dizziness: the basic
TRANSCRIPT

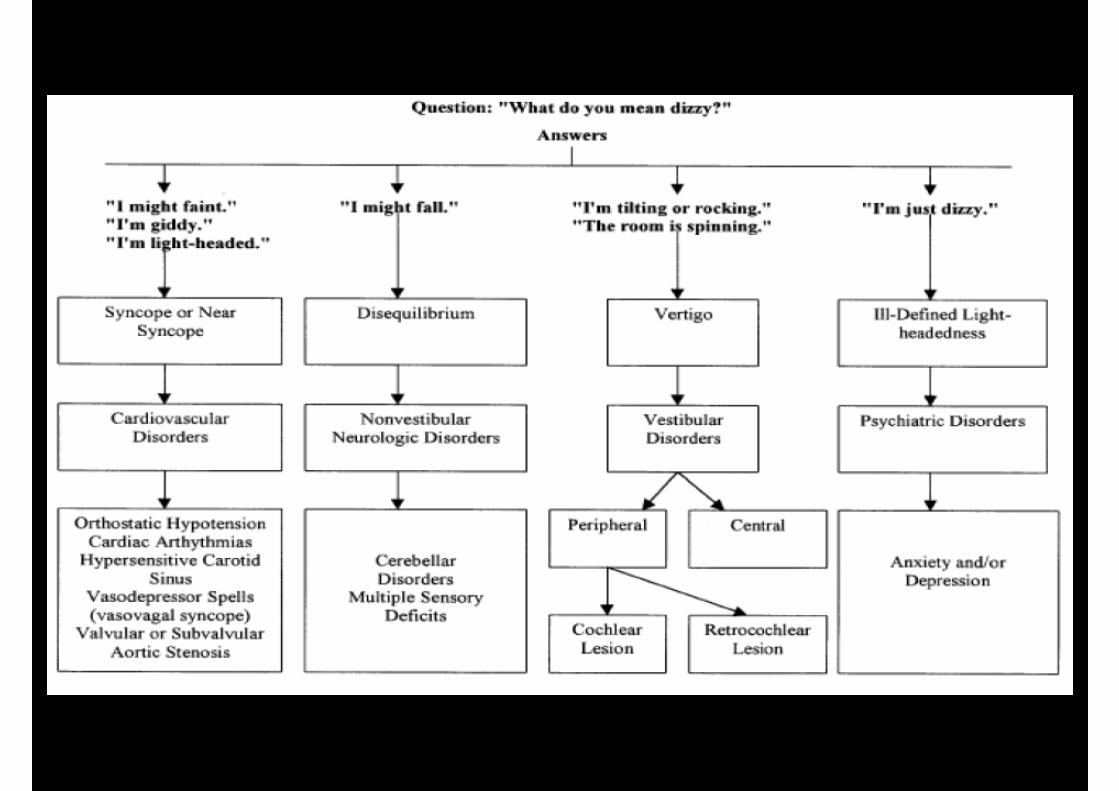
Vertigo

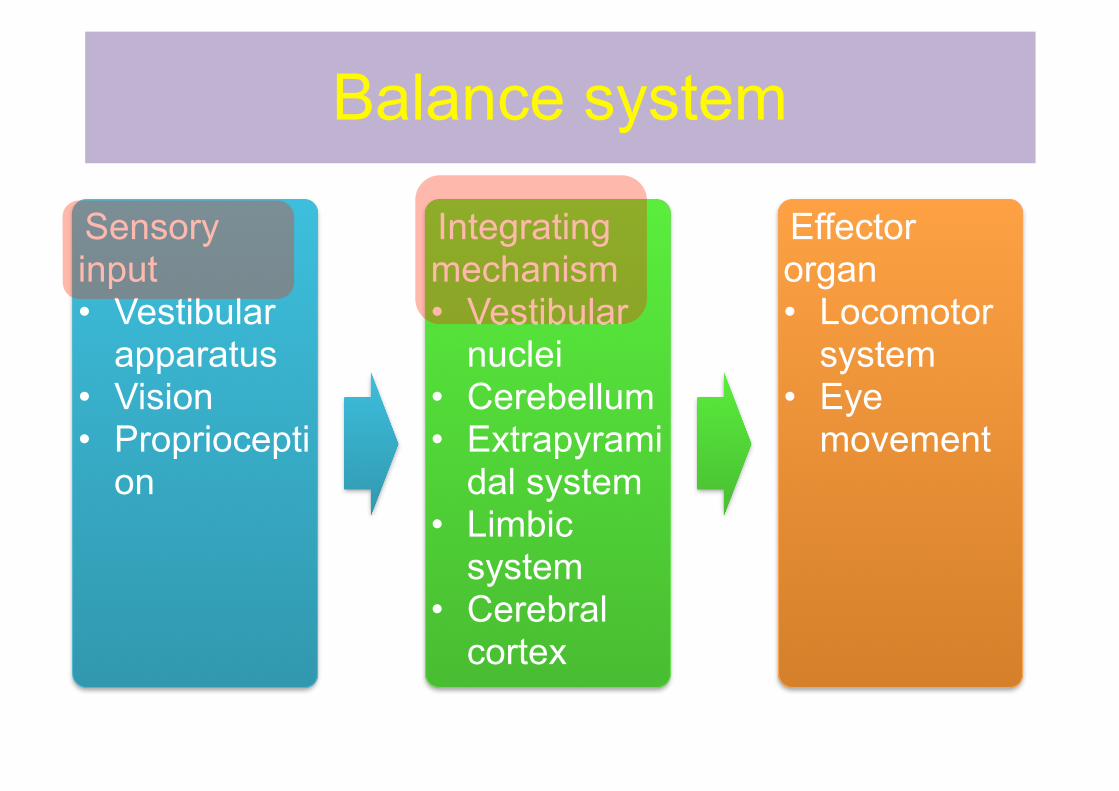
Balance system
Sensory input • Vestibular
apparatus • Vision • Propriocepti
on
Integrating mechanism • Vestibular
nuclei • Cerebellum • Extrapyrami
dal system • Limbic
system • Cerebral
cortex
Effector organ • Locomotor
system • Eye
movement
Difficult in diagnosis
• Complexity of balance system • Adaptation of system
– Uni-bilateral – Acute-chronic
• Varies of symptoms • Various etiology
– Systemic – Degeneration – Aging

Compensatory mechanism in human
• Vestibular compensation – Adaptation and learn new behavior – Rapid symptom recovery following peripheral
pathology • Variety of process
– Adaptation/habituation: recalibration of the gain of the vestibular reflex
– Substitution of sensory input and motor response, together with alteration of stretegies used for balance

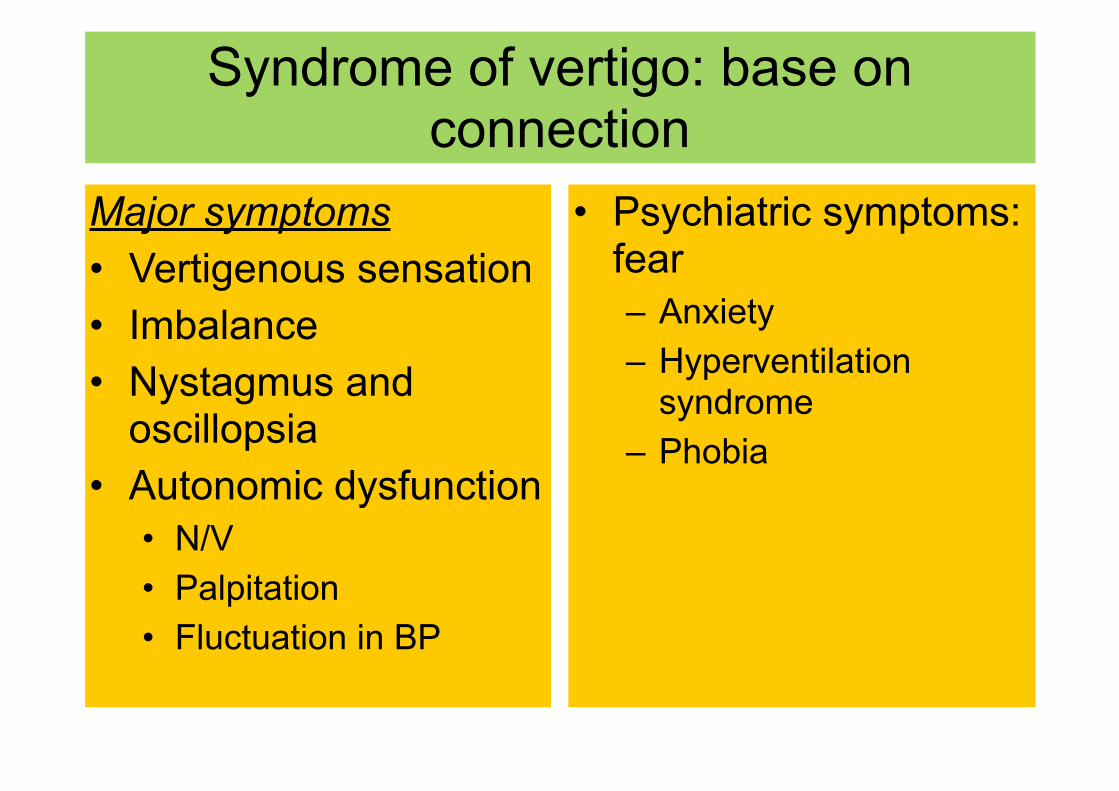
Syndrome of vertigo: base on connection
Major symptoms • Vertigenous sensation • Imbalance • Nystagmus and
oscillopsia • Autonomic dysfunction
• N/V • Palpitation • Fluctuation in BP
• Psychiatric symptoms: fear – Anxiety – Hyperventilation
syndrome – Phobia
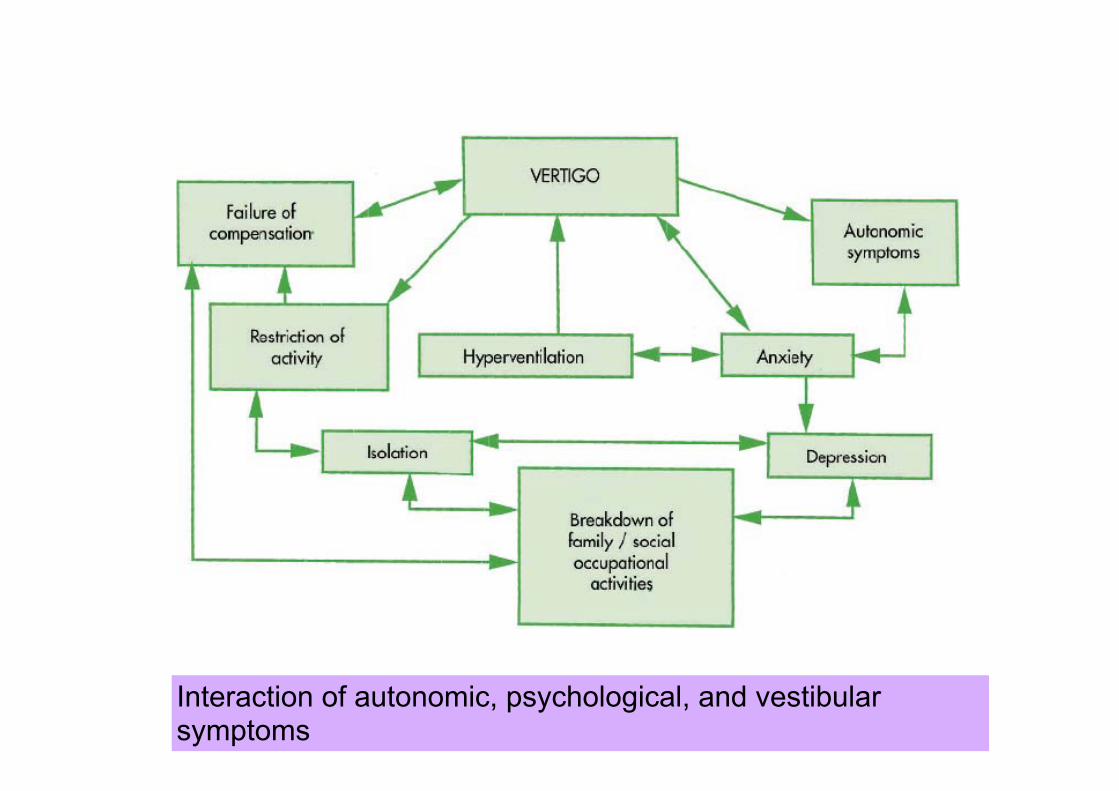
Interaction of autonomic, psychological, and vestibular symptoms
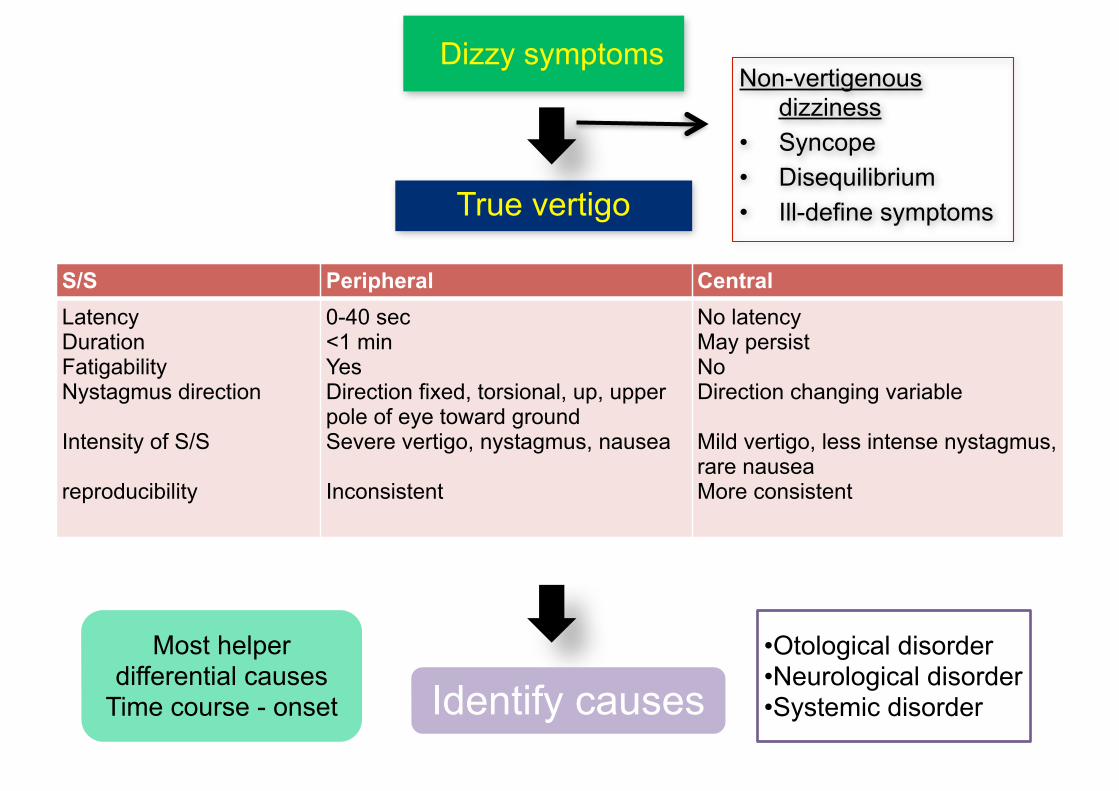
Dizzy symptoms
True vertigo
Non-vertigenous dizziness
• Syncope • Disequilibrium • Ill-define symptoms
S/S Peripheral Central Latency Duration Fatigability Nystagmus direction !Intensity of S/S !reproducibility
0-40 sec <1 min Yes Direction fixed, torsional, up, upper pole of eye toward ground Severe vertigo, nystagmus, nausea !Inconsistent
No latency May persist No Direction changing variable !Mild vertigo, less intense nystagmus, rare nausea More consistent
Identify causes•Otological disorder •Neurological disorder •Systemic disorder
Most helper differential causes
Time course - onset
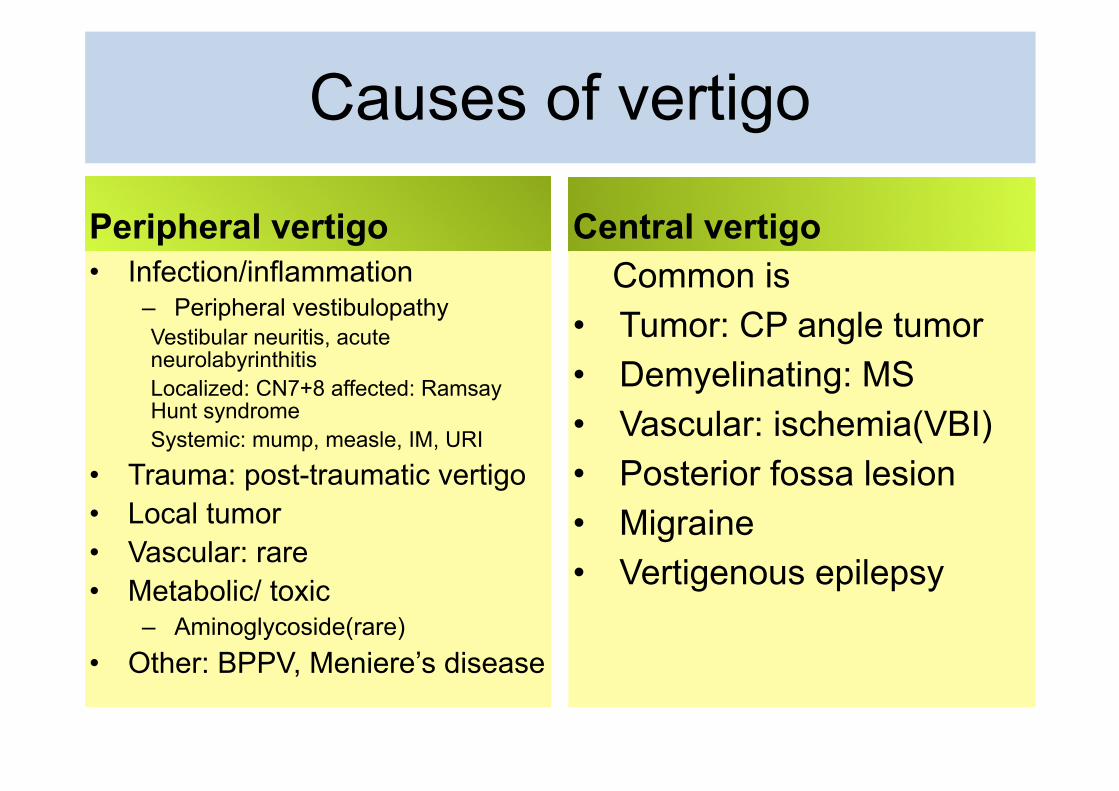
Causes of vertigo
Peripheral vertigo• Infection/inflammation
– Peripheral vestibulopathy Vestibular neuritis, acute neurolabyrinthitis Localized: CN7+8 affected: Ramsay Hunt syndrome Systemic: mump, measle, IM, URI
• Trauma: post-traumatic vertigo • Local tumor • Vascular: rare • Metabolic/ toxic
– Aminoglycoside(rare) • Other: BPPV, Meniere’s disease
Central vertigoCommon is
• Tumor: CP angle tumor • Demyelinating: MS • Vascular: ischemia(VBI) • Posterior fossa lesion • Migraine • Vertigenous epilepsy
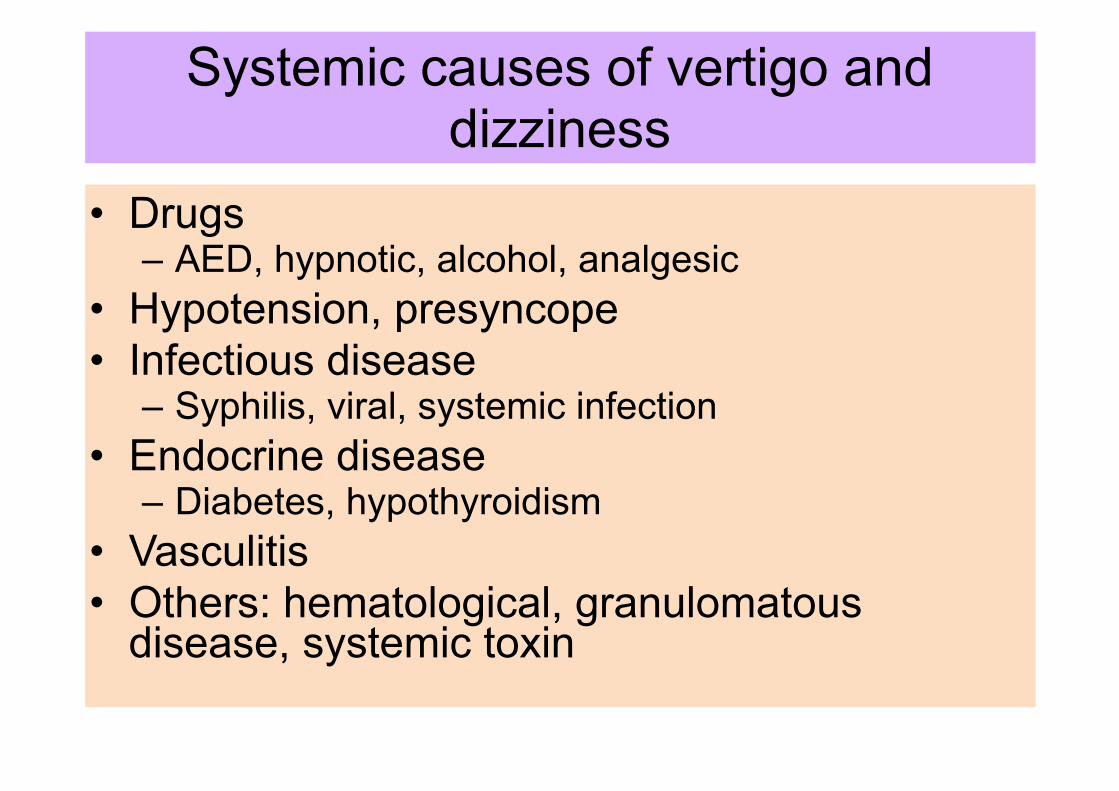
Systemic causes of vertigo and dizziness
• Drugs – AED, hypnotic, alcohol, analgesic
• Hypotension, presyncope • Infectious disease
– Syphilis, viral, systemic infection • Endocrine disease
– Diabetes, hypothyroidism • Vasculitis • Others: hematological, granulomatous
disease, systemic toxin
Some point
• Acute vestibular vertigo • Mimicker peripheral VS central • Some central cause: only vertigo S/S • Acute can caused by vascular VS non-
vascular • Episodic caused by various etiology • Pattern recognition: • Use anatomical and time course-onset
together
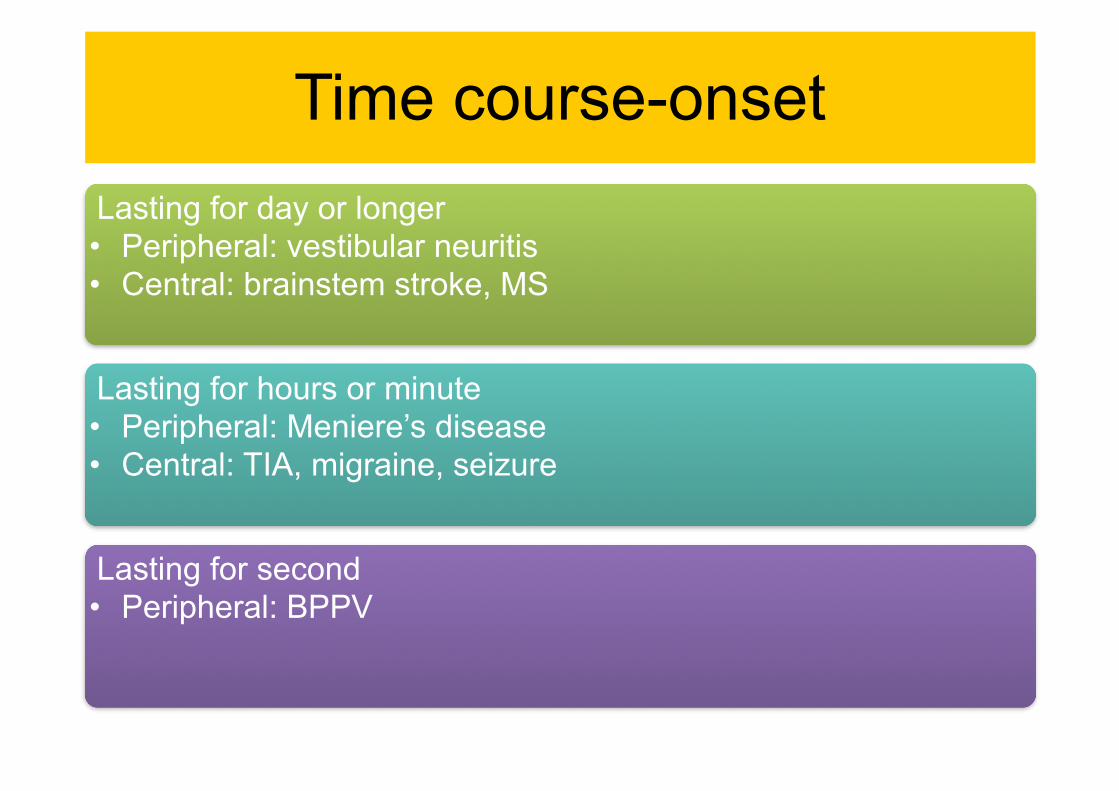
Time course-onsetLasting for day or longer • Peripheral: vestibular neuritis • Central: brainstem stroke, MS
Lasting for hours or minute • Peripheral: Meniere’s disease • Central: TIA, migraine, seizure
Lasting for second • Peripheral: BPPV

Vertigo lasting for day or longer
Vestibular neuritis• Acute • Few hours, peaks in day,
improve within day to weeks
• Viral or post viral?
Brain stem stroke• Sudden • Evidence of
vertebrobasilar ischemia • Some can mimick
peripheral cause: inferior cerebellar and flocculonodular lobe
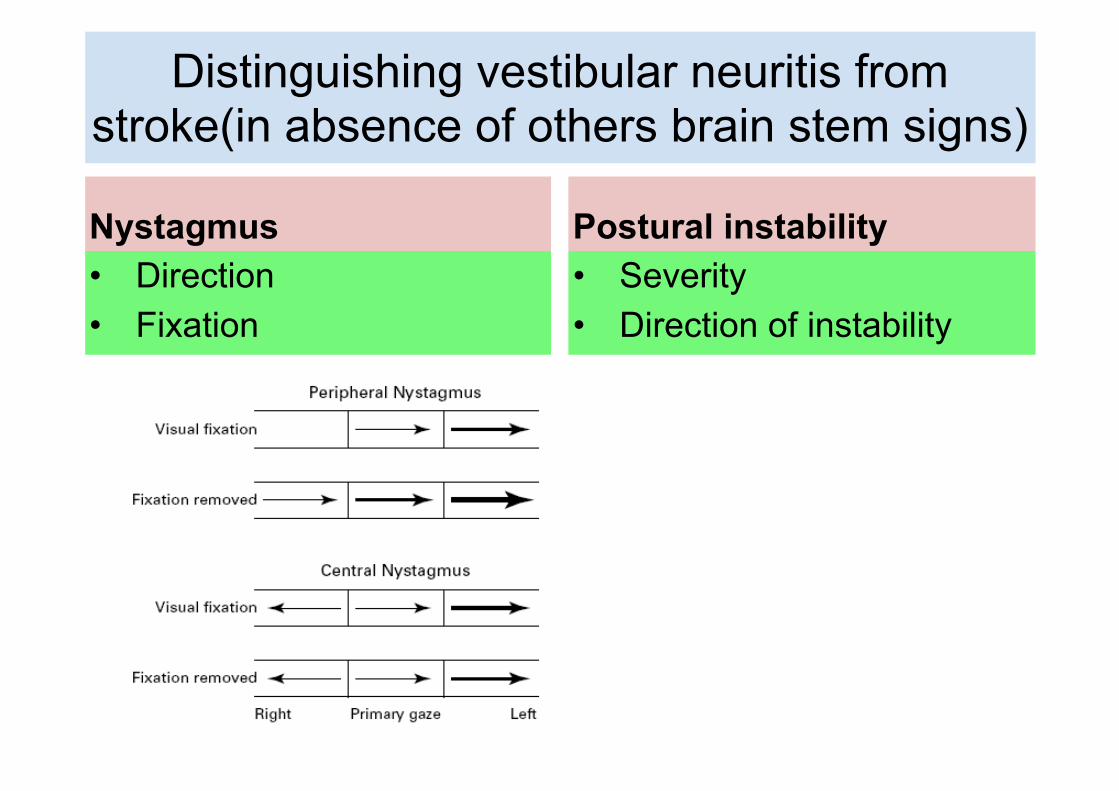
Distinguishing vestibular neuritis from stroke(in absence of others brain stem signs)
Nystagmus• Direction • Fixation
Postural instability• Severity • Direction of instability

Peripheral vertigo management
Five main arms of management intervention: • General medical evaluation, with correction/
ameliorationnof associated morbid conditions • Pharmacological intervention • Vestibular rehabilitation with physiotherapy and
specific physical manoeuvres for the management of benign positional paroxysmal vertigo
• Psychological intervention • Surgery

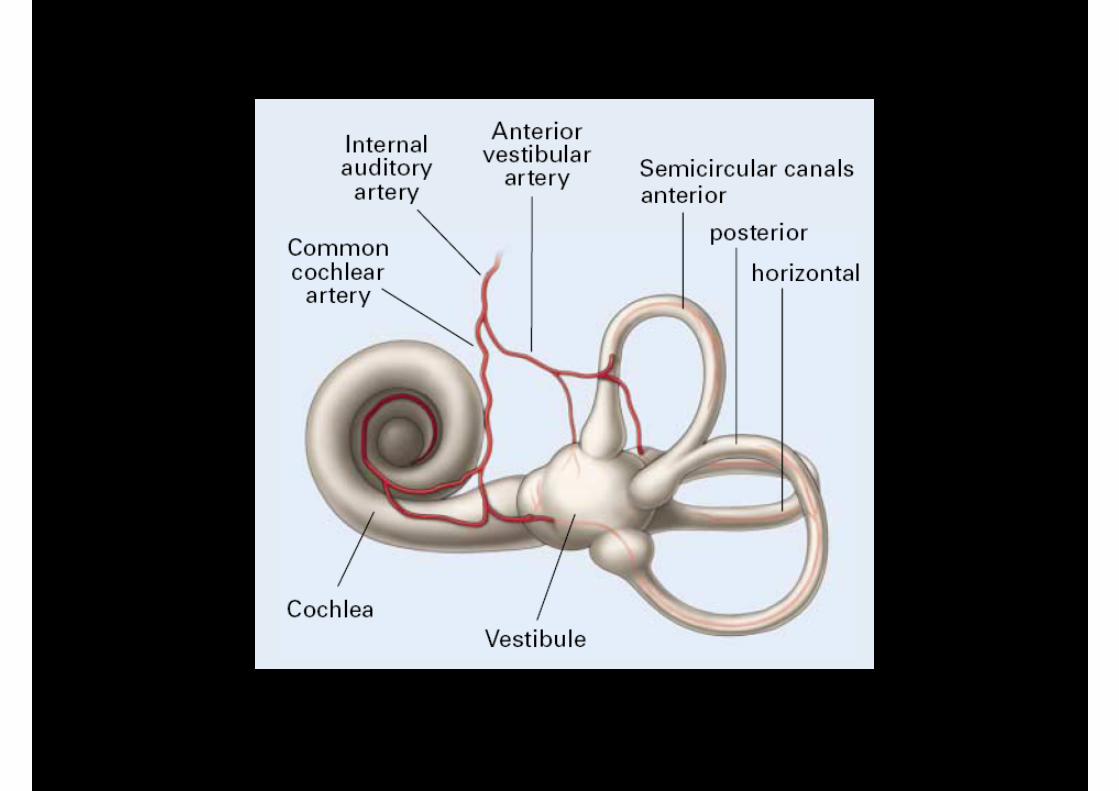
Vascular cause of vertigo
Location of lesion• Paramedian infratentorial
lesion • Thalamus • Vertibular cortex
Vascular territory• Vertebrobasilar system • Middle cerebral artery