diuretics
DESCRIPTION
notesTRANSCRIPT
Cardiovascular/Renal: DIURETICS
WardeHeheman

Regulation of Blood Pressure
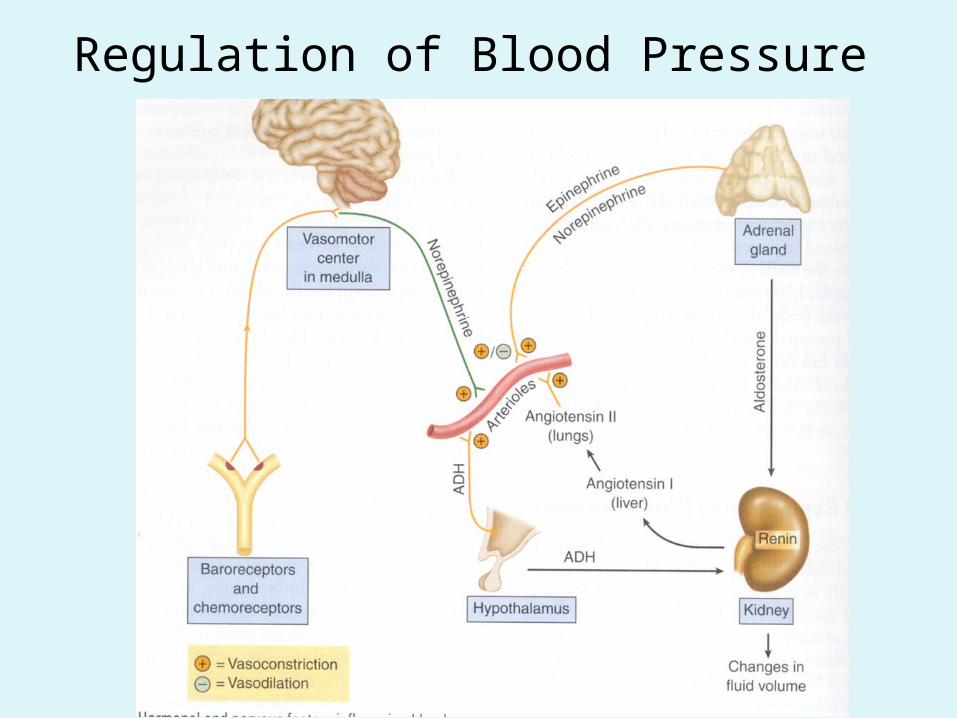
Regulation of Blood Pressure

Diuretics

Review of the Kidney • Kidney, 3 functions: – Cleansing of extracellular fluid and maintenance of
ECF volume and composition– Maintenance of acid-base balance– Excretion of metabolic wastes and foreign
substances.

Review of Kidney Funcion:• Three Basic Processes: Filtration, Reabsorption, &
Active Secretion• 1. Filtration- occurs at the glomerulus; first step in
urine formation– Nonselective process; cannot regulate composition of urine
• 2. Reabsorption- More than 99% of water, electrolytes & nutrients filtered at glomerulus undergo reabsorption– Solutes reabsorbed by active transport– Water follow passively along the osmotic gradient created by
solute reuptake– PD:**Diuretics work by interfering with reabsorption

Review of the Kidney
• Active Tubular Secretion– Kidney: two major pumps for secretion– Organic acid pump– Organic base pump– Excrete a wide variety of molecules: metabolic wastes,
drugs, & toxins– Pumps for active secretion: located in proximal
convoluted tubule


Review of the Kidney• Reabsorption at Specific Sites in Nephron:• Proximal Convoluted Tubule (PCT)– High absorptive capacity, 65% of filtered sodium &
chloride is reabsorbed in PCT– Almost all bicarbonate & potassium in filtrate is
reabsorbed PCT– When filtrate leaves PCT, sodium & chloride are only
solutes that remain in significant amounts
Review of the Kidney• Reabsorption at Specific Sites along the Nephron:• Loop of Henle: – Descending limb is freely water permeable• Water drawn into the interstitial spaces (from the loop)• Concentrates urine
– Ascending limb reabsorbs 20% of filtered sodium & chloride• This portion is not water permeable, water stays in,
sodium & chloride move out. (Returns tubular urine to it’s original tonicity (osmolality)

Review of the Kidney• Reabsorption at Specific Sites Along the Nephron:• Distal Convoluted Tubule (Early Segment)– Reabsorbs 10% of sodium & chloride, water follows
passively• Distal Nephron (Late Distal Convoluted Tubule &
Collecting Duct)– Exchanges sodium for potassium; regulated by aldosterone
• Aldosterone reabsorbs Na+ and gets rid of K+
– Determines final concentration of urine, regulated by antidiuretic hormone (ADH).• ADH allows collecting duct to be permeable to water (body
reabsorbs more water), without ADH large amounts of water can leave the body

PD: How Diuretics Work• PD: Most diuretics share same mechanism of action:
blockade of sodium and chloride reabsorption– Creates osmotic pressure inside nephron that blocks passive
reabsorption of water– If water and solutes are not reabsorbed, they are excreted
from the body• The increase in urine flow is directly related to the
amount of sodium & chloride reabsorption blocked• Diuretics that act early in nephron block the greatest
amount of solute reabsorption (greatest results)• Diuretics increase urine output (UOP) by 1.8 L for every
1% of solute reabsorption that is blocked; if give TOO much, = dehydration


Adverse Effect: Impact on ECF• Diuretics can cause:– Hypovolemia (from excessive fluid loss)– Acid-base imbalance– Altered electrolyte levels.– Short-acting diuretics minimize these effects.
Classification of Diuretics• High ceiling (Loop) diuretics- Furosemide (Lasix)• Thiazide diuretics – hydroclorothiazide (HCTZ)• Osmotic diuretics – mannitol (Osmitrol)• Potassium-sparing diuretics: –Aldosterone antagonists – spironolactone
(Aldactone)–Nonaldosterone antagonists- triamterene
(Dyrenium)

High-Ceiling (Loop) Diuretics• Most effective diuretics available• Produce more loss of fluid & electrolytes than
any other diuretic• Furosemide (Lasix) is most frequently
prescribed loop diuretic
Loop Diuretics: Furosemide• Sulfa based drug* assess hypersensitivity• Acts in ascending limb, Loop of Henle; blocks
reabsorption of sodium & chloride• Can produce profound diuresis• Can be given orally (diuresis starts within 60
minutes, lasts 8 hrs), IV (diuresis in 5 minutes, lasts 2 hrs) and IM.
• *IV therapy is used in critical situations (pulmonary edema)
• *Typically used when less powerful diuretics no longer (*but not always)
Loop Diuretics: Furosemide• Therapeutic Uses:• Pulmonary edema associated with congestive
heart failure• Edema of hepatic, cardiac or renal origin that is
unresponsive to less efficacious diuretics• Hypertension that cannot be controlled with other
diuretics• Other:____• Especially useful in pts with severe renal
impairment, can promote diuresis even when renal blood flow and glomerular filtration rate are low

Loop Diuretics: Furosemide• Adverse Effects:• Hyponatremia, Hypochloremia & Dehydration b/c
can produce excessive loss of sodium, chloride, & water – Severe dehydration can result (hold lasix if dehydration
occurs)– S/S of dehydration: dry mouth, unusual thirst, oliguria,
muscle cramps, anorexia, lethary, restlessness, excessive weight loss
– Dehydration can promote thrombosis & embolism (headache, pain in chest/clavicle, or pelvis)
– Can be minimized by low dose therapy & adjusting dose daily

Loop Diuretics: Furosemide• Adverse Effects:• Orthostatic Hypotension – Due to loss of volume
and relaxation of venous smooth muscle (reduces venous return to the heart).– Monitor BP regularly (teach to monitor at home)– Can cause acute hypotensive episodes from rapid
changes in FV, can lead to circulatory collapse *Elderly • Hypokalemia- Potassium loss due to increased
secretion in distal nephron– Encourage potassium rich foods
Loop Diuretics: Furosemide• Adverse Effects:• Ototoxicity- Rarely causes permanent
deafness/hearing impairment, most hearing impairment is transient, (Usually in high dose, IV, renal impaired)• In ethacrynic acid (Edecrin), another loop diuretic hearing
loss can be permanent– Use caution when given with other ototoxic meds
• Hyperglycemia- Can result from inhibition of insulin release. Watch closely in diabetic pts. (uncommon)
• Hyperuricemia- Frequent, most pts are asymptomatic, but for pts predisposed to gout can cause a gout attack
Loop Diuretics: Furosemide• Adverse Effects:• Pregnancy- Class C, Only used if no other
alternative & with caution (not studied on humans/lab animals caused maternal death, abortion, & and other adverse effects)
• Lipids, Calcium & Magnesium- Furosemide decreases HDL, raises LDL cholesterol & triglycerides. Increases risk of magnesium deficiency, increased excretion of calcium (*elders with Osteoporosis are at risk for fractures)

Loop Diuretics: Furosemide• Drug Interactions:• Digoxin- If potassium is low, serious risk of drug-
induced toxicity (ventricular dysrhythmias) • Ototoxic drugs- (Especially gentamycin) can cause
permanent hearing loss. Avoid combined use of these drugs.
• Potassium-Sparing Diuretics- Can reduce the risk of hypokalemia
• Lithium- Can allow lithium levels to accumulate to toxic levels

Other Loop Diuretics: • Ethacrynic acid (Edecrin) Not sulfa based, safe for
use in sulfa allergy, not for use in children, for edema only, not HTN
• Torsemide (Demadex) metab. to active & inactive metabolites
• Bumetanide (Bumex) for edema only, more potent, *black box warning: More profound diuresis (H2O & electrolytes), not for children, *careful dosing
Loop Diuretics: Furosemide• Drug Interactions:• Anithypertensive Agents- Furosemide can cause
hypotension, potentiated by antihypertensive drugs• Nonsteroidal Aspirin, Anti-inflammatory Drugs
(NSAIDS)- Decrease the effects of diuretics, ACE inhibitors (1st dose hypotension) others… see table
• Contra’s: Sulfa allergy/hypersensitivity, Precautions: *poor renal function, SLE (lupus) Assess

Thiazide Diuretics• PD: Increase renal excretion of sodium, chloride,
potassium, & water• Elevates plasma levels of uric acid & glucose• Greatest difference between thiazides & loop
diuretics: maximum diuresis of thiazides is considerably lower than in loop diuretics
• Thiazides are not effective when urine flow is scant (anuria, severe renal failure)
• Sulfa based drug

Thiazides: Hydrochlorothiazide • Hydrochlorothiazide (HydroDIURIL, HCTZ) most
widely used thiazide diuretic• Promotes urine production by blocking
reabsorption of sodium & chloride in the early segment of the distal convoluted tubule
• Since only 10% of filtered sodium & chloride is normally absorbed where thiazides act, maximum urine flow is lower than with Loop Diuretics
• Cannot be used to promote fluid loss in pts with severe renal impairment
Thiazides: Hydrochlorothiazide • Therapeutic Uses:• Essential Hypertension- Primary use is for HTN, and
is often FIRST DRUG OF CHOICE.• Edema- Mild to moderate, heart failure• Diabetes Insipidus- Causes fluid retention instead
(unsure why)• Postmenopausal Osteoporosis Protection,Promotes
tubular reabsorption of calcium
Thiazides: Hydrochlorothiazide • Adverse Effects:• Hyponatremia, Hypochloremia & Dehydration-
Milder than loop diuretics• Hypokalemia- Eat potassium rich foods, *careful if
taking digoxin.• Pregnancy and Lactation: Direct and Indirect
effects on developing fetus, and impair fetal blood flow– Should not be used routinely during pregnancy,
caution

Thiazides: Hydrochlorothiazide • Adverse Reaction:• Hyperglycemia- Can elevate glucose in diabetic
pts• Hyperuricemia- Retention of uric acid, can cause
gout.• Lipid and Magnesium- Increase LDL, total
cholesterol and triglycerides. Can cause magnesium deficiency.

Thiazides: Hydrochlorothiazide • Drug Interactions:• Same as loop diuretics, Slightly different chemical
structure, indications for use, PK’s• Other Thiazide-Type diuretics:– True Thiazides:• Chlorothiazide (Diuril)• Methyclothiazide (Enduron)
– Related to Thiazides:• Chlorthalidone (Hygroton) not for children, longer half-life
Indapamide (Lozol) specific for edema in CHF, not for children, highly metab. in liver, caution liver impaired• Metolazone (Zaroxolyn) not for children

Potassium-Sparing Diuretics • Produce increased urine production, but limited,
so not often used for diuresis• Produce substantial decrease in potassium
excretion, so these drugs are often used to counteract potassium loss caused by thiazide & loop diuretics.
• Two subcategories:– Aldosterone Antagonists- spironolactone (Aldactone)– Non-aldosterone antagonists- triamterene
(Dyrenium) and amiloride (Midamor)
Potassium-Sparing Diuretics: Spironolactone
• PD: Blocks the actions of aldosterone in distal tubule, (blocks all aldosterone receptors: glucocorticoid, mineral corticoid, androgen, & progesterone)
• Aldosterone promotes sodium uptake in exchange for potassium secretion
• PD: Spironolactone causes retention of potassium and increased excretion of sodium• Effects of spironolactone are delayed (typically takes 48
hrs) because it blocks the action of new proteins but does not stop existing transport proteins

Potassium-Sparing Diuretics: Spironolactone (Aldactone)
• Therapeutic Uses:• HTN & Edema- Most commonly used in
combination with a loop or thiazide diuretic to counteract the potassium-wasting effects of the more powerful diuretics
• Heart Failure (CHF) Proven to reduce mortality and hospital admissions
• Other Uses- Primary hyper-aldosteronism, Off label: premenstrual syndrome, polycystic ovary syndrome, acne * assess what drug is used for

Potassium-Sparing Diuretics: Spironolactone
• Adverse Effects:• Hyperkalemia- Most likely when spironolactone is
used alone, stop use if hyperkalemia develops• Endocrine effects- Similar to other steroid
hormones (progesterone, estradiol, testosterone). Can cause gynecomastia, menstrual irregularities, impotence, hirsutism & deepening of the voice.

Potassium-Sparing Diuretics: Spironolactone
• Drug Interactions• Thiazide & Loop diuretics- given to counteract the
potassium-wasting effects.• Agents that raise potassium levels should never
be given with potassium supplements, salt substitutes or another potassium-sparing diuretic – If given with ACE Inhibitors, ARBs, or direct renin
inhibitors can elevate potassium levels

Potassium-Sparing Diuretics: Triamterene (Dyrenium)
• PD: Like spironolactone, triamterene disrupts sodium-potassium exchange in the distal nephron
• PD:Triamterene is a direct inhibitor of the exchange mechanism itself
• Decreases sodium reabsorption, reduces potassium secretion
• Sodium is excreted, potassium is retained• Acts more quickly than spironolactone because it
inhibits the ion transport directly. (develops in hours vs. days)

Potassium-Sparing Diuretics: Triamterene (Dyrenium)
• Therapeutic Uses:• Used alone or in combination with other diuretics
to treat HTN & edema• If Used alone produces mild diuresis• Used in combination, it augments diuresis &helps
counteract the potassium wasting effects of the more powerful diuretic

Potassium-Sparing Diuretics: Triamterene (Dyrenium)
• Adverse Effects:• Hyperkalemia- excessive accumulation is the most
significant adverse effect, likely when triamterene is used alone. Should never be used with another potassium sparing diuretic or potassium supplements or salt substitutes. Use caution if giving with ACE Inhibitors, ARBs, or direct renin inhibitor (increase the effect of triamterene)
• Other adverse effects- nausea, vomiting, leg cramps, and dizziness.
Potassium-Sparing Diuretics: Amiloride (Midamor)
• Think Triamterene• Used primarily to counteract potassium-wasting
from other diuretics• Adverse Effect is hyperkalemia (watch out with
ACE Inhibitors, ARBs, direct renin inhibitors)

All Potassium Sparing Diuretics• Evaluation- Pt’s BP and serum potassium will
remain WNL; edema will decrease• Drugs- amiloride (Midamor); spironolactone
(Aldactone); triamterene (Dyrenium)• L- Low Sodium• E- Elevated T waves from HYPERkalemia• A- Agranulocytosis with triamterene• K- K+ level must be monitored.
Osmotic Diuretic: Mannitol
• Mannitol is the only osmotic diuretic on the market• Simple, six-carbon sugar• PD: Mechanism of Diuretic Action:– Freely filtered at the glomerulus– Undergoes minimal tubular reabsorption– Undergoes minimal metabolism– Is pharmacologically inert (no direct effects on
biochemistry or physiology of cells)– Pulls off fluid by increased osmotic force/pressure

Osmotic Diuretic: Mannitol
• Administered IV, most of the drug makes it past the glomerulus, creates increased osmotic force that inhibits passive reabsorption of water (Urine flow increases).
• Degree of diuresis is dependent upon the amount of Mannitol in the filtrate (more mannitol more diuresis)
• Does not affect the excretion of potassium or other electrolytes

Osmotic Diuretic: Mannitol• Therapeutic Uses:• Prophylaxis of Renal Failure- (dehydration,
severe hypotension, hypovolemic shock) causes low blood flow to the kidney, causing reduction in filtrate volume. Ceases urine production, =kidney failure
• Mannitol pulls water into the nephron (even when blood flow is low), preserves urine output & may prevent kidney failure

Osmotic Diuretic: Mannitol• Therapeutic Uses:• Reduction of Increased Intracranial Pressure
caused by cerebral edema. Works because its presence in the blood vessels of the brain creates an osmotic force that draws fluid from the brain into the blood (Cannot exit the capillary beds of the brain).
• Reduction of Increased Intra-occular Pressure- Renders the plasma hyperosmotic in respect to intra-occular fluids, mannitol creates the osmotic force that draws occular fluid into the blood.

Osmotic Diuretic: Mannitol• Adverse Effects:• Sudden increase of ECF / Edema- can leave the
vascular space at all capillary beds except the brain. It will draw water with it which causes edema. Watch for *CHF & *pulmonary congestion (most succeptible: pt’s with history of these).
• Other Adverse Effects- headache, nausea, vomiting, major fluid and electrolyte imbalance.

Osmotic Diuretic: Mannitol• Nursing Interventions• Administer only on a pump, low test dose on all
patients with renal impairment, patient on heart monitor, monitor ECG tracings
• Monitor UOP constantly & carefully• Assess vitals,*BP, pulse• Assess lung sounds• High risk for major F/E changes, *safety, orthostatic
hypotension• Contra’s/Prec: children, CHF pts, Preg class C, elderly
with caution, renal failure, electrolyte imbalance, others…

DIURETICD- Diet, increase K (except potassium-sparing)I- Intake, Output, and Daily Wt.U- Undesirable effects; fluid and electrolyte
imbalance.R- Review HR, BP, and electrolytesE- Elderly-cautionT- Take with or after meals and in AMI- Increased risk of orthostatic hypotensionC- Cancel alcohol