disclosure guideline updates 1 48th annual meeting navigating the oceans of opportunity pour some...
TRANSCRIPT

7/19/2014
1
48th Annual Meeting
Navigating the Oceans of Opportunity
Pour Some Sugar On Me –Diabetes Updates for the
Practicing Pharmacist Karen R. Sando, Pharm.D., BCACP, CDE
Clinical Assistant ProfessorUniversity of Florida, College of Pharmacy
Gainesville, FL
Disclosure
I do not have a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with an organization whose philosophy could potentially bias my presentation
I have lived with T1DM since age 8 and use the following devices to manage my diabetes: Animas Ping Insulin Pump
Dexcom G4 Platinum Continuous Glucose Monitor
One Touch Mini Glucose meter
Disclosure
Objectives
Explain updates to widely used guidelines for diabetes management (e.g. ADA)
Describe new therapeutic agents for management of diabetes mellitus and current role in therapy.
Describe new technologies (e.g. new continuous glucose monitors, insulin pumps, apps) for management of diabetes mellitus.
Discuss clinical controversies in diabetes management and provide clinical pearls for navigating controversies in practice.
Guideline Updates
Diabetes and Related Guideline Updates
Nov 2013
• ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults – Focus on Individuals with DM
Dec 2013
• 2014 Evidence-Based Guidelines for Management of High Blood Pressure in Adults (JNC 8) – HTN goals for individuals with DM
Jan 2014
• 2014 American Diabetes Association Standards of Care in Diabetes Mellitus

7/19/2014
2
Foreigner – Double Vision (Look Similar to 2013)
2014 ADA Standards of Care
Diagnosis of Diabetes
Screening for T1DM
Detection and Diagnosis of Gestational Diabetes Mellitus
Glucose Monitoring
Neuropathy
Pharmacological Therapy for Hyperglycemia in T2DM
Medical Nutrition Therapy
Nephropathy
Retinopathy
Diabetes Care in Specific Populations (thyroid and celiac screening)
Diabetes Care in the Hospital
ADA Standards of Care in DM
Diabetes Care January 2014 37:S4
ADA Levels of Evidence Grading System
LOE Description
A Clear evidence from well-conducted, generalizable RCTs that are adequatelypowered
B Supportive evidence from well-conducted cohort or case control studies
C Supportive evidence from poorly controlled or uncontrolled studies OR Conflicting evidence with the weight of evidence supporting the recommendation
E Expert consensus or clinical experience
Diabetes Care January 2014 37:S14-S80
Pharmacologic Therapy in T2DM
2013 - If noninsulin monotherapy at maximal tolerated dose does not achieve or maintain the A1C target over 3–6 months, add a second oral agent, a glucagon-like peptide-1 (GLP-1) receptor agonist, or insulin. (LOE=A)
3 months
2014
Diabetes Care January 2014 37:S14-S80
Clinical Inertia with Treatment Intensification People with diabetes often experience prolonged
(> 5 years) poor glycemic control (A1c >8%) before insulin therapy is initiated
UK data estimates from NICE - takes mean of 7.7 years to initiate insulin after last OAD started (on ≥ 2 OADs)
Bottom line – therapy intensification should be considered every 3 months if not achieving A1c goals
NICE=National Institute for Health and Care Excellence Diabetes Care 2013, 36:3411-3417
Nephropathy
“Microalbuminuria” and “macroalbuminuria” will no longer be used “Persistent albuminuria” at levels 30–299 mg/24 h and
levels ≥ 300 mg/24 h
Normal albumin excretion = < 30 mg/24 h.
ACEI or ARB for primary prevention of diabetic kidney disease is not recommended in those with normal blood pressure and albumin excretion (<30 mg/24 hours) (LOE=B)
Diabetes Care January 2014 37:S14-S80
7/19/2014
3
Nephropathy
For people with DM and diabetic kidney disease (albuminuria >30 mg/24 hour) reducing dietary protein below usual intake is NOT recommended (LOE=A) Previous guidelines recommended limiting protein
intake to 0.8 to 1.0 g/kg body weight/day
Does not alter glycemic measures, cardiovascular risk measures, or GFR decline
May consider if GFR continues to decline despite BP/glucose control and ACEI/ARB on board
Diabetes Care January 2014 37:S14-S80
Diabetes Care in the Hospital
The sole use of sliding scale insulin in the inpatient hospital setting is discouraged (LOE=E)
Sliding scale insulin in the inpatient setting Reactionary vs. proactive
Higher frequency of hyperglycemia
Greater length of stay
“Recommend more physiological regimen including basal, prandial, and correctional insulin is recommended”.
More evidence is needed Diabetes Care January 2014 37:S14-S80
Phil Collins – “I Don’t Care Anymore” (about LDL goals)
2013 ACC/AHA Lipid Guidelines
Lipid Management (Before)
ATP III; JAMA. 2001;285:2486-2497
AHA/ACC 2013 Lipid Guidelines
Four statin benefit groups: Clinical ASCVD
LDL ≥190 mg/dL
Diabetes Mellitus (T1 or T2)
10-yr ASCVD risk ≥ 7.5%
Guideline Comparison
2013 ACC/AHA Lipid Guidelines 2014 ADA Standards of DM Care
Diabetes is 1 of 4 statin benefit Groups1. Clinical ASCVD2. LDL ≥ 190 mg/dL3. Diabetes T1 or T2 (40 to 75 yrs of age) 4. 10-yr ASCVD risk ≥ 7.5%
Statin therapy should be considered regardless of baseline LDL levels in: -with overt CVD -without CVD and over age 40 with one ore more CVD risk factors (family history of CVD, HTN, smoking, dyslipidemia, or albuminuria
Calculate 10-yr ASCVD risk in those withoutclinical ASCVD
LDL goal <100 mg/dL (without overt CVD)LDL < 70 mg/dL (with overt CVD, optional)
If 10-yr ASCVD risk is ≥ 7.5% initiate high intensity statin therapy (lowers LDL by ≥ 50%)
Combination therapy has been shown not to provide additional cardiovascular benefit above statin therapy alone and is not generally recommended Non-statin therapy not recommended in
addition to statins except in certain clinical situations
7/19/2014
4
Bottom Line – Lipids in DM
Statin therapy should be initiated regardless of baseline lipid levels Substantial evidence supporting reduced CVD events
Select appropriate statin intensity based on 10-yr ASCVD risk and clinical history
Non-statin therapies no longer favored except in certain clinical situations
LDL reduction is primary goal of therapy
Monitor lipid levels 4 to 12 weeks after statin initiation for anticipated therapeutic response
Queen – “Under (Less) Pressure”
2014 Hypertension Guidelines (JNC 8)
JNC 8 Guidelines
Bottom Line – HTN in DM
For most patients treat to goal of <140/90 mm Hg Lower goals for those at higher risk of stroke (ADA)
Higher goals for elderly (>60 or >80 yo ?)
For those without CKD or albuminuria, can consider initiating CCB or thiazide-diuretic as first-line therapy African Americans – Low renin, salt-sensitive (CCB,
thiazides)
Caucasians – renin-mediated (ACEI, ARB)
Increase doses to achieve goal and intensify with a second agent of a differing mechanism for best results
Led Zeppelin – The Song (and therapeutic class) Remains the Same
New Diabetes Medications
7/19/2014
5
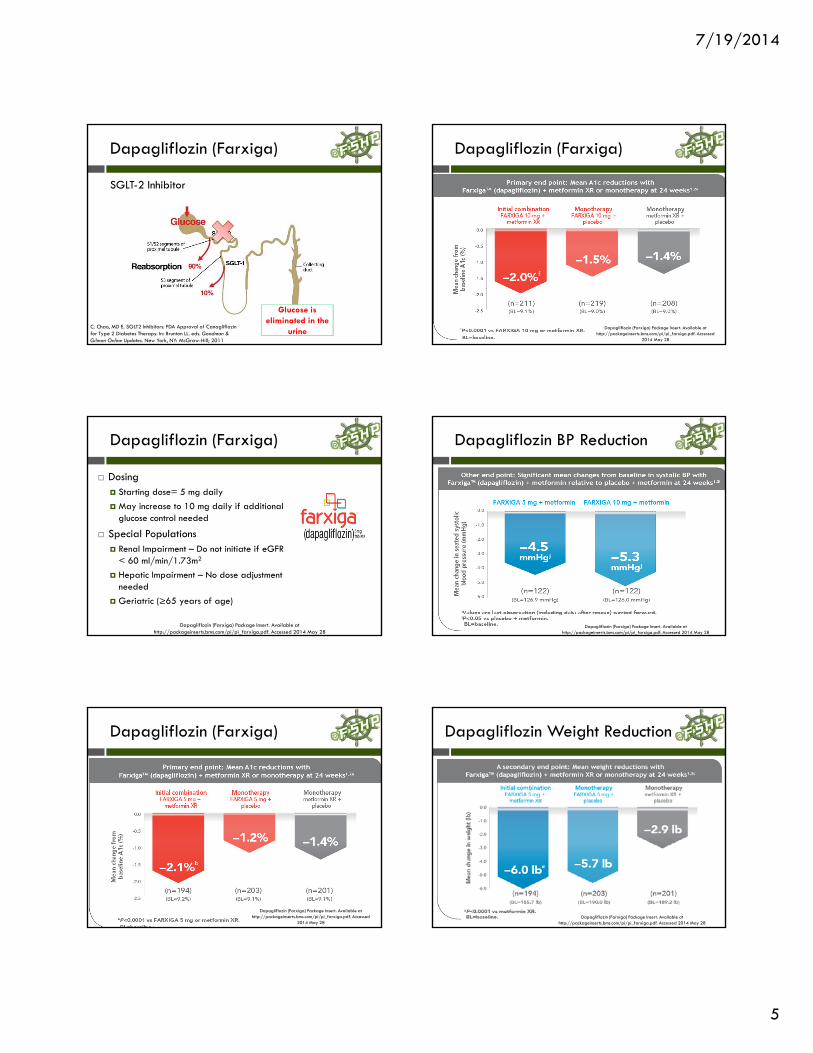
Dapagliflozin (Farxiga)
SGLT-2 Inhibitor
Glucose is eliminated in the
urine C. Chao, MD E. SGLT2 Inhibitors: FDA Approval of Canagliflozin for Type 2 Diabetes Therapy. In: Brunton LL. eds. Goodman & Gilman Online Updates. New York, NY: McGraw-Hill; 2011
Dapagliflozin (Farxiga)
Dosing Starting dose= 5 mg daily
May increase to 10 mg daily if additional glucose control needed
Special Populations Renal Impairment – Do not initiate if eGFR
< 60 ml/min/1.73m2
Hepatic Impairment – No dose adjustment needed
Geriatric (≥65 years of age)
Dapagliflozin (Farxiga) Package Insert. Available at http://packageinserts.bms.com/pi/pi_farxiga.pdf. Accessed 2014 May 28
Dapagliflozin (Farxiga)
Dapagliflozin (Farxiga) Package Insert. Available at http://packageinserts.bms.com/pi/pi_farxiga.pdf. Accessed
2014 May 28
Dapagliflozin (Farxiga)
Dapagliflozin (Farxiga) Package Insert. Available at http://packageinserts.bms.com/pi/pi_farxiga.pdf. Accessed
2014 May 28
Dapagliflozin BP Reduction
Dapagliflozin (Farxiga) Package Insert. Available at http://packageinserts.bms.com/pi/pi_farxiga.pdf. Accessed 2014 May 28
Dapagliflozin Weight Reduction
Dapagliflozin (Farxiga) Package Insert. Available at http://packageinserts.bms.com/pi/pi_farxiga.pdf. Accessed 2014 May 28

7/19/2014
6
Dapagliflozin (Farxiga)
Adverse effects Female genital mycotic infections (6.9% - 9.4% vs.
1.5% placebo)
Nasopharyngitis (6.3% vs. 6.2% placebo)
Urinary tract infections (4.3% - 5.7% vs. 3.7% placebo)
Medication Guide required Bladder cancer risk Across 22 clinical studies only 4 cases in treatment group
0.17% (dapagliflozin) vs. 0.03% in placebo/comparator
Dapagliflozin (Farxiga) Package Insert. Available at http://packageinserts.bms.com/pi/pi_farxiga.pdf. Accessed 2014 May 28
Dapagliflozin (Farxiga)
Significant drug interactions Not metabolized by CYP450 system
No clinically significant interactions
May cause hypotension due to intravascular volume depletion Caution in those on antihypertensives
Patient Counseling and Monitoring Experience increase urine volume
Hypoglycemia
Hemoglobin A1c and renal function
Dapagliflozin (Farxiga)
Place in therapy Consider as add-on therapy in patients who
do not achieve A1c goals on metformin monotherapy
Some beneficial effects on weight and BP –common comorbidities with diabetes
Avoid in renal impairment
Minimal risk of hypoglycemia
Cost $310 to $320 per 30-day supply (5 mg tablet)
Cost information available at www.goodrx.com. Accessed 2014 May 28
Albiglutide (Tanzeum)
Mechanism of Action - GLP-1 Agonist
Not recommended as initial monotherapy
Dosing 30 mg injected subcutaneously once weekly
May increase to 50 mg once weekly if inadequate response
Special Populations – no suggested renal/hepatic impairment dose adjustments
Albiglutide Monotherapy
Albiglutide (Tanzeum) Package Insert. Available at https://www.gsksource.com/gskprm/htdocs/documents/TANZEUM-PI-MG-IFU-COMBINED.PDF. Accessed
2014 May 28
Combination Therapy
Study Design Significant Results
104-Week RCT comparing add-ontherapy in those inadequately controlled on metformin (N=249)
-0.9% A1c reduction (vs. placebo + MET) -0.4% A1c reduction (vs. sitagliptin + MET) -0.3% A1c reduction (vs. glimepiride + MET) Lost significantly more body weight than those on glimepiride + MET (-1.2 kg)
52-week RCT comparing add-ontherapy in those inadequately controlled on pioglitazone (≥30 mg/day) (±metformin) (N=249)
-0.8% A1c reduction (vs. placebo + pioglitazone) -30 mg/dL FPG reduction (vs. placebo +pioglitazone
52-week RCT comparing add-on vs. pioglitazone in those uncontrolled on metformin + sulfonylurea (N=657)
-0.9% A1c reduction (vs. placebo+ MET + sulf) + 0.25% A1c increase (vs. PIO + MET + sulf) Did NOT meet non-inferiority margin for comparison with PIO Significantly more weight loss vs. PIO add-on (-4.9 kg)

7/19/2014
7
Comparison to Liraglutide
• MORE injection site reactions with albiglutide vs. liraglutide • LESS GI adverse effects with albiglutide vs. liraglutide
Comparison to Insulin Glargine
Adverse Effects
GI upset (N/V/D) – Discontinuation in 2% of patients in pooled placebo controlled trials
Injection site reactions
Cough
Back pain/arthralgias
Rare and Precautions Black box warning – thyroid C-cell, MTC, or MEN-2
tumors
Risk of pancreatitis (0.3% albiglutide vs. 0% placebo)
Slows gastric emptying
Albiglutide Patient Counseling
Step 1 –1. Twist Pen clockwise to mix
lyophilized powder with diluent
2. Rock pen side to side 5 times
Step 2 – Wait 15 minutes while solution mixes
Step 3 –1. Attach needle 2. Rock pen side to side 5 more
times3. Tap pen 2 to 3 times to remove
large air bubbles 4. Twist clockwise again to prime
Albiglutide Place in Therapy
Adds to available GLP-1 agonists Exenatide (Byetta) – twice a day, more GI side effects, not
recommended in significant renal impairment (CrCl <30 ml/min)
Liraglutide (Victoza) – once daily, no renal impairment dosing, less GI side effects vs. exenatide
Exenatide LAR (Bydureon) – once weekly, use not recommended with CrCl < 30 ml/min
Consider as add-on therapy in those inadequately controlled on metformin
Weight loss in overweight/obese patients
Cost ???
Beatles – When I’m Sixty-Four (turn my insulin pump off)
Devices, Apps, and the Future

7/19/2014
8
Combined insulin pump and continuous glucose monitor (CGM)
“Threshold Suspend” feature User controlled on/off
Threshold 60 to 90 mg/dL
Pump will suspend basal delivery for up to 2 hours
Medtronic MiniMed 530G
Study of Threshold Suspend Pump
Bergenstal RM et al. N Engl J Med 2013;369:224-232.
• Patients with T1DM and documented nocturnal hypoglycemia (N=247)
• Randomized to sensor-augmented pump with and without suspend feature for 3 months
Study Design
• Primary safety outcome – change in A1c • Primary efficacy outcome – AUC for nocturnal
hypoglycemic events
Primary and Secondary Outcomes
• Changes in A1c similar between two groups (no statistically significant difference)
• Mean AUC for hypoglycemia 37.5% lower in threshold-suspend group vs. control (p<0.001)
Results
Artificial Pancreas Project (JDRF)
Smart Insulin 2003 MIT chemical
engineer founded a company called SmartCells
2010 Merck has acquired SmartCells
Working to develop glucose-dependent insulin
Future Directions
Information available at www.jdrf.org. Accessed 2014 May 28
Logbooks Glooko Logbook
dLife Diabetes Companion
WaveSense diabetes manager
Carb-Counting My Glucose Buddy
Sanofi-Aventis Go Meals
Useful Apps
Information Available at: http://diabetes.ufl.edu/my-diabetes/diabetes-resources/diabetes-apps/. Accessed 2014 May 28
Peter Frampton – Show Me the Way
Clinical Controversies and Pearls
Common Clinical Controversies
Scenario #1 Maximized on metformin and sulfonylurea and not achieving
A1c goals
What should you add next?
Scenario #2 Oral agents + basal insulin and still not achieving goal
Should we think about mealtime insulin?
Scenario #3 Achieving previously set LDL goals but not on the
appropriate intensity statin
Should I stay or should I go (to a more potent statin)

7/19/2014
9
Scenario #1
BW is a 62 yo female with T2DM on metformin 1000 mg BID and glipizide 10 mg BID. Current A1c is 8.3% (last A1c 8.1% 3 months ago). BMP WNL, Wt=201 lbs (BMI=30.1). Her doctor wishes to add something to her diabetes regimen but isn’t sure what to do. He asks your advice.
“Hey, are you the pharmacist? Can I get some help with this
patient?”
“Hey, are you the pharmacist? Can I get some help with this
patient?”
ADA/EASD Treatment Algorithm
Inzucchi SE et al. Diabetologia. 2012 Jun;55(6):1577-96
AACE 2013 Algorithm
Comparison of Additional Therapy
Basal Insulin vs. GLP-1 RA
• Multicenter, open-label, randomized two-arm parallel trial design• 390 patients with T2DM aged ≥18 with suboptimal glucose control
despite maximum tolerated doses of metformin or metformin + sulfonylurea
• Randomized to insulin glargine initiated at 10 units daily and titrated vs. exenatide weekly 2 mg sub-Q
Study Design
• Change in A1c• % of patients achieving A1c <7.0 and <6.5%• Body weight• Incidence of hypoglycemia • Overall safety
Outcomes
• A1c decreased by -1.2% (EQW) vs. -1.0% (IG) (p=0.029) • Greater percentage of EQW treated patients achieved A1c <7% or ≤6.5% (p=0.084)
• EQW treated patients lost 2.1 kg vs. 2.4 kg gained in IG group (P<0.001) • Less hypoglycemia in metformin alone AND metformin + sulfonylurea EQW-
treated vs. IG-treated (p<0.001) • More diarrhea and nausea occurred in EQW vs. IG
Results
Diamant M et al. Diabetes Care 35:683–689, 2012
Scenario #1 Bottom Line
GLP-1 RA has advantage of weight loss and less hypoglycemia. GI ADE common, injectable
TZDS use caution in those with HF, also causes fluid retention/weight gain
DPP-IV neutral for weight loss, hypoglycemia, generally well-tolerated, linagliptin does not require renal dose adjustment
Basal insulin effective, large A1c reductions, weight gain, hypoglycemia
Bromocriptine moderate GI symptoms, high pill burden (0.8 mg tablets, may take up to 6 tabs/day)
SGLT2 inhibitors caution with renal impairment, increased risk of mycotic infections in female, cost/insurance coverage?

7/19/2014
10
Scenario #2
TG is a 56 yo male with T2DM x 15 years. Current meds include metformin 1000 mg BID, glimepiride 8 mg daily, sitagliptin 100 mg daily, insulin glargine 75 units QHS. Most recent A1c is 9.1%. Compliant with current meds. BMP WNL. Wt=100 kg. His physician refers TG to your diabetes clinic and asks you to figure out what is going on with his diabetes!!
When should we think about adding mealtime insulin?
Not meeting A1c goals despite 3-6 months titration of basal insulin to achieve fasting goal (70-130 mg/dL)
Significant post-prandial glucose excursions (>180 mg/dL)
Overnight lows or between meal lows when basal insulin increased
TDD of insulin exceeds 0.5 units/kg/day 75 units/100 kg=0.75 units/kg/day
A1c above goal of <7.0%Inzucchi SE et al. Diabetologia. 2012 Jun;55(6):1577-96
Initiation and titration
Option #1 Initiate fixed dose of prandial insulin before meal responsible for
largest glucose excursion
Add second injection, then third to other meals
Option #2 Initiate fixed dose of prandial insulin prior to each meal
Typically 10% of total daily basal dose recommended
For TG that would be 7 to 8 units
Option #3 Calculate carbohydrate ratio insulin sensitivity factor (ISF)
Carb ratios Written as 1 unit of
insulin: x grams of carbs
Calculate by dividing TDD (basal) into 500
ISF or correction factor Written as 1unit: x
mg/DL >target BG
Calculate using the “1800 rule”
Carb ratios and ISF
Let’s Do Some Math!
500/75 units (TG’s basal dose) = ~6.7
1 unit: 7 grams of carbohydrate
1800/75 units (TG’s basal dose) =24
1 unit of insulin will lower TG’s blood sugar by ~24 mg/dL
Round to 25 mg/dl for easier math
Putting this into Practice
TG checked his blood sugar before lunch (result=175 mg/dL) and will eat 45 grams of carbohydrates. His target blood sugar before lunch is 100 mg/dL. How much prandial insulin should TG deliver before he eats lunch?
Carb ratio (1:7 grams)
45 grams ÷7 grams per unit of insulin=6.4 units6 units
ISF (1:25 mg/dL > 100 mg/dL)
175 mg/dL-100 mg/dL (target)=75mg/dL
75 mg/dL ÷ 25 mg/dL 3 units
Total to deliver is 9 units
Mealtime Insulin Titration
• Check blood glucose 2-hrs after start of meal OR• Check prior to each meal
• If above goal pre-lunch, increase breakfast prandial dose • If above goal pre-dinner, increase lunch prandial dose, etc.
Meneghini L et al. Endocr Pract. 2011; 17(5): 727-736

7/19/2014
11
Scenario #2 Bottom Line
The case of TG Metformin 1000 mg BID Continue
Glimepiride 8 mg daily Discontinue
Sitagliptin 100 mg daily Continue (for now)
Insulin glargine 75 units daily May reduce dose when initiating prandial insulin
Initiate insulin aspart/glulisine/lispro 7 units prior to meal with largest glucose excursion (usually
dinner OR breakfast)
Increase by 2 if pre-bedtime BG is >180 mg/DL
Scenario #3
HS is a 63 yo WF with T2DM, hyperlipidemia, and HTN that is managed by your lipid clinic. She has no history of ASCVD. She is in for follow-up today of her most recent lipid panel. Current cholesterol med=pravastatin 40 mg QHS
Lipid panel results are: TC=166 mg/dL, TG=162 mg/dL, HDL=41 mg/dL, LDL (calc)=92 mg/dL
BP 138/80 mm Hg
According to the new lipid guidelines, how should we manage this patient?
Scenario #3
HS is meeting previously established LDL treatment goal of <100 mg/dL (per ATP III and ADA 2014 guidelines)
However, is she on appropriate intensity statin?
Statin Intensity
Considering Risk
Globally consider risk for CVD Smoker?
Family history of CVD?
Blood pressure/DM controlled?
Calculate 10-yr ASCVD risk using online calculator http://tools.cardiosource.org/ASCVD-Risk-Estimator/
10-yr calculated risk=16.4% high-intensity statin
How much additional benefit will HS receive from switching to a high-dose statin?
Montori VM et al. JAMA. 2014;311(5):465-466
Statin decision aid
Available at http://staindecisionaid.mayoclinic.org

7/19/2014
12
Statin decision aid
Scenario #3 – Bottom Line
With established ASCVD, guidelines clearly recommend high-intensity statin
For those already established on statin therapy with T2DM: Is it appropriate intensity given their history? If low intensity statin –should likely increase to at least a
moderate-intensity statin (e.g. pravastatin 40 mg, simvastatin 20 mg)
If moderate-intensity –evaluate cardiac risk, will the patient gain additional benefit from high-intensity statin?
Involve patient in decision making (risks v benefits)
Conclusions
ADA guidelines minimally changed in 2014 but new BP and cholesterol guidelines impact the management of our patients with DM
New medications and devices are steadily added to our armamentarium of diabetes medications
When considering treatment changes for diabetes management or comorbidities involve patient in decision making process and clearly explain risks vs. benefits
48th Annual Meeting
Navigating the Oceans of Opportunity
Pour Some Sugar On Me –Diabetes Updates for the
Practicing Pharmacist Karen R. Sando, Pharm.D., BCACP, CDE
Clinical Assistant ProfessorUniversity of Florida, College of Pharmacy
Gainesville, FL