diversifying aaa/adrcs funding streams: how states … funding... · - acl has drafted a workbook...
TRANSCRIPT

Diversifying AAA/ADRCs Funding Streams:
How states and their local partners can draw down federal Medicaid Administrative
Match for ADRC/NWD Systems
July 30, 2017 n4a Conference

Agenda • What is the value of Medicaid Claiming?
– For the ADRC/NWD System/for my organization
• How is this done? – Implementation Process and Steps – Maryland & Hawaii’s Medicaid Claiming Infrastructure
• How to get buy in? – State Leadership Perspective – Colorado’s Planning Experience
• What’s Happening Now? • ACL Support and Resources
2

What is Medicaid Claiming? • Administrative Medicaid Claiming (aka Federal
Financial Participation (FFP)) is a way in which Medicaid reimburses agencies doing work that supports Medicaid programs.
• This is not a fee-for-service; agencies are not paid per activity.
• FFP reimbursement is calculated based on the results of a time study or daily time documentation
3

• Strengthens the case for State and local funding: – Local money goes twice as far – Demonstrates that the ADRC/NWD network is a core
infrastructure supporting the Medicaid program
• Ongoing source of funding: – Once approved, funding will continue – Medicaid claiming covers about 40% of costs for
Wisconsin’s ADRC/NWD
• Does not require major changes to regular operations
4
What is the Value?

Claiming and Reimbursement Process
5
Operating agency adds all participating staff into "cost
pool"
Operating agency runs time studies to capture
staff time
Local sites submit quarterly documentation of actual
expenditures to operating agency
Operating agency calculates the Medicaid %, documents costs
within the cost pool, and requests reimbursement from
state Medicaid
State Medicaid agency submits claiming report,
receives federal funds, and allocates funds to
operating agency for disbursement

Maryland’s Medicaid Claiming • Maryland uses a random moment time study (RMTS)
methodology – Staff code activity at a randomly selected time
• Less burdensome, more accurate reporting compared to 100% time tracking
• Uses a web-based RMTS software system – Automatically generates the samples each quarter
• Adapted codes that correspond to staff work – Level 1 Screen – Person Centered Counseling – Coordination of services with individuals at risk of Medicaid spend-down
6

2500 samples generated per quarter
150 staff total
Statewide Average for State Fiscal Year 2017: Medicaid Claimable
Percent = 47.65%
Total Claiming Reimbursement = $3,303,000
Maryland’s Claiming Totals
7

Deborah Stone-Walls Maui AAA, Hawaii
8
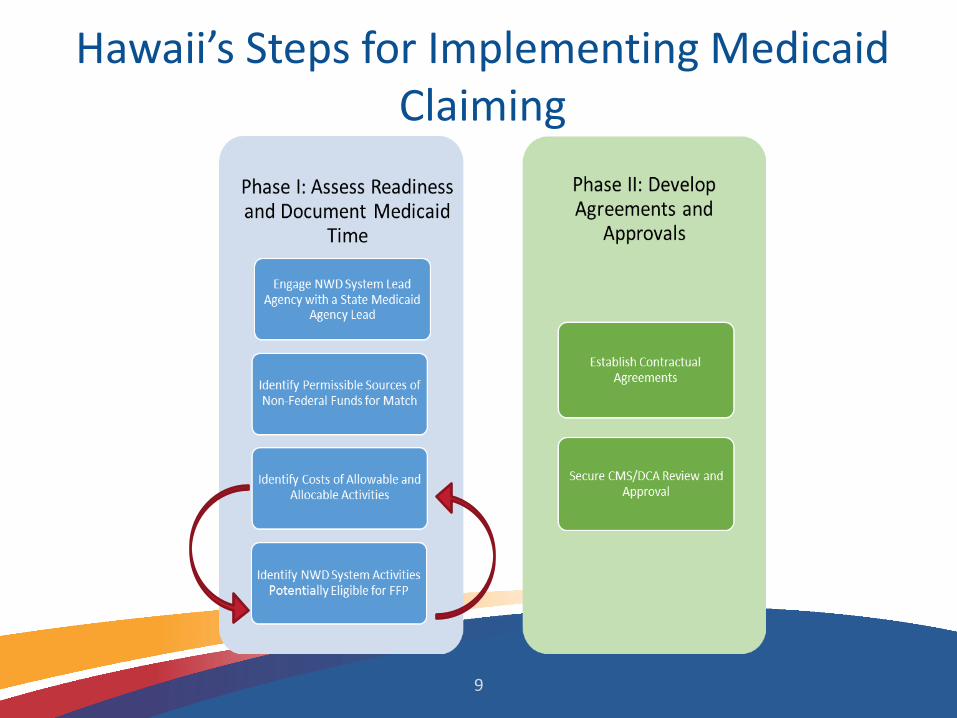
Hawaii’s Steps for Implementing Medicaid Claiming
9

Simply put….
Identify the work that we do
Tease out if the activities are related to Medicaid
Document time spent on Medicaid activities
10

Medicaid Claiming Codes • Codes should support operations • Ordered to make choice of code
clearer • Negotiated with direct staff • Training on the coding process • Random Moments pilots—Survey
Monkey • Analysis/testing of codes • Provides estimates of claimable time
11
1. Reimbursed by another source
2. Medicaid Choice Counseling
3. Call Log/Intake
4. Facilitating Program Applications
5. Assessment/Support Plan Development
6. Referral, Coordination, & Monitoring
7. Outreach
8. Training or Program Admin.
9. General Admin.
10. Other

Pilot Testing
Conduct Pilot A
• Evaluate codes during pilot
• 3 weeks • Update
codes
Conduct Pilot B
• Develop cost and time estimates
• Establish a baseline
• 3 weeks
Implement FFP
• State and Federal approval
• Ongoing time study
12

Establishing the Cost Pool • Personnel: salaries, taxes, fringe for direct,
supervisory and support staff • Operations: Lease/rental, program activities,
printing/publications/advertisement, staff training, supplies, travel, etc.
• Equipment and motor vehicle costs • Report actual costs quarterly
13

Getting Staff On Board
14

15
1. Reimbursed Directly by
Another Source
3. Call Log/ Intake
5. Assessment /Support Plan Development
6. Referral, Coordination, or
Monitoring7. Outreach
8. Training or Program
Administration
9. General Administration 10. OtherNo No No No No
Code 1
Yes
Code 3
Yes
Medicaid an option?
Yes
Code 5a
Code 5b
Code 5c
Yes No
At risk for
spenddown&
institutionalization
Yes
Tied to a specific
program
Medicaid related
Yes
Code 7a Code 7b
Yes
Yes
Code 7c
No
No
Tied to a specific
program
Medicaid related
Yes
Code 8a Code 8b
Yes
Code 8c
No
No
Yes
Code 9
Yes
Code 10
Yes
Medicaid an option?
Code 6a
Code 6b
Code 6c
Yes No
At risk for
spenddown&
institutionalization
4. FacilitatingApplication
2. Quest Integration Choice
Counseling
Code 2
Yes
NoNoNo No
Yes
Medicaid related
Code 4a Code 4b
Yes No
Not Medicaid related
Medicaid related
General administration
Further evaluation required

What’s in it for me? Increase available funding to support activities and STAFF members
Decrease ongoing funding/employment anxiety and burnout
16

Staff Training and Ongoing Monitoring
Engage ALL types of learners Staff trainings Training should have lots of examples and scenarios,
not just code definitions….practice, practice, practice FFP Time Study Guide Bi-weekly “quizzes” to keep code definitions fresh for
staff Ensures accuracy in coding
17

Helpful Hints • Talk with other states to learn from their
experiences • Early collaboration between State and local
staff and preliminary mini-pilots can improve the accuracy of codes and need for further refinement
• Provide thorough training and develop mechanism for answering ongoing questions
18

Helpful Hints, cont. • Set realistic goals for data collection and time
study duration – Smaller agencies may need more time to gather data
• Don’t over complicate!! Staff are already performing tasks; not looking to change day to day operations
• Collect complete costs for staff participating in FFP claiming (e.g., rent, utilities, etc.)
– The greater the associated costs, the higher the return
19

20
Roger Auerbach Lewin Group

What does the ADRC/NWD System do for Medicaid?
• Outreach and consumer education • Intake, triage, application assistance • Planning for future needs – Person Centered
Counseling • Delaying or preventing Medicaid eligibility • Triage and screening to prevent Medicaid spend-
down, including diversion away from long-term institutionalization by providing resources and support in the community
21

What’s in it for Medicaid?
• Reduce Medicaid costs by counseling individuals about non-Medicaid community services and developing person-centered plans
• Streamlining enrollment into Medicaid for services not provided by other programs
• Integrate and coordinate access to Medicaid services
22
Developing Draft Codes, Testing and Approval
• Develop and pilot test draft codes • Evaluate and refine codes • Design a quality management process • Secure final Medicaid approval of the proposal • Develop an MOU • Receive approval from CMS
23
Tim Cortez Colorado Department of Health Care Policy and Financing
24

Colorado’s Background
25
• ADRC grant awarded in 2005 • 16 ADRCs operating in Colorado • ADRCs are partially financed by the Older Coloradans
Act and may have local funds • Colorado received a NWD planning grant in 2014 and
the implementation grant in 2015 • The SUA requested approval to set aside a portion of
state general fund

Colorado Background, Cont.
• The SUA (CDHS) and Medicaid State Agency (HCPF) began engagement with the ADRCs in 2016
• PCG in 2017 developed time study codes and draft amendment for the Medicaid Cost Allocation Plan
– Currently in review by state staff • HZA modified the online time study platform to allow
ADRCs to respond to random time study surveys • ADRCs are currently piloting after initial pilot
26

How Can I Position My Organization?
• Understand what contributions you make or can make to support the Medicaid Program
• Engage with state agencies to identify reimbursable activities and develop time study codes
• Participate in time study pilots • Understand your responsibilities for cost reporting
and participating in time study surveys
27

Return on Investment
28
• New funds for work ADRCs are already doing • Depends on a few factors:
– Availability of funds for state match – Amount of Medicaid related activities per quarter – Local funds available
• If the costs attributable to Medicaid outweigh the administrative strings, then probably a positive ROI.

State Level Agreements
29
• MOU between State Medicaid Agency (HCPF) and State Unit on Aging (CDHS)
– SUA agrees amount of state funds to set aside – SUA submits report to HCPF requesting how much
FFP to cover program costs allocated by time – HCPF agrees to seek reimbursement and transfer
funds to SUA

Local Level Agreements
• Contracts between ADRC and SUA – ADRC submits ADRC cost reports to SUA – ADRC identifies staff to participate in Time Study
Surveys – ADRC agrees to carry out ADRC functions
30

31
Ami Patel ACL

Currently Claiming
DC
HI
MD
DE
NJ CT
RI
MA
NH
VT
ME
MT
ID
CO
WY
NV
CA
NM AZ
MN
KS
TX
IA
IL
WI
TN
IN OH
MI
AL MS
AR
LA
GA
WV
PA
OR SD
ND
MO
OK
NE
NY
SC
NC
KY
FL
VA
AK
WA
Planning
11 states currently claiming for ADRC/NWD activities 13 in the planning phase
ADRC/NWD System Medicaid Claiming
32

What’s Happening Now? • CMS recently issued the “No Wrong Door System Reference
Document for Medicaid Administrative Claiming Guidance” to assist NWD states with implementing Medicaid claiming.
• ACL Workbook and Guidance: - ACL has drafted a workbook that includes various tools and
guidance documents for states to use as they develop a claiming infrastructure. These tools include:
- PowerPoint presentations for engagement of NWD partners and stakeholders
- Cost simulator - Claiming code guidance - Cost allocation spreadsheets, and more
33

Resources
https://nwd.acl.gov
https://www.medicaid.gov/medicaid/financing-and-reimbursement/admin-claiming/no-wrong-door/index.html
34

Contacts
35
Ami Patel [email protected]
Administration for Community Living
Deborah Stone-Walls, [email protected]
Maui, Hawaii Area Agency on Aging
The Lewin Group
Colorado Dept. of Health Care Policy and Financing
Tim Cortez [email protected]
Roger Auerbach [email protected]