do primary cutaneous non-t non-b cd4+cd56+ lymphomas belong to the myelo-monocytic lineage?
TRANSCRIPT

1242 LETTERS TO THE EDITOR THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
was found: the analysis of the distribution of allelic frequencies betweenporphyric and control subjects gave a p 5 0.007 by two-tailed Fisher’sexact test, whereas the number of mutated subjects gave a p 5 0.012.No significant differences were observed between the type I and IIPCT subgroups for both mutations (p . 0.6). No differences werealso observed between serum iron, ferritin, transferrin, and porphyrinlevels or for urinary porphyrin concentrations between mutated andnonmutated (single or both mutations) PCT patients (p at least . 0.21,data not shown). This finding suggests no apparent dependence ofHFE variants on iron metabolism of PCT subjects or on PCT intensity.Finally, HCV positivity was not significantly associated with the samemutations (Cys282Tyr mutation was found in three of seven HCV1patients, as opposed to eight of 13 for His63Asp, p 5 0.64).
In conclusion, the group of PCT patients studied presented only astatistically significant association with a HFE Cys282Tyr mutation.This result cannot support the fact that the HFE Cys282Tyr variantmay be widely involved in PCT pathogenesis, even if a possible roleof this altered molecule as a PCT trigger cannot be excluded in apatients’ subset.
Mauro D’Amato, Annelisa Macri9,* Daniela Griso,*Gianfranco Biolcati,* Franco Ameglio†
Department of Immunobiology, Institute of Cell Biology CNR-,Rome, Italy
*Laboratory of Biochemistry and Porphyria Center and †Laboratoryof Clinical Pathology, Institute S. Gallicano, IRCCS, Rome, Italy
REFERENCES
Beckman LE, Saha N, Spitsyn V, Van Landeghem G, Beckman L: Ethnic differences inthe HFE codon 282 (Cys/Tyr) polymorphism. Hum Hered 47:263–267, 1997
Do Primary Cutaneous Non-T Non-B CD4FCD56F
Lymphomas Belong to the Myelo-Monocytic Lineage?
To the Editor:
Primary cutaneous non-T non-B CD41CD561 tumors are extremelyrare and peculiar neoplasms of unknown origin and of poor prognosis(Petrella et al, 1999). They initially present as cutaneous nodules ortumors with histologic features of pleomorphic medium T celllymphoma, but express a distinguishing phenotype. Indeed, tumor cellsexpress CD4, CD56, and also CD45, CD43, and HLA-DR. All otherT cell and B cell markers are negative, and cells lack T and B cellgene rearrangements. The myelomonocytic markers (CD13, CD14,CD15, CD33, CD117, and lysozyme) are negative except for CD68,which was clearly positive in four cases and weakly expressed in twoof the seven cases of Petrella (Petrella et al, 1999). These tumors cannotbe classified into T, natural killer, or myeloid malignancies as definedin the present classifications, such as the Revised European andAmerican Lymphoma (REAL) (Harris et al, 1994) or the EORTCcutaneous lymphoma classification (Willemze et al, 1997). This malig-nant disorder has initially a clear skin tropism, but secondary extra-cutaneous relapse, mainly occurring in bone marrow, is associated witha very bad prognosis. The CD56 antigen is an isoform of the humanneuroneal cell adhesion molecule (N-CAM) that is expressed bycytotoxic cells and natural killer cells (Griffin et al, 1983; Hercend et al,1985). It has therefore been proposed that these tumors are derivedfrom natural killer cells (Bastian et al, 1998).
Manuscript received July 27, 1998; revised September 14, 1998; acceptedfor publication September 18, 1998.
Reprint requests to: Dr. Martine Bagot, Department of Dermatology andInserm U448, Hopital Henri Mondor, 94010 Creteil, France.
Bonkovsky HL, Poh-Fitzpatrick M, Obando J, et al: Porphyria cutanea tarda, hepatitis C,and HFE gene mutations in North America. Hepatol 27:1661–1669, 1998
D’Alessandro L, Griso D, Biolcati G, Macri9 A, Topi G: Incidence of hereditary porphyriacutanea tarda (PCT) in a sample of italian population. Arch Dermatol Res 284:212–214, 1992
D’Alessandro L, Ameglio F, Biolcati G, et al: Anti-HCV-core specific IgM in porphyriacutanea tarda. J Eur Acad Dermatol Venereol 6:226–231, 1996
Edwards CQ, Griffen LM, Goldgar DE, Skolnick MH, Kushner JP: HLA-linkedhemochromatosis alleles in sporadic porphyria cutanea tarda. Gastroenterology 97:972–981, 1989
Halliday JW: Hemochromatosis and iron need. Nutr Rev 56:S30–S37, 1998Kappas A, Sassa S, Galbraith RA, Nordmann Y: The porphyrias. In: Scriver CR, Beaudet
AL, Sly WS, Valle D (eds). The Molecular and Metabolic Basis of Inherited Disease, 7thedn. New York: McGraw Hill, 1995, pp. 2103–2159
Lebron JA, Bennett MJ, Vaughn DE, et al: Crystal structure of the hemochromatosisprotein HFE and characterization of its interaction with transferrin receptor. Cell93:111–123, 1998
McClatchey KD: Clinical Laboratory Medicine. Roma: Verduci, 1996Piperno A, Sampietro M, Pietrangelo A, et al: Heterogeneity of hemochromatosis in Italy.
Gastroenterology 114:996–1002, 1998Roberts AG, Whatley SD, Morgan RR, Worwood M, Elder GH: Increased frequency of
the hemochromatosis Cys282Tyr mutation in sporadic porphyria cutanea tarda.Lancet 349:321–323, 1997
Sampietro M, Piperno A, Lupica L, et al: High prevalence of the His63Asp HFE mutationin italian patients with porphyria cutanea tarda. Hepatol 27:181–184, 1998
Santos M, Clevers HC, Marx JJM: Mutations of the hereditary hemochromatosis candidategene HLA-H in porphyria cutanea tarda. N Engl J Med 336:1327–1328, 1997
Stuart KA, Busfield F, Jazwinska EC, et al: The C282Y mutation in the hemochromatosisgene (HFE) and hepatitis C virus infection are independent cofactors for porphyriacutanea tarda in australian patients. J Hepatol 28:404–409, 1998
Topi GC, D’Alessandro Gandolfo L, Griso D, Macri9 A, Biolcati GF: The follow-up ofporphyrics: the experience of a Centre for porphyrias. Sem Dermatol 2:198–205, 1986
Waheed A, Parkkila S, Zhou XY, et al: Hereditary hemochromatosis: effect of C282Y andH63D mutations on association with beta-2-microglobulin, intracellular processing,and cell surface expression of the HFE protein in COS-7 cells. Proc Natl Acad SciUSA 94:12384–12389, 1997
Killer-cell inhibitory receptors (KIR) are new major histocompati-bility complex (MHC) class I-specific receptors that have recently beenreported on natural killer cells (Moretta et al, 1994). The well-knownsusceptibility of some cell lines to the so-called natural killer-lysis is infact related to the absence of MHC class I expression by these celllines (Ljunggren and Karre, 1990). There are several natural killerreceptors, discriminating among different allelic groups of MHC classI molecules (Moretta et al, 1997). In humans, MHC-class I-specificinhibitory receptors belong to two distinct molecular families thatdisplay a different specialization. The immunoglobulin superfamilyencompasses several members characterized by several extra-cellularimmunoglobulin-like domains, which specifically recognize groups ofHLA-C (p58.1/CD158a and p58.2/CD158b) (Moretta et al, 1990,1993, 1995; Wagtmann et al, 1995) and HLA-B (p70/NKB1) (Litwinet al, 1993; Lanier et al, 1995; Vitale et al, 1996) alleles. The secondfamily comprises type II membrane molecules that belong to theC-type lectin superfamily. These receptors comprise CD94 covalentlyassociated with NKG2A molecules, which are expressed by the majorityof natural killer cells, and display a specificity toward self-MHCpeptides presented by HLA-E (Lee et al, 1998). Recently, KIR havealso been shown to be expressed on a subset of activated T cells(mainly CD81) in which they can inhibit T cell receptor mediatedfunctions (Mingari et al, 1997).
In this study, we studied skin- and blood-derived tumor cells of a67 y old woman initially presenting with disseminated erythematousnodules. A diagnosis of non-T non-B CD41CD561 lymphoma wasperformed on histologic and immunohistochemical analysis of skinlesions. No rearrangement of T cell receptor or immunoglobulin geneswas detected by polymerase chain reaction analysis. A completestaging was negative. The patient was treated by six courses of
VOL. 111, NO. 6 DECEMBER 1998 LETTERS TO THE EDITOR 1243
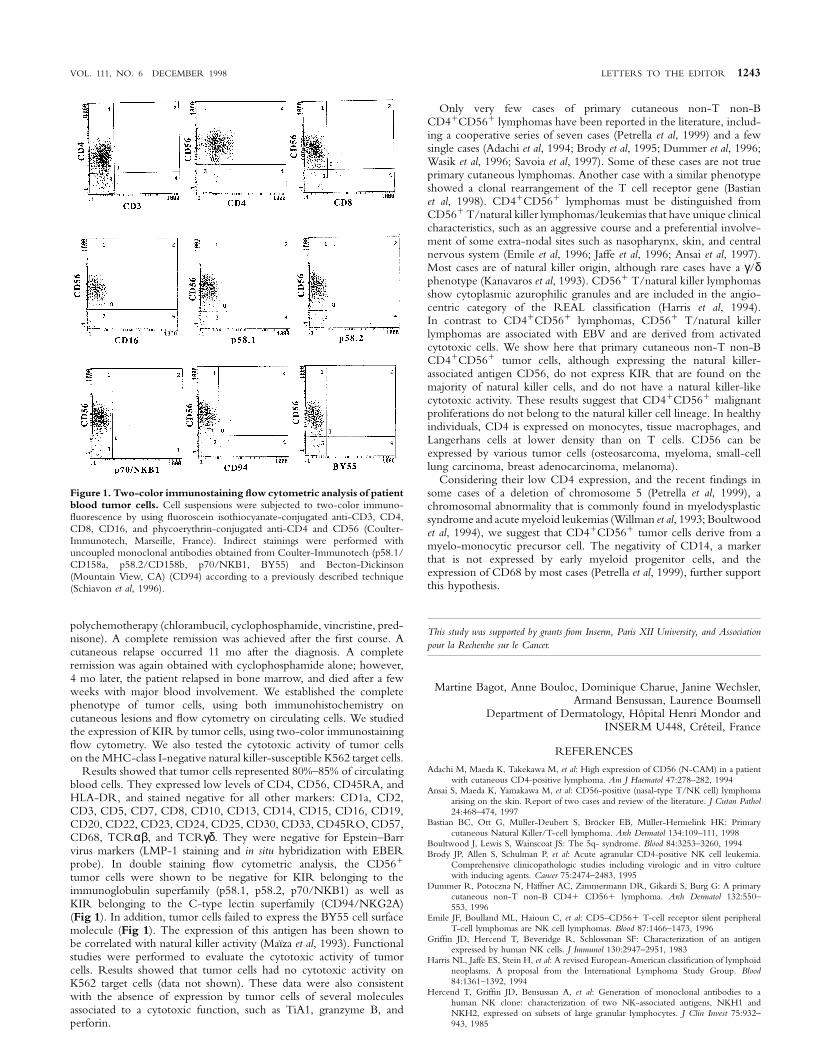
Figure 1. Two-color immunostaining flow cytometric analysis of patientblood tumor cells. Cell suspensions were subjected to two-color immuno-fluorescence by using fluoroscein isothiocyanate-conjugated anti-CD3, CD4,CD8, CD16, and phycoerythrin-conjugated anti-CD4 and CD56 (Coulter-Immunotech, Marseille, France). Indirect stainings were performed withuncoupled monoclonal antibodies obtained from Coulter-Immunotech (p58.1/CD158a, p58.2/CD158b, p70/NKB1, BY55) and Becton-Dickinson(Mountain View, CA) (CD94) according to a previously described technique(Schiavon et al, 1996).
polychemotherapy (chlorambucil, cyclophosphamide, vincristine, pred-nisone). A complete remission was achieved after the first course. Acutaneous relapse occurred 11 mo after the diagnosis. A completeremission was again obtained with cyclophosphamide alone; however,4 mo later, the patient relapsed in bone marrow, and died after a fewweeks with major blood involvement. We established the completephenotype of tumor cells, using both immunohistochemistry oncutaneous lesions and flow cytometry on circulating cells. We studiedthe expression of KIR by tumor cells, using two-color immunostainingflow cytometry. We also tested the cytotoxic activity of tumor cellson the MHC-class I-negative natural killer-susceptible K562 target cells.
Results showed that tumor cells represented 80%–85% of circulatingblood cells. They expressed low levels of CD4, CD56, CD45RA, andHLA-DR, and stained negative for all other markers: CD1a, CD2,CD3, CD5, CD7, CD8, CD10, CD13, CD14, CD15, CD16, CD19,CD20, CD22, CD23, CD24, CD25, CD30, CD33, CD45RO, CD57,CD68, TCRαβ, and TCRγδ. They were negative for Epstein–Barrvirus markers (LMP-1 staining and in situ hybridization with EBERprobe). In double staining flow cytometric analysis, the CD561
tumor cells were shown to be negative for KIR belonging to theimmunoglobulin superfamily (p58.1, p58.2, p70/NKB1) as well asKIR belonging to the C-type lectin superfamily (CD94/NKG2A)(Fig 1). In addition, tumor cells failed to express the BY55 cell surfacemolecule (Fig 1). The expression of this antigen has been shown tobe correlated with natural killer activity (Maıza et al, 1993). Functionalstudies were performed to evaluate the cytotoxic activity of tumorcells. Results showed that tumor cells had no cytotoxic activity onK562 target cells (data not shown). These data were also consistentwith the absence of expression by tumor cells of several moleculesassociated to a cytotoxic function, such as TiA1, granzyme B, andperforin.
Only very few cases of primary cutaneous non-T non-BCD41CD561 lymphomas have been reported in the literature, includ-ing a cooperative series of seven cases (Petrella et al, 1999) and a fewsingle cases (Adachi et al, 1994; Brody et al, 1995; Dummer et al, 1996;Wasik et al, 1996; Savoia et al, 1997). Some of these cases are not trueprimary cutaneous lymphomas. Another case with a similar phenotypeshowed a clonal rearrangement of the T cell receptor gene (Bastianet al, 1998). CD41CD561 lymphomas must be distinguished fromCD561 T/natural killer lymphomas/leukemias that have unique clinicalcharacteristics, such as an aggressive course and a preferential involve-ment of some extra-nodal sites such as nasopharynx, skin, and centralnervous system (Emile et al, 1996; Jaffe et al, 1996; Ansai et al, 1997).Most cases are of natural killer origin, although rare cases have a γ/δphenotype (Kanavaros et al, 1993). CD561 T/natural killer lymphomasshow cytoplasmic azurophilic granules and are included in the angio-centric category of the REAL classification (Harris et al, 1994).In contrast to CD41CD561 lymphomas, CD561 T/natural killerlymphomas are associated with EBV and are derived from activatedcytotoxic cells. We show here that primary cutaneous non-T non-BCD41CD561 tumor cells, although expressing the natural killer-associated antigen CD56, do not express KIR that are found on themajority of natural killer cells, and do not have a natural killer-likecytotoxic activity. These results suggest that CD41CD561 malignantproliferations do not belong to the natural killer cell lineage. In healthyindividuals, CD4 is expressed on monocytes, tissue macrophages, andLangerhans cells at lower density than on T cells. CD56 can beexpressed by various tumor cells (osteosarcoma, myeloma, small-celllung carcinoma, breast adenocarcinoma, melanoma).
Considering their low CD4 expression, and the recent findings insome cases of a deletion of chromosome 5 (Petrella et al, 1999), achromosomal abnormality that is commonly found in myelodysplasticsyndrome and acute myeloid leukemias (Willman et al, 1993; Boultwoodet al, 1994), we suggest that CD41CD561 tumor cells derive from amyelo-monocytic precursor cell. The negativity of CD14, a markerthat is not expressed by early myeloid progenitor cells, and theexpression of CD68 by most cases (Petrella et al, 1999), further supportthis hypothesis.
This study was supported by grants from Inserm, Paris XII University, and Associationpour la Recherche sur le Cancer.
Martine Bagot, Anne Bouloc, Dominique Charue, Janine Wechsler,Armand Bensussan, Laurence Boumsell
Department of Dermatology, Hopital Henri Mondor andINSERM U448, Creteil, France
REFERENCES
Adachi M, Maeda K, Takekawa M, et al: High expression of CD56 (N-CAM) in a patientwith cutaneous CD4-positive lymphoma. Am J Haematol 47:278–282, 1994
Ansai S, Maeda K, Yamakawa M, et al: CD56-positive (nasal-type T/NK cell) lymphomaarising on the skin. Report of two cases and review of the literature. J Cutan Pathol24:468–474, 1997
Bastian BC, Ott G, Muller-Deubert S, Brocker EB, Muller-Hermelink HK: Primarycutaneous Natural Killer/T-cell lymphoma. Arch Dermatol 134:109–111, 1998
Boultwood J, Lewis S, Wainscoat JS: The 5q- syndrome. Blood 84:3253–3260, 1994Brody JP, Allen S, Schulman P, et al: Acute agranular CD4-positive NK cell leukemia.
Comprehensive clinicopathologic studies including virologic and in vitro culturewith inducing agents. Cancer 75:2474–2483, 1995
Dummer R, Potoczna N, Haffner AC, Zimmermann DR, Gikardi S, Burg G: A primarycutaneous non-T non-B CD41 CD561 lymphoma. Arch Dermatol 132:550–553, 1996
Emile JF, Boulland ML, Haioun C, et al: CD5–CD561 T-cell receptor silent peripheralT-cell lymphomas are NK cell lymphomas. Blood 87:1466–1473, 1996
Griffin JD, Hercend T, Beveridge R, Schlossman SF: Characterization of an antigenexpressed by human NK cells. J Immunol 130:2947–2951, 1983
Harris NL, Jaffe ES, Stein H, et al: A revised European-American classification of lymphoidneoplasms. A proposal from the International Lymphoma Study Group. Blood84:1361–1392, 1994
Hercend T, Griffin JD, Bensussan A, et al: Generation of monoclonal antibodies to ahuman NK clone: characterization of two NK-associated antigens, NKH1 andNKH2, expressed on subsets of large granular lymphocytes. J Clin Invest 75:932–943, 1985

1244 LETTERS TO THE EDITOR THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
Jaffe E, Chan JKC, Su IJS, et al: Report of the workshop on nasal and related extranodalangiocentric T/Natural Killer cell lymphomas. Definitions, differential diagnosis,and epidemiology. Am J Surg Pathol 20:103–111, 1996
Kanavaros P, Lescs MC, Briere J, et al: Nasal T-cell lymphoma. A clinicopathologic entityassociated with peculiar phenotype and with Epstein-Barr virus. Blood 81:2688–2695, 1993
Lanier LL, Gumperz JE, Parham P, Melero I, Lopez-Botet M, Phillips JH: The NKB1,HP-3E, 4NK cell receptors are structurally distinct glycoproteins and independentlyrecognize polymorphic HLA-B and HLA-C molecules. J Immunol 154:3320–3327, 1995
Lee N, Llano M, Carretero M, Ishitani A, Navarro F, Lopez-Botet M, Geraghty DE:HLA-E is a major ligand for the NK inhibitory receptor CD94/NKG2A. Proc NatlAcad Sci USA 95:4791–4794, 1998
Litwin V, Gumperz J, Parham P, Phillips JH, Lanier LL: Specificity of HLA class I antigenrecognition by human NK clones: evidence for clonal heterogeneity, protection byself and non-self alleles, and influence of the target cell type. J Exp Med 178:1321–1336, 1993
Ljunggren HG, Karre K: In search of the ‘‘missing self’’. MHC molecules and NK cellrecognition. Immunol Today 11:237–244, 1990
Maıza H, Leca G, Mansur IG, Schiavon V, Boumsell L, Bensussan A: A novel 80-kD cellsurface structure identifies human circulating lymphocytes with NK activity. J ExpMed 178:1121–1126, 1993
Mingari MC, Ponte M, Cantoni C, et al: HLA-class I specific inhibitory receptors inhuman cytolytic T lymphocytes: molecular characterization, distribution in lymphoidtissues and co-expression by individual T cells. Int Immunol 9:485–491, 1997
Moretta A, Moretta L: HLA class I specific inhibitory receptors. Curr Opin Immunol 9:694–701, 1997
Moretta A, Bottino C, Pende D, et al: Identification of four subsets of human CD3–CD161 NK cells by the expression of clonally distributed functional surface
Heterozygosity for Premature Termination Codon Mutations inLAMB3 in Siblings with Non-Lethal Junctional EpidermolysisBullosa
To the Editor:
Junctional epidermolysis bullosa (JEB; OMIM nos. 226650 and 226700)is clinically characterized by fragility of the skin and various extra-cutaneous epithelia (Fine et al, 1991; Pulkkinen et al, 1999). Diagnosticelectron microscopy and immunoepitope mapping of the JEB patients’skin have revealed that tissue separation occurs within the laminalucida, associated with abnormalities in hemidesmosomes, criticalattachment structures at the dermal–epidermal basement membranezone (Tidman and Eady, 1986; Verrando et al, 1991). Clinically, JEBhas been divided into the lethal, Herlitz variant (H-JEB), which resultsin early demise, and nonlethal forms characterized by protractedblistering without compromising the lifespan of the affected individuals.
Previously, a number of mutations in the three genes, LAMA3,LAMB3, and LAMC2, which encode the subunit polypeptides oflaminin 5, have been demonstrated in patients with JEB (Pulkkinenet al, 1999). The majority of these mutations reside in the LAMB3gene, which accounts for µ80% of all laminin 5 mutations. Thepredominance of LAMB3 mutations, in comparison with LAMA3 orLAMC2, can be explained, at least in part, by two recurrent ‘‘hotspot’’mutations, R635X and R42X (Kivirikko et al, 1996).
Examination of the laminin 5 mutation database in JEBhas revealed general rules for genotype/phenotype correlations.Specifically, the mutations resulting in premature termination codonfor translation (PTC) in both alleles have invariably been associatedwith H-JEB, whereas in nonlethal variants of JEB at least one or
Manuscript received July 20, 1998; revised July 23, 1998; accepted forpublication July 29, 1998.
Reprint requests to: Dr. Jouni Uitto, Department of Dermatology andCutaneous Biology, Jefferson Medical College, 233 S 10th Street, Suite 450,Bluemle Life Sciences Building, Philadelphia, PA 19107-5541.
molecules. Correlation between subset assignment of NK clones and ability tomediate specific alloantigen recognition. J Exp Med 172:1589–1598, 1990
Moretta A, Vitale M, Bottino C, et al: p58 molecules as putative receptors for MHC classI molecules in human Natural Killer (NK) cells. Anti-p58 antibodies reconstitutelysis of MHC class I-protected cells in NK clones displaying different specificities.J Exp Med 178:597–604, 1993
Moretta L, Ciccone E, Mingari MC, Biassoni R, Moretta A: Human NK receptors: origin,clonality, specificity and receptors. Adv Immunol 55:341–380, 1994
Moretta A, Sivori S, Vitale M, et al: Existence of both inhibitory (p58) and activatory(p50) receptors for HLA-C molecules in human Natural Killer cells. J Exp Med182:875–884, 1995
Petrella T, Dalac S, Maynadie M, et al: CD41CD561 cutaneous neoplasms. A distincthematological entity? Am J Surg Pathol 1999 in press
Savoia P, Fierro MT, Novelli M, Quaglino P, Verrone A, Geuna M, Bernengo MG: CD56-positive cutaneous lymphoma: a poorly recognized entity in the spectrum ofprimary cutaneous disease. Br J Dermatol 137:966–971, 1997
Schiavon V, Roth P, Bolton WE, Farcet JP, Bensussan A, Boumsell L: Lymphocytes subsetsin normal individuals: analysis by four color immunofluorescence and flow cytometryon whole blood. Tissue Antigens 48:312–318, 1996
Vitale M, Sivori S, Pende D, et al: Physical and functional independency of p70 and p58NK cell receptors for HLA class I. their role in the definition of different groups ofalloreactive NK cell clones. Proc Natl Acad Sci USA 93:1453–1457, 1996
Wagtmann N, Biassoni R, Cantoni C, et al: Molecular clones of the p58 NK cell receptorreveal immunoglobulin-related molecules with diversity in both the extra- and intra-cellular domains. Immunity 2:439–449, 1995
Wasik MA, Sackstein R, Novick D, et al: Cutaneous CD561 large T-cell lymphomaassociated with high serum concentration of IL-2. Hum Pathol 27:738–744, 1996
Willman CL, Sever CE, Pallavicini MG, et al: Deletion of IRF-1, mapping to chromosome5q31.1, in human leukemia and preleukemic myelodysplasia. Science 259:968–971, 1993
both alleles have a missense or an in-frame exon skip mutation(Pulkkinen et al, 1999). Thus far, there have been no exceptionsto this general rule. In this study, we report a proband withnonlethal JEB in her late twenties. Mutation detection analysesrevealed LAMB3 mutations in both alleles, but surprisingly, thepatient was a compound heterozygote for PTC.
The proband of this Family (born July 18, 1968) was noted at birthto have blisters and erosions, associated with subsequent developmentof milia and nail abnormalities. At the age of 27 y, she had widespreadblistering on the torso and extremities. There was no blistering in themouth, and her hair was normal without evidence of scarring alopecia.The patient has history of corneal erosions and scarring, mitral valveprolapse, and Wolffe-Parkinson-White disease. At the age of 16 y,severe dental caries due to extensive enamel hypoplasia necessitatedfull dentures. The proband had a younger brother with very similarclinical presentation, whereas a younger sister and the parents wereclinically unaffected. Histopathology revealed noninflammatorydermal–epidermal separation, and immunohistochemistry with a poly-clonal rabbit anti-laminin antibody (Life Technologies, Gaithersburg,MD) raised against pepsinized human laminin suggested lower laminalucida separation. Transmission electron microscopy revealed subepider-mal cleft with intact basal keratinocytes. In some areas, occasionalhemidesmosomes were noted, whereas in other areas they were absent.Anchoring fibrils were present in abundance and were attached to thelamina densa in the floor of the blister. These findings are diagnosticfor JEB.
DNA obtained from the proband and her immediate familymembers (Fig 1A) was screened for the recurrent R635X mutationby polymerase chain reaction (PCR) amplification of exon 14 ofLAMB3, followed by BglII restriction enzyme digestion (Kivirikkoet al, 1996). This revealed the presence of R635X in one allele ofthe proband as well as in the proband’s clinically affected youngerbrother, in the clinically normal mother, and in the younger sister(Fig 1A). Subsequent scanning of the remaining LAMB3 exons