disclosuresn.b5z.net/i/u/10109262/f/osborn__cindy.hanouts.pdfdiagnosis “triple i” -huh?...
TRANSCRIPT
4/3/2018
1
Post-delivery disposition and risk
stratification for the near term and term
newborns born to mothers with
chorioamnionitis (“Triple I”)
Cindy Osborn, RN
Alexander Gurfinkel, MD
April 13, 2018
Disclosures
• I have nothing to disclose
Objectives
• Recognize and implement the new Triple I criteria into your practice
• Explain and utilize the EOS (Early Onset Sepsis) calculator to determine the initial EOS score for newborn assessment.
• Identify the multi-disciplinary culture changes required for successful implementation
• Identify tools for sustaining this process in YOUR workplace

4/3/2018
2
Background
• Chorioamnionitis complicates 2-3% of term
pregnancies in the US.
• Up to 40-70% of preterm pregnancies
• In term and near term infants the incidence of
sepsis is extremely low (0.14%-0.3%)
• Currently ALL infants are recommended to
receive antibiotics (CDC, 2010)
Chorioamnionitis
• Fever PLUS 1 or 2 of the following:
–Maternal leukocytosis (>15,000)
– Fetal tachycardia
– Foul smelling amniotic fluid
–Maternal tachycardia
– Uterine tenderness
• Practitioner to practitioner variation in making
diagnosis
“Triple I” - huh?
• “Intrauterine Infection, Inflammation or both”
• Chorioamnionitis is ambiguous
• Known risk factor for EOS (Early Onset Sepsis),
therefore standardization is needed
• Isolated maternal fever is NOT synonymous
with chorioamnionitis
ACOG Committee Opinion #712 (2017)
4/3/2018
3
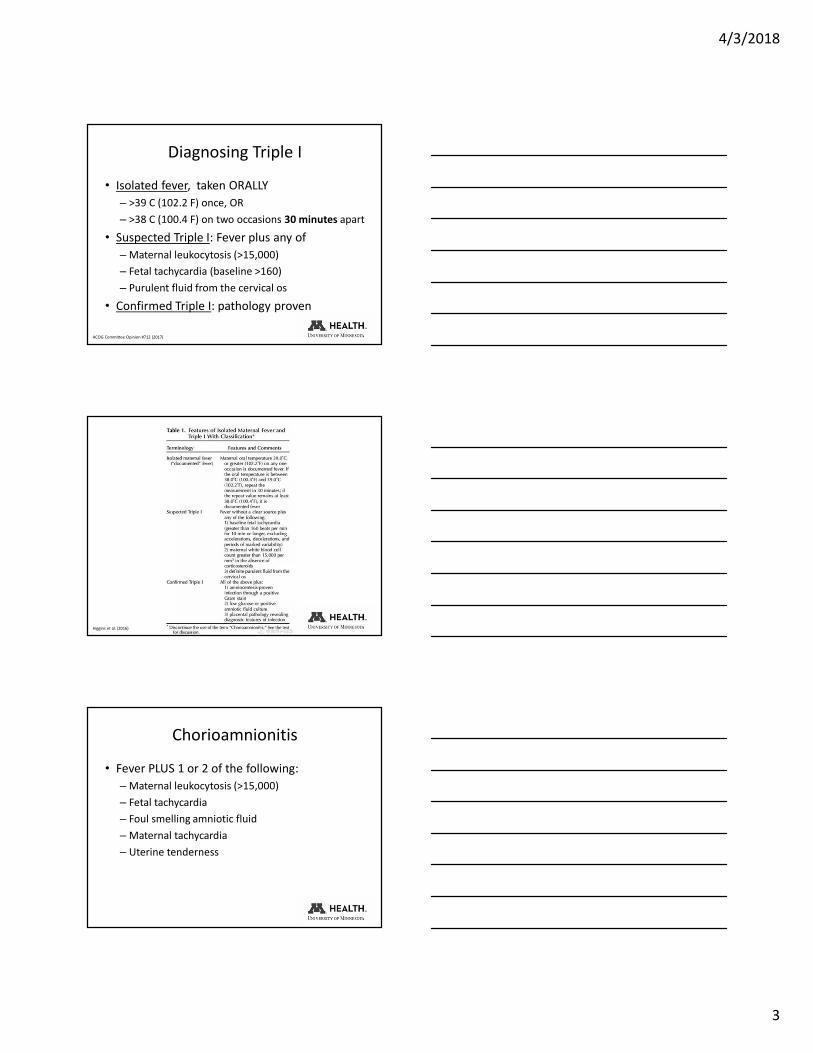
Diagnosing Triple I
• Isolated fever, taken ORALLY
– >39 C (102.2 F) once, OR
– >38 C (100.4 F) on two occasions 30 minutes apart
• Suspected Triple I: Fever plus any of
–Maternal leukocytosis (>15,000)
– Fetal tachycardia (baseline >160)
– Purulent fluid from the cervical os
• Confirmed Triple I: pathology proven
ACOG Committee Opinion #712 (2017)
Higgins et al. (2016)
Chorioamnionitis
• Fever PLUS 1 or 2 of the following:
–Maternal leukocytosis (>15,000)
– Fetal tachycardia
– Foul smelling amniotic fluid
–Maternal tachycardia
– Uterine tenderness

4/3/2018
4
Suspected Triple I
• Fever PLUS ANY of the following:
–Maternal leukocytosis (>15,000)
– Fetal tachycardia (>160 BPM)
– Purulent fluid from the cervical os
–Maternal tachycardia
– Uterine tenderness
• Temperature is assessed twice 30 min apart
allowing for earlier recognition and treatment
Isolated Maternal Fever
Potential Causes
• Epidural anesthesia
• Room temperature
• Prostaglandin use
• Hyperthyroidism
• Dehydration
Treatment
• Isolated fever
–Monitor for other signs
– Treat underlying cause as appropriate
• Suspected Triple I
– Antibiotics are indicated
– Ampicillin and Gentamicin are a frequently used
combination

4/3/2018
5
Work that is underway
• A Pathway is being proposed for consistent care and treatment- all stakeholders are reviewing this for an anticipated “Go live” in May
• An update to the Triple I Maternal Order Set-various antibiotic combinations based on ACOG’s recommendation on GBS status and allergy status.
QI Project
Problem
• All newborns born to mothers with a diagnosis of chorioamnionitis at delivery are being separated from mothers and admitted to the NICU for IV antibiotic therapy
• Bonding immediately after birth is critical, as lack of it may lead to:
– Increase in stress levels
– Thermoregulation issues
– Delayed initiation of breastfeeding
– Increased cost of care
– Utilization of NICU beds by healthy newborns
4/3/2018
6
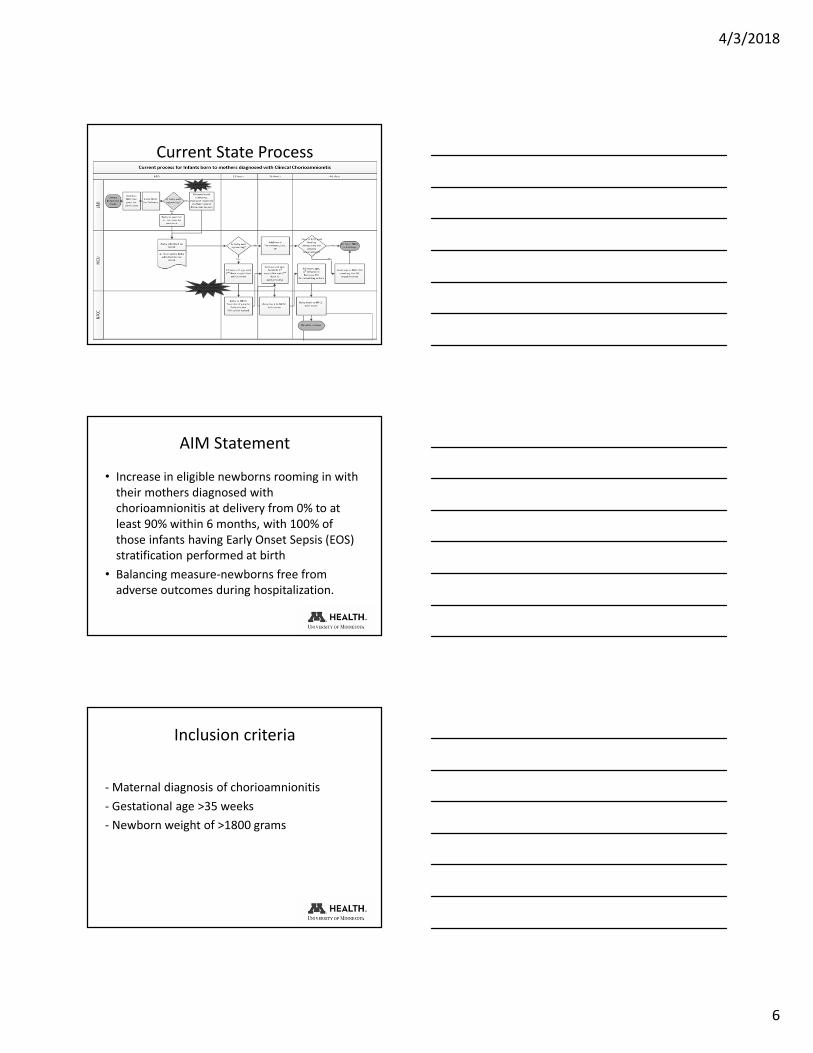
Current State Process
AIM Statement
• Increase in eligible newborns rooming in with
their mothers diagnosed with
chorioamnionitis at delivery from 0% to at
least 90% within 6 months, with 100% of
those infants having Early Onset Sepsis (EOS)
stratification performed at birth
• Balancing measure-newborns free from
adverse outcomes during hospitalization.
Inclusion criteria
- Maternal diagnosis of chorioamnionitis
- Gestational age >35 weeks
- Newborn weight of >1800 grams

4/3/2018
7
Description of Project
• Risk of EOS is calculated based on 5 maternal factors:
Gestational age of baby at delivery
Rupture of membranes duration
Highest degree of maternal fever
GBS status
Timing of prophylactic antibiotics while in labor
• Numerical score is assigned based on the algorithm
Description of Project
Infants with EOS score of 1.54 or less (“mild” and “moderate” risk)
would be admitted to the NFCC (“eligible”)
4/3/2018
8
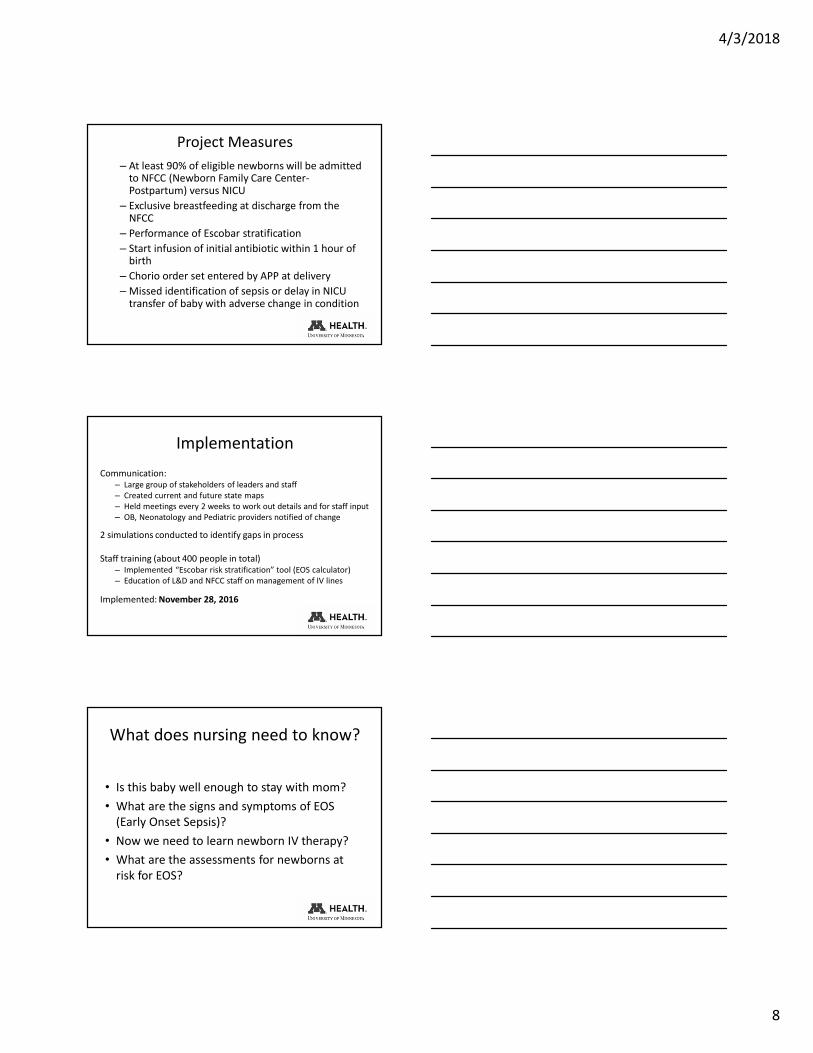
Project Measures
– At least 90% of eligible newborns will be admitted to NFCC (Newborn Family Care Center-Postpartum) versus NICU
– Exclusive breastfeeding at discharge from the NFCC
– Performance of Escobar stratification
– Start infusion of initial antibiotic within 1 hour of birth
– Chorio order set entered by APP at delivery
–Missed identification of sepsis or delay in NICU transfer of baby with adverse change in condition
Implementation
Communication:– Large group of stakeholders of leaders and staff
– Created current and future state maps
– Held meetings every 2 weeks to work out details and for staff input
– OB, Neonatology and Pediatric providers notified of change
2 simulations conducted to identify gaps in process
Staff training (about 400 people in total)– Implemented “Escobar risk stratification” tool (EOS calculator)
– Education of L&D and NFCC staff on management of IV lines
Implemented: November 28, 2016
What does nursing need to know?
• Is this baby well enough to stay with mom?
• What are the signs and symptoms of EOS
(Early Onset Sepsis)?
• Now we need to learn newborn IV therapy?
• What are the assessments for newborns at
risk for EOS?

4/3/2018
9
What does nursing need to know-
(cont)
• Do these newborns need closer monitoring?
• How do we staff for these babies?
• Epic modifications for documentation
• Escobar build
Care of the Newborn-education needs
• Newborn IV management
• Antibiotic administration
• Early Onset Sepsis signs and symptoms
• Central capillary refill and blood pressure
assessments- mean cuff pressure
• Pulse oximetry- assessed with vital signs
Critical
Determinants

4/3/2018
10
Staff Roles and ResponsibilitiesRoles for Newborn Early Onset Sepsis Process
NICU/APP Shared
NICU/L&D
L&D NFCC
Su
pp
lie
s
[ ] PIV start kit
[ ] Venipuncture/Arterial stick Kit
[ ] Umbilical Cord Cart
[ ] Medfusion pump/pole
[ ] Microbore tubing- 60”
[ ] One Link IV Connector
(hub)
[ ] Space Lab Monitor
[ ] BP cuff
[ ] Extra tubing/supplies for PIV
[ ] Space lab monitor
Task
s
[ ] Exam
[ ] Assign Apgar’s
[ ] Disposition Decision
[ ] Update family w/ plan
[ ] Place PIV
[ ] Blood Culture (venipuncture
or placental)
[ ] Label and bring cultures to
NICU lab
[ ] APP to enter Newborn Sepsis
Prevention order-set
[ ] APP enters .escobar note and
billing note
[ ] Chart interventions (including
LDA for the PIV, enter vitals
and weight)
[ ] Release Blood Culture Lab
order
[ ] Weight
[ ] Set of
vitals
[ ] Baby
Bands
[ ] Calculate initial EOS
score
[ ] Start Amp (1st) & Gent
(2nd) when arrives from
main pharmacy
[ ] Continue Vital Signs
[ ] POC glucose
[ ] Acknowledge EOS orders
[ ] Pediatric provider to interpret CBC
results
[ ] Provider to check on culture results
daily
[ ] Lock PIV
[ ] Complete Antibiotic course
[ ] Replace any infiltrated PIVs
1. Vascular Access
2. Ped’s Flyer
3. NICU staff
4. Consider IM if only 1 Amp dose
remains. Call NICU APP to order IM
Amp as concentration is different.
[ ] Discuss PIV removal with provider
[ ] Hearing screen after antibiotics are
infused
Newborn Management Highlights
• CBC drawn at 24h
• Blood culture at birth (placenta or peripheral)
• Antibiotics for 48 hrs
Vitals (frequency)Other Vital
Signs/AssessmentsProvider Evaluation
At birth x1
q15” x4
q30” x4
q2° x4
q3-4° until 48o
then unit routine
BP, mean BP, central cap
refill:
x1 in L&D
w/ all VS after
If newborn vitals fall outside
of order set parameters,
contact the hospitalist for
newborn evaluation.
Role of the Delivering staff
• Initial EOS scoring with diagnosis
• Preparation of pump and IV tubing
• If at time of delivery the newborn is vigorous,
may go skin-to-skin
• Delayed cord clamping
• APP will examine the newborn
• NICU staff will obtain blood cultures from the
placenta
4/3/2018
11
Role of the Delivering staff (cont)
• Weigh the newborn asap for antibiotic order
• NICU staff to start IV
• Pharmacy provides RTA antibiotic versus needing to reconstitute
• Labor and Delivery nurse to start IV antibiotic within 1 hour of delivery- preferably Amp
• The labor nurses will determine who will coordinate VS, glucose check, release of Suspected Sepsis order set
Role of the Postpartum staff
• Hand off from Labor and Delivery staff
• Assessment of mother and baby on arrival
• Pediatric notification of newborn on the unit
• PIV restarts- Should the PIV infiltrate, consider
if last dose of Ampicillin can be given IM. NICU
IV restart versus Vascular Access team
• Timing of hearing screen
Role of the Postpartum staff (cont)
• Discharge timing- the newborn should not be
discharged sooner than 48 hours after birth
due to antibiotic therapy
• The mother is able to be discharged if meets
discharge milestones, baby remains a patient
until appropriate
• No change to the newborn bath timing- bath
does not need to be delayed or expedited

4/3/2018
12
General
• Poor feeding
• Irritability
• Lethargy
• Temperature instability
Central nervous system
• Hypotonia, stupor, poor spontaneous
movement, coma
• Irritability
• Seizures, rigidity
• Bulging anterior fontanelle
Respiratory
• Grunting
• Nasal flaring
• Intercostal retractions
• Tachypnea, apnea, irregular respirations
• Abnormal breath sounds, decreased breath
sounds, rales
Circulatory
• Bradycardia, tachycardia
• Hypotension
• Cyanosis
• Decreased perfusion (pallor, gray,
mottled, ashen, delayed capillary refill)
Metabolic
• Hypoglycemia/Hyperglycemia
Other
• Jaundice
The clinical signs of early onset sepsis are nonspecific and are associated with the causative organism. Therefore,
it is prudent to provide treatment for suspected neonatal sepsis while excluding the presence of infection.
A frequent indication of serious
infection is an inability to
maintain the body temperature in
the neutral thermal zone
(usually 97.7°F and 99°F axillary).
Newborn Suspected Sepsis Management Order Set
Frequency of Vital Signs (HR, RR,
Temperature, Oxygen Saturation
and Central Capillary Refill)
• At Birth
• Every 15 minutes X4
• Every 30 minutes X4
• Every 2 hours X4
• Every 3-4 hours with feeding
cues and cares
Blood pressure (including mean
pressure)
• Once in the delivery room
within 2 hours after birth
• Every 3-4 hours with feeding
cues and cares

4/3/2018
13
The newborn will receive more frequent monitoring of clinical presentation
and vital signs for the first 12 hours. Notify the APP if the newborn has, at
least 2 instances of 1 of the following, with “instance” meaning that there
were 2 measurements 2 hours apart.
• Report abnormal findings to the APP.
• Heart rate greater than 160
• Temperature greater than 100.4oF or
less than 97.5oF
• Respiratory distress (grunting, flaring, or
retracting)
Newborn Suspected Sepsis Management Order Set
• It is important to obtain, monitor and document mean cuff pressure
{arterial pressure (MAP)} in the newborn born with risk of early onset
sepsis.
• The mean pressure is an important indicator of blood pressure change,
and represents the newborn’s average tissue perfusion pressure.
• Mean cuff pressure values are easier to trend than changes in systolic or
diastolic pressures.
IMPORTANCE OF MEAN CUFF PRESSURE
Report a mean cuff pressure of
less than 35 mmHg to the APP.
Determine and document mean
cuff pressure with every BP.
Although you may hear this value reported as the MAP (mean arterial pressure), it is more accurate to refer
to this value as the mean cuff pressure. A MAP is used when monitoring arterial BPs via an arterial line.
Hypotension with decreased perfusion and diminished pulses are signs of early onset sepsis. In
addition to vital signs like blood pressure, signs of decreased perfusion must be evaluated in the
newborn at risk for EOS.
Central capillary refill will be evaluated with each vital sign.
1. Blanch the skin on the newborn’s chest.
2. Watch for blood return.
3. If capillary refill takes greater than 3 seconds, report
capillary refill time, blood pressure, and mean cuff
pressure to the NNP.
ASSESSING CENTRAL CAPILLARY REFILL

4/3/2018
14
• The newborn at risk for early onset sepsis
is at risk for metabolic symptoms including
hypoglycemia.
• Blood glucose will be checked in the
delivery room 30 minutes after the first
feeding attempt but no later than 2 hours
of age.
• If the baby has other risk factors for
hypoglycemia, initiate the hypoglycemia
order set and algorithm.
How should I staff for these babies?
Labor: Staff a nurse for mom and a nurse
for baby with the delivery.
Postpartum: Consider staffing up the first
several hours of life.
Utilize the Resource Nurse to assist with
vitals, etc.
Outcomes
Measure Target, % Actual, %
Accurate documentation of Escobar stratification 100 75
Percentage of eligible newborns born to mothers
with Triple I who were managed on NFCC
90 100
Start infusion of initial antibiotic within 1 hour of
birth
100 41
Newborn EOS order set entered by APP at delivery 100 100
Exclusive breastfeeding at discharge (those babies
who were admitted directly to the NFCC)
95 62
Missed identification of sepsis or delay in NICU
transfer of baby with adverse change in condition
0 0
All infants were appropriately dispositioned.
22 in NFCC
15 in NICU (7 were transferred to NFCC once stable)
Families expressed relief not being separated from their babies

4/3/2018
15
Patient Experience
• “I felt so comfortable having my baby in my
room with me and knowing that we both had
the same nurse, put me at ease.”
• “I am so thankful to have my baby with me. I
can hold her and breastfeed anytime I want.”
• “Thank you for letting my baby stay with me.”
Lessons… Issues…
• Assess the scope of your project as you learn more about the
issue
• Identify the right team and engage early in regular
communications
• Ask for honest feedback
• Look at education gaps and roll out learning modules early in
the process
• Ask for EPIC builds early
– Automated reporting of new cases is currently being trialed
– Need for institution-specific baseline EOS data
• Acknowledge staff efforts
Sustainability
• Stressing the importance of this project to our
customers and the organization
• Clearly assigned roles, becomes part of the routine
• Regular review of cases every 2 months
• We have a small number of subjects (may see a
bump)
– Historically UMMC has seen 44-45 “chorio” infants admitted
to NICU annually
– Visual reminders
• Posting results

4/3/2018
16
Project Evolution
• Roll out: Ridges and in process at Maple Grove
and the University of Chicago. Interest shown
at Mercy Hospital in Des Moines
• State, National and International OB and
Hospitalist conferences and workshops
• 2018 National AWHONN conference- poster
• Selective use of antibiotics is a possibility in
the future as results are analyzed
Acknowledgements
• Tom George, MD
• Cathy Bendel, MD
• Angela Hanson, MD
• Marla Mills, RN
• Shelly Krueger, RN
• Cathy McCarty, RN
• Becky Gams, APNL
• Nanette Vogel, CDS
• Janet Kubly, RPh
• Christie McNeil, RN
• Kim Killam, RN
• Marylou Salzer, RN
• Darla Nyquist, NNP
• Julianne Cramer, APNL
• Caroline Kaylor, NNP
• Brittany Stanley, NNP
• Jodie Allen, RN
• Sheila Powers, RN
• Lisa Archer, RN
• Debbie Allen, IBCLC, NNP
• Sponsor: Jordan Marmet, MD
• Sponsor: Jody Rock, RN
• Coach: Kyung Park, RN
This project would not be possible without
the support and dedication of these people
THANK YOU!
• “We see our customers as invited guests to a party, and we are
the hosts. It’s our job every day to make every important aspect
of the customer experience a little bit better.” (Jeff Bezos)
• “You’ve got to start with the customer experience and work
back toward the technology, not the other way around.” (Steve
Jobs)

4/3/2018
17
Contact Information
• Cindy Osborn
• Alexander Gurfinkel
References
• ACOG (2017). Intrapartum management of intraamniotic infection. Committee. Opinion No. 712. American College of Obstetricians and Gynecologists. Obstetrics & Gynecology, 130 (2). e95–101.
• Escobar, G. J., Puopolo, K. M., Wi, S., Turk, B. J., Kuzniewicz, M. W., Walsh, E. M., Newman, T. B., Zupancic, J. Lieberman, E. & Draper, D. (2014). Stratification of risk of early-onset sepsis in newborns ≥ 34 weeks’ gestation. Pediatrics 133(1), 30-36. doi: 10.1542/peds.2013-1689
• Higgins et al. (2016). Evaluation and management of women and newborns with a maternal diagnosis of chorioamnionitis: Summary of a workshop. Obstetrics & Gynecology, 127 (3), 426-36. doi: 10.1097/ACOG.0000000000001246
• Puopolo, K.M. (2016, September 9). Assessing risk of early onset sepsis among term infants. Retrieved from http://www.d6an.org/uploadFunctionality2/files/Puopolo%20Early%20Onset%20Sepsis.pdf
• Puopolo, K. M., Draper, D., Wi, S., Newman, T. B., Zupancic, J., Lieberman, E., Smith, M.Y. & Escobar, G. J. (2011). Estimating the probability of neonatal early-onset infection on the basis of maternal risk factors. Pediatrics, 128(5), e1155-1163. doi: 10.1542/peds.2010-3464
Let’s Review
Early Onset Sepsis QUIZ