA occlusion is
possible preoperatively and during surgical procedure. First,
we need to evaluate the patency of distal ICA. In case 2,
preoperative vertebral angiogram showed patent both distal
ECA and ICA (Riles type 1A). However, in case 1,
preoperative vertebral angiogram demonstrated only retro-
grade ECA filling as proximal as occipital artery, although
the ipsilateral retrograde cavernous to petrous ICA opaci-
fication was noted through cross-flow in delayed arterial
phase of contralateral carotid injection. Therefore, in the
preoperative evaluation, we could determine that at least still
patent ECA back to near carotid bifurcation, however, were
uncertain as for the distal ICA patency. During surgery, by
confirming substantial back flow from small arteriotomy in
distal carotid ICA, we could determine the patency of distal
ICA for certain. In the series of carotid endarterectomy for
ICA occlusion (with patent CCA and ECA), the retrograde
reflux visualization of occluded ICA back to the cavernous

T. Inoue et al. / Surgical Neurology 69 (2008) 620–626626
portion or further back to the petrous portion in preoperative
angiography has been associated with 50% and 71%
successful reopening of ICA, respectively [4]. Second, we
need to secure bsoundQ proximal CCA end. In the 2 cases,
preoperative angiography showed still opacified CCA
stump several centimeters from innominate artery, and
during operation, bsoundQ proximal CCA, which was
externally soft on palpation and with internally thin enough
intima after removal of plaque, was obtained by extending
the skin incision up to the superior margin of the clavicle
and splitting the omohyoideus muscle. If the organized
occlusion of CCA extends as far as its origin, the application
of direct carotid endarterectomy would be limited. In
addition, we need to consider the occluded side because
right CCA origin (innominate artery) is easier to access than
left CCA origin (aorta). Because the present 2 cases were
both right-side occlusion, we were able to secure the
proximal end relatively easily based on the several-
centimeter stump in preoperative angiography. In the left-
side case, a longer residual stump that extends at least above
the superior margin of clavicle would be needed to secure
the proximal end. Third, the condition of adventitia and
media across the occluded CCA before and after removal of
atheromatous plaque as well as organized thrombus need to
be evaluated during the operation to obtain a safe and long-
term patency. In both cases, enough vasa vasorum was
obvious externally after exposure of occluded CCA showing
bsoundQ adventitia and, internally, some oozing of blood
from media was noted after removal of plaque across
completely occluded portion.
In conclusion, direct carotid endarterectomy for CCA
occlusion to restore primary CCA-ICA flow is possible, and
good midterm patency as well as neurologic results can be
expected, although several special conditions need to be
evaluated preoperatively and during the procedure.
References
[1] Kobayashi T, Houkin K, Ito F, Kohama Y. Transverse cervical artery
bypass pedicle for treatment of common carotid artery occlusion: new
adjunct for revascularization of the internal carotid artery domain.
Neurosurgery 1999;45:299 -302.
[2] Levine SR, Welch KMA. Common carotid artery occlusion. Neurology
1989;39:178-86.
[3] Martin III RS, Edwards WH, Mulherin JL, Edwards Jr WH. Surgical
treatment of common carotid artery occlusion. Am J Surg
1993;165:302 -6.
[4] McCormick PW, Spetzler RF, Bailes JE, Zabramski JM, Frey JL.
Thromboendarterectomy of the symptomatic occluded internal carotid
artery. J Neurosurg 1992;76:752-8.
[5] Melgar MA, Sahni D, Weinand M. Throcervical trunk-external carotid
artery bypass for positional cerebral ischemia due to common carotid
artery occlusion. Technical note. J Neurosurg 2005;103:170 -5.
[6] Rabb CH, Moneta GL. Staged cerebral revascularization in a patient
with an occluded common carotid artery. Stroke 2005;36:e68-e70.
[7] Riles TS, Imparato AM, Posner MP, Eikelboom BC. Common
carotid occlusion. Assessment of the distal vessels. Ann Surg 1984;
199:363-6.
Commentary
This is a nice compilation of 2 cases, emphasizing what I
believe are still highly selective cases, where diagnostic
intra-arterial angiography is essential to document patent
arterial systems, and to craft revascularization procedures to
the angioarchitecture defined. This rare syndrome was
expertly managed by common carotid endarterectomy and
restoration of flow, with primary CCA repair. One would
expect, as the authors have demonstrated, long-term patency
from this operative approach. It is also of note that, with the
watershed infarct in patient 1, significant attention to
postoperative blood pressure management is essential,
because the risk of hyperperfusion and its intracranial
complications is a concern. I would also add, although the
authors did not cover this in their discussion, that a series of
Fogarty catheters can be quite useful in this scenario,
particularly if the common carotid origin is out of view and
accessibility in the operative field. Neurosurgeons would do
well to continue using intra-arterial angiography in select
cases, to tailor restoration of flow, to what the patient’s
angioarchitecture requires. The authors should be congrat-
ulated for bringing it to our attention again.
John L.D. Atkinson, MD
Department of Neurosurgery
Mayo Clinic
Rochester, Minnesota 55905, USA