do you need to be afraid of pacemakers &...
TRANSCRIPT

West Herts Cardiology
Do you need to be afraid of Pacemakers & ICDs?
East Midland Conference Centre, Nottingham
10th November 2011
Dr John Bayliss
Consultant Cardiologist, West Hertfordshire NHS Trust
Arrhythmia lead, Beds & Herts Heart & Stroke Network

West Herts Cardiology
Devices intro
Pacemaker types
Brady
CRT
ICD
Unipolar v Bipolar
Effects of Diathermy
How to avoid problems
Be safe, not sorry: Knowledge + Confidence
Do you need to be afraid of Pacemakers & ICDs?
West Herts Cardiology
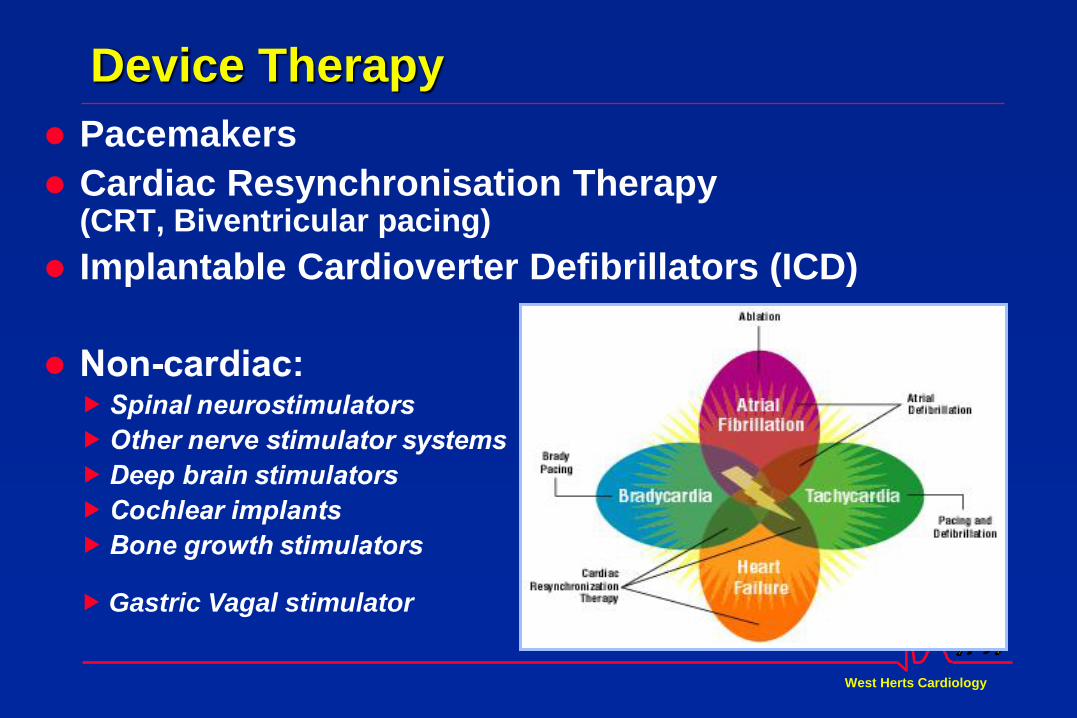
Device Therapy
Pacemakers
Cardiac Resynchronisation Therapy (CRT, Biventricular pacing)
Implantable Cardioverter Defibrillators (ICD)
Gastric Vagal stimulator
West Herts Cardiology
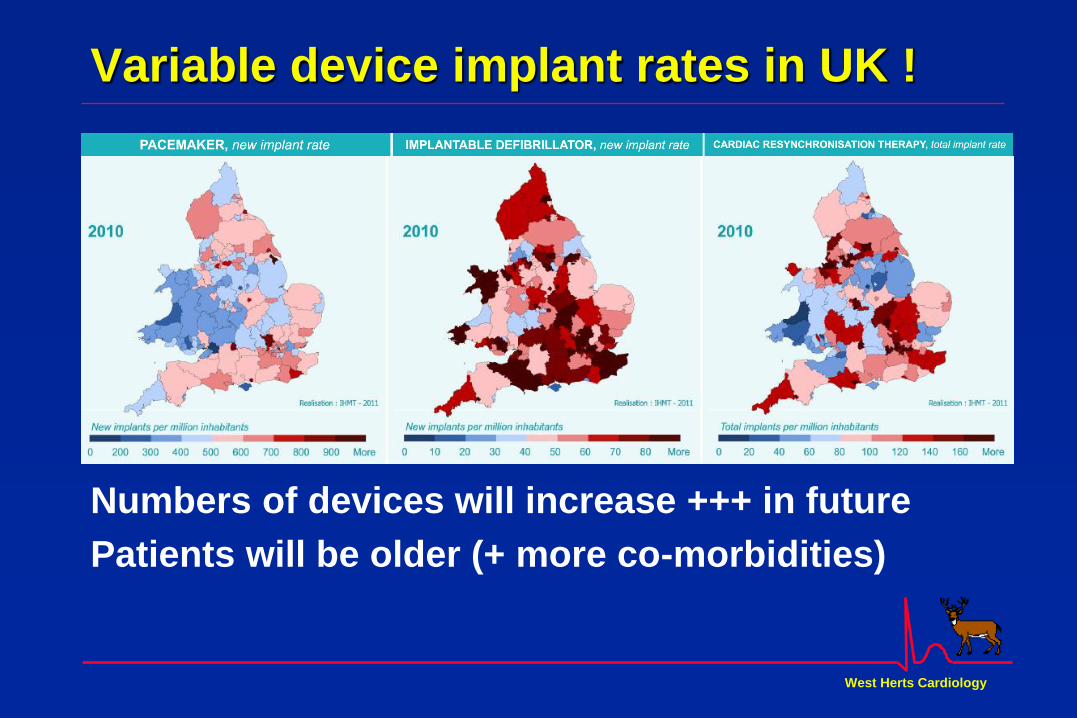
Variable device implant rates in UK !
Numbers of devices will increase +++ in future
Patients will be older (+ more co-morbidities)

West Herts Cardiology
Conduction system : Indications for devices
Brady Pacing
Sick Sinus
syndrome
Atrio-
Ventricular
Block
+
Conduction
disease
ICD
VT / VF
CRT
CHF
+LBBB
West Herts Cardiology
Indications for device therapy
1. Pacing for Bradycardias
AV Block: 3° or 2 ° (even if asymptomatic)
Sinus Node Disease (“Sick Sinus Syndrome”)
AVB + SND
AVB + AF (“Slow AF”)
Vasovagal Syndromes (cardioinhibitory = asystole)
2. Pacing in HCM to “desynchronise” LV septum
3. Pacing in CHF Biventricular pacing for Cardiac Resynchronisation Therapy (CRT) to “resynchronise” LV
4. Anti-tachy pacing → ICD
West Herts Cardiology
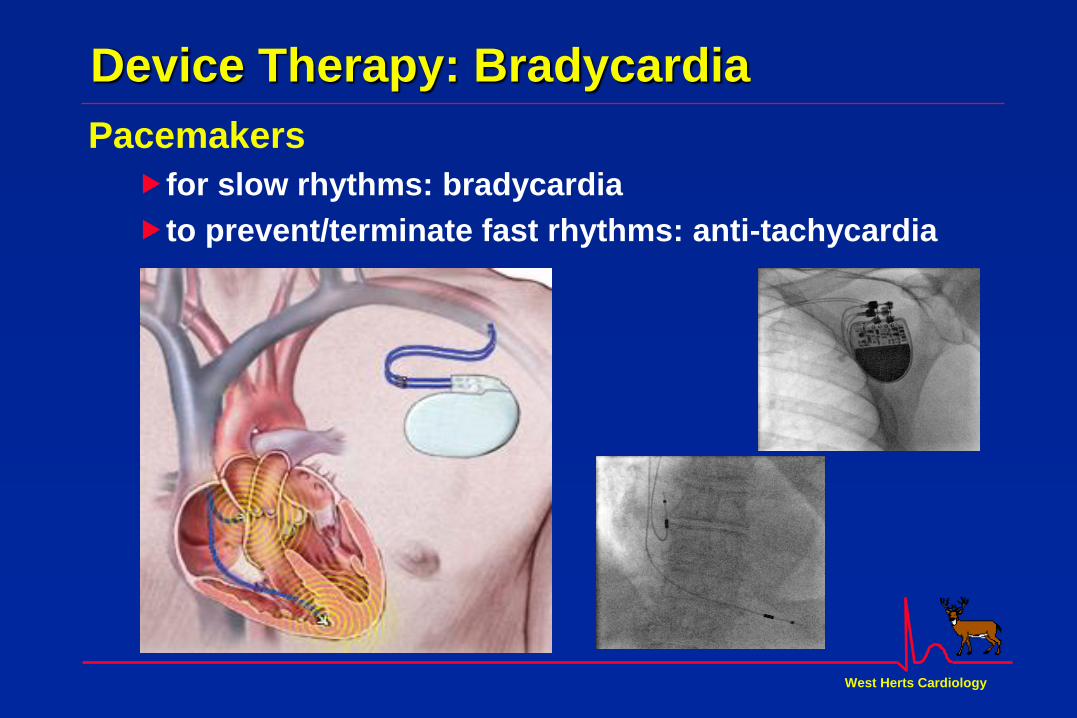
Device Therapy: Bradycardia
Pacemakers
for slow rhythms: bradycardia
to prevent/terminate fast rhythms: anti-tachycardia

West Herts Cardiology
Permanent Pacing Codes
Paced Chamber Sensed Chamber Action if sensed
A Atrium A Atrium I Inhibit pacing
V Ventricle V Ventricle T Trigger pacing
D Dual (A+V) D Dual (A+V) D Dual (I+T)
O None O None
-R Rate responsive = pacing rate ↑ with exercise VOO Ventricular pacing (asynchronous) = Fixed rate VVI Ventricular “demand” pacing VVI-R Ventricular “demand” pacing, rate responsive DDD Dual chamber, AV sequential, “physiological” DDD-R Dual chamber pacing, rate responsive
West Herts Cardiology
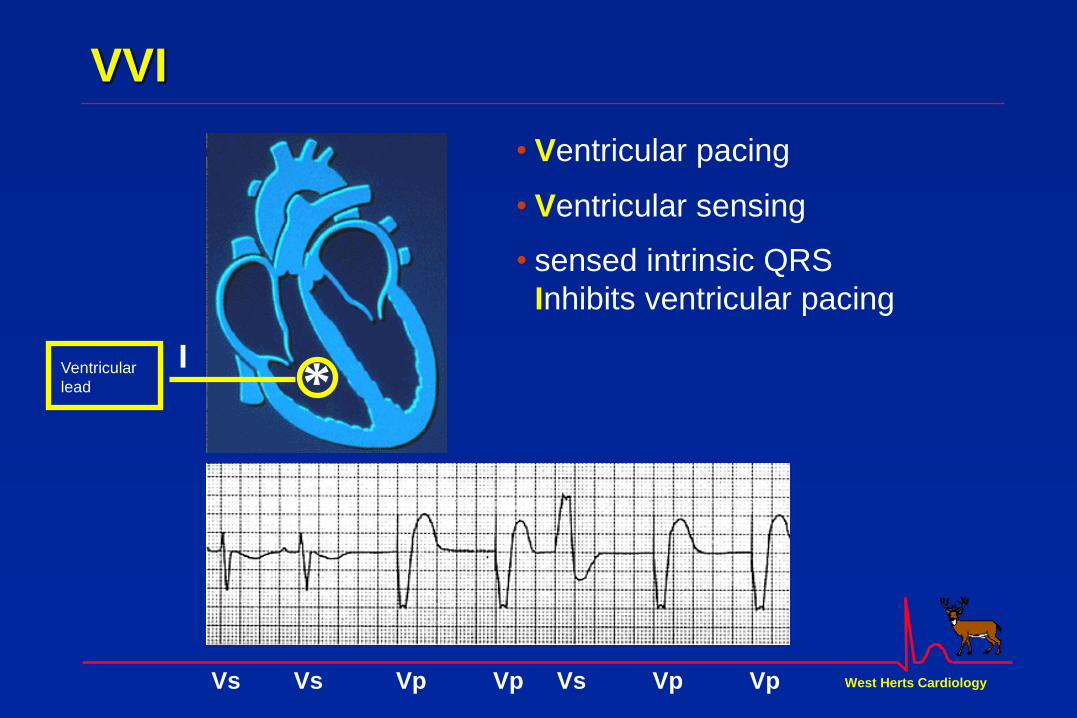
I *
Ventricular
lead
• sensed intrinsic QRS
Inhibits ventricular pacing
• Ventricular pacing
• Ventricular sensing
VVI
Vs Vs Vp Vp Vs Vp Vp

West Herts Cardiology
T / I
*
* Atrial
lead
Ventricular
Lead
• Pacing in both the atrium
and ventricle (Dual)
• Sensing in both the atrium
and ventricle (Dual)
• i • intrinsic P wave or intrinsic
QRS can Inhibit pacing
• Intrinsic P Wave can
“Trigger” a paced QRS
I
DDD
Dual
AsVs ApVs ApVp ApVp AsVp AsVp

West Herts Cardiology
Device Therapy: CRT
Cardiac Resynchronisation Therapy
in Heart Failure with LBBB (usually in SR)
(CRT, “Biventricular pacing”)
Leads to RA+RV+LV (CRT-P) : 3 leads
may include ICD capability (CRT-D) : ?thicker ICD lead
RA
RV
LV

West Herts Cardiology
Device Therapy: CRT
Cardiac Resynchronisation Therapy

West Herts Cardiology
Device Therapy: ICD
Implantable Cardioverter Defibrillator: ICD – 1 lead
Brady pacing
Anti-Tachy therapies
VT: anti-tachy pacing
VF: DC Shock(s)
Note thicker shock coil lead
compared to simple pacing lead

West Herts Cardiology
Device Therapy: ICD
Implantable Cardioverter Defibrillator: CRT-D
Brady pacing
Anti-Tachy therapies
VT: anti-tachy pacing
VF: DC Shock(s)
Note thicker shock coil lead
compared to simple pacing lead

West Herts Cardiology
ICD function
VT termination by ramp pacing
VT sense
Tachy pace →SR

West Herts Cardiology
ICD function
VT terminated by single shock
VT sense
Charge→Shock→SR

West Herts Cardiology
ICD function
VF terminated by single 34J shock
VF sense
Charge→Shock →SR

West Herts Cardiology
Pacing ± ICD Systems: Summary
Single Dual Biventricular
chamber chamber
1 lead 2 leads 3 leads
Usually RV RA+RV RA+RV+LV
(might be RA)
West Herts Cardiology
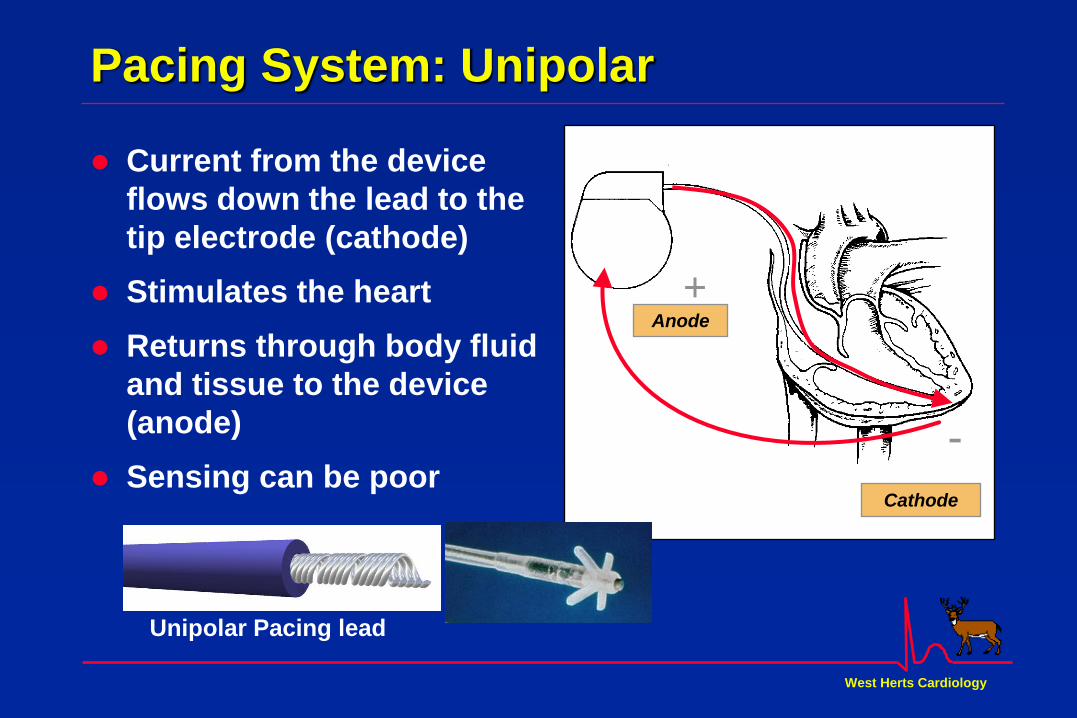
Current from the device
flows down the lead to the
tip electrode (cathode)
Stimulates the heart
Returns through body fluid
and tissue to the device
(anode)
Sensing can be poor
Cathode
Anode
-
+
Unipolar Pacing lead
Pacing System: Unipolar

West Herts Cardiology
Pacing System: Bipolar
Current from the device
flows down the lead to the
tip electrode (cathode)
Stimulates the heart
Returns to the device via
the ring electrode (anode)
above the lead tip and
back up the lead
Coaxial Bipolar Pacing lead
Anode
Cathode

West Herts Cardiology
Diathermy System
Monopolar
Wide spread of
electrical “noise”
towards plate
Bipolar
Small area of electrical
“noise” between
forceps

West Herts Cardiology
Effects of diathermy on Cardiac Devices
Effect of sensing the diathermy current
Effect of current / energy transmitted via lead(s)
Effect of current / energy on device

West Herts Cardiology
Effects of diathermy on Cardiac Devices
Effect of sensing the diathermy current Inhibition of pacing
(= Asystole if pacemaker dependent)
Triggering heart rate increase
ICD interpreting as VT/VF → ICD function
(tachy pace or ICD Shock, may cause VF !)
Effect of current / energy transmitted via lead(s)
Effect of current / energy on device
West Herts Cardiology
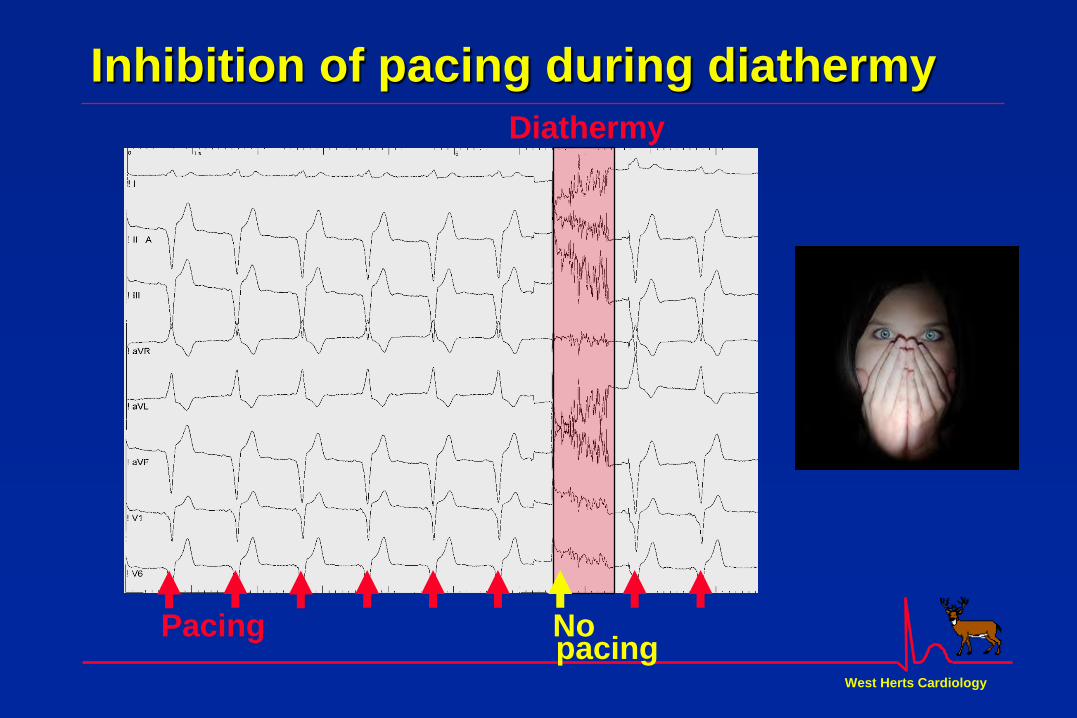
Inhibition of pacing during diathermy
Diathermy
Pacing No pacing
West Herts Cardiology
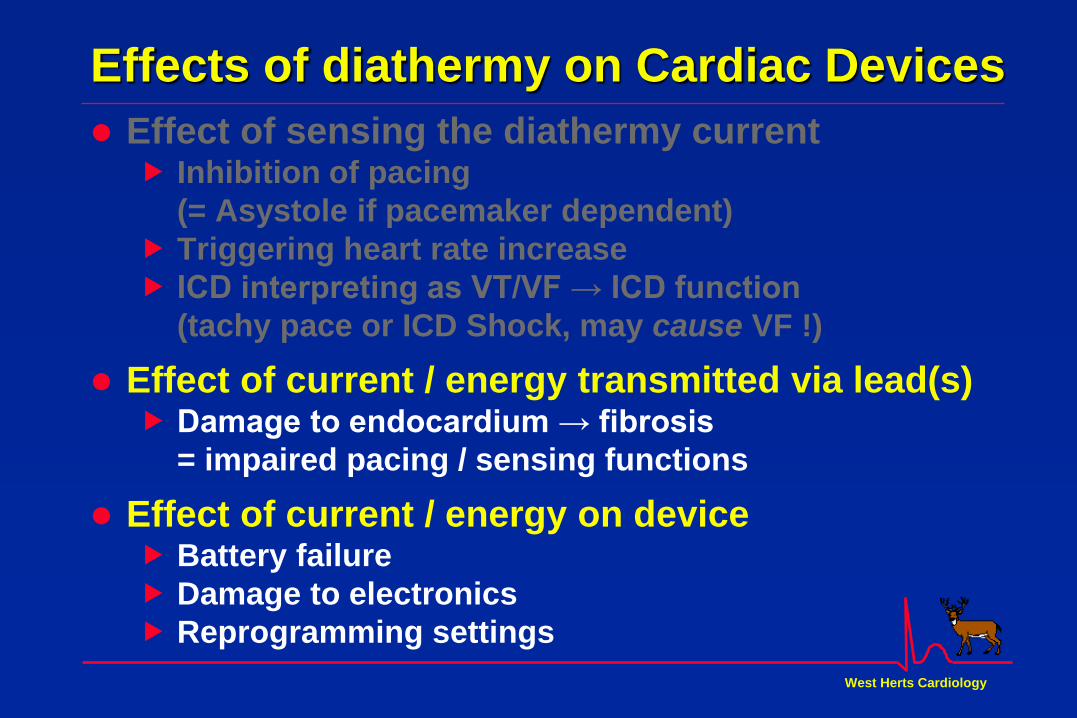
Effects of diathermy on Cardiac Devices
Effect of sensing the diathermy current Inhibition of pacing
(= Asystole if pacemaker dependent)
Triggering heart rate increase
ICD interpreting as VT/VF → ICD function
(tachy pace or ICD Shock, may cause VF !)
Effect of current / energy transmitted via lead(s) Damage to endocardium → fibrosis
= impaired pacing / sensing functions
Effect of current / energy on device Battery failure
Damage to electronics
Reprogramming settings

West Herts Cardiology
Worse if pacemaker dependent or battery nearly depleted
Diathermy may cause
Endocardial damage at pacing lead tip
= Elevated pacing capture threshold…
Sudden further loss of battery power
Intermittent failure to capture = Asystole
Pacing failure after diathermy
No pacing = asystole

West Herts Cardiology
Is a magnet over the pacemaker useful ?
To disable sensing, so pacemaker ignores electrical
“noise”, or any spontaneous beats
= makes pacemaker pace

West Herts Cardiology
“Magnet Mode” of pacemakers
Unpredictable
? Dangerous
DO NOT USE

West Herts Cardiology
Inappropriate effect of Magnet mode
Magnet mode causing fixed rate asynchronous pacing
Intrinsic beat in vulnerable period → VF
Salukhe T V et al. Br. J. Anaesth. 2004;93:95-104
West Herts Cardiology

West Herts Cardiology
Risk of not treating Risk of treating
Benefit of not treating Benefit of treating
Risks v Benefits


West Herts Cardiology
MHRA guidelines - 2006
Caution
Using surgical diathermy / electrocautery on patients with an
implantable pacemaker or implantable cardioverter defibrillator
(ICD) can present additional risk of electrical interference and
appropriate precautions need to be considered.
Manufacturers either contraindicate or give strong warnings
against its use, particularly the monopolar mode.
Where the risk/benefit analysis favours the use of surgical
diathermy/electrocautery - particularly in emergency situations,
the use of bipolar operating mode should first be considered.
However, it should be noted that interference remains a
possibility with bipolar mode.
West Herts Cardiology
MHRA guidelines - 2006
Notes
Interference generated by monopolar surgical diathermy
(electrocautery) is more severe than bipolar and can be sufficient
to temporarily inhibit pacemaker output, give rise to a temporary
increase in pacing, or cause a loss of programmed settings.
For ICDs there is a possibility that noise/interference may be
misinterpreted as ventricular tachycardia or ventricular fibrillation
causing inappropriate initiation of therapy.
Where the implant’s internal power source is low, device
operation may be uncertain during or after the application of
monopolar surgical diathermy/electrocautery.

West Herts Cardiology
Guidance for peri-op management of devices
All patients
All practitioners who assess a patient who may need
diathermy, shortwave, microwave or ultrasound diathermy
should ask the patient (and if necessary their relatives)
about possible device implants before planning to use such
techniques. (Note also that MRI is contraindicated in such patients).
Radiofrequency (short wave), microwave or ultrasound
diathermy therapy should NEVER be used in any patient
with a device / lead(s). (Note that Leads may remain implanted even after the device box is removed).
Diathermy / electrocautery should be avoided whenever
possible in all patients with a pacemaker or ICD.
1

West Herts Cardiology
Guidance for peri-op management of devices
All cases, including emergency cases - 1 Staff must hold ILS accreditation, and be prepared to resuscitate .
There must be an external defibrillator with external pacing capability
within the operating room.
The patient must be attached to an ECG monitor and to the external
pacing defibrillator during the procedure.
(beware ECG monitor “paced” mode misinterpreting asystole)
Do NOT place a ring magnet over the device hoping that this will
somehow avoid problems, unless advised to do so by a Cardiac
Physiologist/Cardiologist.
In the event that the patient becomes asystolic, has a ventricular
arrhythmia, or any pulseless electrical activity during a surgical
procedure, resuscitation and medical intervention should take place
without delay in the usual manner of managing a cardiac arrest –
irrespective of the patient’s device.
2

West Herts Cardiology
Guidance for peri-op management of devices
All cases, including emergency cases - 2 Electrocautery diathermy should NEVER be used near a pacemaker / ICD
If electrocautery diathermy must be used in any other area away from the
pacemaker/ICD:
Use Bipolar diathermy if possible (eg diathermy forceps)
If Monopolar diathermy is essential, apply the indifferent plate/pad to
leg opposite pacemaker/ICD to minimise generated electrical circuit
near device (eg if pacemaker/ICD is in upper left chest, then place pad on right thigh).
Use diathermy for short bursts, 1 second or less,
with ECG monitoring to observe the effect on the rhythm.
In a patient with a pacemaker, allow 3 second delay between each
1 second burst of diathermy to allow recovery from any asystole that
occurs during the diathermy.
In a patient with an ICD, allow 10 second delay between each
1 second burst of diathermy to reduce the possibility of triggering a
shock, and to dissipate energy conduction through the ICD lead.
3

West Herts Cardiology
Guidance for peri-op management of devices
All cases, including emergency cases - 3 If serious arrhythmia develops during diathermy,
treat the arrhythmia as usual, stop using diathermy, complete the
operation as safely as possible and contact a Device Physiologist.
A 12-lead ECG must be performed immediately after surgery.
If the heart rate is below 50bpm on the 12-lead ECG there may be a
problem with the device and a Device Physiologist should be contacted.
A pacemaker/ICD check should be performed post-operatively as an
inpatient prior to discharge.
4

West Herts Cardiology
Guidance for peri-op management of devices
Planned procedures - 1 Patients with implanted devices or leads (even if box has been removed),
can be identified at routine pre-admission screening.
When a patient is identified as having an implanted device this should be
recorded in the notes and the key clinical and surgical staff informed.
The Hospital responsible for device follow-up (may not be the hospital in
which surgery is planned…), device manufacturer and model number,
and reason for implant (e.g. heart block etc) should be recorded.
The Cardiology/Device team responsible for the patient should be
contacted for advice, following a local protocol.
If diathermy is essential, discuss with the Device team well in advance,
so arrangements can be made for them to review the patient to make any
adjustments that might be necessary to facilitate use of diathermy.
5

West Herts Cardiology
Guidance for peri-op management of devices
Planned procedures - 2 Each patient’s case should be risk assessed individually by the Device
team. At least 2 weeks’ notice between referral and operation date is
usually required to allow time for this.
The patient may not need to be seen in the Pacing Clinic,
if a pacemaker has been checked within the past 12 months,
or an ICD checked within 6 months.
It is important to determine and be aware :
If the patient is pacemaker dependent ?
= patient at risk of asystole if the device malfunctions.
If the device battery is near to depletion ?
= device may cease to function if affected by diathermy.
What the “magnet mode” is programmed to?
= What effect placing a magnet over the pacemaker may have.
What ICD settings are programmed to detect and treat VT/VF
6

West Herts Cardiology
Guidance for peri-op management of devices
Planned procedures - 3 If the patient has an ICD, the Device Physiologist will probably
program the device to a no-shock mode for the duration of the op.
The Physiologist will need to be available on the day of the operation to
turn the device therapies off pre-procedure and turn them back on
immediately post- procedure.
During the time the device shock mode is turned off, the surgical/theatre
team must be ready to provide immediate resuscitation.
Any Beta Blocker or anti-arrhythmic therapy should usually be continued
pre-, peri- and post operatively, and not withheld.
If the patient is at high cardiovascular risk and is due to have major
surgery, and is not on a Beta Blocker, consideration should be given to
planned initiation of the Beta Blocker pre-operatively, as this reduces
cardiovascular complications.
7