disclaimer - anestesiar.org · patients are able to resume rest when not stimulated1 cooperative...
TRANSCRIPT

Disclaimer
The content for this deck was developed independently of the commercial supporter. All materials are included with permission. The opinions expressed are those of the collective faculty and are not to be construed as those of the publisher or grantor.
CME/CE accreditation is applied to the live educational activity. You are required to participate in a scheduled live activity to receive CME/CE credit. If you have not already done so, please register online www.accessCME.org, choose Live Event and select the corresponding activity.
Readers are advised that one or more presentations in this deck may contain references to unapproved or unlabeled uses of drugs or devices. Participants should note that the use of these agents outside current approved labeling is considered investigational and are advised to consult current prescribing information for these products.
Educational PurposeThis curriculum deck will update readers on recent advances regarding the use of analgesia and sedation in acute care settings.
Learning ObjectivesUpon completion of this activity, participants should be able to
Describe the rationale for the use of analgesia and sedation in acute care settingsCompare the current analgesics and sedatives, and assess their benefits and limitationsReview the clinical study evidence supporting the use of currentagents for acute care sedation and analgesiaDiscuss the rationale for pharmacoeconomic analyses of therapeutic agents in various acute care settings
Program Overview
General Anesthesia and Sedation BackgroundComfort Care in the Acute Care SettingOverview of Current Sedative and Analgesic AgentsDexmedetomidinePharmacoecononmic DataNeurological EffectsPediatric ApplicationsDexmedetomidine in Bariatric SurgeryAlgorithmsSummary

General Analgesia and
Sedation Background
Purpose of Analgesia and Sedation in Acute Care Settings
Provide adequate pain control1Optimize safety for patients and their caregivers2
Enhance patient comfort1Facilitate mechanical ventilation3
Reduce anxiety1
Prevent delirium1
Induce sleep when required1
Induce appropriate level of amnesia3
1Ely EW, et al. JAMA. 2003;289:2983-2991.2Blanchard AR. Postgrad Med. 2002;111:59-74.
3Kress JP, et al. Am J Respir Crit Care Med. 2002;166:1024–1028.

Need for Analgesia and Sedation in Acute CarePhysiological and Neurobehavioral Considerations
• Failure to address pain in acute care patients may lead to– Agitation and anxiety– Hypermetabolic states – Increased endogenous catecholamine activity – Myocardial ischemia
• Acute care patients may demonstrate periods of disorientation during which psychotic behavior occurs
• Certain types of sedation can reduce the risk of harm to the patient or others
Kress JP, et al. Am J Respir Crit Care Med. 2002;166:1024–1028.
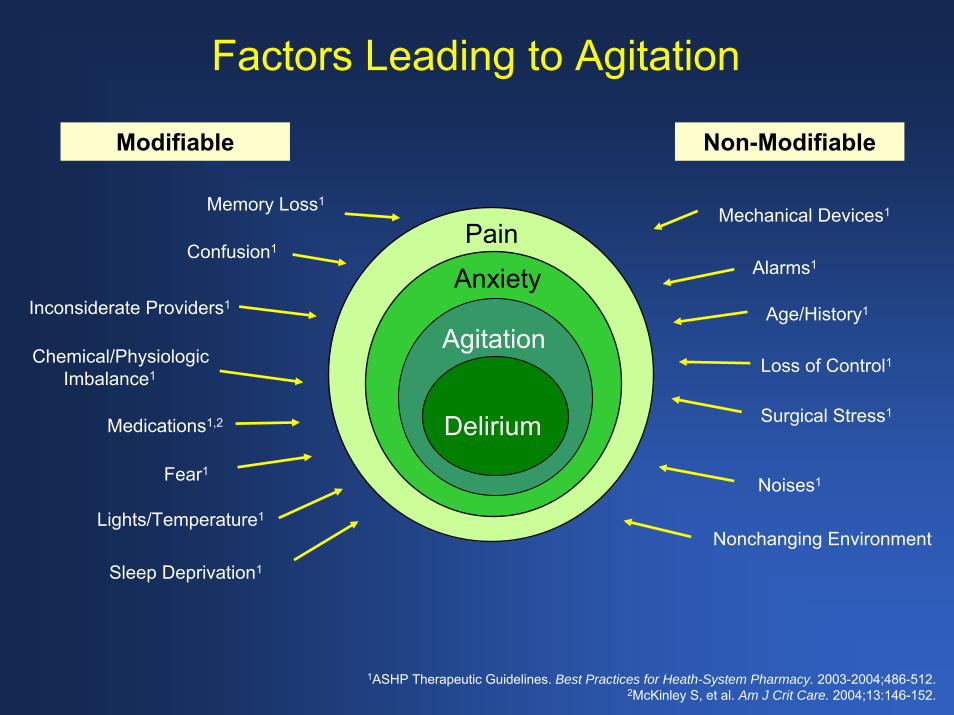
Factors Leading to Agitation
Modifiable Non-Modifiable
Inconsiderate Providers1
Alarms1
Lights/Temperature1
Mechanical Devices1
Loss of Control1
Nonchanging Environment
Sleep Deprivation1
Noises1
Memory Loss1
Confusion1
Fear1
Medications1,2 Surgical Stress1
Chemical/PhysiologicImbalance1
Pain
Anxiety
Agitation
Delirium
Age/History1
1ASHP Therapeutic Guidelines. Best Practices for Heath-System Pharmacy. 2003-2004;486-512.2McKinley S, et al. Am J Crit Care. 2004;13:146-152.

Goals of Sedation and Analgesia
Optimize safety for acute care patients and their caregivers1,2
Relieve pain and anxiety1-3
Attenuate the harmful adrenergic response1,2
Improve compliance with care1,2
Facilitate communication with caregivers and family members1,2
Avoid or reduce delirium1,2,4
1Blanchard AR. Postgrad Med. 2002;111:59-74.2Jacobi J, et al. Crit Care Med. 2002;30:119-141.
3Dasta JF, et al. Pharmacotherapy. 2006;26:798-805.4Ely EW, et al. JAMA. 2004;291:1753-1762.
Characteristics of an Ideal Sedative
Rapid onset of action allows rapid recovery after discontinuation1
Effective at providing adequate sedation with predictable dose response1,2
Easy to administer1,3
Lack of drug accumulation1
Few adverse effects1-3
Minimal adverse interactions with other drugs1-3
Cost effective3
Predictable dose response2
Promotes natural sleep4
1Ostermann ME, et al. JAMA. 2000;283:1451-1459. 2Jacobi et al. Crit Care Med. 2002;30:119-141.
3Dasta JF, et al. Pharmacotherapy. 2006;26:798-805..4Nelson LE, et al. Anesthesiology. 2003;98:428-436.

Targeting Patient Comfort
Oversedation
Undersedation
On-target sedation:Decreases weaning period1
Is not associated with muscular atrophy1
Decreases LOS and cost2Provides cardiovascular1
and intraoperative hemodynamic stability3
Improves patient safety1,3
Facilitates neurological assessment3
On-Target
Sedation
1McGaffigan PA. Crit Care Nursing. 2002;Feb Suppl:29-36.2Dasta et al. Pharmacotherapy. 2006;26:798-805.
3Arbour R. Am J Crit Care Nursing. 2004;13:66-73.

Importance of Optimizing Levels of Sedation
Undersedation OversedationAnxiety1 Prolonged weaning3
Ventilator dysynchrony2 Respiratory depression4
Dislodging invasive lines/ devices1
Lack of patient cooperation for assessment and therapeutic measures1
May increase posttraumatic stress syndrome1
Inability to communicate with health care providers or family members1
Increased O2 consumption1 Delirium2
Delirium2 Hypoactivity1
Hyperactivity1
Minimal amnesia2
1McGaffigan PA. Crit Care Nursing. 2002;Feb Suppl:29-36.2ASHP Therapeutic Guidelines. Best Practices for Heath-System Pharmacy. 2003-2004;486-512.
3Carrasco G. Crit Care. 2000;4:217–225.4Blanchard AR. Postgrad Med. 2002;111:59-74.
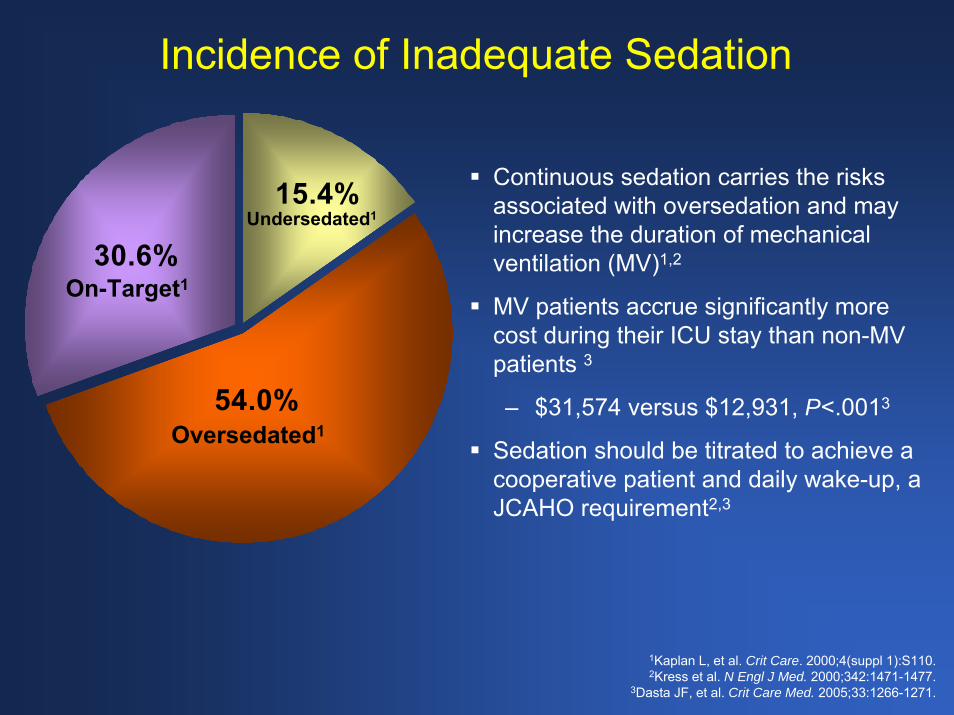
Incidence of Inadequate Sedation
15.4%
30.6%
54.0%
Undersedated1
Oversedated1
On-Target1
Continuous sedation carries the risks associated with oversedation and may increase the duration of mechanical ventilation (MV)1,2
MV patients accrue significantly more cost during their ICU stay than non-MV patients 3
– $31,574 versus $12,931, P<.0013
Sedation should be titrated to achieve a cooperative patient and daily wake-up, a JCAHO requirement2,3
1Kaplan L, et al. Crit Care. 2000;4(suppl 1):S110.2Kress et al. N Engl J Med. 2000;342:1471-1477.
3Dasta JF, et al. Crit Care Med. 2005;33:1266-1271.
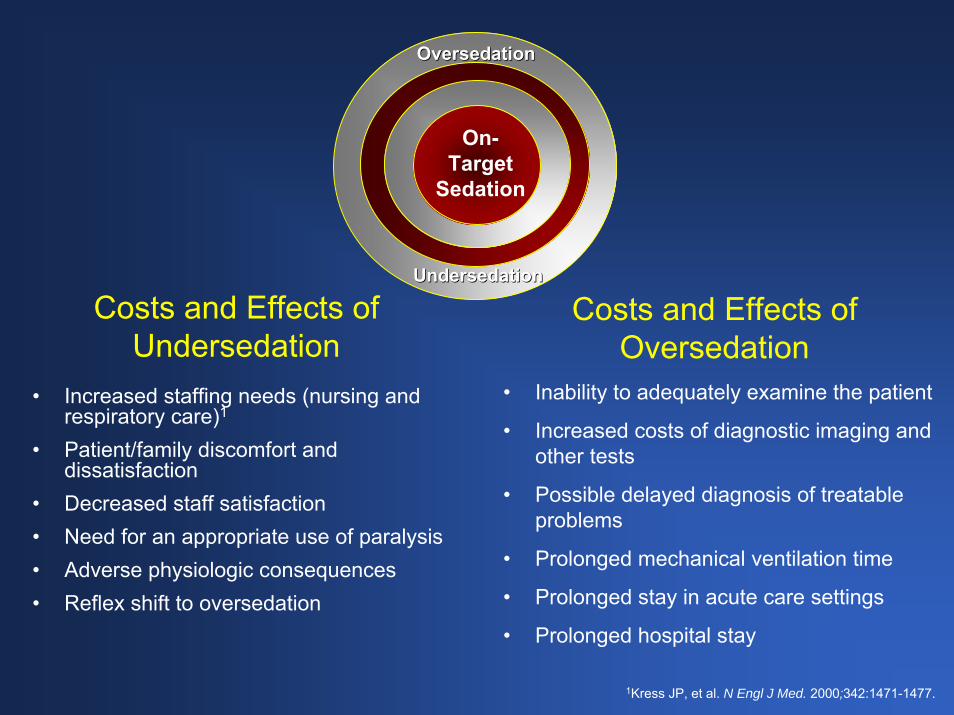
Costs and Effects of Undersedation
• Increased staffing needs (nursing and respiratory care)1
• Patient/family discomfort and dissatisfaction
• Decreased staff satisfaction• Need for an appropriate use of paralysis• Adverse physiologic consequences• Reflex shift to oversedation
• Inability to adequately examine the patient
• Increased costs of diagnostic imaging and other tests
• Possible delayed diagnosis of treatable problems
• Prolonged mechanical ventilation time
• Prolonged stay in acute care settings
• Prolonged hospital stay
Costs and Effects of Oversedation
On-Target
Sedation
OversedationOversedation
UndersedationUndersedation
1Kress JP, et al. N Engl J Med. 2000;342:1471-1477.
Guidelines and Standards
JCAHO Standards 2002 SCCM GuidelinesAnesthesia Patient Safety FoundationASA GuidelinesInstitute of Medicine

Comfort Care in the
Acute Care Setting
Assessing Pain
Faces Pain Rating Scale1
Visual Analog Scale (VAS)1
Pain questionnaire1
– Qualitative aspects1
Sympathetic response to pain1
1Jacox A, et al. Management of Cancer Pain. AHCPR publication 94-0592. 1994.
Assessing Sedation
Ramsay Sedation Scale
Observer’s Assessment of Alertness/Sedation Scale (OAA/SS)
Motor Activity Assessment Scale (MAAS)
Riker’s Sedation-Agitation Scale (SAS)
Richmond Agitation-Sedation Scale (RASS)
Brain function monitoring
Assessing Anxiety and Delirium
State-Trait Anxiety Inventory (STAI)1
Hamilton Rating Scales for Depression and Anxiety2
The Hospital Anxiety and Depression Scale3
Linear Analog Anxiety Scale4
Surrogate markers of stress response5
The Confusion Assessment Method for the Diagnosis of Delirium in the ICU (CAM-ICU)6
1Shedletsky R, et al. J Pers. 1974;42:511-527.2Hamilton M. Br J Soc Clin Psychol. 1967;6:278-296.
3Zigmond, AS, et al. Acta Psychiatr Scand. 1983;67:361-370. 4Sriwatanakul K, et al. Clin Pharmacol Ther. 1983;34:234-239.
5Lewis KS, et al. Am J Hosp Pharm. 1994;51:1539-1554.6 Ely EW, et al. Crit Care Med. 2001; 29:1370–1379.

Characteristics of Cooperative Sedation
In cooperative sedation, patients easily transition from sleep to wakefulness and task performance when aroused1
Patients are able to resume rest when not stimulated1
Cooperative sedation is most useful during procedures in which communication with the patient must be maintained1
Facilitates participation in therapeutic maneuvers2
Allows for patient interaction in care decisions2
May contribute to shorter recovery room convalescence3
Reduces risk of developing drug-induced complications3
1Bekker AY, et al. Neurosurgery. 2005;57(1 Suppl 1):1-10.2Burns AM, et al. Drugs. 1992;43:507-515.
3Sedation. Encyclopedia of Medicine. Ed. Jacqueline L. Longe. Thomson Gale, 2002. eNotes.com. 2006. 6 Mar, 2006 http://health.enotes.com/medicine-encyclopedia/sedation
Examples of Cooperative Sedation
Allows for accurate evaluation of the neuropsychological status of mechanically ventilated patients1
Facilitates direct evaluation of cerebral perfusion during carotid endarterectomy2
Patients are comfortable and responsive during cortical mapping2
1Bekker AY, et al. Neurosurgery. 2005; 57(1 Suppl):1-10. 2Ard JL, et al. Surgical Neurology. 2005;63:114-117.

Negative Outcomes Associated With Poor Cooperative Sedation
Pain that is not communicated in acute care settings can result in1
– Increased stress response– Guarding of muscles and muscle rigidity around
area of pain, leading to pulmonary dysfunction– Exhaustion and disorientation– Poor patient cooperation
Inability to assess patients can result in– Increased number of diagnostic tests– Increased time on ventilator– Increased LOS– Increased overall costs
1Jacobi J, et al. Crit Care Med. 2002;30:119-141.
Institutional Effects of Implementing Rational Use Guidelines
Prospective analysis of 156 ICU patients who required mechanical ventilation and continuous analgesia, sedation, and/or neuromuscular blockade1
One group (n = 84) was tracked after guidelines were implemented1
Length of hospital and ICU stay and duration of mechanical ventilation were all shorter in the guidelines group1
Institution of the guidelines led to a decline in mean drug costs across all drug classes studied1
1Mascia MF, et al. Crit Care Med. 2000;28:2300-2306.

Implementation of Clinical PathwaysClinical Outcome and Cost Burden
Large-scale implementation project with comparison to historic controls1
Outcomes management study including evidence-based clinical pathways and protocols for weaning acute care patients1
Participants included 595 pre-outcomes management patients and 510 post-outcomes management patients mechanically ventilated for >3 consecutive days1
1Burns SM, et al. Crit Care Med. 2003;31:2752-2763.

Implementation of Clinical PathwaysClinical Outcome and Cost Burden (Cont’d)
Significant differences in clinical outcomes were demonstrated between the 2 groups1
– Decreased ventilator duration by 1 day (P=.0001)1
– ICU stay reduced by 3 days (P=.0008)1
– Hospital length of stay reduced by 2 days (P=.0001)1
– Mortality rate declined from 38% to 31% (P=.02)1
More than $3 million cost savings were realized in the OM group1
1Burns SM, et al. Crit Care Med. 2003;31:2752-2763.

Overview of Current Sedative and
Analgesic Agents

Overview of Current Sedative and Analgesic Agents
Drug Class Examples Year FDA Approved
Opioids Morphine Prior to 1938Fentanyl 1968
Butyrophenones Haloperidol 1967
Sedatives/hypnotics Propofol 1989α2 Agonists Clonidine 1986
Benzodiazepines Diazepam 1963Lorazepam 1963Midazolam 1985
Dexmedetomidine 1999
http://www.fda.gov/cder/ob/default.htm
Opioids
Clinical EffectsAnalgesia1
Sedation1
1Harvey MA. Am J Crit Care. 1996;5:7-16.2Wagner BKJ, et al. Clin Pharmacokinet. 1997;33:426-453.
3Dean AJ, et al. J Psychiatry Neurosci. 2006;31:38-45.4Gerra G, et al. Drug Alcohol Depend. 2004;75:37-45.
MorphineFentanyl
Adverse EffectsRespiratory depression1,2
Hypotension1,2
Bradycardia1,2
Constipation1
Tolerance1
Withdrawal symptoms1,2
Dysphoria3,4
Haloperidol
Clinical Effects
Hypnotic agent with antipsychotic properties1
– For treatment of delirium in critically ill adults1
Does not cause respiratory depression1
1Harvey MA. Am J Crit Care. 1996;5:7-16.2Crippen DW. Crit Care Clin. 1990;6:369-392.
FO
NOH
CI
Haloperidol
Adverse Effects
Dysphoria2
Adverse CV effects include QT interval prolongation, extrapyramidal symptoms, neuroleptic malignant syndrome (rare)1
Metabolism altered by drug-drug interactions2
Benzodiazepines Lorazepam
Clinical EffectsSedation, anxiolysis, and amnesia1
Commonly used for long-term sedation2
Adverse EffectsSlower onset of action than midazolam2,3
Metabolic Acidosis (propylene glycol toxicity)4,5
Retrograde and anterograde amnesia can exceed desirability6
Delirium7
1Lerch C, et al. Br Med Bull. 1999;55:76-95. 2Shafer A. Crit Care Med. 1998;26:947-956.
3Wagner BKJ, et al. Clin Pharmacokinet. 1997;33:426-453.4Neale BW, et al. Ann Pharmacother. 2005;39:1732-1736.
5Wilson KC, et al. Chest. 2005;128:1674-1681.6Mathew A, et al. Psychpharmacol. 2002;16:345-354.
7Pandharipande P, et al. Anesthesiology. 2006;104:21-26.
BenzodiazepinesMidazolam
Clinical EffectsSedation, anxiolysis, and amnesia1
Rapid onset of action intravenously1
1Blanchard AR. Postgrad Med. 2002;111:59-74.2Harvey MA. Am J Crit Care. 1996;5:7-16.
3Shafer A. Crit Care Med. 1998;26:947-956. 4Midazolam [package insert]. Weston, FL: Apotex Corp; 2000.
Adverse EffectsMay accumulate in liver and/or renal failure1
Anterograde amnesia2
Prolonged recovery after long-term use3
Combination with opioids increases hypotensive effects1
Respiratory depression4
Adverse hemodynamic events have been reported in pediatric patients with cardiovascular instability4

Propofol
Clinical EffectsSedation1
Hypnosis1
Anxiolysis1
Muscle relaxation1
↓ ICP1
↓ Cerebral metabolic rate1
Antiemetic2
Adverse EffectsRespiratory depression (exacerbated by opioids)1
Hypotension1
Decreased myocardial contractility3
Preservative issues4
Potential for infection4
Tolerance5
Propofol infusion syndrome6
↑ Serum triglycerides4
1Harvey MA. Am J Crit Care.1996;5:7-16.2Apfel CC, et al. Anaesthesist. 2005;54:201-9.
3Lerch C, et al. Br Med Bull. 1999;55:76-95.4Diprivan [package insert]. AstraZeneca Pharmaceuticals; 2004.
5Zapantis A, et al. Crit Care Nurs Clin N Am. 2005;17:211-223.6Riker RR, et al. Pharmacotherapy. 2005;25(5 Pt 2):8S-18S.
(CH3)2 CH CH (CH3)2
OH

α2 Agonists: Clonidine
Clinical EffectsAntihypertensive1,2
Analgesia1
Anxiolysis1
Sedation1
↓ Shivering1
N
N
H
N
Cl
Cl
Clonidine
Adverse EffectsBradycardia1
Dry mouth1
Hypotension3
1Kamibayashi T, et al. Anesthesiology. 2000;93:1345-1349; 2Catapres [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals Inc; 2004. 3Nishima K, et al. Anesthesiology. 2004;59:323-329.
α2 Agonists: Dexmedetomidine
Clinical EffectsAntihypertensive1,2
Sedative1,2
Analgesic1,2
↓ Shivering3
Anxiolytic effects4
Patient rousability4
Potentiates effects of opioids, sedatives, and anesthetics2
Decreased sympathetic activity5
Dexmedetomidine
CH3
CH3
N
N
CH3H
Adverse EffectsBradycardia6
Hypotension6
Dry mouth2
Vasoconstriction with rapid infusion or at high doses2
Nausea2
1Kamibayashi T, et al. Anesthesiology. 2000;93:1345-1349.2Precedex [package insert]. Lake Forest, IL: Hospira Inc; 2004.
3Doufas AG, et al. Stroke. 2003;34:1218-1223.4Riker RR, et al. Pharmacotherapy. 2005;25(5 Pt 2):8S-18S.
5Venn RA, et al. Brit J Anaesthesia. 2001;87:684-690.6Shehabi Y, et al. Intensive Care Med. 2004;30:2188-2196.
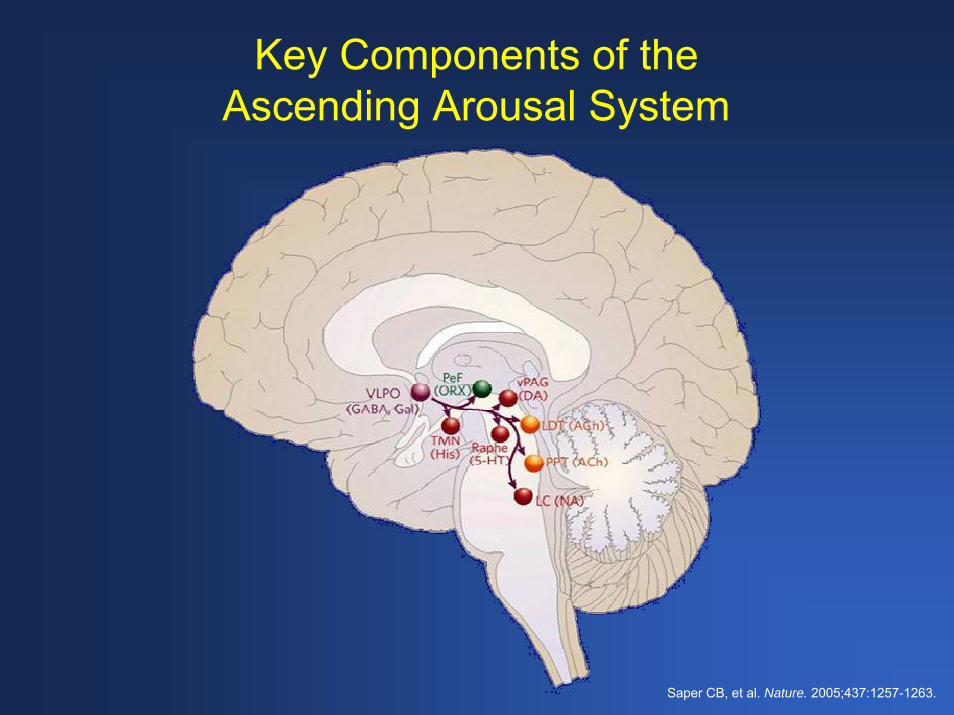
Saper CB, et al. Nature. 2005;437:1257-1263.
Key Components of theAscending Arousal System

Key Projections to theAscending Arousal System
Saper CB, et al. Nature. 2005;437:1257-1263.

“Switch” Mechanisms of Alertness and Sleep
Sleep
VLPOeVLPO
LCTMNRaphe
Awakea LC
TMNRaphe
VLPOeVLPO
ORX
On
ORXb
Off
Saper CB, et al. Nature. 2005;437:1257-1263.
Clinical Characteristics of Dexmedetomidine
Cooperative sedation1
Analgesia2,3
Organ Protection (ie, neural, renal, cardiac)1
Anxiolysis2,3
Controls hyperadrenergic response to stress1-3
Reduces shivering3
Diuretic action4
Mimics Natural Sleep1
1Aantaa R, et al. Drugs of the Future. 1993;18:49-56.2Kamibayashi T, et al. Anesthesiology. 2000;93:1345-1349. 3Wagner BKJ, et al. Clin Pharmacokinet. 1997;33:426-453.
4Goodman LS, et al. The Pharmacological Basis of Therapeutics. New York, NY: McGraw-Hill;2004:232-235.
Anxiolysis
α2B
X
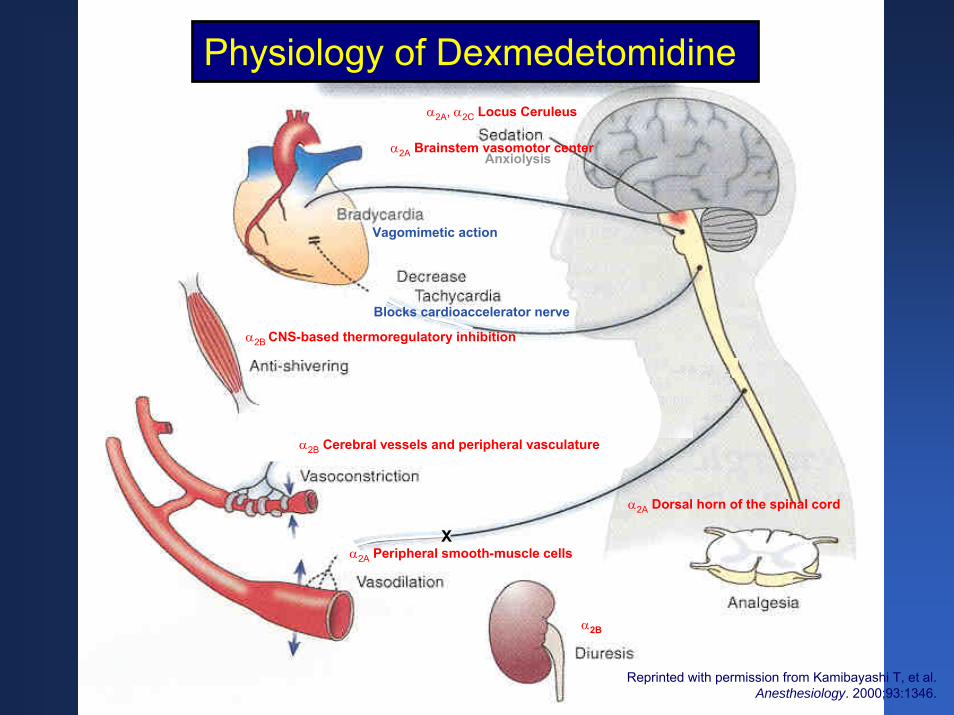
Physiology of Dexmedetomidine
Reprinted with permission from Kamibayashi T, et al. Anesthesiology. 2000;93:1346.
α2A, α2C Locus Ceruleus
α2B CNS-based thermoregulatory inhibition
α2B Cerebral vessels and peripheral vasculature
α2A Peripheral smooth-muscle cells
α2A Dorsal horn of the spinal cord
α2A Brainstem vasomotor center
Blocks cardioaccelerator nerve
Vagomimetic action

Comparison of Clinical EffectsBenzo-
diazepines Propofol Opioids Dexmedetomidine Haloperidol
Sedation X X X X X
Alleviate anxiety1,2 X X
Analgesic Properties1-4 X X
Promote arousability during sedation2-4
X
Facilitate ventilation during weaning2-4 X
No respiratorydepression1-4 X X
Control delirium1-4 X X
1Blanchard AR. Postgrad Med. 2002;111:59-74.2Kamibayashi T, et al Anesthesiology. 2000;95:1345-1349.
3Maze M. et al. Anesthetic Pharmacology: Physiologic Principals and Clinical Practice. Churchill Livingstone; 2004.4Maze M, et al. Crit Care Clin. 2001;4:881.
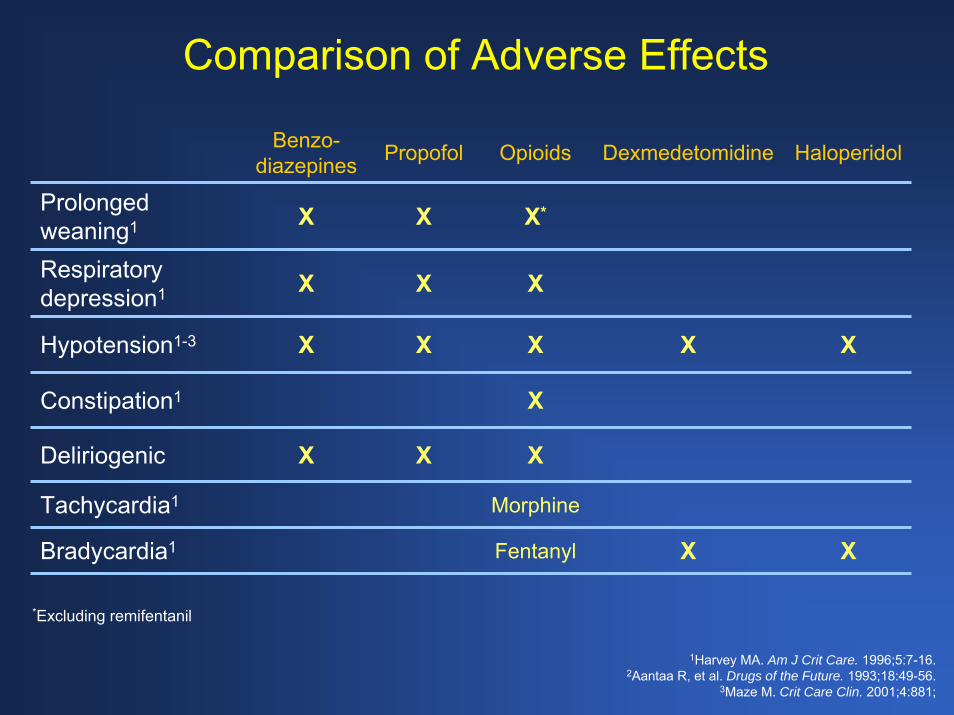
Comparison of Adverse Effects
Benzo-diazepines Propofol Opioids Dexmedetomidine Haloperidol
X*
X
Tachycardia1 Morphine
X
X
X
X
X
Fentanyl
Prolonged weaning1 X X
Respiratory depression1 X X
Hypotension1-3 X X X
Constipation1
Deliriogenic X X
Bradycardia1 X
*Excluding remifentanil
1Harvey MA. Am J Crit Care. 1996;5:7-16.2Aantaa R, et al. Drugs of the Future. 1993;18:49-56.
3Maze M. Crit Care Clin. 2001;4:881;
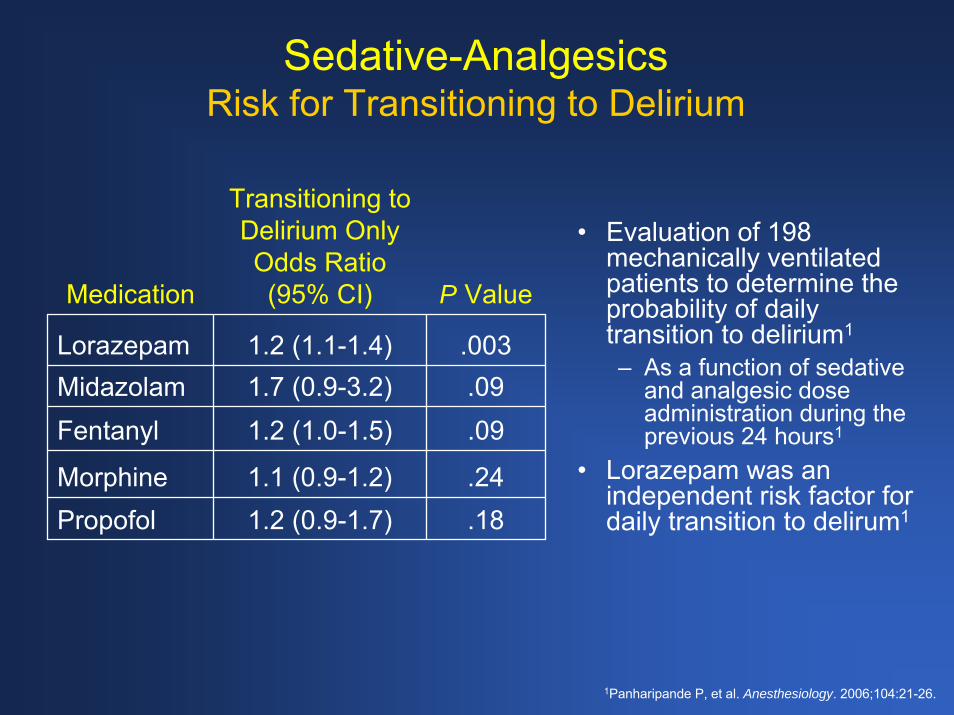
Sedative-AnalgesicsRisk for Transitioning to Delirium
• Evaluation of 198 mechanically ventilated patients to determine the probability of daily transition to delirium1
– As a function of sedative and analgesic dose administration during the previous 24 hours1
• Lorazepam was an independent risk factor for daily transition to delirum1
Medication
Transitioning to Delirium Only Odds Ratio (95% CI) P Value
Lorazepam 1.2 (1.1-1.4) .003Midazolam 1.7 (0.9-3.2) .09Fentanyl 1.2 (1.0-1.5) .09
Morphine 1.1 (0.9-1.2) .24Propofol 1.2 (0.9-1.7) .18
1Panharipande P, et al. Anesthesiology. 2006;104:21-26.
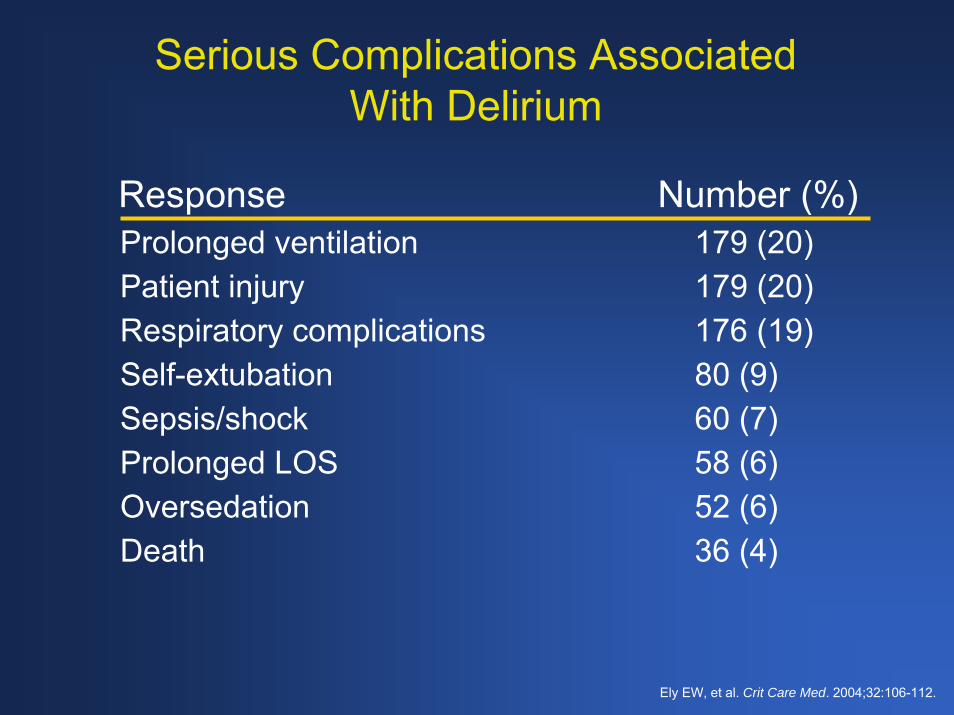
Serious Complications Associated With Delirium
Prolonged ventilation 179 (20)Patient injury 179 (20)Respiratory complications 176 (19)Self-extubation 80 (9)Sepsis/shock 60 (7)Prolonged LOS 58 (6)Oversedation 52 (6)Death 36 (4)
Response Number (%)
Ely EW, et al. Crit Care Med. 2004;32:106-112.
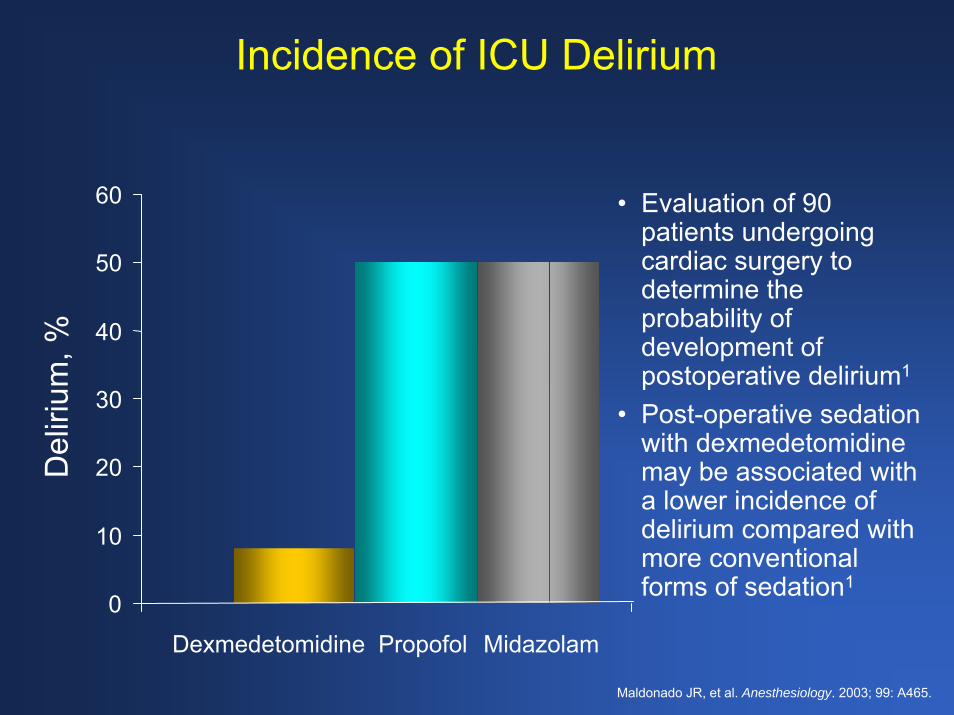
Incidence of ICU Delirium
60 • Evaluation of 90 patients undergoing cardiac surgery to determine the probability of development of postoperative delirium1
• Post-operative sedation with dexmedetomidine may be associated with a lower incidence of delirium compared with more conventional forms of sedation1
50
Del
irium
, % 40
30
20
10
0
Dexmedetomidine Propofol Midazolam
Maldonado JR, et al. Anesthesiology. 2003; 99: A465.
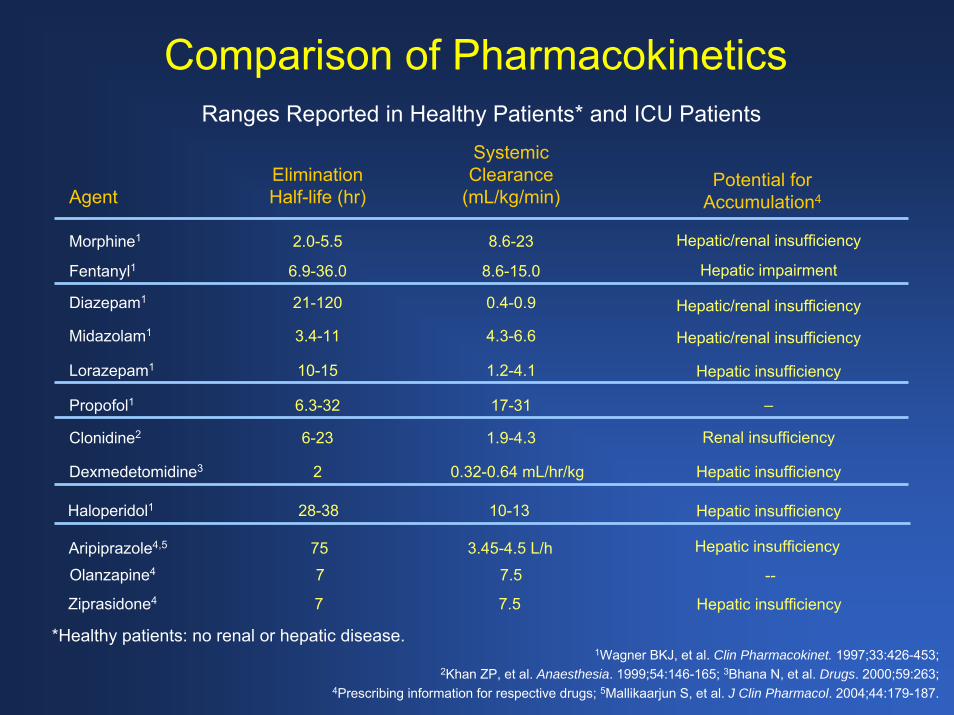
Comparison of PharmacokineticsRanges Reported in Healthy Patients* and ICU Patients
0.32-0.64 mL/hr/kg2Dexmedetomidine3
1.9-4.36-23Clonidine2
17-316.3-32Propofol1
1.2-4.110-15 Lorazepam1
4.3-6.63.4-11Midazolam1
0.4-0.921-120Diazepam1
8.6-15.06.9-36.0Fentanyl18.6-232.0-5.5Morphine1
10-1328-38Haloperidol1
Hepatic/renal insufficiency
Hepatic impairment
Hepatic/renal insufficiency
Hepatic/renal insufficiency
Hepatic insufficiency
Hepatic insufficiency
Hepatic insufficiency
Renal insufficiency
–
Systemic Clearance
(mL/kg/min)EliminationHalf-life (hr)Agent
Potential for Accumulation4
*Healthy patients: no renal or hepatic disease.
3.45-4.5 L/h75Aripiprazole4,5
7.57Olanzapine4 --
7.57Ziprasidone4 Hepatic insufficiency
Hepatic insufficiency
1Wagner BKJ, et al. Clin Pharmacokinet. 1997;33:426-453; 2Khan ZP, et al. Anaesthesia. 1999;54:146-165; 3Bhana N, et al. Drugs. 2000;59:263;
4Prescribing information for respective drugs; 5Mallikaarjun S, et al. J Clin Pharmacol. 2004;44:179-187.

Dexmedetomidine
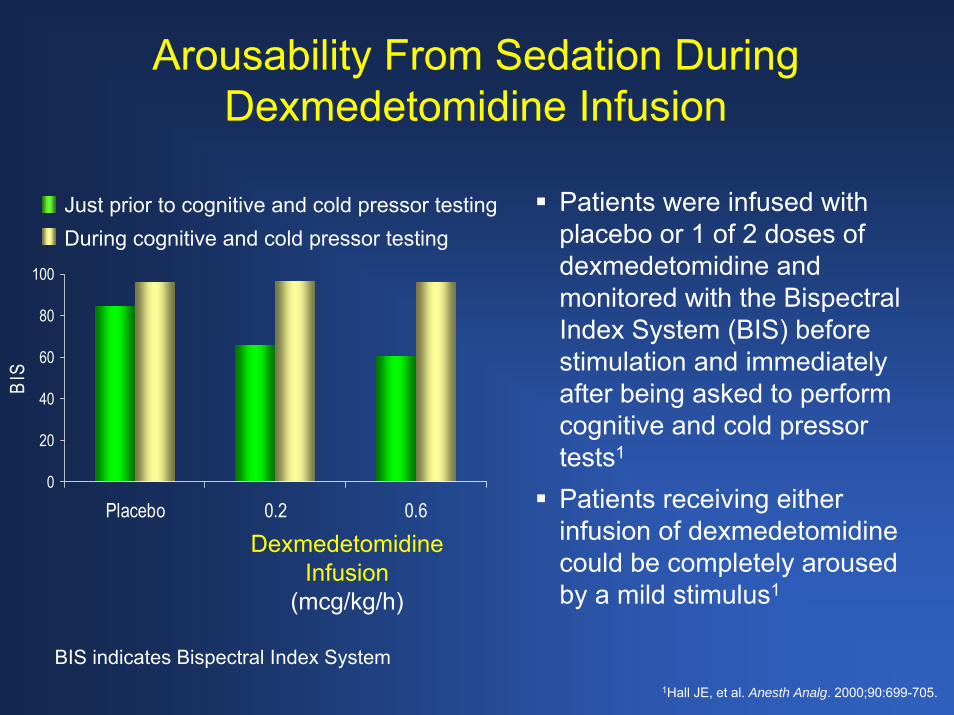
Arousability From Sedation During Dexmedetomidine Infusion
During cognitive and cold pressor testingJust prior to cognitive and cold pressor testing
Dexmedetomidine Infusion
(mcg/kg/h)
0
20
40
60
80
100
Placebo 0.2 0.6
BIS
Patients were infused with placebo or 1 of 2 doses of dexmedetomidine and monitored with the Bispectral Index System (BIS) before stimulation and immediately after being asked to perform cognitive and cold pressor tests1
Patients receiving either infusion of dexmedetomidine could be completely aroused by a mild stimulus1
BIS indicates Bispectral Index System1Hall JE, et al. Anesth Analg. 2000;90:699-705.

Comparison of Dexmedetomidine With Propofol
20 adult ICU patients were randomized to either dexmedetomidine or propofol1– Dexmedetomidine; 10-minute 2.5 mcg/kg/h
loading dose, 0.2-2.5 mcg/kg/h maintenance dose1
– Propofol; ≤1 mg/kg 10-minute loading dose (if required), 1-3 mg/kg/h maintenance dose1
Additional analgesia, if necessary, was provided by alfentanil1Depth of sedation was measured with RSS and BIS1
Dexmedetomidine and propofol produced an equivalent depth of sedation1
1Venn RM, et al. Br J Anaesth. 2001;87:684-690.

Predictable Effects on Heart Rate and Arterial Pressure
1Venn RM, et al. Br J Anaesth. 2001;87:684-690. 2Venn RM, et al. Br J Anaesth. 2001;86:650-656.
5060708090
100110120
0 1 2 3 4 5 6 7 8
Mea
n H
eart
Rat
e, b
eats
/min
+4 +8 +12 +16 +20 +24
40557085
100115130145160175
0 1 2 3 4 5 6 7 8Mea
n A
rteria
l Pre
ssur
e, m
m H
g
+4 +8 +12 +16 +20 +24
Sedative Discontinued
PropofolDexmedetomidine
HeartRate
SBP
DBP
Significantly lower heart rates in the dexmedetomidine group during intubation (P=.034) but not after sedative discontinuation (P=.15)1
− Predictable 10% decrease with plateau1
No significant differences in systolic and diastolic blood pressures (P=.60)1
Attenuates postoperative tachycardia2
Note: Reductions from baseline shown.

Postoperative Effects of Dexmedetomidine
0
10
20
30
40
100
VAS
Pain
Less
Pai
nM
ore
Pai
n PropofolDexmedetomidine
Improved postoperative pain and greater sedation with dexmedetomidine compared with propofol1
* †
0
40
60
80
100
VA
S S
edat
ion
Less
Ale
rtM
ore
Ale
rt
* †
Pre-surg
SurgEnd
5 35 50 6520
Time After Surgery, minutes
*P<.05 difference over time compared with baseline†P<.05 difference between groups
1Arain SR, et al. Anesth Analg. 2002;95:461-466.

Morphine-Sparing Effects in Inpatient Surgery
34 patients scheduled for inpatient surgery1
Randomized to either dexmedetomidine or morphine1
Agents were started 30 minutes before the end of surgery1
Dexmedetomidine reduced the early postoperative need for morphine by 66%1
0
2.5
5
7.5
10
12.5
Morphine Dexmedetomidine
Ave
rage
Tot
al M
orph
ine
Use
d, m
g
P<.01
0
2
4
6
8
10
12
0 10 20 30 40 50 60 70
Minutes in PACU
Cum
ulat
ive
Mor
phin
eU
sed,
mg
MorphineDexmedetomidine
P<.01
1Arain SR, et al. Anesth Analg. 2004;98:153-158.

Reduction of Postoperative Requirement for Epidural Opioids With Dexmedetomidine
Prospective, randomized, double-blind study with 28 patients scheduled for thoracotomy for wedge resection, lobectomy, or pneumonectomy1
Bupivacaine was administered in an acute care setting through a thoracic epidural, and patients were randomized to receive either IV placebo or IV dexmedetomidine (20-minute, 0.5 mcg/kg loading dose plus infusion of 0.4 mcg/kg/h)1
Supplemental analgesia (fentanyl), vital signs, and blood gasses were monitored1
1Wahlander S, et al. J Cardiothorac Vasc Anesth. 2005;19:630-635.
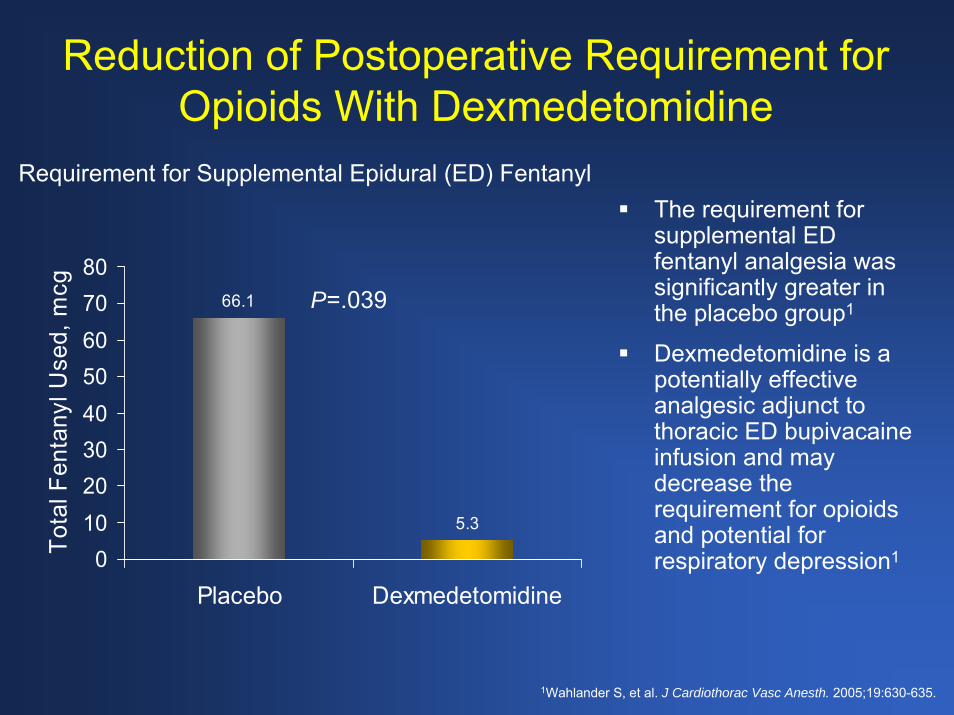
Reduction of Postoperative Requirement for Opioids With Dexmedetomidine
Requirement for Supplemental Epidural (ED) FentanylThe requirement for supplemental ED fentanyl analgesia was significantly greater in the placebo group1
Dexmedetomidine is a potentially effective analgesic adjunct to thoracic ED bupivacaine infusion and may decrease the requirement for opioids and potential for respiratory depression1
66.1
5.3
01020304050607080
Placebo Dexmedetomidine
Tota
l Fen
tany
l Use
d, m
cg P=.039
1Wahlander S, et al. J Cardiothorac Vasc Anesth. 2005;19:630-635.

Injury and Liability Associated With Monitored Anesthesia Care
Bhananker and colleagues assessed the patterns of injury and liability associated with monitored anesthesia care (MAC; n = 121) compared with general (n = 1519) and regional anesthesia (n = 312)The proportion of claims for death and permanent brain damage was reduced in regional anesthesia compared with MAC In contrast, the severity of injury was similar between MAC claims and those associated with general anesthesia
0
10
20
30
40
50
60
Death/Perm BrainDamage
Permanent Disabling Temp/Nondisabling
MAC General Regional
*
*
*
*
* P<.025 MAC versus Regional
Cla
ims
in A
nest
hesi
a G
roup
, %
Bhananker S, et al. Anesthesiology. 2006;104:228-34.
Injury and Liability Associated With Monitored Anesthesia Care (Cont’d)
Respiratory depression due to sedative, hypnotic, and/or analgesic overdose was responsible for 21% of MAC-related claims – 24% occurred during endoscopic procedures– Nearly 75% received a combination of two or more drugs
• Either a benzodiazepine and an opioid or propofol plus others
Death or brain damage resulted in most of the claims related to oversedationResolution of legal claims associated with oversedation cost an average of $254,000 per patient
Bhananker S, et al. Anesthesiology. 2006;104:228-34.

Pharmacoeconomic Data
Factors Affecting ICU Cost
ICU stays account for nearly a third of total inpatient costs1
High ICU costs may be due to mechanical ventilation (MV) and/or delirium1,2
Sedatives have the potential to prolong MV and may increase healthcare costs3,4
Incorporation of a daily sedation interruption policy into a medical ICU guideline can significantly reduce ICU stays and days of MV5
1Dasta JF, et al. Crit Care Med. 2005;33:1266-1271.2 Milbrant EB, et al. Crit Care Med. 2004;32:955-962.
3Ostermann ME, et al. JAMA. 2000;283:1451-1459.4MacLaren R, et al. Pharmacotherapy. 2005;25:1319-1328.
5Wittbrodt ET. Pharmacotherapy. 2005;25(5 Pt 2):3S-7S.

Limitations of Pharmacoeconomic Studies on Sedation
Small sample sizes1
Results not applicable to other clinical sites1
Too few have been conducted to date1
Most do not evaluate total cost1,2
1Ostermann ME, et al. JAMA. 2000;283:1451-1459.2MacLaren R, et al. Pharmacotherapy. 2005;25:1319-1328.

Pharmacoeconomic AnalysisOutcomes Analysis in Cardiac Surgery
12-month retrospective administrative claims database analysis (2003-2004)1
Nationally representative sample of 250 medical and surgical hospitals1
Comparison of patients receiving either midazolam plus propofol (M+P, n = 9996) or dexmedetomidine plus M+P (D+M+P, n = 356)1
– Patients who were admitted to the hospital for either a cardiovascular valve or vessel procedure1
– Patient demographics and outcomes were obtained from the hospital billing claim form, UB-921
Admissions with lengths of stay more than 100 days were excluded from all analyses
1Dasta JF, et al. Pharmacotherapy. 2006;26:798-805.
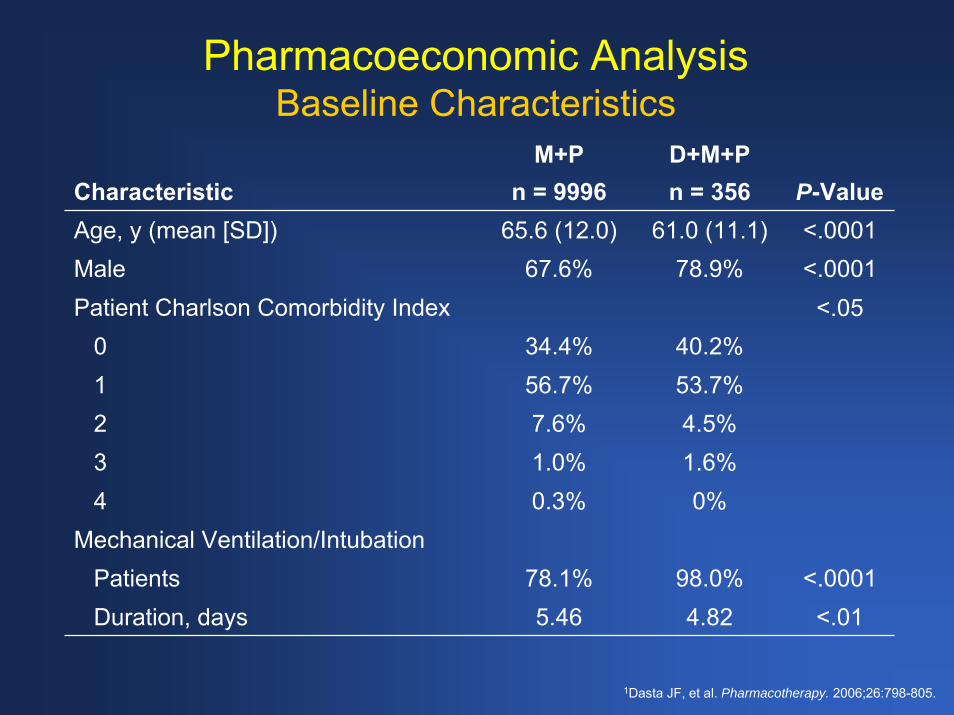
Pharmacoeconomic AnalysisBaseline Characteristics
CharacteristicM+P
n = 9996D+M+Pn = 356 P-Value
Age, y (mean [SD]) 65.6 (12.0) 61.0 (11.1) <.0001Male 67.6% 78.9% <.0001Patient Charlson Comorbidity Index <.05
0 34.4% 40.2%1 56.7% 53.7%2 7.6% 4.5%3 1.0% 1.6%4 0.3% 0%
Mechanical Ventilation/IntubationPatients 78.1% 98.0% <.0001Duration, days 5.46 4.82 <.01
1Dasta JF, et al. Pharmacotherapy. 2006;26:798-805.
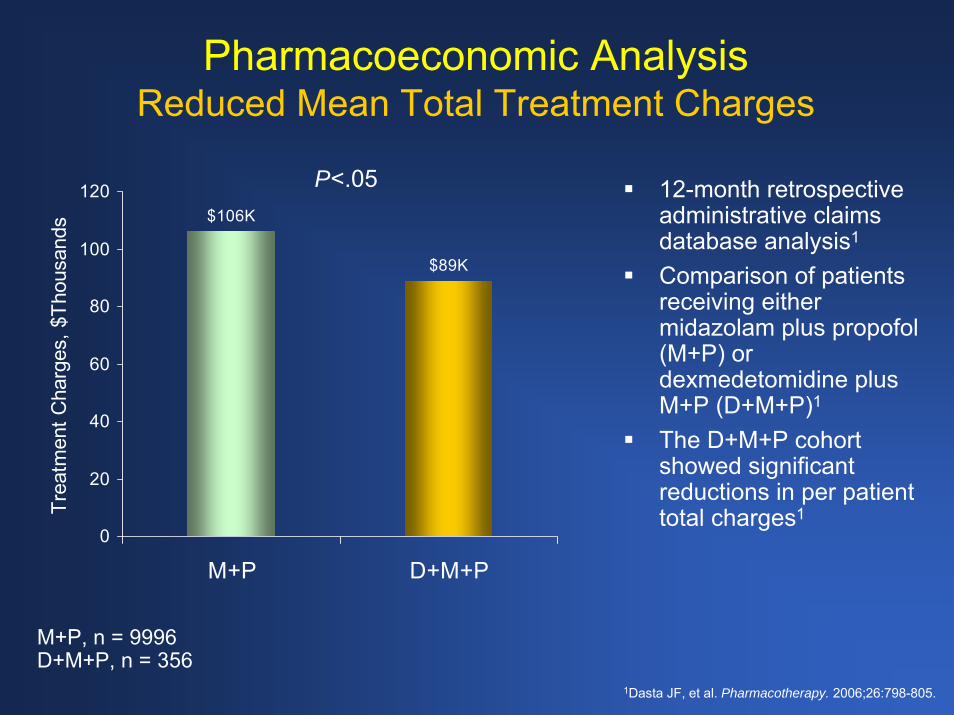
Pharmacoeconomic AnalysisReduced Mean Total Treatment Charges
$106K
$89K
0
20
40
60
80
100
120
M+P D+M+P
Trea
tmen
t Cha
rges
, $Th
ousa
nds
P<.05 12-month retrospective administrative claims database analysis1
Comparison of patients receiving either midazolam plus propofol (M+P) or dexmedetomidine plus M+P (D+M+P)1
The D+M+P cohort showed significant reductions in per patient total charges1
M+P, n = 9996D+M+P, n = 356
1Dasta JF, et al. Pharmacotherapy. 2006;26:798-805.

Pharmacoeconomic AnalysisDepartmental Treatment Charges
$17.7K
$2.8K
02468
101214161820
M+P D+M+P
Cha
rges
, $Th
ousa
nds P<.0001
ICU/CCU
$12.7K
$16.7K
02468
1012141618
M+P D+M+P
Cha
rges
, $Th
ousa
nds P<.0001
Pharmacy
$17.3K
$12.8K
02468
101214161820
M+P D+M+PC
harg
es, $
Thou
sand
s P<.0001Operating Room
$2.5K
$3.4K
0
1
2
3
4
M+P D+M+P
Cha
rges
, $Th
ousa
nds P<.0001
Anesthesia
M+P, n = 9996D+M+P, n = 356
Reductions in ICU and OR charges offset increases in other areas
1Dasta JF, et al. Pharmacotherapy. 2006;26:798-805.
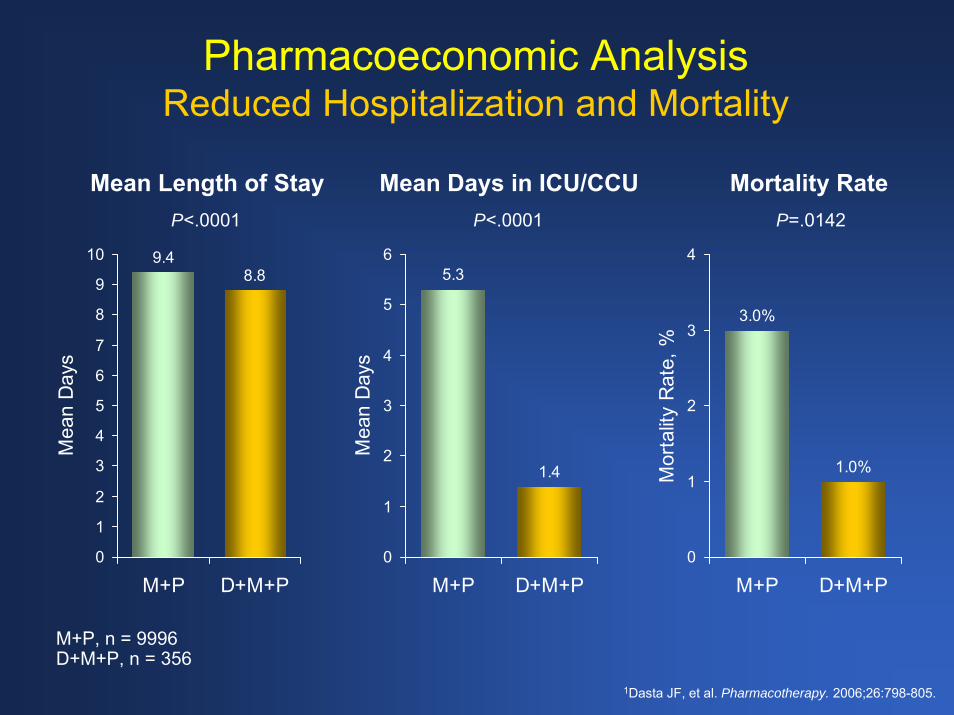
Pharmacoeconomic AnalysisReduced Hospitalization and Mortality
Mean Length of Stay Mean Days in ICU/CCU Mortality RateP<.0001 P<.0001 P=.0142
5.3
1.4
0
1
2
3
4
5
6
M+P D+M+P
Mea
n D
ays
9.48.8
0
1
2
3
4
5
6
7
8
9
10
M+P D+M+P
Mea
n D
ays
3.0%
1.0%
0
1
2
3
4
M+P D+M+P
Mor
talit
y R
ate,
%M+P, n = 9996D+M+P, n = 356
1Dasta JF, et al. Pharmacotherapy. 2006;26:798-805.

Pharmacoeconomic AnalysisReduced Charges, Hospitalization, and Mortality in
Patients With Cardiac Vessel Procedures
Mean Total Charges Mean Length of Stay Mortality Rate
$97K
$80K
0
20
40
60
80
100
120
M+P D+M+P
Cha
rges
, $Th
ousa
nds
P<.05 P<.01 P=.1074
8.98.1
0
1
2
3
4
5
6
7
8
9
10
M+P D+M+P
Mea
n D
ays
2.5%
1.0%
0
0.5
1
1.5
2
2.5
3
M+P D+M+P
Mor
talit
y R
ate,
%M+P, n = 7577D+M+P, n = 293
1Dasta JF, et al. Pharmacotherapy. 2006;26:798-805.

Pharmacoeconomic AnalysisStudy Limitations
DosageDuration of therapies Influence of practice patterns/institutional variability unknown Lack of randomization of patients to treatment introduced risk of selection or channeling biasAssigning causality based on results not possible1
1Dasta JF, et al. Pharmacotherapy. 2006;26:798-805.

Pharmacoeconomic AnalysisStudy Conclusions
Dexmedetomidine was added to standard sedative regimens (midazolam + propofol) under actual practice conditions1
Largest study measuring the pharmacoeconomic and clinical outcomes of any sedation agent in this populationPotential demonstrable clinical and economic benefits of including dexmedetomidine in sedation regimens1
– Addition of dexmedetomidine to the standard of care was associated with significant reductions in total LOS, stay in ICU/CCU, and mortality1
– Significantly lower total treatment charges1
1Dasta JF, et al. Pharmacotherapy. 2006;26:798-805.

Properties of Dexmedetomidine in Cardiovascular Surgery
Lack of respiratory depressionCooperative sedation aids in assessing neurophysiological function during vascular procedures such as endarterectomy Hemodynamic stabilization is desirable during cardiovascular surgeryAttenuates hypertension and tachycardia
Aantaa R, et al. Eur J Anaesthesiol. 2006;23:361-372.
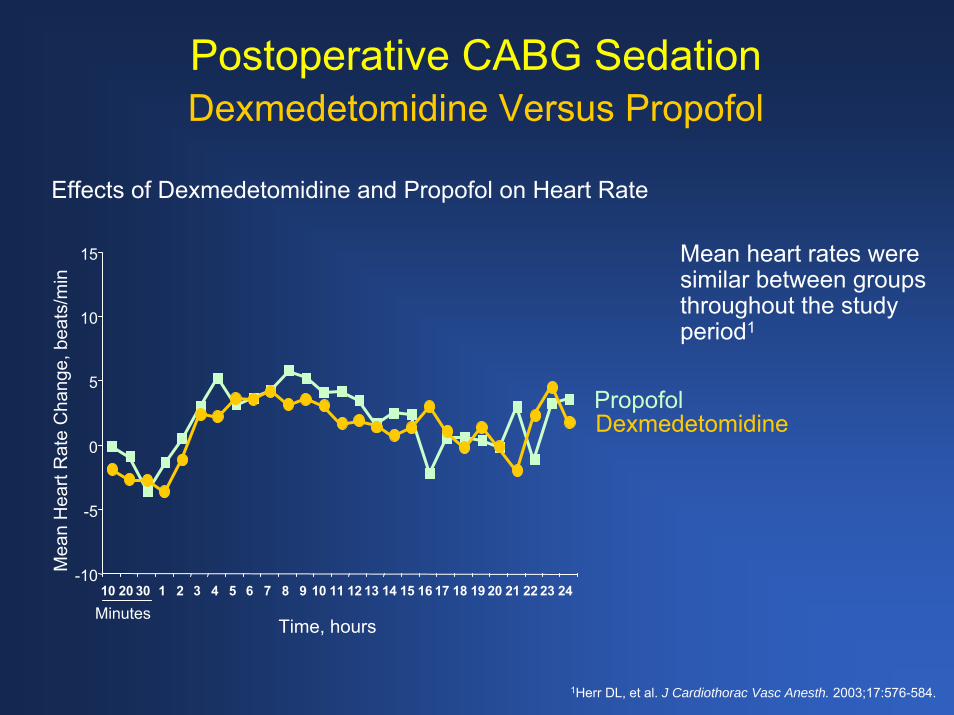
Postoperative CABG Sedation Dexmedetomidine Versus Propofol
Effects of Dexmedetomidine and Propofol on Heart Rate
Mean heart rates were similar between groups throughout the study period1
-10
-5
0
5
10
15
10 20 30 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Mea
n H
eart
Rat
e C
hang
e, b
eats
/min
Time, hoursMinutes
PropofolDexmedetomidine
1Herr DL, et al. J Cardiothorac Vasc Anesth. 2003;17:576-584.
Immediate Extubation Following Cardiac Surgery
Horswell et al conducted a study of immediate extubation after off-pump coronary artery bypass graft (OPCAB) in 514 patientsFollowing surgery, each patient received 2 or more of the following: epidural anesthesia, IV morphine on demand, IV ketorolac on schedule, and/or continuous IV dexmedetomidineAll patients were successfully extubated immediately after dressing applicationThe investigators concluded that immediate extubation of OPCAB patients is feasible and probably safe1
1Horswell JL, et al. J Cardiothorac Vasc Anesth. 2005;19:282-287.

Use of Perioperative Dexmedetomidine in Vascular Surgery
Significant between group changes from baseline for plasma epinephrine (P<.05) and norepinephrine (P<.001) Plasma norepinephrine concentrations were 2 to 3 times lower in the dexmedetomidine group at both tracheal extubation and at 60 min after arrival to PACU Plasma epinephrine concentrations were lower in the dexmedetomidine group only during tracheal extubation
1Talke P, et al. Anesth Analg. 2000;90:834-839.
Dexmedetomidine Placebo
200
250
300
350
100
150
mg/gm creatinine
Metanephrine
baseline intraop POD1 AM POD1 PM POD2 AM POD2 PM
5
4
2
3
1
0
nmol/mL
Epinephrine
baseline preop intub extub PACU PACU+60
#*
* *
200
300
400
500
600
700
800
900
1000
1100mg/gm creatinine
Normetanephrine
baseline intraop POD1 AM POD1 PM POD2 AM POD2 PM
#*
#*#
*
10
8
9
7
6
5
4
2
1
3
1
nmol/mL
Norepinephrine
baseline preop intub extub PACU PACU+60
#*
#*
*
# Significantly different (P<.05) from dexmedetomidine group. * Significantly different (P<.05) from baseline.
Neurological Effects
Properties of Dexmedetomidine in Neurosurgery
Intraoperative hemodynamic stability1
Lack of respiratory depression1
Patients easily transition from sleep to wakefulness and task performance when aroused, and then back to sleep when not stimulated1
Does not increase intracranial pressure1
Allows for consistent and reliable somatosensory evoked potential amplitudes or latencies1
1Bekker A, Sturaitis MK. Neurosurgery. 2005;57:1-10.

Examples of Cooperative SedationNeurological Examples
Intracranial surgical procedures often require patient cooperation for functional assessment1– The procedure is frequently limited by the location/spatial extent
of the lesion and its relationship to functioning tissue1
– Surgeons balance the benefits of an aggressive resection with anticipated neurological dysfunction1
Intraoperative neurophysiological testing1
– Can verify that surgical target has been localized1
– Is used to assess the production of an intended functional change1
Carotid endarterectomy performed in awake patients allows evaluation of cerebral perfusion by continuous examination of neurologic function2
1Bekker AY, et al. Neurosurgery. 2005; 57(1 Suppl):1-10.2Bekker AY, et al. J Neurosurg Anesthesiol. 2004;16:126-135.
Dexmedetomidine and Cerebral Blood FlowClinical Data
Reduced cerebral blood flow (CBF) has also been demonstrated in human studies1
– Reduced CBF may be advantageous for situations such as traumatic brain injury or large brain tumors1
No detrimental effect on local brain tissue oxygenation in patients undergoing cerebral vascular surgery1
Under normotensive conditions in the setting of compromised cerebral circulation, dexmedetomidine has no apparent adverse effects1
It has been shown that dexmedetomidine is suitable for preoperative sedation of patients with subarachnoid hemorrhage (SAH)2
1Bekker A, Sturaitis MK. Neurosurgery. 2005;57:1-10.2Sato K, et al. Masui. 2006;55:51-54.

Dexmedetomidine and Cerebral Blood FlowDecreased Cerebral Metabolic Rate
Prielipp and colleagues analyzed data from nine supine volunteers to assess the potential for dexmedetomidine induced decreases in regional and global CBF Patients were infused with a 1 mcg/kg IV loading dose of dexmedetomidine, followed by an infusions of either – 0.2 mcg/kg/h (Low Dose) – 0.6 mcg/kg/h (High Dose)
Prielipp RC, et al. Anesth Analg.2002;95:1052-1059.
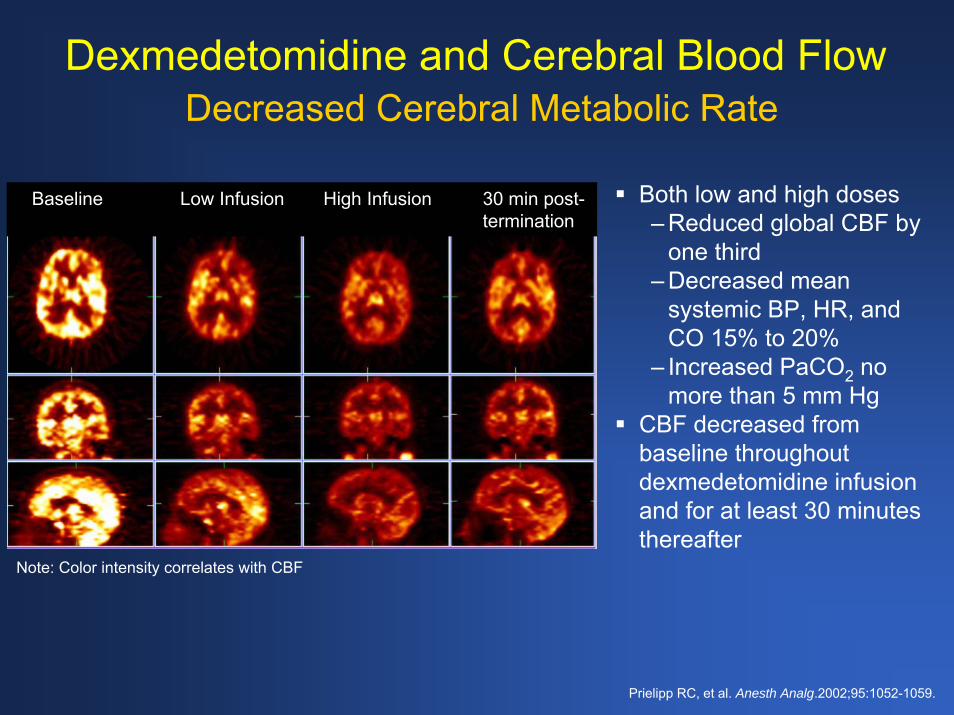
Dexmedetomidine and Cerebral Blood FlowDecreased Cerebral Metabolic Rate
Both low and high doses– Reduced global CBF by
one third– Decreased mean
systemic BP, HR, and CO 15% to 20%
– Increased PaCO2 no more than 5 mm Hg
CBF decreased from baseline throughout dexmedetomidine infusion and for at least 30 minutes thereafter
Baseline Low Infusion High Infusion 30 min post-termination
Note: Color intensity correlates with CBF
Prielipp RC, et al. Anesth Analg.2002;95:1052-1059.
Dexmedetomidine and Cerebral Blood FlowCerebral Perfusion in Severe Head Injury
Prospective study on the effect of dexmedetomidine in patients with severe head injury
– 12 ICU patients (aged 15 to 64 years) – Glasgow Coma Scale <8– Intracranial pressure <20 mm Hg – O2 saturation monitoring of blood from jugular bulb
3 hours of progressive IV dexmedetomidine perfusion (0.2, 0.4, 0.7 mcg/kg/h)
– All other sedative-analgesic medications previously withdrawn
Grille P, et al. Neurocirugia. 2005;16:411-8.
Dexmedetomidine and Cerebral Blood FlowCerebral Perfusion in Severe Head Injury (Cont’d)
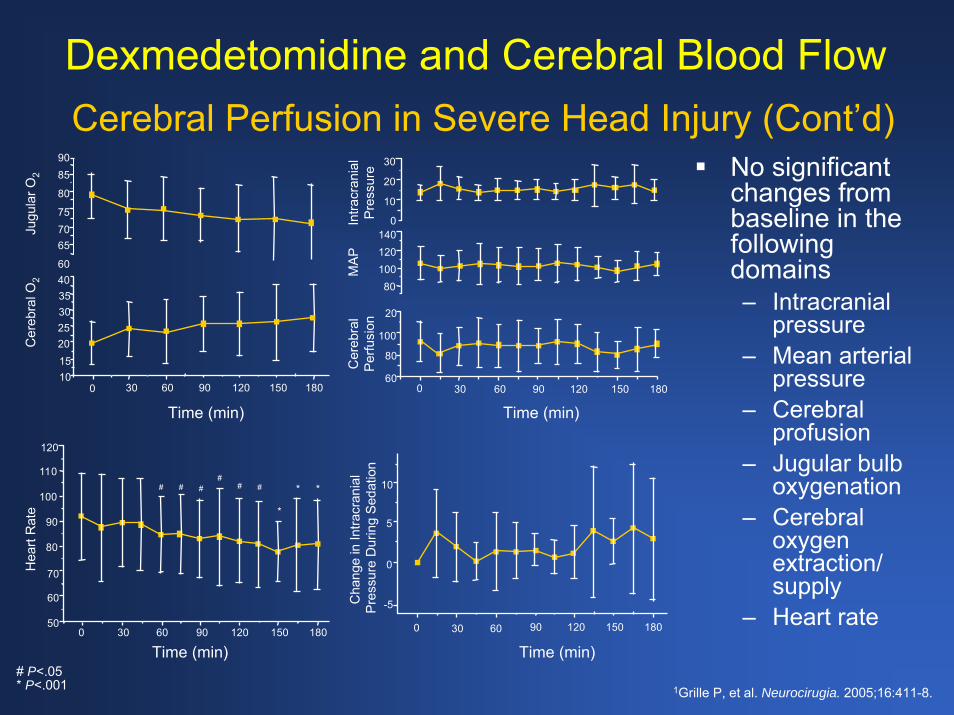
No significant changes from baseline in the following domains– Intracranial
pressure– Mean arterial
pressure– Cerebral
profusion– Jugular bulb
oxygenation– Cerebral
oxygen extraction/ supply
– Heart rate
60
65
7570
80
8590
201510
25
3540
30
906030 120 150 180
100
110
60
50
70
80
90
120
90600 30 120 150 180
# ## # ##
*
* * 10
906030 120 150 180
0
0
5
-5
60
80
100
100
20
20
30
120
906030 120 150 180
1400
10
80
Time (min)
Time (min)
Cha
nge
in In
tracr
ania
l Pr
essu
re D
urin
g Se
datio
nC
ereb
ral
Perfu
sion
Intra
cran
ial
Pres
sure
0
Time (min)
Time (min)
Hea
rt R
ate
Cer
ebra
l O2
Jugu
lar O
2
0
MAP
# P<.05* P<.001 1Grille P, et al. Neurocirugia. 2005;16:411-8.

Pediatric Applications
Use of Dexmedetomidine in MRI
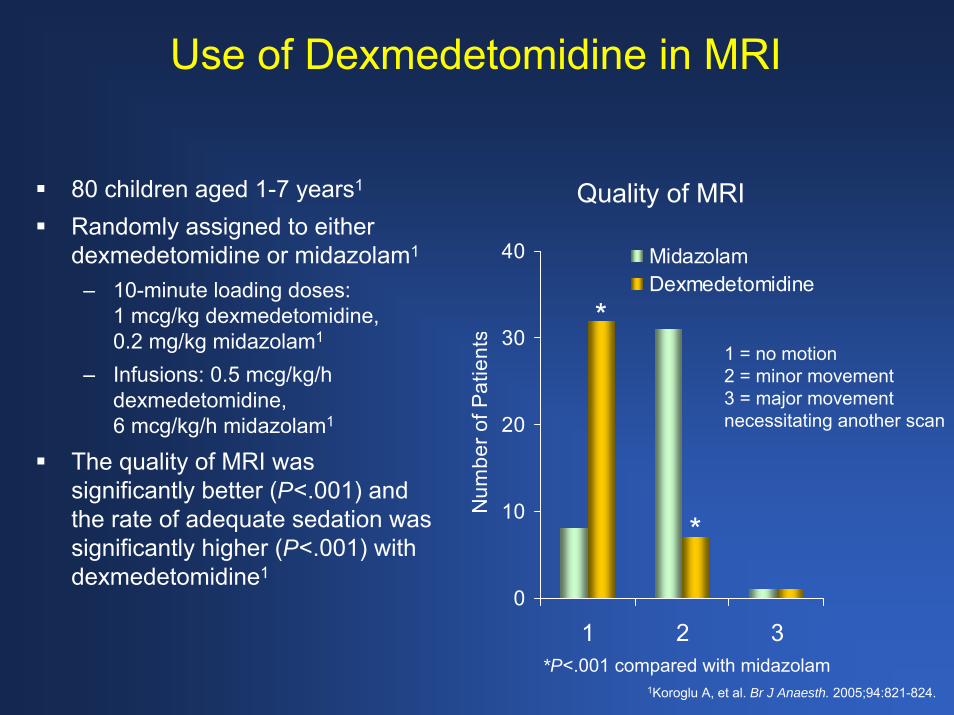
80 children aged 1-7 years1
Randomly assigned to either dexmedetomidine or midazolam1
– 10-minute loading doses: 1 mcg/kg dexmedetomidine, 0.2 mg/kg midazolam1
– Infusions: 0.5 mcg/kg/h dexmedetomidine, 6 mcg/kg/h midazolam1
The quality of MRI was significantly better (P<.001) and the rate of adequate sedation was significantly higher (P<.001) with dexmedetomidine1
0
10
20
30
40
1 2 3
Num
ber o
f Pat
ient
s
MidazolamDexmedetomidine
1 = no motion2 = minor movement3 = major movement necessitating another scan
Quality of MRI
*P<.001 compared with midazolam
*
*
1Koroglu A, et al. Br J Anaesth. 2005;94:821-824.
Dexmedetomidine Superior to Midazolam in Pediatric Acute Care Patients
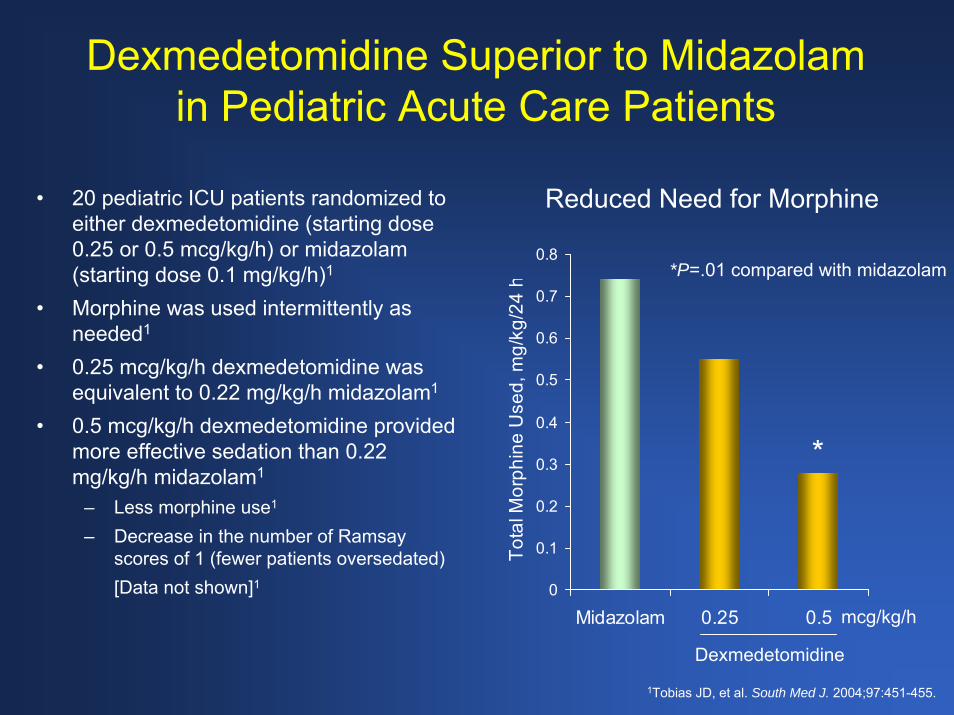
Reduced Need for Morphine• 20 pediatric ICU patients randomized to either dexmedetomidine (starting dose 0.25 or 0.5 mcg/kg/h) or midazolam (starting dose 0.1 mg/kg/h)1
• Morphine was used intermittently as needed1
• 0.25 mcg/kg/h dexmedetomidine was equivalent to 0.22 mg/kg/h midazolam1
• 0.5 mcg/kg/h dexmedetomidine provided more effective sedation than 0.22 mg/kg/h midazolam1
– Less morphine use1
– Decrease in the number of Ramsay scores of 1 (fewer patients oversedated)[Data not shown]1 0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
Midazolam 0.25 0.5
Tota
l Mor
phin
e U
sed,
mg/
kg/2
4 h
Dexmedetomidine
*
*P=.01 compared with midazolam
mcg/kg/h
1Tobias JD, et al. South Med J. 2004;97:451-455.

Propofol Black Box Warnings for Pediatric Use
Not recommended for – Induction of anesthesia in patients aged <3 years1
– Maintenance of anesthesia in patients aged <2 months1
Pediatric use– Not indicated for ICU sedation or for MAC
sedation for surgical, nonsurgical, or diagnostic procedures1
– Co-administration of fentanyl and propofol may result in serious bradycardia1
1Propofol [package insert]. Bedford, OH: Bedford Laboratories; 2005.

Dexmedetomidine in
Bariatric Surgery

Intraoperative Use of Dexmedetomidine in Bariatric Surgery
Rising incidence of morbid obesity is increasing the need for bariatric surgery1,2
Respiratory comorbidities in morbid obesity may profoundly impact anesthetic management1,2
– Opioid use may lead to severe respiratory depression1,2
– Ideal analgesics should be free of significant/long-lasting respiratory effects1,2
In one center, over 2000 bariatric procedures have been performed safely using the perioperative administration of dexmedetomidine, which was shown to be cardioprotective and neuroprotective while providing a hemodynamically stable course and reducing the need for opioids and inhalational agents3
1Hofer RE, et al. Can J Anaesth. 2005;52:176-180.2Feld JM, et al. J Clin Anesthesia. 2006;18:24-28.
3Ramsay MA. Semin Anesth.2006;25:51-56.

Dexmedetomidine Attenuates Blood Pressure in Bariatric Surgery
Feld and colleagues evaluated whether dexmedetomidine infusion could replace fentanyl in open gastric bypass surgery1
During surgery, blood pressure and heart rate were significantly decreased with dexmedetomidine compared with fentanyl1
Dexmedetomidine was associated with significantly lower postoperative pain and morphine use1
1Feld JM, et al. J Clin Anesthesia. 2006;18:24-28.
120
100
80
60
40
120
100
80
60
40
FentanylDexmedetomidine
Time (min)0 60 120 180
Mea
n Bl
ood
Pres
sure
(mm
Hg)
Hea
rt R
ate,
BPM
(min
-1)
Algorithms
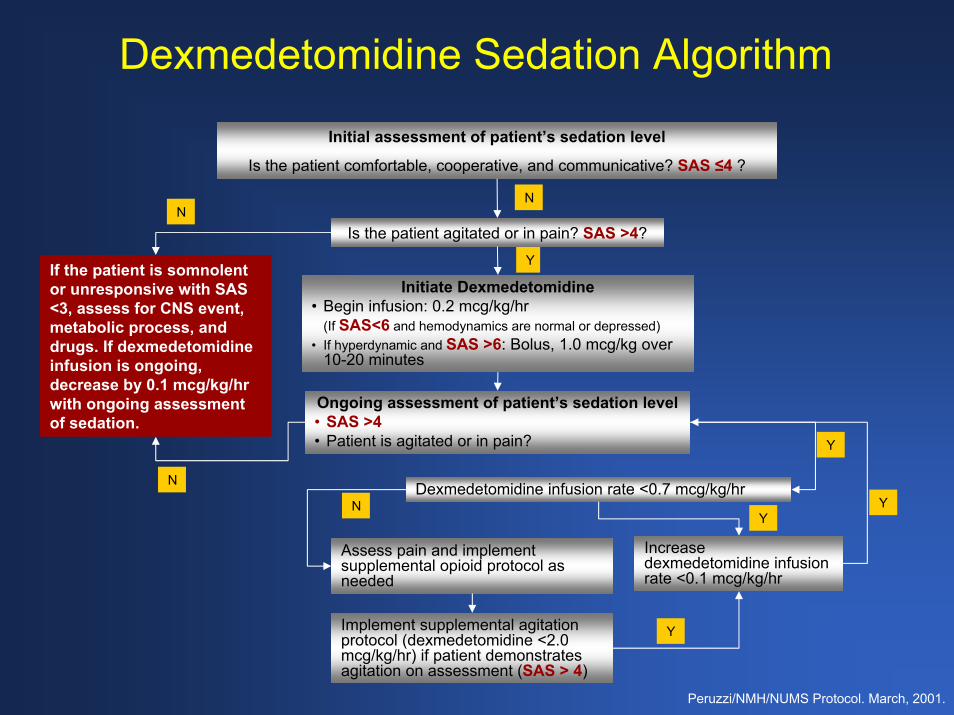
Dexmedetomidine Sedation Algorithm
Peruzzi/NMH/NUMS Protocol. March, 2001.
Is the patient agitated or in pain? SAS >4?
Initial assessment of patient’s sedation level
Is the patient comfortable, cooperative, and communicative? SAS ≤4 ?
Initiate Dexmedetomidine• Begin infusion: 0.2 mcg/kg/hr
(If SAS<6 and hemodynamics are normal or depressed)• If hyperdynamic and SAS >6: Bolus, 1.0 mcg/kg over
10-20 minutes
Ongoing assessment of patient’s sedation level• SAS >4• Patient is agitated or in pain?
Dexmedetomidine infusion rate <0.7 mcg/kg/hr
Increase dexmedetomidine infusion rate <0.1 mcg/kg/hr
Assess pain and implement supplemental opioid protocol as needed
Implement supplemental agitation protocol (dexmedetomidine <2.0 mcg/kg/hr) if patient demonstrates agitation on assessment (SAS > 4)
N
N
Y
YIf the patient is somnolent or unresponsive with SAS <3, assess for CNS event, metabolic process, and drugs. If dexmedetomidine infusion is ongoing, decrease by 0.1 mcg/kg/hr with ongoing assessment of sedation.
N
N
YY
Y
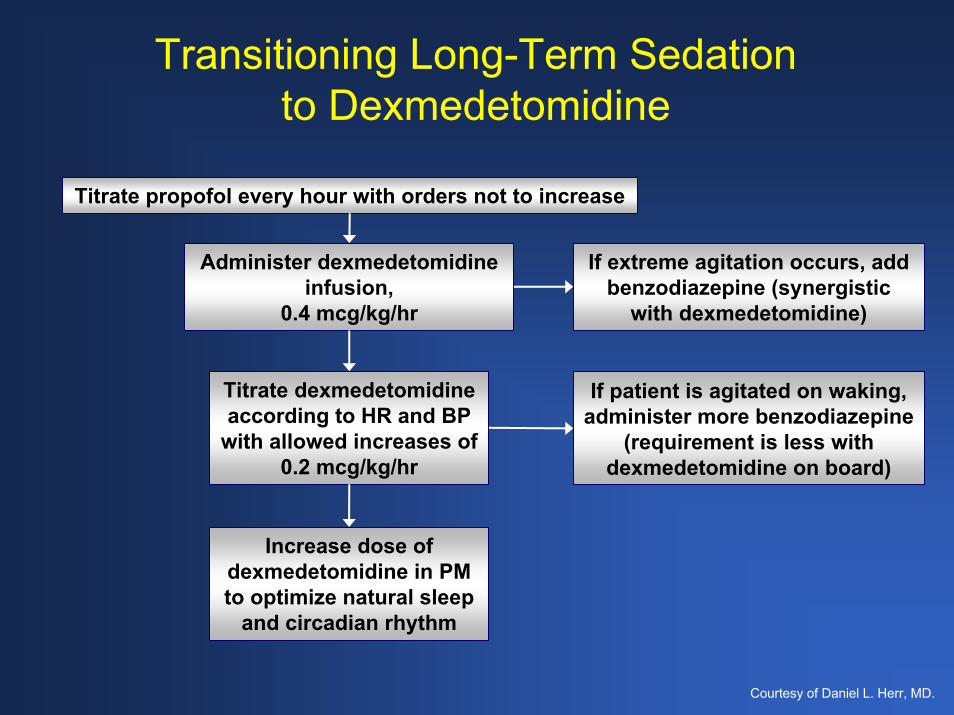
Transitioning Long-Term Sedation to Dexmedetomidine
Titrate propofol every hour with orders not to increase
Administer dexmedetomidine infusion,
0.4 mcg/kg/hr
If extreme agitation occurs, add benzodiazepine (synergistic
with dexmedetomidine)
Titrate dexmedetomidine according to HR and BP
with allowed increases of 0.2 mcg/kg/hr
If patient is agitated on waking, administer more benzodiazepine
(requirement is less with dexmedetomidine on board)
Increase dose of dexmedetomidine in PM to optimize natural sleep
and circadian rhythm
Courtesy of Daniel L. Herr, MD.

Abdominal Aortic Aneurysm
Patients undergoing endovascular repair of abdominal aortic aneurysms with general (n = 217; 22 used for direct comparison) versus dexmedetomidine (n = 14) sedationDexmedetomidine sedation resulted in
– Reduced time for surgery – Reduced time for anesthesia– Reduced opioid requirement
Administer supplemental O2 via nasal cannulae
Initiate maintenance dexmedetomidine infusion (0.3 to 0.7 mcg/kg/h)
Cannulate arteries and insert grafts
Administer dexmedetomidine loading dose 1 mcg/kg via infusion pump
Administer 0.5% bupivacaine
Access femoral arteries via 2 small surgical incisions in both groins
Awaken patient and request holding of breath to induce apnea. Patient must remain still.
Complete procedure and bring patient to lighter sedation level prior to OR discharge
Brown BJ, et al. Proc (Bayl Univ Med Cent). 2006;19:213-215.
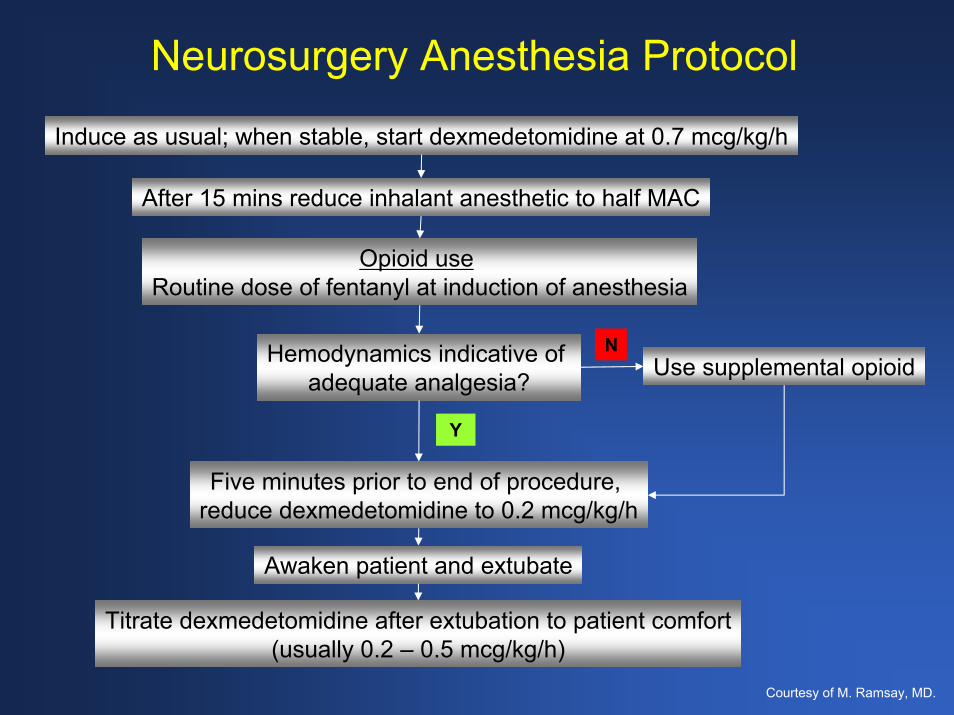
Neurosurgery Anesthesia Protocol
Induce as usual; when stable, start dexmedetomidine at 0.7 mcg/kg/h
After 15 mins reduce inhalant anesthetic to half MAC
Opioid use Routine dose of fentanyl at induction of anesthesia
Hemodynamics indicative of adequate analgesia?
Five minutes prior to end of procedure, reduce dexmedetomidine to 0.2 mcg/kg/h
Use supplemental opioid
Awaken patient and extubate
Titrate dexmedetomidine after extubation to patient comfort(usually 0.2 – 0.5 mcg/kg/h)
N
Y
Courtesy of M. Ramsay, MD.
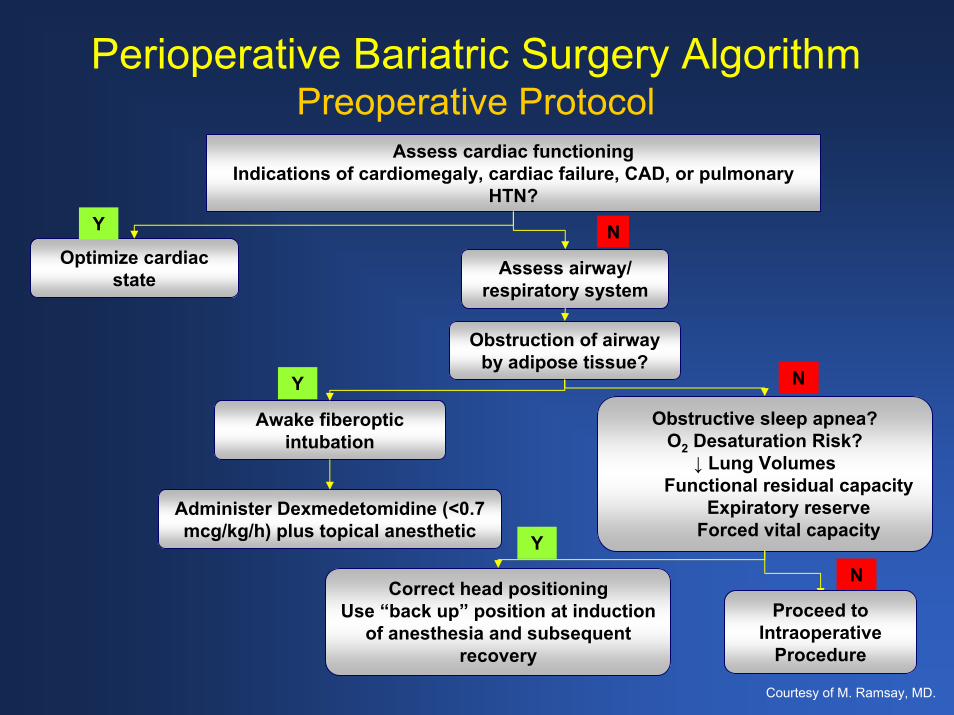
Perioperative Bariatric Surgery AlgorithmPreoperative Protocol
Assess cardiac functioning Indications of cardiomegaly, cardiac failure, CAD, or pulmonary
HTN?
Optimize cardiac state Assess airway/
respiratory system
Y N
Obstruction of airway by adipose tissue?
Awake fiberoptic intubation
Obstructive sleep apnea?O2 Desaturation Risk?
↓ Lung VolumesFunctional residual capacity
Expiratory reserveForced vital capacity
N
Administer Dexmedetomidine (<0.7 mcg/kg/h) plus topical anesthetic
Correct head positioningUse “back up” position at induction
of anesthesia and subsequent recovery
Y
YN
Proceed to Intraoperative
Procedure
Courtesy of M. Ramsay, MD.
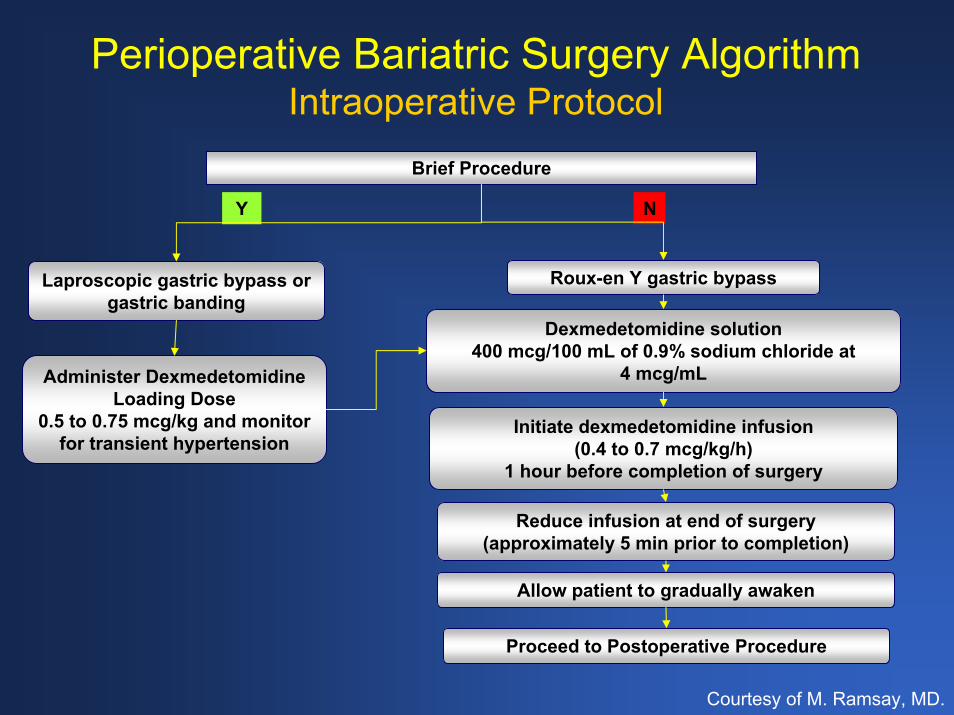
Perioperative Bariatric Surgery AlgorithmIntraoperative Protocol
Brief Procedure
Laproscopic gastric bypass or gastric banding
Roux-en Y gastric bypass
Y N
Dexmedetomidine solution400 mcg/100 mL of 0.9% sodium chloride at
4 mcg/mL
Initiate dexmedetomidine infusion (0.4 to 0.7 mcg/kg/h)
1 hour before completion of surgery
Reduce infusion at end of surgery (approximately 5 min prior to completion)
Administer Dexmedetomidine Loading Dose
0.5 to 0.75 mcg/kg and monitor for transient hypertension
Proceed to Postoperative Procedure
Allow patient to gradually awaken
Courtesy of M. Ramsay, MD.
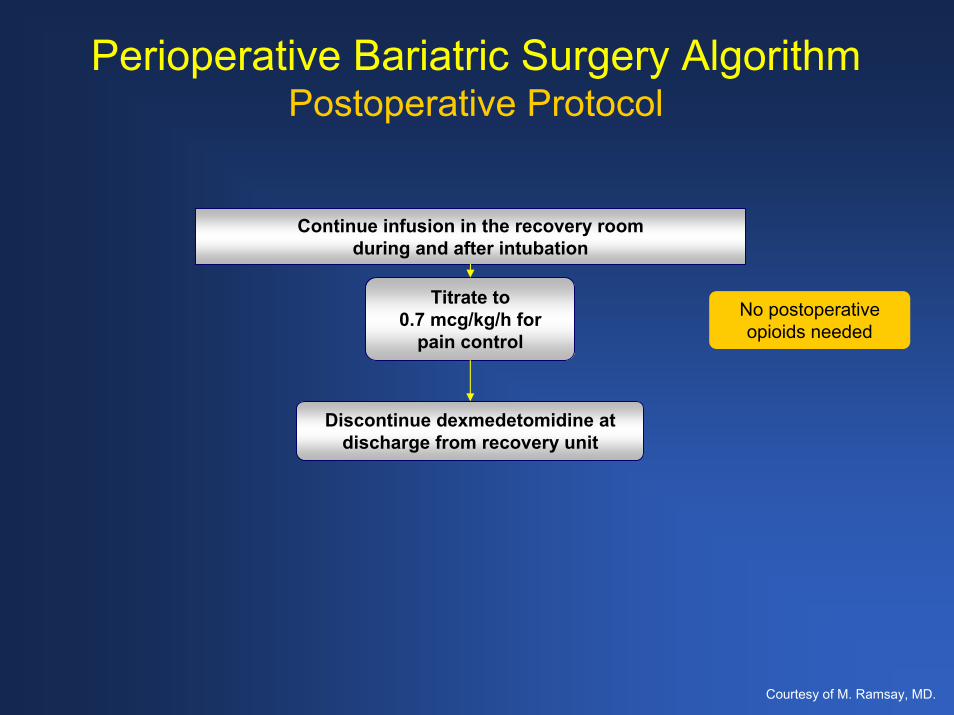
Perioperative Bariatric Surgery AlgorithmPostoperative Protocol
Continue infusion in the recovery room during and after intubation
Titrate to 0.7 mcg/kg/h for
pain control
Discontinue dexmedetomidine at discharge from recovery unit
No postoperative opioids needed
Courtesy of M. Ramsay, MD.

Overall Summary
Patient care and safety, as well as physiological and neurobehavioral considerations, reinforce the need for sedation in acute care settingsAttenuating reactions to pain and stress while optimizing patient communication are important acute care goalsInappropriate sedation and analgesic therapy in acute care settings leads to poor clinical and economic outcomesGuidelines, standards, clinical pathways, and algorithms clarify the manner in which sedatives should be used in acute care settings– Institutions should have multidisciplinary agreements to
use scale assessment and documentation
Overall Summary (Cont’d)
Ongoing developments influence changes in guidelines and standards– It is anticipated that JCAHO will add new sedation criteria– Currently under revision, new SCCM guidelines are
expected in 2007
Implementation of rational use guidelines in acute care sedation can result in improved LOS and reduced costs for medications The addition of dexmedetomidine to the current standard of care is associated with improved clinical outcomes and reduced total hospital costs