doc2 a review part1 -...
TRANSCRIPT

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
i
A Review of the TechnicalBasis for the Control ofConditions Associated withGroup A StreptococcalInfections
Department of Child and Adolescent Health and DevelopmentWorld Health Organization
DISCUSSION PAPERS ON CHILD HEALTHG
ROUP
A S
TREP
TOCO
CCAL
DIS
EASE
SC
AH
WHO/FCH/CAH/05.08

ii
GROUP A STREPTOCOCCUS
© World Health Organization 2005
All rights reserved. Publications of the World Health Organization can be obtained from Marketing andDissemination,World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476;fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce or translate WHOpublications – whether for sale or for noncommercial distribution – should be addressed to Publications, at theabove address (fax: +41 22 791 4806; email: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expression ofany opinion whatsoever on the part of the World Health Organization concerning the legal status of any country,territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lineson maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed orrecommended by the World Health Organization in preference to others of a similar nature that are not mentioned.Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
The World Health Organization does not warrant that the information contained in this publication is complete andcorrect and shall not be liable for any damages incurred as a result of its use.
The named authors alone are responsible for the views expressed in this publication.
Acknowledgements
WHO/CAH wishes to thank Prof. Jonathan R Carapetis, Centre for International Child Health, University of MelbourneDepartment of Paediatrics, Royal Children's Hospital, Melbourne, Australia for undertaking this review, and Dr.Andrew C Steer and Prof. E. Kim Mulholland, Royal Children's Hospital, Melbourne, Australia, for contributing to it.WHO/CAH is grateful to Drs. Alan Bisno, Singh Chhatwal, Hala Hamsa, Ed Kaplan, Fran Rubin, and Anne Schuchatfor reviewing the draft manuscript and providing valuable comments.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
iii
Table of ContentsExecutive summary ................................................................................................................................................. ivIntroduction .............................................................................................................................................................. 1Potential approaches to controlling GAS diseases ................................................................................................ 2
Primary prevention ............................................................................................................................................. 3Reducing overall exposure to GAS ............................................................................................................. 3Primary prophylaxis...................................................................................................................................... 3Primary prevention of skin infections ........................................................................................................... 4Antibiotic treatment to interrupt transmission of organisms ........................................................................ 4Immunisation ................................................................................................................................................ 4
Secondary prevention ....................................................................................................................................... 4Early and correct diagnosis of ARF. ............................................................................................................ 4Secondary prophylaxis. ............................................................................................................................... 4
Tertiary prevention ............................................................................................................................................. 4Management of RHD patients. ..................................................................................................................... 5Treatment and rehabilitation of invasive GAS infections. ............................................................................ 5
Evidence for certain control strategies ................................................................................................................... 6Primary prophylaxis ........................................................................................................................................... 6
Public health impact of treating GAS pharyngitis ........................................................................................ 7Primary prevention of skin infections ............................................................................................................... 10
The potential benefits of controlling skin infections ................................................................................... 14Antibiotic treatment to interrupt transmission of GAS ..................................................................................... 14Immunisation .................................................................................................................................................... 15Comprehensive streptococcal control programs ........................................................................................... 16Secondary prophylaxis and RHD control programs ....................................................................................... 16
Diagnosis of ARF ........................................................................................................................................ 19Medical and surgical management of RHD patients ...................................................................................... 20Cost-effectiveness of different prevention strategies ...................................................................................... 21
Conclusions ........................................................................................................................................................... 24Priority Issues ........................................................................................................................................................ 26Appendix 1: The possible link between GAS skin infections and acute rheumatic fever .................................. 27References ............................................................................................................................................................ 31

iv
GROUP A STREPTOCOCCUS
Executive summary
Group A streptococcus (GAS) causes a diverse spectrum of disease. In the past, most GAS control activitieshave fallen under the categories of register-based rheumatic heart disease (RHD) secondary prophylaxis programs,and management of acute rheumatic fever (ARF), RHD and sore throat / GAS pharyngitis. The prevention andcontrol of ARF/ RHD and streptococcal pharyngitis have also been the most researched topics in the literature.However, these activities do not encompass the entire range of potential strategies for controlling GAS diseases.
Of the available control strategies, secondary prophylaxis (defined as the delivery of regular doses of penicillin toARF/RHD patients to prevent recurrent ARF and worsening RHD) is the only one that has been shown to be botheffective and cost-effective at the community/population level. In populations with high prevalence of RHD, deliveryof secondary prophylaxis should be the major priority for control of GAS diseases. Coordinated register-basedRHD control programs appear to be the most effective method for delivering secondary prophylaxis and have theadded benefit of improving clinical follow-up of patients and providing a mechanism for delivery of targetedhealth promotional messages. Past efforts to expand RHD control programs have had mixed success. Futurestrategies should concentrate on ensuring that programs are properly resourced, not overly ambitious in theirearly stages, and are systematically evaluated. The issue of the availability and quality of BPG supplies requiresurgent attention. The diagnosis of ARF remains difficult in many countries, and the American Heart Association'sJones Criteria Working Group has called for more clinical research in this area. It is clear that this research shouldparticularly be focused in developing countries and other populations with high ARF incidence.
Tertiary prevention of RHD (the provision of medical and surgical treatment to patients with RHD and heart failure)is expensive and largely palliative. Moreover, it deals with the provision of care to patients with preventabledisease. Therefore, tertiary prevention of RHD should theoretically be the least important and therefore leastresourced aspect of GAS control. Unfortunately, in many countries this strategy has become the focus of RHDcontrol and consumes the majority of the RHD control budget (and a substantial proportion of the entire healthbudget). While the importance of treating patients in cardiac failure from RHD cannot be ignored, the cost-effectiveness of improving adherence to secondary prophylaxis - and thus reducing the number of RHD patientsrequiring surgical and medical treatment - clearly argues in favour of secondary rather than tertiary prevention.
There is currently no strategy for primary prevention of GAS diseases that has a proven cost-effective benefit atthe population level. Of the existing primary prevention interventions, primary prophylaxis of ARF (antibiotic treatmentof symptomatic GAS pharyngitis) has been the most intensively studied, advocated and practised. In particular,the use of simpler antibiotic treatment regimens (e.g. once-daily oral amoxicillin) and clinical algorithms for thediagnosis of GAS pharyngitis have received considerable attention in recent years. However, the available evidencesuggests that, even when implemented at an optimal level using school-based surveillance and treatment (programsthat are neither practical nor affordable for most less developed countries), primary prophylaxis can prevent onlya minority of cases of ARF. The efficacy of large-scale primary prophylaxis programs in reducing transmission ofGAS and incidence of GAS pharyngitis has been demonstrated, although this strategy is unlikely to be cost-effective. The impact of this approach on invasive GAS disease and acute post-streptococcal glomerulonephritis(APSGN) is not known. Although some middle-income countries may choose to implement surveillance-basedprimary prophylaxis programs on a large scale for the prevention of ARF, this strategy cannot be recommendedfor poorer countries, where the major burden of ARF exists.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
v
Community-based approaches for controlling scabies have had demonstrated success in reducing the prevalenceand severity of GAS skin infections. It is possible that mass administration of ivermectin for filariasis in manycountries may have had an important secondary benefit by reducing scabies and skin infections; this is notknown, but could be relatively easily determined. There is the potential for other strategies addressing personaland community hygiene (including swimming pools), insect bites, and targeted antibiotic treatment to be addedto scabies programs to further reduce rates of skin infections; this has not been properly studied. The control ofGAS skin infections and the likely effect of preventing APSGN and invasive disease is sufficient argument tosupport the widespread implementation of healthy skin programs in communities with high rates of scabies andpyoderma. The possibility that these programs may have the added benefits of preventing ARF and improvingother aspects of child health is further impetus for their implementation and for a detailed evaluation of their healthimpact. This strategy has the potential to be the most effective and practical approach for primary prevention ofGAS diseases in less developed countries.
Mass antibiotic treatment remains a valid strategy for prevention and control of outbreaks of GAS diseases inparticular situations. These include the prevention of ARF in military institutions and control of focal APSGNoutbreaks. Targeted antibiotic treatment - e.g. to family contacts of cases of invasive GAS disease - is of unprovenefficacy and could potentially only prevent a very small minority of cases.
The most successful GAS control activities have combined multiple strategies including primary prophylaxis,treatment of skin infections, health promotion, secondary prophylaxis and RHD registers. Although effective, thesecomprehensive programs require a substantial commitment from individuals and organisations (including Ministriesof Health).
In light of the current lack of a clear strategy for primary prevention of GAS infections, there is definitely a place fora safe, effective, affordable and practical GAS vaccine. It appears likely that the vaccine most advanced indevelopment - a multivalent, type-specific vaccine - will not provide sufficient and long-lasting protection in lessdeveloped countries, although this should be assessed.
vi
GROUP A STREPTOCOCCUS

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
1
Introduction
Large-scale activities to control GAS diseases historically have fallen mainly under the categories of register-based rheumatic heart disease (RHD) secondary prophylaxis programs, and management of acute rheumaticfever (ARF), RHD and sore throat / GAS pharyngitis. The prevention and control of ARF/ RHD and streptococcalpharyngitis have also been the most researched topics in the literature. However, because these activities do notencompass the entire range of potential strategies for controlling GAS diseases, this review will cover the technicalbasis for past and current approaches, as well as other potential approaches.
Because some diseases caused by GAS are not due to active infections (e.g. ARF, RHD, and acute post-streptococcal glomerulonephritis - APSGN), this report will refer to GAS diseases rather than GAS infections,except where specific active infections are inferred (e.g. invasive GAS infections).

2
GROUP A STREPTOCOCCUS
Potential approaches to controlling GAS diseases
Figure 1 outlines a simplified approach to understanding the spectrum of GAS diseases, and Table 1 details the types ofprevention strategies that could potentially be used. There is some debate as to whether the following interventionstechnically fall into the categories of primary, secondary and tertiary prevention as defined by Last. (1) For example, itcan be argued that secondary prophylaxis is tertiary, rather than secondary prevention. However, such argumentsare largely semantic. These categories are retained for simplicity.
This document will focus on approaches that can be implemented at a community or population level. Althoughissues such as the diagnosis of ARF and treatment of invasive GAS diseases are important and may have asubstantial impact on public health approaches to controlling these diseases, they are primarily clinical issuesand are therefore beyond the scope of this review.
Figure 1. A simplified approach to the spectrum of GAS diseases and potentialprevention strategies
Group A streptococcus
Skin Upper respiratory tract
Infection (Pyoderma) Infection (Pyoderma)ColonisationColonisation
Post-streptococcalglomerulonephritis
Acute rheumatic feverInvasive disease
Recurrent acuterheumatic fever
Rheumatic heart diseaseChronic renal damage
StrokeEndocarditisToxic shock,amputations, scars, etc
End-stage renaldisease
Cardiac failure,etc
Primaryprevention
Secondaryprevention
Tertiaryprevention

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
3
PRIMARY PREVENTIONThis refers to measures aimed at reducing exposure to GAS organisms, preventing GAS disease once the organismhas been encountered, or to preventing the direct sequelae of superficial infection. The following primary preventionstrategies may be considered:
Reducing overall exposure to GASThis refers to interventions that reduce the number of organisms in a population, or the likelihood of transmission.This is the main mechanism by which many GAS diseases have become relatively uncommon in more developedcountries over the past century. In this context, it mainly refers to improved living standards and improved hygiene.GAS is a highly transmissible organism. (2, 3) The importance of crowding in transmission of GAS has been welldemonstrated in US military studies and other case reports of focal outbreaks. (4-7) Some strategies within thiscategory may theoretically be feasible – e.g. reducing classroom sizes in schools – but for the most part thesechanges are intrinsically linked with economic development. Although this must remain the ultimate goal, itcannot form the basis of a coherent control strategy in the short to medium term, and will not be further addressedhere. The exception is mass antibiotic treatment (see below).
Primary prophylaxisThis refers to the prevention of ARF by timely and complete antibiotic treatment of GAS pharyngitis. It has beenvery well demonstrated that a 10-day course of an appropriate oral antibiotic (usually oral penicillin V) or a singledose of long-acting intramuscular penicillin (benzathine penicillin G - BPG), if administered within 9 days of theonset of symptoms of GAS pharyngitis, will prevent most cases of ARF. (8-10) It has never been demonstratedthat antibiotic treatment of GAS pharyngitis or pyoderma is able to prevent APSGN. (11)
1. Primary prevention
Reducing overall exposure to GASPrimary prophylaxisPrimary prevention of skin infectionsAntibiotic treatment to interrupt transmission of organismsImmunisation
2. Secondary prevention
Early and correct diagnosis of ARF*
Secondary prophylaxis
3. Tertiary prevention
Management of RHD patientsTreatment and rehabilitation of invasive GAS infections *
Table 1. Outline of approaches to preventing GAS diseases
* Not addressed further in this document, as these topics relate primarily to clinical care rather than public healthinterventions.

4
GROUP A STREPTOCOCCUS
Primary prevention of skin infectionsBecause GAS skin colonisation precedes skin infection, and superficial skin trauma (e.g. from scratching due toscabies infestation or insect bites) is a pre-requisite for GAS infection, there is the potential for preventing skininfections by preventing or eradicating GAS colonization (e.g. via washing and other hygiene interventions) orunderlying infestations (e.g. scabies control programs).
Antibiotic treatment to interrupt transmission of organismsThis intervention is aimed at treating the infection and also preventing transmission of virulent organisms to others.Interruption of transmission is a consequence of antibiotic treatment of GAS pharyngitis (e.g. by eradicatingcarriage of pharyngitis-causing GAS organisms, they cannot be spread to others), and also of antibiotic treatmentof skin infections. This approach may be extended to the possibility of mass antibiotic treatment of a group of at-risk people, in an attempt to simultaneously treat those infected with a virulent GAS strain and prevent transmissionto those not yet infected. Such a strategy may be particularly useful in certain disease outbreaks (e.g. APSGN,ARF) or when close contacts of infected people are considered at increased risk (e.g. invasive GAS infections).
ImmunisationAlthough there have been multiple attempts to produce a GAS vaccine for approximately a century, none of thecandidate vaccines has proceeded beyond preliminary animal or human studies until recently. Currently, there isone GAS vaccine in phase 2 human trials, and a number of others approaching human trials.
SECONDARY PREVENTIONThis refers to early detection of GAS diseases, such that interventions can be instituted to prevent sequelaedeveloping. The only secondary prevention measures widely practiced are those aimed at ARF and RHD:
Early and correct diagnosis of ARFThis is difficult in many settings, because of the non-specific nature of the diagnostic criteria for ARF, and the lackof suitable laboratory and echocardiographic facilities. Accurate diagnosis has the potential to be life-saving, notonly because severe acute cardiac failure may be managed, but also because secondary prophylaxis may becommenced.
Secondary prophylaxisThis refers to the regular administration of antibiotics (usually intramuscular BPG every 3 to 4 weeks or twice-dailyoral penicillin V) for many years to people with ARF or RHD, in order to prevent recurrences of ARF that may leadto the onset or increased severity of RHD.
TERTIARY PREVENTIONThis refers to measures to reduce the severity or long-term impact of GAS diseases. In practice, it mainly refers tomanagement of patients with RHD or the sequelae of invasive GAS infections. Because the extent to which APSGNcontributes to end-stage renal disease (ESRD) prevalence is not clear, renal failure management programs willnot be included here. However, it should be recognized that APSGN may be a major causative factor in somepopulations with very high rates of ESRD (e.g. Aboriginal Australians). (12)

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
5
Management of RHD patientsThis specifically refers to the treatment of cardiac failure (including medical and surgical treatment such as cardiacvalvotomy, valve repair or replacement), and prevention and management of endocarditis and stroke. Ideally, themanagement and follow-up of RHD patients is linked with register-based secondary prophylaxis delivery, as partof a coordinated RHD control program.
Treatment and rehabilitation of invasive GAS infectionsThis particularly refers to the sequelae of necrotising fasciitis. These patients may suffer amputations or scarring,requiring long-term physical and psychological rehabilitation.

6
GROUP A STREPTOCOCCUS
Evidence for certain control strategies
PRIMARY PROPHYLAXISThe efficacy of primary prophylaxis in preventing individual cases of ARF is proven beyond doubt. There havebeen some questions in recent years about the most appropriate regimen, given that the incidence of penicillintreatment failure of GAS pharyngitis appears to be increasing. (13, 14) However, the affordability, availability, andcontinued high efficacy of penicillin mean that it remains the recommended first-line therapy for GAS pharyngitis.(15, 16) Recent studies have suggested that once-daily oral amoxycillin may be as effective as twice- or thrice-daily oral penicillin,(17, 18) although direct comparisons with single-dose benzathine penicillin G have not beenmade.
In 1991, the WHO Global Acute Respiratory Infection treatment programme recommended that, in countrieswhere there were no other guidelines and in the absence of adequate microbiological diagnostic facilities, childrenaged less than 5 years should be presumptively treated for streptococcal pharyngitis if they had pharyngealexudate and tender, enlarged cervical lymph notes.(19) It is widely acknowledged that these recommendationsapply to school aged children as well. A 1999 WHO meeting called for the development of better tools for theclinical diagnosis of GAS pharyngitis.(20) The use of clinical algorithms to identify patients with a high likelihood ofGAS pharyngitis has been contentious for many years. Numerous studies have produced highly variable positiveand negative predictive values of such algorithms. (21-28) It has been argued that, if clinical algorithms performimperfectly under research conditions, they are even less likely to be useful in countries where the working conditionsand training of health staff are highly variable. (29) WHO is presently co-funding another multi-centre study todetermine the performance of the WHO criteria and other clinical predictors.(30) The report of that study is not yetavailable. It is mainly hospital based, so may not have the potential to evaluate the effectiveness of the algorithmat the level of the community clinic. A better clinical algorithm could substantially reduce over-prescription ofantibiotics for sore throat in many settings, although an algorithm that is insensitive would potentially result in manycases of ARF that could otherwise have been prevented with primary prophylaxis.
It has been suggested that, should it be demonstrated that clinical algorithms have insufficient sensitivity andspecificity, WHO should support an effort to develop a cheap rapid antigen test that could be used in developingcountries for microbiological confirmation of GAS pharyngitis. (31, 32) Supplying primary care clinics in developingcountries with rapid antigen tests and ensuring that health care workers were properly trained in their use wouldbe difficult and expensive. This approach should only be undertaken in the knowledge that it would have asubstantial benefit in terms of ARF prevention, and would be cost-effective.
It is not clear, however, that primary prophylaxis is effective as a public health strategy. Recommendations forprimary prophylaxis range from targeted treatment of those with proven GAS culture- or antigen-positive pharyngitis(usually not requiring serological confirmation), to targeted treatment of those with an increased likelihood of GASpharyngitis based on clinical features, to mass treatment of all children with sore throat without the need for throatswabbing. It has been acknowledged that the facilities, resources, skills and patient compliance available in mostless developed countries make a strategy based on microbiological diagnosis of patients with sore throatunworkable. (33, 34)
A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
7
Because only approximately one-third of cases of sore throat in children (and 5-10% in adults) in affluent,temperate countries are due to GAS, (35, 36) the approach of treating all patients with sore throat wouldbe very expensive and result in unnecessary antibiotic treatment of many patients who do not have GASpharyngitis. This has the associated dangers of adverse events and emergence of antibiotic-resistancein organisms such as pneumococci. A policy of treating all sore throats in children using intramuscularBPG, introduced in Costa Rica during the 1970s, was temporally associated with a dramatic reduction inthe incidence of ARF (Arguedas & Mohs, 1992). However, the major part of the decline occurred prior tothe increased use of BPG. This suggests that other factors, possibly related to the establishment of anational health plan at the same time, may have contributed to the reduction in new cases of acuterheumatic fever. In some populations with high ARF incidences, for example in Aboriginal Australians,this strategy is recommended. (37) However, neither the American Heart Association or WHO recommendsthis strategy universally.
In some countries where ARF is now rare (e.g. the United Kingdom and Australia), there are increasingcalls to abandon the antibiotic treatment of GAS pharyngitis, with the argument that the clinical effect oftreatment is minimal, and the rarity of ARF makes its prevention a minor consideration. (38-40)
So, there continues to be debate about the treatment regimen that should be used in GAS pharyngitis,the most appropriate means of identifying which sore throat patients should be treated, or even whetherGAS pharyngitis should be treated at all. The cost-effectiveness of primary prophylaxis is discussedlater in this report. However, there is conflicting evidence to support the contention that, even if anagreed and workable diagnostic and treatment strategy can be identified for the treatment of GASpharyngitis, it will have a substantial public health impact, particularly on the incidence of ARF.
Public health impact of treating GAS pharyngitisOn theoretical grounds, it is not clear that such a strategy would have the potential to prevent most casesof ARF in a population. Even if all cases of sore throat caused by GAS were identified within nine days ofonset and all of these cases took a complete course of an appropriate antibiotic, and assuming that suchan intervention retained the high level of efficacy found in the early studies of primary prophylaxis, mostcases of ARF do not follow a symptomatic sore throat and are therefore not preventable using sore throattreatment. In a careful study from Chile, 52% of ARF patients had no evidence of prior sore throat orscarlet fever, and another 40% had doubtful histories of prior GAS infection. (41) During the resurgenceof rheumatic fever in the USA during the 1980s, only 28% of patients reported a history of sore throat. (42)In the Australian Aboriginal population, <10% of ARF cases reported a preceding sore throat. (43)Moreover, many people with sore throat do not attend medical services or do not receive antibiotics ifthey do attend. In the recent US outbreaks, more than one-third of people with ARF who reported arecent sore throat either did not see a doctor at the time or were not prescribed antibiotics. (42) In Chile,only 8% of ARF patients had a definite GAS pharyngitis preceding the episode, of whom three-quartersattended a medical clinic and half received an antibiotic prescription. (41) The difficulty in interpretingthese data is that they do not provide information about the number of cases of GAS pharyngitis (andthus potentially avoided ARF cases) that were treated with antibiotics in the same population. In countriessuch as the USA, where sore throat diagnosis and GAS pharyngitis treatment is widely advocated, it maybe that most potential ARF cases are prevented by treatment of GAS pharyngitis. Better data from countriesthat claim lower rates of antibiotic treatment of GAS pharyngitis – e.g. some countries in Europe – mayclarify the potential impact of primary prophylaxis on ARF incidence.
8
GROUP A STREPTOCOCCUS
Of course, the overall effect in a population of primary prophylaxis may be greater than the direct effect on thosetreated if this strategy reduces the transmission of “rheumatogenic” GAS strains to others. As will be discussedlater, antibiotic treatment of GAS pharyngitis has the potential to eradicate carriage of GAS, and mass treatmentwith antibiotics can prevent transmission to others. However, the effectiveness of treating GAS pharyngitis as ameans of interrupting transmission of rheumatogenic GAS strains is unknown.
The potential for school-based surveillance and treatment of streptococcal pharyngitis to prevent ARF on a largescale was first raised in the USA during the 1950s, initially in a program with limited success, (44) but then later ina more comprehensive approach in the district of Casper in Wyoming, USA. (45) Over two years, 6,460 primaryschool children were asked daily if they had symptoms of respiratory infection, and those with symptoms hadnasopharyngeal cultures taken. Any child with a beta-haemolytic streptococcus was prescribed intramuscular ororal penicillin and excluded from school until therapy had started or until culture-negative. This was augmentedby screening of families of children with repeated positive cultures, and some carriage screening in schools. Thisdramatic approach resulted in a steady decline in both the proportion of swabs taken that grew beta-haemolyticstreptococci (from over 9% early in the school year to less than 4% later in the year) and in the proportion ofenrolled children with positive swabs (from 2 to 3% early in the year to approximately 1% later in the year). Atransient increase in cases following the Christmas break suggested that the program itself was having an impact,rather than other factors such as seasonality. Only 5 cases of ARF were found in these children during the 2 years(incidence 30 per 100,000 during the second school-year) which was dramatically less than in two comparisonschool districts in Wyoming (240 and 410 per 100,000, respectively, during the second school-year). Althoughthe lack of true control data makes it difficult to be certain of the impact of this program, the data suggest that mayhave been effective. As a minimum, this program demonstrated the effectiveness of surveillance-based treatmentin reducing streptococcal transmission. This was subsequently demonstrated in other US streptococcal controlprograms, most of which were labour and cost-intensive, and often applied strict legally-enforceable school-exclusion to children with streptococcal pharyngitis. (46-48)
An alternative approach was tried during the late 1960s and early 1970s in eight counties in Ohio. (49) Thisprogram aimed to make the process of throat culturing patients with pharyngitis easier, by providing free swabbingkits and a centralized culturing and reporting service. Between 1966 and 1970, the number of cultures approximatelydoubled, but the proportion of GAS positive swabs remained relatively constant at about 20% (about 10% inwarmer months and 25 to 30% in colder months). The impact on ARF incidence is not clear. During 1966-67, theaverage annual attack rate of ARF was 17.5 per 100,000 people aged 5-19 years, compared to 30 per 100,000during 1964-65. However, the incidence of ARF during ensuing years of the program was not reported.
A larger four-year project involving approximately 17,000 Navajo Indian school students during the 1970s includedcultures of symptomatic children, carriage surveillance every 1 to 2 months, and treatment of those with GAS-positive cultures. (50) ARF incidence in the approximately 50% of children who attended schools considered tobe active in the program was compared with that in the other 50% attending “uncovered” schools. Twenty-fourpercent (7 of 29) of ARF cases occurred in active schools (p<0.05) and most of these children had missed theroutine cultures prior to their ARF episodes. Based on data prior to the program, the authors concluded that theoverall rate reduction due to the program was 21% (from 12.6 to 10.0 per 100,000 per year), representing 3.1 ARFcases prevented per year. Although the program appeared to have a significant impact on ARF incidence, it costUS $200,000 per year to run (almost US $12 per enrolled child per year, in 1970s currency), or almost US $65,000per ARF case prevented. By comparison, the total cost of an ARF case was estimated to be US $10,560, so 19cases per year (rather than 3.1) would have had to be prevented for the program to be cost-neutral.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
9
A similar control program in Alaskan Eskimo children from 1972-76 reached slightly different conclusions. (51)This program combined swabbing of symptomatic children, regular surveillance swabbing of asymptomaticchildren, benzathine penicillin G (BPG) treatment of those with GAS-positive swabs (whether symptomatic or not),and mass prophylaxis with BPG in villages where GAS epidemics occurred. During the five years of the program,the risk of GAS colonization reduced steadily to 55% of the baseline risk, but reducing the frequency of surveillanceswabbing from every 4 weeks to every 8 weeks led to a 37% increased risk of colonization. There were 11 ARFcases in the participating villages (total population approx 2500, of whom just over 1,000 were aged 3-18 years)during the five years prior to the program, compared to 0 during the five years of the program. In a group of similarcomparison villages (total population 2350) there were 7 and 4 ARF cases during the same respective periods.Therefore, there may have been a positive impact on ARF incidence, although this is uncertain. The program costapproximately US $113,000 over five years in 1971 currency (or US $21.50 per child per year). The authorsestimated that the average cost of an ARF case in this population was US $35,500, so only approximately 3 caseswould have had to be prevented over five years to make the program cost-neutral.
In Hawaii, where ARF was largely confined to Hawaiian and Samoan children, a similar school based surveillanceprogram was established during the 1970s. Children with GAS isolated from throat swabs were excluded fromschools until antibiotic treatment had started. (52) However, the incidence of ARF in participating schools was nodifferent to that in non-participating schools, so this program was abandoned.
A community-based ARF control program in an Australian Aboriginal community included widespread communityeducation, and throat swabbing of 4-16 year olds three times per year for six years (with antibiotic treatment ofGAS carriers). (53) The ARF incidence in the community was said to be 4 per 1,000 per year prior to the program,whereas only one case occurred in the 6 years of the program. While this report raised the possibility that ARFcould be effectively controlled in the Aboriginal population, questions were raised about the completeness of thedata included in the report, and subsequently a number of ARF cases occurred in the community. (54)
A recent randomised controlled trial from south Auckland, New Zealand has provided the best available data onthe effectiveness of primary prevention of ARF based on GAS sore throat detection and treatment. (55) Thisregion has a high proportion of Maori and Pacific Island residents, who live in relative poverty and have a highincidence of ARF. In this study, schools were randomised either to receiving a sore throat intervention or not. Inthe intervention schools, a full-time nurse was employed. Each child in these schools was asked every day if theyhad a sore throat, in which case a throat swab was taken. Children with a positive swab for GAS were offered a 10-day course of oral amoxicillin twice a day. At the conclusion of the study, 29 cases of ARF had been detected incontrol schools compared to 24 in intervention schools. Overall, the program cost approximately US $50 perchild enrolled per year, and did not lead to a significant reduction of ARF incidence. A subsequent re-analysis ofthe data has led to a re-allocation of some cases, resulting in the program having a significant effect on ARFincidence, although the re-analysed data have not yet been released (Personal Communication, D Lennon, June2003). A further year of data is to be collected, and an economic analysis will be performed. Therefore, a finalconclusion about this study cannot yet be made. However, the effect size is likely to be no greater than a one-thirdreduction of ARF incidence, and the overall cost of the program will remain expensive. This study was conductedunder rigorous research conditions, which would be impossible to replicate in most less developed countries.Even if such a program could be conducted in less developed countries, very few countries could justify such anexpense in order to reduce ARF incidence by one-third.

10
GROUP A STREPTOCOCCUS
In summary, school and community-based studies from the USA suggest that an intensive and expensivesurveillance and treatment strategy is likely to reduce throat colonisation rates with GAS, may reduce the incidenceof GAS pharyngitis, and may also reduce the incidence of ARF. This latter contention is not supported by controlleddata from those studies. The US studies also suggested that such programs are expensive to run, and may not becost-neutral or cost-saving. Programs in populations with higher incidences of ARF – particularly in indigenouspopulations in North America – demonstrated even less convincing results. The best data come from the NewZealand randomised trial, the effectiveness of which was limited, and the rigour by which it was conducted unlikelyto be achievable in any less developed country public health program. The data from Costa Rica are inadequateto conclusively demonstrate the efficacy of universal sore throat treatment with penicillin.
Therefore, the limited efficacy in ARF prevention, the expense (the cost of these programs exceeds the annualper-capita health care budget of most less developed countries), and the complexity of these approaches, makeit impossible to recommend them widely to less developed countries as a public health strategy. Some middle-income countries may choose to make the public health investment in a systematic sore-throat treatment strategy,in the knowledge that the majority of ARF cases will probably not be prevented. Regardless of the public healthapproach taken, primary prophylaxis remains important for individuals who present with GAS pharyngitis, whenthe facilities exist to diagnose and/or treat it. This conclusion has also been reached by WHO. (34)
PRIMARY PREVENTION OF SKIN INFECTIONSCommunity control of skin infections by treating and preventing scabies infestation has been remarkably successful.A program in Panamanian island communities began with mass treatment with 5% permethrin cream, followed byregular screening and re-treatment of persistently or recurrently infested individuals, with the result that scabieswas virtually eradicated and bacterial skin infections were dramatically reduced. (56) This approach led to similardramatic reductions in an Australian Aboriginal community, and had the further benefit of halving the rate ofimpetigo in children, with remaining impetigo lesions being, on the whole, mild. (57) Scabies control programscontinue successfully in some Aboriginal communities. (58)
More recently, the oral medication ivermectin has been used for scabies control in the Solomon Islands. (59)Ivermectin is widely used for lymphatic filariasis and is cheaper, much easier to use, and usually less culturallysensitive than permethrin cream (which requires whole body application). The whole populations of five smallisland communities in the Solomon Islands study were treated with oral ivermectin (or topical permethrin creamfor children <15 kg or pregnant women). Two treatments were offered to each resident, two weeks apart, andvisitors to the island were also offered treatment. Surveillance was maintained for 3 years (with further treatmentsoffered to occasional children who had persistent or recurrent scabies). Scabies prevalence reduced from 25%to <5% after 4 months, and steadily declined to <1% over 3 years. The impetigo prevalence declined from 40%to 21%, and GAS recovery from the fingertips of children reduced from 61% to 32%. The prevalence of microscopichaematuria in children also reduced significantly, suggesting an effect on subclinical post-streptococcalglomerulonephritis. Ivermectin treated children had less treatment failure than those treated with permethrin, andno adverse effects of ivermectin were noted. A control island was observed during the first 6 months of theprogram, and no change in scabies prevalence was noted. These results are similar to those from the Aboriginalcommunity study, (57) and also demonstrate the efficacy and safety of ivermectin.
An observational study in Papua New Guinea found that mass ivermectin treatment for filariasis appeared tosubstantially reduce scabies prevalence. (60) The impact on scabies, skin infections, and post-streptococcal

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
11
diseases of mass treatment with ivermectin for filariasis and onchocerciasis in Africa has not been evaluated (LSavioli, personal communication 2002).
The success of community scabies control programs raises the possibility of other community-based measures incontrolling skin infections. The addition of hygiene measures to scabies control programs has not been evaluated(such an evaluation is presently planned in Australia), but there is evidence from Burkina Faso that health promotionalactivities related to children’s hygiene can change levels of understanding and some simple practices such ashandwashing at the community level. (61)
Personal hygiene is an important pyoderma risk factor. In a study in Colombia, climate was the most importantdeterminant of pyoderma prevalence, but within each climatic zone the children with poor hygiene had higherrates of pyoderma than those with good hygiene. (62) In a longitudinal study of six native American families,weekly showering in school may have contributed to declining rates of pyoderma during the month after the startof the school year. (63) In a cross-sectional survey of children in Mali, poor individual hygiene (assessed subjectively)was associated with a significantly increased risk of pyoderma (odds ratio 1.68, 95% CI 1.20-2.35). Interestingly,in this arid area the mean number of baths per week per child was 10, and 85% of children used soap.
A Tanzanian study found that rural children had lower cleanliness scores than urban infants attending child healthclinics, who in turn had lower scores than older urban children attending nursery and secondary schools. (64)Scabies-related pyoderma correlated with personal hygiene (41% in rural children, 16.8% in urban child healthclinic children, and 7.9 to 10% in the older urban children), but non-scabies related pyoderma remained relativelyconstant regardless of these variables. However, a number of methodological problems compromised the findingsof this study.
A placebo-controlled study from Trinidad during the early 1970s looked at the effect of plain soap, antisepticsoap, and benzathine penicillin G on pyoderma prevalence in children of two villages. (65) Seventeen families ineach village were assigned alternately to treatment or placebo groups. Following 12 weeks of observation, thetreatment group were washed twice daily with plain soap for eight weeks and then antiseptic soap for eight weeksbefore receiving two doses of benzathine penicillin G over the following eight weeks, after a two week rest period.The placebo group received only a placebo medication each evening. The rather surprising findings includedsignificantly increased rates of pyoderma in the treatment group compared to the control group during the trialwith plain soap and with antiseptic soap, and no decrease in pyoderma rates during the penicillin treatmentperiod (despite GAS isolation from these lesions decreasing to 0 during this time). The authors concluded thathygiene interventions in themselves could not be expected to control GAS skin infections, but should be combinedwith measures to prevent minor trauma and biting insects. However, the rates of pyoderma were already significantlyincreased in the treatment group in the pre-treatment period of observation, raising questions about the adequacyof randomisation, and there were a number of other methodological problems. Regardless, this study suggeststhat the use of soaps alone to control pyoderma may not hold great promise.
Others have found little benefit in using soaps for the treatment of established pyoderma. One controlled studyfound that erythromycin cured most cases of pyoderma whereas compresses and soap offered no benefit overplacebo. (66) In another study, antiseptic scrubs alone cleared only 9% of pyoderma after two weeks comparedto 39% when combined with local antibiotic ointment, 83% when combined with oral penicillin V and 96% whencombined with intramuscular BPG. (67)

12
GROUP A STREPTOCOCCUS
Although most studies of the impact of water supply on health, particularly on diarrhoeal diseases, have hadmethodological problems, (68) the weight of evidence about the role of water use in pyoderma favours theimportance of water quantity rather than quality. However, improved water availability alone may not substantiallyreduce rates of transmissible skin diseases in the absence of education about how best to use the water toimprove personal hygiene. (69)
A case-control study in a Gambian village which was designed to look at water use and trachoma also includedan assessment of pyoderma. (70) In the five families where at least one child had pyoderma, the mean volume ofwater used for washing children was significantly less than in the 29 families without pyoderma (2.68 litres/child/day compared to 5.71, p=0.015). A comparison study in Panama evaluated in-house water taps on one islandwith a traditional distant stream water source on another island. (71) Water use in the former island was substantiallygreater than in the latter (7.1 litres/person/day compared to 2.3), and the incidence of childhood pyoderma wassignificantly greater on the island with poor water availability (0.6 episodes/child-year compared to 0.2, p<0.05),although it is not clear that this difference could be attributed to water availability. Another observational study intwo villages in Mozambique found an apparently significantly reduced prevalence of skin infections (11% comparedto 17%) in a village with its own water supply compared to one with a distant supply. In a Ugandan study, childrenin one village with “poor” nutritional status and “poor” water supply had a 75% prevalence of skin disease, comparedto 29.8% among children from a village with “adequate” nutrition and “good” water supply. [Porter, 1977 #1100.In a 24-week prospective study in the southern USA, there was a trend to reduced prevalence and severity ofpyoderma in children with a piped water supply in their house; 37.9% of those with piped water and 32.1% ofthose without piped water had no pyoderma, whereas 44.3% of those with piped water and 48.8% of those withoutpiped water had “high prevalence” of pyoderma. (72) A study in two Tanzanian villages found no associationbetween the distance from household to water source and the prevalence of transmissible skin disease, using 20minutes distance as the cut-off point, although pyoderma made up less than 10% of all transmissible skin diseasein this study. (73)
On the same theme of water supply and hygiene, there is some evidence that regular use of swimming pools maybe effective in controlling skin infections. An early report suggested that the opening of a swimming pool in anAustralian Aboriginal community was associated with reduced prevalence of skin infections in children who swamseveral times each week. (74) A further evaluation of the introduction of swimming pools in two remote Aboriginalcommunities in Western Australia is ongoing. (75) In the first 12 months after the introduction of the pool in onecommunity, the prevalence of impetigo has decreased from 64% to 21%, and the prevalence of “severe sores”has reduced from 28% to 3%. The pools have also been associated with improvements in chronic ear infectionsand perforations (47% of children had improved ears), nasal discharge (which resolved in 26% of children),school attendance, and juvenile crime rates (the latter presumably being attributed to the effects of the pools inimproving community morale and cohesion). In the other community, the prevalence of mild impetigo lesions hasnot changed, but the prevalence of “severe sores” reduced from 28% to 5% after one year. Overall, the skincondition improved for 42% of children at this community, the ear condition improved for 33%, and running nosedisappeared in 23%. These results show a clear short term benefit for child health and also suggest morewidespread social benefits of community swimming pools in remote Aboriginal communities. The ongoing studywill confirm if these benefits are sustained in the long term, and will document any microbiological changes thathave accompanied the changes in impetigo prevalence.
Household crowding is associated with pyoderma. In the same Tanzanian study, people who lived in houses withmore than 10m2 per person had significantly less transmissible skin disease than those with less than 10m2 per

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
13
person (10.5% compared to 21.4%, p<0.01). (73) A survey of 17,687 people in Vanuatu found that the prevalenceof skin infections increased from 10% in people living with 1 to 2 people per household up to 17% in those with 11or more people per household. (76) The southern USA study already cited found no association between householdcrowding and pyoderma prevalence, although the study population may have been too homogenous to detectdifferences in environmental influences. (72) In New Zealand high school students, the highest rates of pyodermawere found in Pacific Island Polynesian (PIP) (3.2%) and Maori (2.3%) students, who also showed high rates ofovercrowding (29% of PIP and 21% of Maori students lived in houses with ³5 children compared to 3% of Europeanstudents. (77) No specific analyses were performed on these data to directly associate overcrowding withpyoderma. In a regional survey in Mali, no association with overcrowding was found, but most of the people in theregion lived in overcrowded houses (an average of 20 people per house). (78)
Malnutrition has not been extensively studied as an independent risk factor for pyoderma. Taplin and Allen (1975)commented about their Colombian studies that they found no such association because all of the children theysaw “showed every evidence of adequate diet,” although no evidence in support of this statement was provided.Porter (1977) referred to an individual’s susceptibility to infectious skin diseases being influenced by nutrition,among other factors. There is little evidence to support this claim.
A frequent theme in studies of pyoderma is the contribution made by biting insects. Many of the studies alreadycited as well as others refer to secondary infection of bites from insects like mosquitoes and sandflies. (69, 79, 80)In Tanzania the insect populations in the home and school environments were assessed, with the claim thatchildren aged less than 2 years most frequently had insect bites underlying their pyoderma lesions, whereasthose over 2 years more commonly had underlying trauma. (64) There were no studies available on the impact ofinsect control measures on pyoderma prevalence.
Hot, humid weather is the most consistently found contributor to pyoderma prevalence. (62, 69, 72, 79, 81-84)There is evidence that pyoderma is also more common in warmer months in temperate climates, including in theUSA and Australia. (85, 86) However, exceptions to this seasonality have been documented from Trinidad, wherepyoderma occurred at similar rates throughout the year, and outbreaks of pyoderma-related acute post-streptococcal glomerulonephritis did not follow a seasonal pattern. (87) This was attributed to the relativelyconstant year-round climate of this tropical island. (83) (Dillon, 1970).
The contribution of warm climates to high pyoderma rates may be multifactorial; relating to skin trauma andtransmission of pathogens by insects and scabies mites, possibly to higher loads of pathogens present on skin,insects and fomites, and possibly to other undefined factors. But the fact that endemic pyoderma also occurs innon-tropical areas (e.g. Red Lake studies from the USA), presumably if other factors are present. The influence ofpersonal hygiene and volume of water may be critical.
In conclusion, of the many risk factors for pyoderma, those most amenable to intervention are scabies, hygiene,and household crowding. Community based scabies control programs have had documented success in reducingpyoderma prevalence and severity. The impact of mass ivermectin treatment may be substantial and should befurther evaluated. The added impact of hygiene measures (including swimming pools) is less clear but preliminarydata are encouraging. There are good reasons to expand skin disease control programmes in economicallydisadvantaged regions, but more evidence is needed relating the components of ideal programs, particularly assome recommendations may involve changes to personal and cultural practices, housing policies, and water andsanitation infrastructure programs.

14
GROUP A STREPTOCOCCUS
The potential benefits of controlling skin infectionsStreptococcal skin infections have numerous sequelae. The best described is acute post streptococcalglomerulonephritis (APSGN). Outbreaks of APSGN occur periodically in many less developed countries, and caninvolve hundreds of children. (88-97) The risk of developing APSGN during an epidemic is increased by five forchildren with skin sores and doubled for children with scabies. (96) APSGN in childhood has been shown toincrease the risk of adult renal disease amongst Australian Aboriginal people by six times. (12) Thus there is a linkbetween scabies and skin infections in childhood, and high rates of end-stage renal failure in some populations.
It has also been hypothesised that streptococcal skin infection may be linked with acute rheumatic fever andrheumatic heart disease, although this has not been proven. The details surrounding this issue are outlined inAppendix 1. The recent randomised controlled trial of sore throat-based primary prevention of ARF in NewZealand that failed to demonstrate a major effect on ARF incidence supports the hypothesis that not all ARF isdirectly due to throat infection with GAS. (55) A number of ARF-related GAS throat isolates from that study camefrom typical “skin”-associated emm types. (D Lennon, personal communication 2002)
Skin infections are the major underlying cause of serious bacterial infections with both GAS and Staphylococcusaureus in many communities. These infections are common in tropical less developed countries and have highmortality. (98-102) Moreover, children in tropical communities commonly have many skin sores (rather than theone or two sores that would raise alarm in other settings). (57) Skin infections are among the most commonreasons for childhood presentations to clinics in tropical less developed countries, and consequently for theprescription of antibiotics. (103) For example, scabies and skin infections were the two most common reasons forpresentation to an Australian Aboriginal primary care clinic, accounting for over 15% of all presentations. (104) Inaddition to the financial cost of these treatments, they undoubtedly contribute to the spreading epidemic of antibioticresistance.
It is not difficult to envisage that the bacteria from these skin sores may cause a proportion of the cases ofpneumonia and febrile illness that are common reasons for attending clinics or being admitted to hospital.Furthermore, chronic, persistent and severe skin infection may have effects on children’s immune systems andgeneral state of well-being, which lead to the inability to fight other infections (e.g. leading to increased frequencyand severity of some of the more common childhood infections such as pneumonia or gastroenteritis) and alsoimpairs children’s appetites, exacerbating malnutrition. Although plausible, the data to support these assertionsare only anecdotal. During a 2 year scabies control program in one Aboriginal community, (57) an apparentdramatic reduction in the proportion of children with malnutrition and the number with serious medical complaintswas noticed.
ANTIBIOTIC TREATMENT TO INTERRUPT TRANSMISSION OF GASThe early school-based studies of streptococcal control using surveillance and treatment of those infected with orcarrying GAS demonstrated that these strategies could reduce overall colonisation rates. The subsequent findingthat regular administration of antibiotics to patients with a history of ARF or RHD could prevent subsequentstreptococcal infections and recurrent episodes of ARF (see below, under Secondary Prophylaxis), raised thepossibility of mass administration of antibiotics to healthy people in high-risk situations, in order to avoid thepossibility of streptococcal infections. This strategy has been used for many years in the United States military toreduce the incidence of pharyngitis and ARF outbreaks. (105-108)

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
15
This approach has also been used for the control of skin infections. Benzathine penicillin G protects against GASskin infection for approximately 4 weeks (similar to the duration of protection against GAS pharyngitis). (109)Subsequently, mass administration of BPG has been used in populations with high rates of skin infections andAPSGN, with the intention of halting transmission of the virulent strain of GAS (as there is no evidence that treatmentof an individual already infected with a nephritogenic strain will prevent the development of APSGN). (88, 94, 110,111) The reports are anecdotal, but when considered together they provide compelling evidence of theeffectiveness of this strategy. This approach has been refined in the Northern Territory of Australia, such thatrecent outbreaks of APSGN have been contained by administration of BPG only to children with impetigo. (96)
There is not complete agreement on the use of antibiotics in close contacts of people with invasive GAS infections.Surveillance of over 10 million people over 2.5 years in Ontario detected four cases of invasive GAS infection in1360 household contacts of other cases (attack rate 294 per 100,000 compared to the incidence of sporadicdisease in the wider population of 2.4 per 100,000; an increased risk of over 120-fold). (112) This study also foundthat all GAS isolates in the throats of close contacts were identical to those in the index cases. As a result, theOntario GAS Study Group recommended antibiotic prophylaxis for close contacts, and the Ontario Ministry ofHealth stated that chemoprophylaxis “may be considered” for contacts. (113, 114) By contrast, surveillance ofover 12 million people over 2.5 years in several US states detected only one case in 1514 household contacts(attack rate 66 per 100,000 compared to the incidence of sporadic disease of 3.5 per 100,000; an increased riskof approximately 19-fold).(115, 116) As a result, the CDC recommends against routine screening or antibioticprophylaxis for contacts of invasive disease cases.
It is clear from the above studies that, although close contacts of cases of invasive GAS disease may be atincreased risk of the same disease, these secondary cases represent a very small proportion of all cases in thecommunity (<0.6% of all cases in the two studies mentioned above). Therefore, antibiotic prophylaxis to contactsis likely to prevent very few cases, although the potential effect may be somewhat increased if the interventionreduces circulation of virulent GAS in the community in addition to preventing direct cases in close contacts.Moreover, it is not proven that antibiotic prophylaxis to contacts will prevent disease. The CDC conclusions havebeen questioned in the light of a number of descriptions of household clusters and other outbreaks of invasiveGAS disease.(117-121) Although the use of antibiotic prophylaxis to contacts of individual cases of invasive GASdisease may have a role, as a public health measure (including the establishment of active surveillance) it isunlikely to be cost-effective and could only prevent a very small minority of invasive GAS cases.
IMMUNISATIONA summary of the status of GAS vaccines currently in development and of the critical issues in preparing to havea GAS vaccine for less developed countries has been prepared as a separate part in this series of documents. Inlight of the current lack of a clear strategy for primary prevention of GAS infections, there is definitely a place for asafe, effective, affordable and practical GAS vaccine. For reasons outlined in the GAS vaccine summary document,it appears likely that the vaccine most advanced in development – a multivalent, type-specific vaccine – will notprovide sufficient and long-lasting protection in less developed countries, although this should be assessed.There is an urgent need for an organization such as WHO to undertake oversight and coordination of GAS vaccinedevelopment on a global scale. The priorities must be to ensure that a vaccine becomes available specifically forthe prevention of GAS diseases in less developed countries, that any vaccines are therefore tested for safety andefficacy in less developed countries (or similar settings) using ARF, APSGN and skin infections as primary endpoints,and that preparations begin now for compiling important regional disease burden data that will be used in makingdecisions about introducing a GAS vaccine.

16
GROUP A STREPTOCOCCUS
COMPREHENSIVE STREPTOCOCCAL CONTROL PROGRAMSA comparative observational study in Baltimore during the 1960s demonstrated a dramatic reduction in ARFincidence in poor, predominantly black, inner-city regions where comprehensive medical care programs hadbeen established, whereas areas of similar demographic and socio-economic make-up experienced increasedrates. (122) Although it was thought most likely that the effect could be attributed to improved treatment of GASpharyngitis, the effect of other less-defined influences that may have accompanied the introduction ofcomprehensive care programs could not be excluded. The decline in ARF incidence in inner-city Baltimorecontinued, reducing from 14.0 to 1.0 per 100,000 between 1965 and 1981-83, which may partly be due to expansionof comprehensive care programs. (123) This study suggested that primary prevention of ARF was likely to becomplex, and to require a wider approach than simply focusing on sore throat management.
This was subsequently highlighted by a more comprehensive ARF control program in the French Caribbean.(124) This program involved the establishment of an ARF/RHD register and an extensive education campaignabout the nature and treatment of primary GAS infections, including pyoderma. The consequent reduction inincidence of ARF was impressive. However, the specific impact of individual factors of the program (e.g. sorethroat treatment) and of the economic development that took place in these countries over the same periodcannot be deciphered. For example, during the second half of the twentieth century many Caribbean countriesunderwent an “epidemiological transition”, in which infant and child mortality and communicable disease mortalityrates steadily reduced, at the expense of increasing adult mortality due to “Western diseases” (e.g. diabetesmellitus, ischaemic heart disease). (125, 126) This transition was attributed to improved socio-economic status ascountries moved from low-income to middle income levels, and is likely also to have affected other risk factors forrheumatic fever such as housing standards and access to medical care. Nonetheless, the French Caribbeanstudy offers hope that comprehensive GAS control programs can be effective.
The Cuban situation is also instructive. A formal RHD control program was instituted in 1972. Between the early1970s and the mid 1980s, the incidence of ARF and prevalence of RHD in Cuba decreased dramatically. Thiswas attributed to the combined effects of specific interventions including health education relating to ARF/RHDand secondary prophylaxis programs, together with improved economic and living standards and a universalhealth care system. (127, 128) In the Philippines the concept of using school curricula to introduce importanthealth promotion topics relating to cardiovascular diseases has been demonstrated. (129)
SECONDARY PROPHYLAXIS AND RHD CONTROL PROGRAMSStudies in the USA between 1939 and the 1960s clearly demonstrated that regular doses of antibiotics administeredto people with a history of ARF or RHD could prevent further recurrences of ARF. (9, 130-136) It has been clearlydemonstrated that monthly injection of intramuscular BPG is more effective than oral penicillin or sulfadiazine forboth the prevention of streptococcal pharyngitis and recurrent ARF. (137) A number of studies have documentedARF recurrence rates less than 0.6 per 100 patient-years on BPG prophylaxis. (summarised in (138)) In Gisborne,New Zealand, oral penicillin secondary prophylaxis was used between 1958 and 1973 and parenteral BPG wasused after 1974. In the oral prophylaxis period there was an average of 14 ARF admissions per year of which 35%were recurrences, but during the parenteral prophylaxis period this reduced to 7.7 admissions per year of whichonly 18% were recurrences. (139) The administration of regular antibiotics – usually BPG every 3 or 4 weeks, orevery month – for many years is now recommended for all people with a history of ARF or RHD. (140, 141)

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
17
The efficacy of secondary prophylaxis in not only preventing recurrent ARF, but also in reducing the severity ofRHD has been well documented. In the era before secondary prophylaxis, only 11% of 1,000 RHD patients werefree of heart murmurs after 10 years of follow-up. (142) By comparison, the MR murmur resolved in 70% of 79RHD patients on secondary prophylaxis after up to 8.5 years of follow-up. (143) A follow-up study of 497 childrenwith ARF found that 60% of patients with ARF recurrences had RHD after 10 years, compared to 34% of thosewithout recurrences, and the greatest effect was in those with mild MR at initial admission (89% with recurrenceshad persistent RHD compared to 18% of those without recurrences). (144) A 12-year comparative study of 249patients from Taiwan found that 3-weekly BPG led to reduced incidence of breakthrough streptococcal infectionsthan 4-weekly (7.5 compared to 12.6 per 100 patient-years, p<0.01), less recurrences of ARF (0.25 compared to1.29 per 100 patient-years, p=0.015), and resolution of MR murmurs in 66% of patients compared to 46% in the 4-weekly group (p<0.05). A number of other studies have documented that heart disease regresses in approximately50% to 70% of patients with RHD who comply with secondary prophylaxis over a decade. (145-147) The bestdata of the effect on mortality come from Taiwan, where after 8 years of follow-up, 3.4% of patients not on prophylaxishad died, compared to 0.6% of those on prophylaxis. (148)
Secondary prophylaxis is effective if delivered regularly. However, poor adherence to prophylaxis regimens hasbeen a major problem in many parts of the world. In Aboriginal Australians, only two-thirds of scheduled BPGinjections were delivered over a 12-month period, and 28% of recipients received d— 50% of scheduled injections.(149, 150) Others have found high rates of loss to follow-up and poor adherence to secondary prophylaxis to beassociated with worse outcome. (151-153)
To ensure that secondary prophylaxis is effectively delivered, it is also important to identify and follow-up potentialrecipients; i.e. people who have RHD or a history of ARF. Most people with RHD are asymptomatic, and thereforewill only be detected serendipitously when being examined, if they recall a previous episode of ARF and understandits implications, or as a result of screening. People who present with a new diagnosis of ARF or RHD will receivelong-term prophylaxis only if there is a mechanism in place to ensure the delivery of prophylaxis and long-termfollow-up. The World Health Organization recommends that secondary prophylaxis should be the cornerstone ofan RHD control program, which includes monitoring of ARF and RHD patients via a register, regular communicationbetween those who maintain the register and those who deliver secondary prophylaxis or clinical services in thecommunity, surveillance to detect new cases, clinical review of RHD patients, and some streptococcal surveillance.(140, 141) WHO and associated organisations have produced numerous guideline documents detailing the keyaspects of these control programs, often with an emphasis on education and training, integration with primaryhealth care, and the essential role of laboratory support. (20, 34, 140, 154-156)
The WHO Global Programme for the Prevention of Rheumatic Fever and Rheumatic Heart Disease aimed toestablish RHD control programs in 23 countries (16 in the initial phase of the program, with an additional 7countries added after 1991). (157, 158) The Programme prescribed a three-phase introduction of a controlprogram in each country: a pilot in a small region (Phase 1), expansion to a whole region or district (Phase 2), andthen national coverage with the addition of primary prevention measures where feasible (Phase 3). By 1990,almost 1.5 million school-age children had been screened, and over 3,000 cases of RHD or prior ARF had beendetected. (159) Many personnel had been trained, and health promotional activities undertaken. However, anumber of impediments to progress were also identified, relating in particular to shortage of resources, loss tofollow-up of participants, and problems in regularity and quality of reporting. A 1999 review of the progress of theProgramme (which has since been abandoned due to lack of funding) found excellent success in case finding

18
GROUP A STREPTOCOCCUS
(with >15 million school children screened) and in using the program to improve compliance with secondaryprophylaxis (overall compliance rates were 63%, ranging from 48% to 95%). (20) A review of a prior iteration ofthe Global Programme reported decreases in recurrence rate of ARF by 89.3% and in the number of streptococcalinfections by 66.2% in the 3382 patient-years of regular BPG secondary prophylaxis, and that a total of 9,500hospital days were averted by regular prophylaxis. (160, 161) Patients with poor adherence to prophylaxis regimensspent six times as much time in hospital as those who were fully adherent, and improving adherence had thepotential to avoid a further 6,500 hospital days. The major problem identified was the inability of most countries tomove beyond Phase 1, mainly due to lack of resources.
The major difficulty in assessing the Global Programme is the inability to evaluate the data quality, and the lack ofstandardisation of evaluation data, in all countries. For example, four of five countries reported reductions in RHDprevalence, attributed to the control programme, but in no case was it clear that the methods and population usedfor data collection were the same for the before and after surveys, or between countries (e.g. in most of thesesurveys, there was no attempt to validate the screening tools using echocardiography). The 1999 consultationrecognised this, and developed a set of standardised definitions to be used in future evaluations. (20) In fact,control programs can be expected to lead to an apparent initial increase in RHD prevalence. For example, systematiccase detection has been in place in the Aboriginal population of the Australia’s Top End since 1994, and since1997 this has taken the form of a register-based control program. The number of cases of RHD in this populationcontinues to rise as more cases are detected; from approximately 450 in 1998 to over 700 in 2002. (162)
A more recent evaluation of the effectiveness of control programs has been conducted in three countries withmore extensive reporting; Cuba, Egypt and Sudan.(P Nordet, unpublished data) Between 1986 and 1996, therewas clear improvement in Cuba and Egypt in compliance with follow-up and secondary prophylaxis, ARF incidencerates, and RHD prevalence (down from 1.9 to 0.2 per 1,000 in Cuba, and from 5.3 to 2.3 per 1,000 in Egypt). Theprograms were being extended to other areas of these two countries. In Sudan, compliance with follow-up andsecondary prophylaxis remained a problem, although showed some improvement, but there were insufficientdata to evaluate the effectiveness of the program on ARF incidence or RHD prevalence.
The New Zealand experience is perhaps the most compelling in favour of formal register-based control programs.During the early 1980s, many NZ health districts introduced these programs with documented success. (163,164) For example, in Auckland between 1972 and 1981, prior to the introduction of a control program, 22% of allARF episodes in children <15 years were recurrences, but between 1982 and 1992 this reduced to 6%, with arecurrence rate of 0.6 per 100 patient-years. (138) By 1998, half of New Zealand’s 24 health districts had RF/RHDregisters, covering over 94% of notified ARF cases. (165) These registers were categorised as either “Surveillanceregisters” whose main function is maintaining client lists and promoting notifications, or “Management registers”that perform the same functions as surveillance registers but in addition coordinate the management of secondaryprophylaxis provision
However, in countries with less resources, where health services are poorly coordinated, or where access ofhealth services to substantial proportions of the population is limited by geography or other factors, implementing,maintaining and evaluating RHD control programs is more difficult. For example, the Top End Australian ControlProgram has led to improved case detection of RHD (outlined above), and initially saw reductions in ARF incidenceand the proportion of cases that were recurrences (from over 40% at the start of the program to less than 30%during 2000 and 2001). (162) But 2002 saw a resurgence in ARF incidence and the proportion of recurrent cases(to 48%), highlighting the difficulties in maintaining adherence with secondary prophylaxis even with formal controlprograms.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
19
There are a number of examples of successful register-based secondary prophylaxis programs in India. In theAmbala District of northern India, an RHD control program was established in 1987. An evaluation during 1995found very high levels of awareness of the importance of secondary prophylaxis, high levels of satisfaction withthe program, and that >90% of patients missed no more than one monthly injection per year during the first 7years of the program. (166) Only one patient reported a recurrence of ARF. A further follow-up in 1999 confirmedthat compliance rates were maintained >90% for the 12 years of the program. (167) In the Shimla Hills of northernIndia a strategy was devised to integrate RHD screening in children with more comprehensive cardiologicalsurveillance, with the result that other cardiac conditions including congenital heart disease were also detectedand referred for management. (168) A comparative study in the Haryana state of northern India contrasted RHDcase detection and management in a rural region that introduced an RHD control program with that in an adjacentarea without a control program. (169) They found that case detection in the region with the control programincreased approximately 8-fold, while remaining relatively unchanged in the comparator region. Compliance withsecondary prophylaxis in the RHD control program region was maintained at 85% to 95%. The authors concludedthat their experience documented how a management-based control program could be successfully implementedin a less developed country, using existing infrastructure and at low cost.
Secondary prophylaxis programs require the availability of high-quality BPG. In recent times, there have beenproblems with both the availability and quality of BPG around the world. In many countries, this medication is inshort supply, and often has been unavailable for prolonged periods (Personal communication, E. Kaplan). Evenmore concerningly, the quality of the medication is highly variable – there are a number of studies documentingthat different batches may have variable pharmacokinetic properties, and the batches may vary physically (e.g.some are very difficult to draw up into a syringe and administer). (170-173) It is clear that many forms of benzathinepenicillin G presently used around the world do not reliably lead to adequate serum penicillin levels after 28 days,as was found in the original studies of this regimen. (133 )
In summary, the overall messages of the Global Programme review – that coordinated RHD control programs canbe successfully implemented, and can improve adherence to secondary prophylaxis, reduce ARF recurrencerates, improve clinical care of RHD patients, and be acceptable to the population - are supported in part by moredetailed evaluations of individual programs. A major problem has been the inability in many countries to scale upfrom pilot programs to regional or national programs. The countries where this has occurred – particularly NewZealand and India – have relied on adequate funding and the enthusiasm of core local staff. The critical questionsof the impact of these programs on RHD prevalence and mortality are less clearly defined and will require longerterm, targeted evaluations.
Diagnosis of ARFEffective secondary prophylaxis programs rely on accurate identification of people with a history of ARF or RHD.The diagnosis of ARF can be difficult, especially in tropical developing countries where many patients haveatypical presentations and there is a long list of differential diagnoses (e.g. arboviral infections may present withfever and arthritis or arthralgia, which is the most common presenting syndrome of ARF). The Jones Criteria havebeen repeatedly revised and updated, each time increasing the specificity at the expense of sensitivity.(174-176)This was largely in response to the rapidly declining incidence of ARF in the United States,(177, 178) and wasappropriate for settings where ARF has become increasingly uncommon. However, in populations where theincidence of ARF is high, the importance of missed diagnoses of ARF (i.e. missed opportunities for secondaryprevention, with consequent ARF recurrences and worsening of RHD) may outweigh that of over-diagnosis (i.e.
20
GROUP A STREPTOCOCCUS
subjecting some individuals to secondary prophylaxis when it is not needed). Therefore, it has been argued thatsome of the current minor manifestations in the Jones criteria – particularly arthralgia and mono-arthritis – shouldbe treated as major manifestations in populations with high ARF incidence.(43, 179-181) The use ofechocardiography in the diagnosis of rheumatic carditis has also been the subject of extensive discussion. Thearguments and relevant references are summarised in the proceedings of the most recent meeting of the AmericanHeart Association’s Jones Criteria Working Group.(182) Similary, the use of streptococcal serology in the diagnosisof a recent GAS infection is notoriously unreliable in populations with highly endemic streptococcal infections,particularly pyoderma. This issue has been discussed several times at WHO meetings,(31, 32, 183) but as yet abetter test has not emerged. The Jones Criteria Working Group decided not to change the 1992 updated Jonescriteria, arguing that there were insufficient data to justify either a relaxing of the major manifestations or theaddition of echocardiographic diagnosis of carditis. The Group also recommended that clinical research in theseareas was needed, and it is clear that this research should particularly come from regions of high ARF incidence,where research findings will have the greatest implications on clinical and public health practice.
MEDICAL AND SURGICAL MANAGEMENT OF RHD PATIENTSTreatment of patients with moderate or severe cardiac valve lesions due to RHD may prolong and/or save lives. Inrecent times, valvotomy and valve repair, rather than valve replacement, have emerged as the standard of carefor RHD valve lesions that require surgery. These approaches avoid the complications associated with long-termanticoagulation in populations where adherence to treatment and monitoring regimens may be difficult. Theirmajor disadvantage is that valve lesions may recur with time, and further surgery may be needed. (184-190)
Although there has been great progress in medical and surgical treatment of RHD, these approaches remain veryexpensive and, in the case of surgery, require the availability of sophisticated facilities and highly trained personnel.Therefore, these treatments are beyond the reach of most RHD patients, who are usually among the poorestpeople living in less developed countries. Some examples of the expense of providing treatment for RHD areoutlined below in the discussion of cost-effectiveness of different control strategies. To further illustrate the dramaticcosts involved, each year Samoa sends 25 to 40 RHD patients to New Zealand for valve surgery at a cost of overUS $680,000 (which equates to $4 per capita for the entire Samoan population of approximately 170,000) (PersonalCommunication, S Viali June 2003). The per-capita Gross National Product of Samoa is approximately US $1,500per year, and the per-capita expenditure on health is approximately US $34 per year. (191) Therefore, RHD valvesurgery consumes approximately 12% of the Samoan health budget, yet Samoa does not have an effectivelyfunctioning secondary prophylaxis program. Similar situations are reported from other Pacific island nations.Over the past 10 years, 81 cardiac surgical procedures have been performed for RHD in Vanuatu, at a cost ofmany hundreds of thousands of dollars, and many more patients have died without surgery.(Personalcommunication, Dr R Wells and Dr M McDonald). In Tonga, 50% of all patients seen during cardiology consultationshave RHD, of whom 44% are aged <20yrs, and 40% need surgery at an average cost of US $30,000 (Personalcommunication, Dr T Fakakovi). Neither of these countries have effective secondary prophylaxis programs inplace.
There is little sense in advocating a public health strategy that concentrates on providing expensive palliativecare for a condition that is preventable using relatively cheap interventions (e.g. secondary prophylaxis). Therefore,although it is clearly important to provide good clinical care to RHD patients, it would be a mistake to directsubstantial resources to this strategy at the expense of a well-resourced secondary prophylaxis program.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
21
COST-EFFECTIVENESS OF DIFFERENT PREVENTION STRATEGIES
Many authors have argued the cost-effectiveness of different prevention strategies. All models used relating toprimary prophylaxis are sensitive to the underlying assumptions about the proportion of sore throats that are dueto GAS, the proportion of GAS episodes that lead to ARF, and the outcome of individual cases of ARF. Regardlessof which model is used, the assumptions are heavily weighted towards simple, low-cost methods of preventingthe development of RHD, in order to prevent the less common, but very expensive, medical and surgical interventionsnecessary to treat RHD. For example, a follow-up study from Brazil found that 17% of over 1,000 RHD patientsaged <16 years required cardiac surgery over an 8-year period, at a cost per patient of US $8,000 to $10,000.(192) In New Zealand, RHD cost the Auckland Area Health Board $3.6 million in 1987, of which approximately$2.7 million was for treatment of RHD. (193) Aside from the direct costs of medical and surgical management ofpatients, the socio-economic costs can be dramatic. In Brazil, 100 consecutive RHD patients who had at least oneyear of follow-up were studied. (194) The mean duration of disease in the study was 3.9 years. During this period,the 100 patients had a total of 1657 medical consultations and 22 hospital admissions (including four to theintensive care unit). Parents missed 901 days of work and 5% of parents lost their jobs. Twenty-two percent ofpatients failed school. The authors calculated that RHD costs Brazil over US $51 million each year, which representsapproximately 1.3% of annual family income.
The costs of primary prevention programs based around coordinated surveillance, case detection and treatmentof sore-throats have already been discussed in this report. It has been estimated that 2,000 cases of pharyngitiswould have to be treated to avert one case of RHD. (161) A series of analyses in the USA during the 1970s cameto varying conclusions, although all agreed that all people with sore throat should be treated during epidemics.(195-197) A consensus view from the USA was that endemic pharyngitis should be treated only after amicrobiological diagnosis has been made, with the exception of patients at high risk of rheumatic fever or followingscarlet fever. (161) A Nigerian study estimated that 2.25% of all untreated GAS pharyngitis patients would developRHD, based on the assumptions that 3% of GAS pharyngitis episodes lead to ARF and 75% of ARF episodes intropical less developed countries lead to RHD. Both of these assumptions are likely to be overestimates. Thesame study concluded that providing antibiotic treatment to 10,000 children with GAS pharyngitis would prevent225 cases of RHD, and that the cost of this (based on penicillin alone) was 5.4 times less than the cost of caringfor 225 RHD patients for one year. (198) Regardless of the assumptions, it is clear that any primary prophylaxisstrategy either must include microbiological diagnosis of GAS pharyngitis (which is impractical in most lessdeveloped countries), or be willing to accept that most courses of antibiotics to treat sore throat will not preventARF.
By contrast, secondary prophylaxis has almost universally been found to be very cost effective. This is notsurprising, given that the intervention (monthly BPG injections) is cheap, that a high-risk group is targeted, andthat prevention of recurrent ARF is known to prevent worsening of RHD and associated mortality. In 1970, anearlier version of the WHO Global Programme in 7 countries was evaluated, with the conclusion that the cost of theprogram was US $325 per month (including associated register costs, etc) whereas the cost of maintainingpaediatric beds for RHD patients was $1,260 per month. (199) A WHO pilot study concluded that only 3.14injections of BPG were needed to prevent one day of admission to hospital, that there were many other incidentalbenefits to secondary prophylaxis-based control programs, and that secondary prophylaxis is very cost effective.(161) In New Zealand, the average cost per patient treated (in USD) was $10,749 for valve replacement or repair,$2,230 for an ARF admission, $2,757 for a non-surgical RHD admission, and $439 for a year of secondary
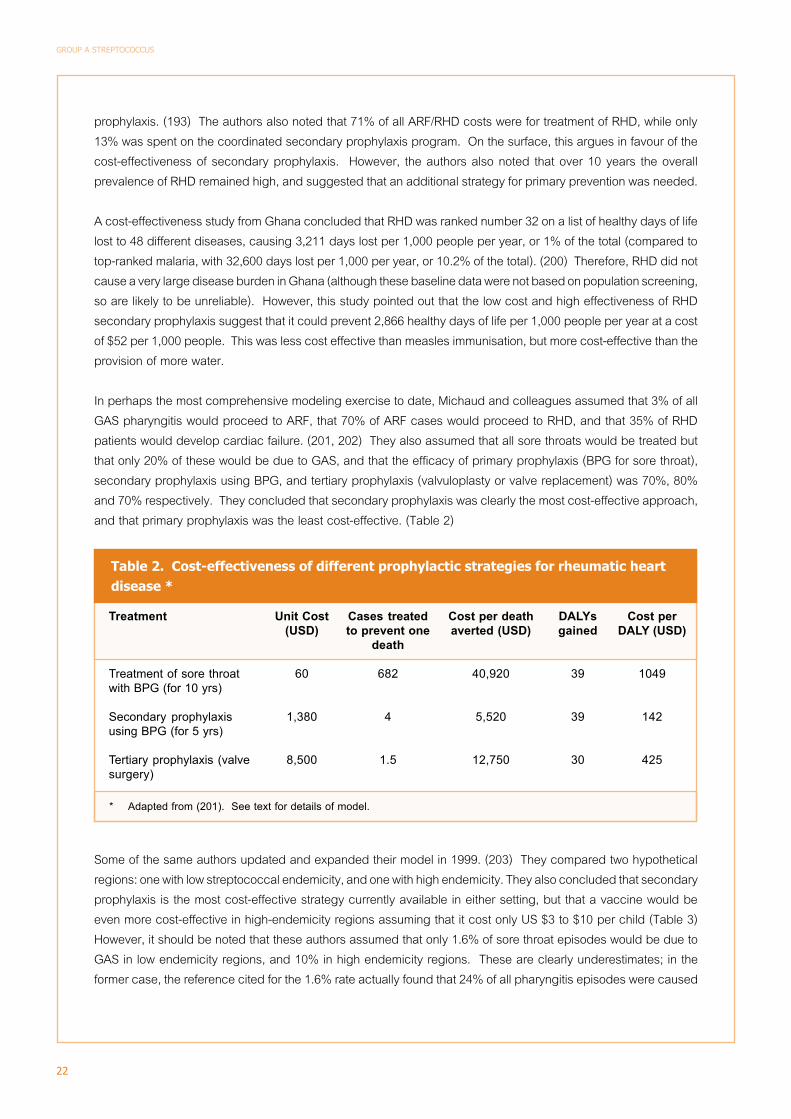
22
GROUP A STREPTOCOCCUS
prophylaxis. (193) The authors also noted that 71% of all ARF/RHD costs were for treatment of RHD, while only13% was spent on the coordinated secondary prophylaxis program. On the surface, this argues in favour of thecost-effectiveness of secondary prophylaxis. However, the authors also noted that over 10 years the overallprevalence of RHD remained high, and suggested that an additional strategy for primary prevention was needed.
A cost-effectiveness study from Ghana concluded that RHD was ranked number 32 on a list of healthy days of lifelost to 48 different diseases, causing 3,211 days lost per 1,000 people per year, or 1% of the total (compared totop-ranked malaria, with 32,600 days lost per 1,000 per year, or 10.2% of the total). (200) Therefore, RHD did notcause a very large disease burden in Ghana (although these baseline data were not based on population screening,so are likely to be unreliable). However, this study pointed out that the low cost and high effectiveness of RHDsecondary prophylaxis suggest that it could prevent 2,866 healthy days of life per 1,000 people per year at a costof $52 per 1,000 people. This was less cost effective than measles immunisation, but more cost-effective than theprovision of more water.
In perhaps the most comprehensive modeling exercise to date, Michaud and colleagues assumed that 3% of allGAS pharyngitis would proceed to ARF, that 70% of ARF cases would proceed to RHD, and that 35% of RHDpatients would develop cardiac failure. (201, 202) They also assumed that all sore throats would be treated butthat only 20% of these would be due to GAS, and that the efficacy of primary prophylaxis (BPG for sore throat),secondary prophylaxis using BPG, and tertiary prophylaxis (valvuloplasty or valve replacement) was 70%, 80%and 70% respectively. They concluded that secondary prophylaxis was clearly the most cost-effective approach,and that primary prophylaxis was the least cost-effective. (Table 2)
Some of the same authors updated and expanded their model in 1999. (203) They compared two hypotheticalregions: one with low streptococcal endemicity, and one with high endemicity. They also concluded that secondaryprophylaxis is the most cost-effective strategy currently available in either setting, but that a vaccine would beeven more cost-effective in high-endemicity regions assuming that it cost only US $3 to $10 per child (Table 3)However, it should be noted that these authors assumed that only 1.6% of sore throat episodes would be due toGAS in low endemicity regions, and 10% in high endemicity regions. These are clearly underestimates; in theformer case, the reference cited for the 1.6% rate actually found that 24% of all pharyngitis episodes were caused
Treatment
Treatment of sore throatwith BPG (for 10 yrs)
Secondary prophylaxisusing BPG (for 5 yrs)
Tertiary prophylaxis (valvesurgery)
Unit Cost(USD)
60
1,380
8,500
Cost per deathaverted (USD)
40,920
5,520
12,750
Table 2. Cost-effectiveness of different prophylactic strategies for rheumatic heartdisease *
DALYsgained
39
39
30
Cases treatedto prevent one
death
682
4
1.5
* Adapted from (201). See text for details of model.
Cost perDALY (USD)
1049
142
425

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
23
by GAS. (204) As a result this model is flawed. However, the correction figure is equally applicable to all parts ofthe model, so the relative cost-effectiveness of different strategies may not be dramatically affected.
Intervention
Vaccine (@$3-10)
Primary prophylaxis of pharyngitis
Secondary prophylaxis
Surgery
High endemicity region
137 – 458
22,075 – 33,113
999 – 1,123
1,861
Table 3. Cost per RHD DALY averted in high and low endemicity regions *
Low endemicity region
5,3330 – 17,765
68,346 – 102,520
982 – 1,103
1,861
* Adapted from (203)
Cost per DALY averted (USD)

24
GROUP A STREPTOCOCCUS
Conclusions
Secondary prophylaxis delivered to ARF/RHD patients is the only control strategy for GAS diseases that has beenshown to be both effective and cost-effective at the community / population level. In populations with high prevalenceof RHD, delivery of secondary prophylaxis should be the major priority for control of GAS diseases. Coordinatedregister-based RHD control programs appear to be the most effective method for delivering secondary prophylaxisand have the added benefit of improving clinical follow-up of patients and providing a mechanism for delivery oftargeted health promotional messages. Past efforts to expand RHD control programs have had mixed success.Future strategies should concentrate on ensuring that programs are properly resourced, not overly ambitious intheir early stages, and are systematically evaluated. Further, the issue of the availability and quality of BPGsupplies requires urgent attention. The diagnosis of ARF remains difficult in many countries, and the AmericanHeart Association’s Jones Criteria Working Group has called for more clinical research in this area. It is clear thatthis research should particularly be focused in developing countries and other populations with high ARF incidence.
Because it deals with the provision of expensive palliative care to patients with preventable disease, tertiaryprevention of RHD should theoretically be the least important and therefore least resourced aspect of GAS control.Unfortunately, in many countries this strategy has become the focus of RHD control and consumes the majority ofthe RHD control budget (and a substantial proportion of the entire health budget). While the importance oftreating patients in cardiac failure from RHD cannot be ignored, the cost-effectiveness of improving adherence tosecondary prophylaxis – and thus reducing the number of RHD patients requiring surgical and medical treatment– clearly argues in favour of secondary rather than tertiary prevention.
There is currently no strategy for primary prevention of GAS diseases that has a proven cost-effective benefit atthe population level. A vaccine that protects against ARF, APSGN, invasive GAS disease and skin infection couldhave a major impact if able to be supplied to less developed countries. Such a vaccine is not likely to be availablein the foreseeable future (although efforts to develop one should be supported).
Primary prevention by reducing exposure to GAS has been extremely effective in reducing the incidence of GASdiseases in more developed countries over the past century, but there are very few interventions in this categorythat do not accompany economic development. Therefore, such an approach cannot be part of a coherentcontrol strategy for less developed countries in the short to medium term.
Of the remaining primary prevention interventions, primary prophylaxis of ARF has been the most intensivelystudied, advocated and practised. There are clinical issues that require further research in this area, particularlythe development of better clinical algorithms for the diagnosis of GAS pharyngitis. However, the available evidencesuggests that, even when implemented at an optimal level (a level that is neither practical nor affordable for mostless developed countries), primary prophylaxis can prevent only a minority of cases of ARF. The efficacy of large-scale primary prophylaxis programs in reducing transmission of GAS and incidence of GAS pharyngitis has beendemonstrated, although this strategy is unlikely to be cost-effective. The impact of this approach on invasive GASdisease and APSGN is not known. Although some middle-income countries may choose to implement surveillance-based primary prophylaxis programs on a large scale for the prevention of ARF, this strategy cannot berecommended for poorer countries, where the major burden of ARF exists.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
25
Community-based approaches for controlling scabies have had demonstrated success in reducing the prevalenceand severity of GAS skin infections. It is possible that mass administration of ivermectin for filariasis in manycountries may have had an important secondary benefit by reducing scabies and skin infections; this is notknown, but could be relatively easily determined. There is the potential for other strategies addressing personaland community hygiene (including swimming pools), insect bites, and targeted antibiotic treatment to be addedto scabies programs to further reduce rates of skin infections; this has not been properly studied. The control ofGAS skin infections and the likely effect of preventing APSGN and invasive disease is sufficient argument tosupport the widespread implementation of healthy skin programs in communities with high rates of scabies andpyoderma. The possibility that these programs may have the added benefits of preventing ARF and improvingother aspects of child health is further impetus for their implementation and for a detailed evaluation of their healthimpact. This strategy has the potential to be the most effective and practical approach for primary prevention ofGAS diseases in less developed countries.
Mass antibiotic treatment remains a valid strategy for prevention and control of outbreaks of GAS diseases inparticular situations. These include the prevention of ARF in military institutions and control of focal APSGNoutbreaks. Targeted antibiotic treatment – e.g. to family contacts of cases of invasive GAS disease – requiresfurther study.
The most successful GAS control activities have combined multiple strategies including primary prophylaxis,treatment of skin infections, health promotion, secondary prophylaxis and RHD registers. Although effective,these comprehensive programs require a substantial commitment from individuals and organisations (includingMinistries of Health).
26
GROUP A STREPTOCOCCUS
Priority Issues
1. Secondary prophylaxis of RHD should be supported as the most important control strategy for countries withhigh rates of ARF and RHD. A coordinated strategy is needed to audit the extent and penetration of existingcontrol programs, improve awareness and training in practical strategies for establishing and evaluating controlprograms, expand model programs, ensure the availability of quality supplies of BPG, and develop simplemodels for countries to calculate the cost-effectiveness of secondary prophylaxis in their setting.
2. In populations where high rates of scabies-associated pyoderma exist, community-based scabies controlprograms should be advocated.
3. The results and costs of recent large-scale primary prophylaxis programs based on school-based surveillanceof sore throat should be disseminated so that countries can make informed decisions about such strategies
4. Primary prophylaxis should continue to be advocated for individual patients presenting to clinics with sorethroat where facilities exist to offer treatment. To that end, better clinical algorithms are required for the diagnosisof GAS pharyngitis that have been evaluated at the level of community clinics in less developed countries
5. The effectiveness of programs to reduce the prevalence and severity of skin infections on a wide range of GASdiseases and other health outcomes should be properly evaluated, and compared with existing sore-throatbased strategies.
6. Clinical research is needed to improve the clinical diagnosis and simplify treatment of GAS pharyngitis, and toimprove the diagnostic criteria for ARF in high-incidence populations. This research should logically takeplace in high-incidence populations.
7. There is an urgent need for oversight and coordination of GAS vaccine development, to ensure that a vaccinebecomes available that is safe, affordable and of demonstrated efficacy against the most important GASdiseases in less developed countries.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
27
APPENDIX 1The possible link between GAS skin infections and
acute rheumatic fever
Note: This appendix has been adapted from a draft chapter for the PhD thesis of Dr Malcolm McDonald(working under the supervision of the author of this report) with his permission.
It is widely believed that ARF invariably follows GAS infection of the upper respiratory tract, but never follows skininfection. (205, 206) However, it is well known that many populations living in tropical climates, where ARF andRHD are major problems, have low rates of GAS throat carriage. The best example is in the Aboriginal populationof Australia, where the incidence of ARF is the highest reported in the world yet GAS is rarely isolated from theupper respiratory tract and GAS pharyngitis is apparently uncommon, yet GAS skin infections are rampant. (33,207) Such information is difficult to reconcile with a conviction that only GAS throat infection may lead to ARF, andjustifies a re-evaluation of the evidence underlying this dogma.
The established story: that GAS throat infection alone causes acute rheumatic feverThere is no doubt that ARF may follow GAS upper respiratory infection or scarlet fever. (208-212) Adequateantibiotic treatment of documented streptococcal pharyngitis reduces the incidence of subsequent ARF. (9, 213,214) However, this does not negate the possibility that skin infections may also cause ARF.
There is some evidence against a skin-ARF link from outbreak studies. In Native American children, outbreaks ofskin infections were associated with APSGN but not ARF. (215) In Trinidad, ‘nephritogenic’ strains were absentfrom patients with ARF, a history of recent sore throat preceded 50% of 93 cases of ARF (vs 8% of patients withAPSGN – P <0.001 ) and a history of recent skin infection preceded 92% of 195 cases of APSGN (vs 28% with ARF– P <0.001). (87)
The seasonal separation between ARF and APSGN is also often cited as evidence. In Tennessee there was asummer-autumn peak of pyoderma accompanied by a peak incidence of APSGN. (216) The peak incidence ofpharyngitis was two months later and coincided with the peak of ARF, although there was a second and unexplainedsmaller peak of ARF in early spring. Further evidence comes from serological studies, thanks to the fact that theASO titre is strongly associated with throat infection and less so with skin infection, whereas anti-DNase B (ADB)titres respond to both throat and skin infection. (217) Most patients with ARF have elevated antibody titres tostreptolysin O (ASO), whether or not they recall an antecedent sore throat. (218) Moreover, there is a relationshipbetween the magnitude of the ASO rise and the ARF attack rate. (219) The ASO titre was subsequently adoptedas the preferred serological indicator for ARF.
The concept of separate throat and skin strains, and that pyoderma strains can cause APSGN but not ARF, datesto the 1960s. (205, 216, 220) ‘Rheumatogenic’ strains were observed to have abundant M-protein and the colonieshad a ‘mucoid’ appearance on blood agar plates linked with greater expression of the hyaluronic acid capsule.(221) Specific M-types were also associated with throat infection and ARF, whereas ‘skin’ strains had different M-types or could not be typed using available sera. (86, 87, 222, 223). GAS species can be differentiated into two

28
GROUP A STREPTOCOCCUS
antigenic groups (I and II) on the basis of an M-associated protein, and these groups correlate with known ‘skin’and ‘throat’ strains. (224) ‘Skin’ strains of GAS possess a lipoproteinase known as serum opacity factor (SOF orSfbII), whereas known ‘rheumatogenic’ M-types are predominantly SOF-negative, although SOF-positive GASstrains may be recovered from throats of some children. (225-227) A further differentiation of strains based ondifferences within the conserved C repeat region of the M protein resulted in the identification of Class I strains,correlating with SOF-negative strains and containing serotypes associated with outbreaks of ARF, and Class IIstrains which are associated with skin tropism. (228, 229) Patients with ARF were shown to mount a strongantibody response to Class I-specific epitopes, but not epitopes specific to Class II. (230) Further studiesdemonstrated that the arrangement of emm and emm-like genes allowed GAS isolates to be categorised in fivepatterns, A through E. Patterns A-C were associated with throat infections and ARF, pattern D with skin infectionsand pattern E with infections at either site. (231)
Epidemiological evidence for strain differences also came from studies done in Trinidad where both impetigo andrheumatic fever were common; both M-typing and T-typing were used to show that strains colonizing the skinwere not associated with ARF. (87)
In explanation of the host response, it has been suggested that because the pharynx has a large repository oflymphoid tissue, it may be important in the initiation of the abnormal humoral response by the host to thoseantigens cross-reactive with target organs. Pyoderma strains do colonize the pharynx; however, they do notappear to elicit as strong an immunologic response as the pharyngeal strains. (217, 232)
Lastly, despite a wealth of published material linking GAS throat infection to ARF, there is a dearth of cases ofclearly documented ARF following skin infection. One well-documented case appeared in the literature a quarterof a century ago, but there it ends. (233)
Evidence that challenges the established storyHigh prevalences of GAS skin infection and low throat carriage rates of GAS have been found in many resource-poor countries and indigenous communities, (33, 87, 234, 235) and a possible relationship between GAS skininfection and ARF/RHD in the tropics was raised more than 25 years ago (87). However, most studies have beenlimited by lack of prospectively collected surveillance data and modern laboratory tools to better define theepidemiology.
The epidemiology of GAS and other beta-haemolytic streptococci in non-urban Aboriginal communities in Australianow seems to be distinct from that described in the US, Europe and other temperate climate settings. Classic‘rheumatogenic’ M-serotypes of GAS are not to be found despite the rates of ARF/RHD. (236, 237) Moreover,most local strains cannot be M protein typed using available antisera. (237, 238). Modern molecular techniqueshave provided the key to understanding the epidemiology in more detail. One study of emm-patterns of GASisolates from a remote Aboriginal community with a high incidence of ARF/RHD showed that skin-trophic strains ofGAS (emm patterns D and E) were predominant and the relationships were quite different to that found in temperateregions. (239) For example, although patterns A-C were most common in the throat, 70% of the ‘throat’ strains(emm patterns A-C) came from skin sores. There was relatively poor differentiation between strains that infectedthe skin and those found in the throat; in this setting, skin lesions appeared to be the principle tissue reservoir forall GAS strains, irrespective of emm pattern. In northern Thailand, six of thirteen previously undescribed emmtypes of GAS were isolated from both the skin and the throat of impetigo and pharyngitis/ARF patients, and in
A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
29
many cases the authors could not differentiate skin strains or throat strains that could be associated with ARF oracute glomerulonephritis. (240)
Lack of seasonal variation of ARF and APSGN has not been found in many high-incidence countries where it hasbeen studied; examples include Kuwait, Trinidad, Ethiopia and Chile. (87, 241-244) In the New Zealand Maoripopulation, peaks of ARF and APSGN both occur in the autumn and coincide with peak rates for GAS skininfection. (245). Thus, the argument of seasonal variation may not necessarily apply where the risk of disease ishighest.
According to the serological evidence, children with ARF should all have elevated ASO titres with or withoutelevated ADB titres. Yet, in a large study of Aboriginal children with unequivocal ARF, 55 had elevated ADB butnormal ASO titres. REF Either the ASO titre is an unreliable indicator of throat infection or GAS infection at anothersite, such as skin, preceded a significant number of cases. There are a number of possible reasons for a lack ofASO titre rise in some cases of ARF, including maturity of the immune response and the effect of early treatment,and that Groups C and G streptococci also produce streptolysin O which may be a confusing factor. (246) Lackof uniform ASO response in children with ARF has been noted elsewhere, including Kuwait, South India, Trinidad,Nigeria and ‘underprivileged, black inner-city children’ of Miami-Dade County. (247-252) Likewise, in Brazil, daSilva and others documented a lack of significant ASO response in a third of 786 confirmed cases of ARF seen inseven paediatric rheumatology clinics in the state of Sao Paulo. (253)
Despite the lack of published episodes of ARF following skin infection, the case published by Popat and Ridingwas well documented and followed skin infection with a common pyoderma serotype. (233, 254) Thus it canhappen. Proving that it occurs more frequently, especially in a tropical setting, is difficult. In temperate climates,where overall GAS infection is less common and diagnostic facilities are available, a patient with GAS pharyngitisis much more likely to be identified clinically and the infection then confirmed with appropriate investigations.Whereas, in an environment where GAS infection is common and children may have multiple infections withmultiple strains, a case of ARF cannot be easily attributed to any particular GAS infection or strain, especiallywhen it can only be done in hindsight.
There is also the intriguing possibility that Group G and/or Group C beta-haemolytic streptococci may play role inthe pathogenesis of ARF. The rate of throat carriage of Group C (GCS) and Group G (GGS) streptococci is higher(15-20%) in Northern Territory Aboriginal populations than GAS. (57, 255) This finding has also been documentedin other tropical and sub-tropical settings. (256-258) Both organisms can cause pharyngitis, post-infectiouspolyarthritis and invasive disease; GCS can cause APSGN. (259-263) Human strains of GGS & GCS have Mprotein and share other virulence factors with GAS. (261, 264-268) Cross-reactivity has been demonstratedbetween GCS & GGS M protein and cardiac myosin. (255) Furthermore, there is clear evidence of habitual genetransfer between strains of GAS and GCS & GGS. (269-272) The role of GCS & GGS in the pathogenesis of ARF/RHD, if any, remains undefined and deserves further investigation.
The traditional story regarding the pathogenesis of ARF/RHD is now being questioned in Australia, the Pacificisland nations and beyond. (33, 245, 273, 274) In populations with high rates of both pyoderma and ARF, there isa growing body of circumstantial evidence that skin infection may be implicated and there are several possiblemechanisms. It could be fairly straightforward with GAS infection of the skin directly leading to ARF; alternativelystrains from pyoderma lesions could first infect the throat and then cause ARF. Another possibility is that ofimmune ‘priming’. Beta-haemolytic streptococcal infections (GAS and others) promote type-specific and non-

30
GROUP A STREPTOCOCCUS
type specific immune responses in the host. They are both humoral and cellular in nature, in part genetically-determined and apparently exaggerated in ‘susceptible’ people. (275, 276) It has been clearly established thatrepeated exposure to streptococcal infections plays a central role in the development of ARF (277, 278) andconstant antigenic challenge from either the skin or the throat seems to ‘prime’ the immune response bothquantitatively and qualitatively. Thus, in high incidence settings, it may be recurrent streptococcal pyoderma thatsets the stage for a ‘rheumatogenic’ strain, either in the throat or on the skin, to cause ARF.
Should it be found that streptococcal pyoderma does have a pathogenic role, it is still probable that the risk ofdeveloping ARF after an episode of pharyngitis is much greater than that following pyoderma. Nevertheless, inpopulations with a high incidence of skin infection and low incidence of streptococcal pharyngitis, the number ofcases of ARF resulting from pyoderma could still represent a substantial proportion the total number of casesseen each year.(33)

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
31
References
1. Last JM, Abramson JH, Friedman GD, Porta M, Spasoff RA, Thuriaux M. A dictionary of epidemiology, 3rdedition. New York: Oxford University Press, 1995.
2. Levine JI, Chapman SS, Guerra V, Cooper J, Krause RM. Studies on the transmission within families ofgroup A hemolytic streptococci. J Lab Clin Med 1966;67:483-494.
3. Musher DM. How contagious are common respiratory tract infections? N Engl J Med 2003;348:1256-66.4. Wedum AG, Wedum BG. Rheumatic fever in Cincinnati in relation to rentals, crowding, density of population
and negroes. Am J Public Health 1944;34:1065-70.5. Coburn AF, Young DC. The epidemiology of hemolytic streptococcus during World War II in the United
States Navy. Baltimore: Williams and Wilkins, 1949.6. Gastanaduy AS, Kaplan EL, Huwe BB, McKay C, Wannamaker LW. Failure of penicillin to eradicate group
A streptococci during an outbreak of pharyngitis. Lancet 1980;2:498-502.7. Dagan R, Ferne M, Sheinis M, Alkan M, Katzenelson E. An epidemic of penicillin-tolerant group A
streptococcal pharyngitis in children living in a closed community: mass treatment with erythromycin.Journal of Infectious Diseases 1987;156:514-6.
8. Rammelkamp C.H. J. Epidemiology of streptococcal infections. Harvey Lect 1955;51:113-142.9. Denny FW, Wannamaker LW, Brink WR, Rammelkamp CH, Custer EA. Prevention of rheumatic fever:
treatment of the preceding streptococcic infection. JAMA 1950;143:151-153.10. Catanzaro FJ, Rammelkamp CH, Chamovitz R. Prevention of rheumatic fever by treatment of streptococcal
infections 2: factors responsible for failures. N Engl J Med 1958;259:51-57.11. Dillon HC, Wannamaker LW. Skin infections and acute glomerulonephritis: report of a symposium. Military
Medicine 1971;136:122-127.12. White AV, Hoy WE, McCredie DA. Childhood post-streptococcal glomerulonephritis as a risk factor for
chronic renal disease in later life. Med.J.Aust. 2001;174:492-496.13. Kaplan E. Benzathine penicillin G for treatment of group A streptococcal pharyngitis a reappraisal in 1985.
Pediatr Infect Dis J 1985;4:592-596.14. Kaplan EL, Johnson DR. Unexplained reduced microbiological efficacy of intramuscular benzathine penicillin
G and of oral penicillin V in eradication of group a streptococci from children with acute pharyngitis.Pediatrics 2001;108:1180-6.
15. Dajani A, Taubert K, Ferrieri P, Peter G, Shulman S. Treatment of acute streptococcal pharyngitis andprevention of rheumatic fever: a statement for health professionals. Committee on Rheumatic Fever,Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, the AmericanHeart Association. Pediatrics 1995;96:758-64.
16. Bisno AL, Gerber MA, Gwaltney JM, Jr., Kaplan EL, Schwartz RH. Practice guidelines for the diagnosis andmanagement of group A streptococcal pharyngitis. Infectious Diseases Society of America. Clin Infect Dis2002;35:113-25.
32
GROUP A STREPTOCOCCUS
17. Shvartzman P, Tabenkin H, Rosentzwaig A, Dolginov F. Treatment of streptococcal pharyngitis withamoxycillin once a day. Bmj 1993;306:1170-2.
18. Feder HM, Jr., Gerber MA, Randolph MF, Stelmach PS, Kaplan EL. Once-daily therapy for streptococcalpharyngitis with amoxicillin. Pediatrics 1999;103:47-51.
19. World Health Organization. Acute respiratory infections in children: case management in small hospitals indeveloping countries. A manual for doctors and other senior health workersq. Geneva: World HealthOrganization, 1991.
20. World Health Organization. The WHO Global Programme for the Prevention of Rheumatic Fever andRheumatic Heart Disease: Report of a consultation to review progress and develop future activities. Geneva,29 November - 1 December 1999. Geneva: World Health Organization, 2000:1-49.
21. Breese BB. A simple scorecard for the tentative diagnosis of streptococcal pharyngitis. Am J Dis Child1977;131:514-7.
22. Walsh BT, Bookheim WW, Johnson RC, Tompkins RK. Recognition of streptococcal pharyngitis in adults.Arch Intern Med 1975;135:1493-7.
23. Centor RM, Witherspoon JM, Dalton HP, Brody CE, Link K. The diagnosis of strep throat in adults in theemergency room. Med Decis Making 1981;1:239-46.
24. Steinhoff MC, Abd el Khalek MK, Khallaf N, et al. Effectiveness of clinical guidelines for the presumptivetreatment of streptococcal pharyngitis in Egyptian children. Lancet 1997;350:918-21.
25. McIsaac WJ, White D, Tannenbaum D, Low DE. A clinical score to reduce unnecessary antibiotic use inpatients with sore throat. Cmaj 1998;158:75-83.
26. Wald ER, Green MD, Schwartz B, Barbadora K. A streptococcal score card revisited. Pediatr Emerg Care1998;14:109-11.
27. Attia MW, Zaoutis T, Klein JD, Meier FA. Performance of a predictive model for streptococcal pharyngitis inchildren. Arch Pediatr Adolesc Med 2001;155:687-91.
28. Danchin MH, Curtis N, Nolan TM, Carapetis JR. Treatment of sore throat in light of the Cochrane verdict: isthe jury still out? Med J Aust 2002;177:512-5.
29. Kaplan EL. Clinical guidelines for group A streptococcal throat infections. Lancet 1997;350:899-900.30. USAID / WHO / JHSPH GRASP / TOPS study operations manual. Baltimore: Johns Hopkins School of
Public Health, 2001:1-65.31. World Health Organization. Meeting on the WHO Programme of Streptococcal Diseases Complex for 1986-
1987 and on the Evaluation of the Non-Culture Rapid Group A Streptococcus Test, Geneva, 3-4 February1986 report. Geneva: World Health Organization, 1986.
32. World Health Organization. Meeting on the evaluation and development of WHO programmes to combatstreptococcal diseases and meningococcal infections, Geneva, 10-13 October 1988. WHO/MIM/STREP/CSM/89.2. Geneva: World Health Organization, 1989.
33. Carapetis JR, Currie BJ, Kaplan EL. The epidemiology and prevention of group A streptococcal infections:acute respiratory tract infections, skin infections and their sequelae at the close of the 20th century. ClinInfect Dis 1999;28:205-11.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
33
34. Anonymous. Strategy for controlling rheumatic fever/ rheumatic heart disease, with emphasis on primaryprevention: memorandum from a joint WHO/ISFC meeting. Bull World Health Organ 1995;73:583-587.
35. Poses RM, Cebul RD, Collins M, Frager SS. The accuracy of experienced physicians’ probability estimatesfor patients with sore throats: implications for decision making. JAMA 1985;254:925-9.
36. Komaroff Al, T.M. P, M.D. A. The prediction of streptococcal pharyngitis in adults. J Gen Intern Med 1986;1:1-7.37. Anonymous. Acute sore throat. In: Paterson B, ed. Children’s Standard Treatment Manual. Darwin: Northern
Territory Government, 1995:167.38. Del Mar CB, Glasziou PP, Spinks AB. Antibiotics for sore throat. Cochrane.Database.Syst.Rev.
2000:CD000023.39. Anonymous. Management of sore throat and indications for tonsillectomy. A national clinical guideline.
Scottish Intercollegiate Guidelines network, Scottish Cancer Therapy Network. Edinburgh, 1999.40. Royal College of Paediatrics and Child Health. Management of Acute and Recurring Sore Throat and
Indications for Tonsillectomy: RCPCH,Guidelines for Good Practice,London, 2000.41. Berrios X, del Campo E, Wilson C, Blasquez J, Morales A, Quesney F. Acute rheumatic fever in the
southeastern metropolitan area of Santiago, Chile, 1976-1981. Bull Pan Am Health Organ 1984;18:389-96.42. Veasy LG, Tani LY, Hill HR. Persistence of acute rheumatic fever in the intermountain area of the United
States. J.Pediatr. 1994;124:9-16.43. Carapetis JR, Currie BJ. Rheumatic fever in a high incidence population: the importance of monoarthritis
and low grade fever. Arch Dis Child 2001;85:223-227.44. Bunn WH, Bennett HN. Community control of rheumatic fever. JAMA 1955;157:986-989.45. Phibbs B, Becker D, Lowe CR, et al. The Casper Project - an enforced mass-culture streptococcic control
program. JAMA 1958;166:1113-1119.46. Zimmerman RA, Biggs BA, Bolin RA, et al. An effective program for reducing group A streptococcal
prevalence. Pediatrics 1971;48:566-572.47. Phibbs B, Taylor J, Zimmerman RA. A community-wide streptococcal control project. JAMA 1970;214:2018-2024.48. Jackson H. Streptococcal control in grade schools. Amer J Dis Child 1976;130:273-279.49. Houser HB, Schmidt WC, Daugherty SC. The epidemiologic characteristics of a metropolitan community
streptococcal culture program. In: Haverkorn MJ, ed. Streptococcal disease and the community:proceedings of the Fifth International Symposium on Streptococcus Pyogenes, Amsterdam, 27 August-1September, 1972. Amsterdam: Excerpta Medica, 1974:181-188.
50. Coulehan JL, Baacke G, Welty T, Goldtooth NL. Cost-benefit of a streptococcal surveillance programamong Navajo Indians. Publ Health Rep 1982;97:73-77.
51. Brant LJ, Bender TR, Bross DS. Evaluation of an Alaskan streptococcal control program: importance of theprogram’s intensity and duration. Preventive Med 1986;15:632-642.
52. Chun LT, Reddy V, Rhoads GG. Occurrence and prevention of rheumatic fever among ethnic groups ofHawaii. Am J Dis Child 1984;138:476-8.

34
GROUP A STREPTOCOCCUS
53. Neilson G, Streatfield RW, West M, Johnson S, Glavin W, Baird S. Rheumatic fever and chronic rheumaticheart disease in Yarrabah aboriginal community, north Queensland. Establishment of a prophylacticprogram. Med.J.Aust. 1993;158:316-318.
54. Hanna J, O’Rourke S. Rheumatic fever and chronic rheumatic heart disease in Yarrabah aboriginalcommunity, north Queensland. Med.J.Aust. 1993;158:793.
55. Lennon DR. The decline of acute rheumatic fever (ARF): unrelated to sore throat management? 42ndInterscience Conference on Antimicrobial Agents and Chemotherapy. San Diego: American Society forMicrobiology, 2002:Abstract G-1481.
56. Taplin D, Porcelain SL, Meinking TL, et al. Community control of scabies: a model based on use of permethrincream. Lancet 1991;337:1016-1018.
57. Carapetis JR, Connors C, Yarmirr D, Krause V, Currie BJ. Success of a scabies control program in anAustralian aboriginal community. Pediatr.Infect.Dis.J. 1997;16:494-499.
58. Wong LC, Amega B, Connors C, et al. Outcome of an interventional program for scabies in an Indigenouscommunity. Med.J.Aust. 2001;175:367-370.
59. Lawrence G, Leafasia J, Sheridan J, et al. Community control of scabies with ivermectin and permethrinwas followed by reductions in skin sores, streptococcal finger contamination and haematuria in SolomonIslands children. Brisbane, 2003.
60. Bockarie MJ, Alexander ND, Kazura JW, Bockarie F, Griffin L, Alpers MP. Treatment with ivermectin reducesthe high prevalence of scabies in a village in Papua New Guinea. Acta Trop 2000;75:127-30.
61. Curtis, Kanki, Cousens, et al. Evidence of behavioural change following a hygiene promotion programmein Burkina Faso. 2001.
62. Taplin D, Lansdell L, Allen AM, Rodriguez R, Cortes A. Prevalence of streptococcal pyoderma in relation toclimate and hygiene. Lancet 1973;1:501-3.
63. Ferrieri P, Dajani AS, Wannamaker LW, Chapman SS. Natural history of impetigo I: Site sequence ofacquisition and familial patterns of spread of cutaneous streptococci. J Clin Invest 1972;51:2851-2862.
64. Masawe AEJ, Nsanzumuhire H, Mhalu FS. Bacterial skin infections in preschool and school children incoastal Tanzania. Arch Dermatol 1975;111:1312-1316.
65. Sharrett AR, Finklea JF, Potter EV, Poon-King T, Earle DP. The control of streptococcal skin infections inSouth Trinidad. Am J Epidemiol 1974;99:408-413.
66. Burnett JW. Management of pyogenic cutaneous infections. N Engl J Med 1962;266:164-169.67. Dillon HC, Jr. The treatment of streptococcal skin infections. J Pediatr 1970;76:676-684.68. Blum D, Feachem RG. Measuring the impact of water supply and sanitation investments on diarrhoeal
diseases: problems of methodology. Int J Epidemiol 1983;12:357-365.69. Porter MJ. An epidemiological approach to skin disease in the tropics. Tropical Doctor 1977;7:59-66.70. Bailey R, Downes B, Downes R, Mabey D. Trachoma and water use; a case control study in a Gambian
village. Trans.R.Soc.Trop.Med.Hyg. 1991;85:824-828.71. Ryder RW, Reeves WC, Singh N, et al. The childhood health effects of an improved water supply system in
a remote Panamanian island. Am J Trop Med Hyg 1985;34:921-924.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
35
72. Nelson KE, Bisno AL, Brunt J, Moses VK, Haque RU. The epidemiology and natural history of streptococcalpyoderma: an endemic disease of the rural southern United States. Am J Epidemiol 1976;103:270-283.
73. Gibbs S. Skin disease and socioeconomic conditions in rural Africa: Tanzania. Int J Dermatol 1996;35:633-639.74. Carapetis JR, Johnston F, Nadjamerrek J, Kairupan J. Skin sores in Aboriginal children. J.Paediatr.Child
Health 1995;31:563.75. Lehmann D, Silva D, Tennant M, Stanley F. Impact of introduction of swimming pools on health of Aboriginal
children and adolescents living in remote areas of Western Australia. Perth: Telethon Institute for ChildHealth Research, 2002:1-9.
76. Harris M, Nako D, Hopkins T, et al. Skin infections in Tanna, Vanuatu in 1989. P.N.G.Med.J. 1992;35:137-143.77. Lines DR. An Auckland high school health survey. Aust NZ J Med 1977;7:143-147.78. Mahe A, Prual A, Konate M, Bobin P. Skin diseases of children in Mali: a public health problem.
Trans.R.Soc.Trop.Med.Hyg. 1995;89:467-470.79. Porter MJ. Seasonal change and its effect on the prevalence of infectious skin disease in a Gambian
village. Trans R Soc Trop Med Hyg 1979;74:162-168.80. Eason RJ, Tasman-Jones T. Resurgent yaws and other skin diseases in the Western Province of the Solomon
Islands. P N G Med J 1985;28:247-250.81. Belcher DW, Afoakwa SN, Osei-Tutu E, Wurapa FK, Osei L. Endemic pyoderma in Ghana: a survey in rural
villages. Trans R Soc Trop Med Hyg 1977;71:204-209.82. Dillon HC, Jr. Impetigo contagiosa: suppurative and non-suppurative complications 1: clinical, bacteriologic,
and epidmiologic characteristics of impetigo. Amer J Dis Child 1968;115:530-541.83. Dillon HC, Jr. Streptococcal skin infection and acute glomerulonephritis. Postgrad Med J 1970;46:641-652.84. Kristensen JK. Scabies and Pyoderma in Lilongwe, Malawi. Prevalence and seasonal fluctuation.
Int.J.Dermatol. 1991;30:699-702.85. Rogers M, Dorman DC, Gapes M, Ly J. A three-year study of impetigo in Sydney. Med J Aust 1987;147:63-65.86. Anthony BF, Kaplan EL, Wannamaker LW, Chapman SS. The dynamics of streptococcal infections in a
defined population of children: serotypes associated with skin and respiratory infections. Am J Epidemiol1976;104:652-666.
87. Potter EV, Svartman M, Mohammed I, Cox R, Poon-King T, Earle DP. Tropical acute rheumatic fever andassociated streptococal infections compared with concurrent acute glomerulonephritis. J Pediatr1978;92:325-333.
88. Kleinman H. Epidemic acute glomerulonephritis at Red Lake. Minnesota Medicine 1954;37:479-489.89. Poon-King T, Potter EV, Achong J, et al. The epidemiology of acute poststreptococcal nephritis in South
Trinidad. In: Haverkorn MJ, ed. Streptococcal disease and the community. Amsterdam: Excerpta Medica,1974:293-300.
90. Svartman M, Potter EV, Finklea JF, Poon-King T, Earle DP. Epidemic scabies and acute glomerulonephritisin Trinidad. Lancet 1972;1:249-251.
91. Margolis HS, Lum MKW, Bender TR, Elliot SL, Fitzgerald MA, Harpster AP. Acute glomerulonephritis ansstreptococcal skin lesions in Eskimo children. Am J Dis Child 1980;134:681-685.

36
GROUP A STREPTOCOCCUS
92. Rodriguez-Iturbe B. Epidemic poststreptococcal glomerulonephritis. Kidney Int 1984;25:129-36.93. Berrios X. [Epidemic outbreak of acute post streptococcal glomerulonephritis]. Rev.Chil.Pediatr.
1990;61:109-112.94. Carapetis J. An outbreak of acute post-streptococcal glomerulonephritis in an Aboriginal community. NT
Commun Dis Bull 1994;2:1-4.95. Evans C. Acute Post Streptococcal Glomerulonephritis in the Northern Territory 1980 - 2000. Northern
Territory Disease Control Bulletin 2001;8:1-6.96. Kearns T, Evans C, Krause V. Outbreak of acute post-streptococcal glomerulonephritis in the Northern
Territory - 2001. NT Disease Control Bulletin 2001;8:6-14.97. Streeton CL, Hanna JN, Messer RD, Merianos A. An epidemic of acute post-streptococcal glomerulonephritis
among aboriginal children. J.Paediatr.Child Health 1995;31:245-248.98. Nema S, Chitnis DS. Antibiogram study over bacterial isolates from cases of bacteraemias. Indian Journal
of Medical Sciences 1996;50:325-9.99. Hossain MM, Karthikeyan G. Neonatal sepsis: Staphylococcus aureus as the predominant pathogen. Indian
Journal of Pediatrics 2002;69:15-8.100. Duke T, Michael A, Mgone J, Frank D, Wal T, Sehuko R. Etiology of child mortality in Goroka, Papua New
Guinea: a prospective two-year study. Bull.World Health Organ 2002;80:16-25.101. Skull SA, Krause V, Coombs G, Pearman JW, Roberts LA. Investigation of a cluster of Staphylococcus
aureus invasive infection in the top end of the Northern Territory. Aust.N.Z.J.Med. 1999;29:66-72.102. Carapetis JR, Walker AM, Hibble M, Sriprakash KS, Currie BJ. Clinical and epidemiological features of
group A streptococcal bacteraemia in a region with hyperendemic superficial streptococcal infection.Epidemiol.Infect. 1999;122:59-65.
103. Saeed AA. Utilization of primary health services in Port Sudan, Sudan. Trop Geogr Med 1984;36:267-272.104. Thomas DP, Heller RF, Hunt JM. Clinical consultations in an aboriginal community-controlled health service:
a comparison with general practice. Malnutrition and microcephaly in Australian aboriginal children.Australian & New Zealand Journal of Public Health 1998;22:86-91.
105. Heggie AD. Prevention of Streptococcal pharyngitis and acute rheumatic fever in Navy and Marine Corpsrecruits. Navy Med 1988;79:26-8.
106. Frank PF, Stollerman GH, Miller LF. Protection of a military population from rheumatic fever. Routineadministration of benzathine penicillin G to healthy individuals. JAMA 1965;193:775-783.
107. Brundage JF, Gunzenhauser JD, Longfield JN, et al. Epidemiology and control of acute respiratory diseaseswith emphasis on group A beta-hemolytic streptococcus: a decade of U.S. Army experience. Pediatrics1996;97:964-70.
108. Gunzenhauser JD, Longfield JN, Brundage JF, Kaplan EL, Miller RN, Brandt CA. Epidemic streptococcaldisease among Army trainees, July 1989 through June 1991. J Infect Dis 1995;172:124-31.
109. Ferrieri P, Dajani AS, Wannamaker LW. A controlled study of penicillin prophylaxis against streptoccalimpetigo. J Infect Dis 1974;129:429-438.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
37
110. Streeton CL, Hanna JN, Messer RD. An epidemic of acute poststreptococcal glomerulonephritis amongAboriginal children in Far North Queensland. Proceedings of RACP Annual Scientific Meeting, Gold Coast(Abstract) 1995.
111. Johnston F, Carapetis J, Patel MS, Wallace T, Spillane P. Evaluating the use of penicillin to control outbreaksof acute poststreptococcal glomerulonephritis. Pediatr.Infect.Dis.J. 1999;18:327-332.
112. Davies HD, McGeer A, Schwartz B, et al. Invasive group A streptococcal infections in Ontario, Canada.N.Engl.J.Med. 1996;335:547-554.
113. McGeer A, Ontario Group A Streptococcal Study Group. Recommendations for investigation andchemoprophylaxis related to invasive GAS cases, including necrotizing fasciitis and streptococcal toxicshock syndrome, 2003.
114. Ontario Ministry of Health. Guidelines for the management of contacts of cases of invasive group Astreptococcal disease (GAS) including streptococcal toxic shock syndrome (STSS) and necrotizing fasciitis.Ottawa: Government of Canada, 1995.
115. Prevention of Invasive Group ASIWP. Prevention of invasive group A streptococcal disease among householdcontacts of case patients and among postpartum and postsurgical patients: recommendations from theCenters for Disease Control and Prevention.[erratum appears in Clin Infect Dis. 2003 Jan 15;36(2):243.].Clinical Infectious Diseases 2002;35:950-9.
116. Robinson KA, Rothrock G, Phan Q, et al. Risk for severe group A streptococcal disease among patients’household contacts. Emerging Infectious Diseases 2003;9:443-7.
117. Recco RA, Zaman MM, Cortes H, Colucci J, Poomkudy G, Kaplan EL. Intra-familial transmission of life-threatening group A streptococcal infection. Epidemiology & Infection 2002;129:303-6.
118. Schwartz B, anonymous. Nosocomial group A streptococcal infections associated with asymptomatic health-care workers—Maryland and California, 1997. Advances in Pediatric Infectious Diseases 1999;14:129-45.
119. Cockerill FR, 3rd. An outbreak of invasive group A streptococcal disease associated with high carriagerates of the invasive clone among school-aged children.[comment]. Pediatrics 1998;101:136-40.
120. McGeer A, Schwartz B, Green K, Cann D, Simor AE, Low DE. Clusters of invasive group A streptococcal infectionsin family, hospital, and nursing home settings. New England Journal of Medicine 1996;335:547-54.
121. Elliott JA, Butler JC, Simon PA, et al. Streptococcus pyogenes outbreak in a long-term care facility. ClinicalInfectious Diseases 1992;15:277-84.
122. Gordis L. Effectiveness of comprehensive care programs in preventing rheumatic fever. N Engl J Med1973;289:331-335.
123. Gordis L. The virtual disappearance of rheumatic fever in the United States: lessons in the rise and fall ofdisease. Circulation 1985;72:1155-1162.
124. Bach JF, Chalons S, Forier E, et al. 10-year educational programme aimed at rheumatic fever in two FrenchCaribbean islands. Lancet 1996;347:644-648.
125. Pan American Health Organization. Health Statistics from the Americas 1991 Edition. Mortality since 1960.Scientific publication number 537. Washington DC: PAHO, 1991.

38
GROUP A STREPTOCOCCUS
126. Gulliford MC. Epidemiological transition in Trinidad and Tobago, West Indies 1953-1992. Int J Epidemiol1996;25:357-365.
127. Nordet PE. Fiebre reumatica. Magnitud y aspectos - clinicos epidemiologicos. Provincia ciudad de laHabana Cuba, 1972-87. Ministerio de Salud Publica, Instituto de Cardiologia y Cirugia Cardiovascular,Ciudad de Habana, Cuba. Havana, 1988.
128. Lopez R. RF/RHD. Comprehensive programme for prevention. Pinar de Rio, Cuba, 1986-1996 (primaryand secondary prevention). Pinar del Rio: University of Cuba, 2000.
129. Guzman SV, Cabral EJ, Parazo MA, et al. Prevention of cardiovascular diseases through integration in theschool curriculum: the development of the program. Asian Heart Journal 1994;2:4-10.
130. Coburn AF, Moore LV. The prophylacitic use of sulfanilamide in streptococcal respiratory infections withespecial reference to rheumatic fever. J Clin Invest 1939;18:147-155.
131. Thomas CB, France R. A prelimary report of the prophylactic use of sulfanilamide in patients susceptible torheumatic fever. Bull Johns Hopkins Hosp 1939;64:67-77.
132. Stollerman GH. The use of antibiotics for the prevention of rheumatic fever. Am J Med 1954;17:757-767.133. Stollerman GH, Rusoff JH. Prophylaxis against group A streptococcal infections in rheumatic fever patients:
use of a new repository penicillin preparation. N Engl J Med 1952;150:1571-1575.134. Feinstein AR, Spagnuolo M, Jonas S, Kloth H, Tursky A, Levitt M. Prophylaxis of recurrent rheumatic fever
- therapeutic continuous oral penicillin vs monthly injections. JAMA 1968;206:565-568.135. Stollerman GH, Rusoff JH, Hirschfeld I. Prophylaxis against group A streptococci in rheumatic fever. The
use of single monthly injections of benzathine penicillin G. N Engl J Med 1955;252:787-792.136. Markowitz M, Ferencz C, Bonet A. A comparison of oral and intramuscular benzathine penicillin G for the
prevention of streptococcal infections and recurrences of rheumatic fever. Pediatrics 1957;19:201-207.137. Wood HF, Feinstein AR, Taranta A, Epstein JA, Simpson R. Rheumatic fever in children and adolescents.
A long-term epidemiological study of subsequent prophylaxis, streptococcal infections, and clinicalsequelae. III. Comparative effectiveness of three prophylaxis regimens in preventing streptococcal infectionsand rheumatic recurrences. Ann Intern Med 1964;60 (Suppl 5):31-46.
138. Lennon D. Rheumatic fever, a preventable disease? The New Zealand experience. In: Martin DR, Tagg JR,eds. Streptococci and streptococcal diseases: entering the new millenium. Porirua: ESR, 2000:503-512.
139. Frankish JD. Rheumatic fever prophylaxis: Gisborne experience. N Z Med J 1984;97:674-5.140. Anonymous. Community control of rheumatic heart disease in developing countries: 2. Strategies for
prevention and control. WHO Chron. 1980;34:389-395.141. Anonymous. Rheumatic fever and rheumatic heart disease - report of a WHO study group. World Health
Organization Technical Report Series (764). Geneva: World Health Organization, 1988.142. Bland EF, Jones TD. Rheumatic fever and rheumatic heart disease. Circulation 1951;4:836-843.143. Tompkins DG, Boxerbaum B, Liebman J. Long-term prognosis of rheumatic fever patients receiving regular
intramuscular benzathine penicillin. Circulation 1972;45:543-551.144. Rheumatic Fever Working Party. The natural history of rheumatic fever and rheumatic heart disease: ten-
year report of a cooperative clinical trial of ACTH, cortisone, and aspirin. Circulation 1965;32:457-476.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
39
145. Feinstein AR, Stern EK, Spagnuolo M. The prognosis of acute rheumatic fever. Am Heart J 1964;68:817-834.146. Majeed HA, Batnager S, Yousof AM, Khuffash F, Yusuf AR. Acute rheumatic fever and the evolution of
rheumatic heart disease: a prospective 12 year follow-up report. J.Clin.Epidemiol. 1992;45:871-875.147. Sanyal SK, Berry AM, Duggal S, Hooja V, Ghosh S. Sequelae of the initial attack of acute rheumatic fever in
children from North India. Circulation 1982;65:375-379.148. Lue HC, Tseng WP, Lin GJ, Hsieh KH, Hsieh RP, Chiou JF. Clinical and epidemiological features of rheumatic
fever and rheumatic heart disease in Taiwan and the Far East. Indian Heart J 1983;35:139-46.149. Carapetis JR, Currie BJ. Clinical epidemiology of rheumatic fever and rheumatic heart disease in tropical
Australia. Adv.Exp.Med.Biol. 1997;418:233-236.150. Brown A, Purton L, Schaeffer G, Wheaton G, White A, Central Australian RHD Steering Committee. Central
Australian rheumatic heart disease control program: a report to the Commonwealth November 2002. NorthernTerritory Disease Control Bulletin 2003;10:1-8.
151. Fadahunsi HO, Coker AO, Usoro PD. Rheumatic heart disease in Nigerian children: clinical and preventiveaspects. Ann Trop Paediatr 1987;7:54-8.
152. Lutalo SK, Mabonga N. Experience on follow-up of registered rheumatic fever patients in the ZimbabweanMidlands. Trop Geogr Med 1986;38:277-82.
153. Aziz K, Memon AD, Rehman M, Haque A. Rheumatic fever and carditis at the National Institute of Cardio-Vascular Diseases—a follow up study. J Pak Med Assoc 1986;36:196-203.
154. World Health Organization. Rheumatic fever and rheumatic heart disease: report of a WHO study group[meeting held in Geneva from 30 March to 4 April 1987]. Geneva: World Health Organization, 1988.
155. World Health Organization. Prevention and control of rheumatic fever and rheumatic heart diseases: South-East Asia Regional plan. New Delhi: WHO Regional Office for South-East Asia, 1984.
156. Pan American Health Organization. Prevention and control of rheumatic fever in the community: manual ofoperational standards for a program to extend coverage at different levels of care. Washington, D.C: PanAmerican Health Organization, 1985.
157. WHO global programme for the prevention of rheumatic fever / rheumatic heart disease in sixteen developingcountries (AGFUND supported). Meeting of National Programme Managers, Geneva: 4-6 November 1986,1986:1-41.
158. World Health Organization. WHO Global Programme for the prevention of rheumatic fever / rheumaticheart disease in sixteen developing countries (AGFUND supported). Meeting of national programmemanagers, Geneva: 4-6 November 1986. Geneva: World Health Organization, 1987:1-16.
159. WHO Cardiovascular Diseases Unit and principal investigators. WHO programme for the prevention andcontrol of rheumatic fever/rheumatic heart disease in 16 developing countries: report from Phase I (1986-90). Bull World Health Organ 1992;70:213-218.
160. Strasser T, Dondog N, El Kholy A, et al. The community control of rheumatic fever and rheumatic heartdisease: report of a WHO international cooperative project. Bull.World Health Organ 1981;59:285-294.
161. Strasser T. Cost-effective control of rheumatic fever in the community. Health Policy 1985;5:159-64.162. Kelly A. Top End rheumatic heart disease program. A report to the Commonwealth: February - November
2002 (abbreviated). Northern Territory Disease Control Bulletin 2003;10:9-11.

40
GROUP A STREPTOCOCCUS
163. Flight RJ. The Northland rheumatic fever register. N Z Med J 1984;97:671-3.164. Talbot RG. Rheumatic fever and rheumatic heart disease in the Hamilton Health district II: long- term
follow-up and secondary prophylaxis. N Z Med J 1984;97:634-637.165. Thornley C, McNicholas A, Baker M. Rheumatic fever registers in New Zealand. In: Martin DR, Tagg JR,
eds. Streptococci and streptococcal diseases entering the new millenium. Porirua: ESR, 2000:541-543.166. Kumar R, Thakur JS, Aggarwal A, Ganguly NK. Compliance of secondary prophylaxis for controlling rheumatic
fever and rheumatic heart disease in a rural area of northern India. Indian Heart J. 1997;49:282-288.167. Kumar R, Raizada A, Aggarwal AK, Ganguly NK. A community-based rheumatic fever/rheumatic heart
disease cohort: twelve-year experience. Indian Heart J. 2002;54:54-58.168. Thakur JS, Negi PC, Ahluwalia SK, Sharma R. Integrated community-based screening for cardiovascular
diseases of childhood. World Health Forum 1997;18:24-27.169. Iyengar SD, Grover A, Kumar R, Ganguly NK, Anand IS, Wahi PL. A rheumatic fever and rheumatic heart
disease control programme in a rural community of north India. Natl Med J India 1991;4:268-271.170. Bass JW, Longfield JN, Jones RG, Hartmann RM. Serum levels of penicillin in basic trainees in the U.S.
Army who received intramuscular penicillin G benzathine. Clin Infect Dis 1996;22:727-728.171. Kassem AS, Madkour AA, Massoud BZ, Zaher SR. Benzathine penicillin G for rheumatic fever prophylaxis:
2-weekly versus 4-weekly regimens. Indian J.Pediatr. 1992;59:741-748.172. Kaplan EL, Berrios X, Speth J, Siefferman T, Guzman B, Quesny F. Pharmacokinetics of benzathine penicillin G:
serum levels during the 28 days after intramuscular injection of 1,200,000 units. J Pediatr 1989;115:146-150.173. Zaher SR, Kassem AS, Abou-Shleib H, El-Kholy AG, Madkour AA, Kaplan EL. Differences in serum penicillin
concentrations following intramuscular injection of benzathine penicillin G (BPG) from differentmanufacturers. J Pharm Med 1992;2:17-23.
174. American Heart Association. JONES CRITERIA (modified) for guidance in the diagnosis of rheumatic fever;report of the Committee on Standards and Criteria for programs of care. Circulation 1956;13:617-20.
175. Committee on rheumatic fever and bacterial endocarditis of the American Heart Association. Jones criteria(revised) for guidance in the diagnosis of rheumatic fever. Circulation 1984;69:03A-208A.
176. American Heart Association. Guidelines for the diagnosis of acute rheumatic fever: Jones criteria, 1992update. JAMA 1992;268:2069-2073.
177. Shiffman RN. Guideline maintenance and revision. 50 years of the Jones criteria for diagnosis of rheumaticfever. Arch Pediatr Adolesc Med 1995;149:727-32.
178. Markowitz M, Gerber MA. The Jones criteria for guidance in the diagnosis of rheumatic fever. Anotherperspective. Arch Pediatr Adolesc Med 1995;149:725-6.
179. Cherian G. Acute rheumatic fever—the Jones criteria: a review and a case for polyarthralgia. J AssocPhysicians India 1979;27:453-7.
180. Markowitz M. Evolution and critique of changes in the Jones criteria for the diagnosis of rheumatic fever. NZ Med J 1988;101:392-4.
181. Padmavati S, Gupta V. Reappraisal of the Jones criteria: the Indian experience. N Z Med J 1988;101:391-2.
A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
41
182. Ferrieri P. Proceedings of the Jones Criteria workshop. Circulation 2002;106:2521-3.183. World Health Organization. WHO meeting on streptococcal diseases complex, Geneva 15-18 November,
1983, 1983:1-42.184. Gometza B, Balasundaram S, al Halees Z, Duran CM. Valve repair in rheumatic mitral disease. European
Heart Journal 1991;12 Suppl B:34-8.185. Ribeiro PA, Dunn B, Galal O, et al. The problems of valve surgery in a developing country. American Heart
Journal 1992;123:462-5.186. Gometza B, al Halees Z, Duran C, Fawzy ME. Percutaneous mitral valvotomy with the Inoue balloon catheter in
children and adults: immediate results and early follow-up. Journal of Cardiovascular Surgery 1992;33:7-13.187. Duran CM, Gometza B, Saad E. Valve repair in rheumatic mitral disease: an unsolved problem. Journal of
Cardiac Surgery 1994;9:282-5.188. Enriquez-Sarano M, Schaff HV, Orszulak TA, Tajik AJ, Bailey KR, Frye RL. Valve repair improves the outcome
of surgery for mitral regurgitation. A multivariate analysis. Circulation 1995;15:1022-1028.189. Bailey KR, Seward JB, Tajik AJ, Krohn MJ, Mays JM, Skoularigis J. Evaluation of the long-term results of
mitral valve repair in 254 young patients with rheumatic mitral regurgitation. Circulation 1993;87:841-8.190. Carapetis JR, Powers JR, Currie BJ, et al. Outcomes of cardiac valve replacement for rheumatic heart
disease in Aboriginal Australians. Asia Pacific Heart J 1999;8:138-147.191. Anonymous. Annual Report of the Samoan Ministry of Health, 1996-1997. Apia: Government of Samoa, 1997.192. Snitcowsky R. Rheumatic fever prevention in industrializing countries: problems and approaches. Pediatrics
1996;97:996-998.193. North DA, Heynes RA, Lennon DR, Neutze J. Analysis of costs of acute rheumatic fever and rheumatic
heart disease in Auckland. N Z Med J 1993;106:400-403.194. Terreri MT, Ferraz MB, Goldenberg J, Len C, Hilario MO. Resource utilization and cost of rheumatic fever.
Journal of Rheumatology 2001;28:1394-7.195. Tompkins RK, Burnes DC, Cable WE. An analysis of the cost-effectiveness of pharyngitis management and
acute rheumatic fever prevention. Ann Intern Med. 1977;86:481-492.196. Pantell RH. Cost-effectiveness of pharyngitis management and prevention of rheumatic fever. Ann Intern
Med 1977;86:497-9.197. Bisno AL. Therapeutic strategies for the prevention of rheumatic fever. Ann Intern Med 1977;86:494-6.198. Jaiyesimi F. Chronic rheumatic heart disease in childhood: its cost and economic implications. Tropical
Cardiology 1982;8:55-59.199. Hassell TA, Stuart KL. Rheumatic fever prophylaxis: a three-year study. BMJ 1974;2:39-40.200. Dodu, Organization WH. Cost-effectiveness of RF/RHD prevention. Geneva: World Health Organization, 1987.201. Michaud C, Trejo-Gutierrez J, Cruz C, Pearson TA. Rheumatic heart disease. In: Jamison DT, Mosley WH,
Measham AR, Bobadilla JL, eds. Disease control priorities in developing countries. Oxford: Oxford UniversityPress, 1993:221-232.

42
GROUP A STREPTOCOCCUS
202. Michaud C, Gutierrez JT, Cruz C, Pearson TA. The World Bank health sector priorities review: rheumaticheart disease. Washington, D.C.: World Bank, 1991:1-31.
203. Michaud C, Rammohan R, Narula J. Cost-effectiveness analysis of intervention strategies for reduction ofthe burden of rheumatic heart disease. In: Narula J, Virmani R, Reddy KS, Tandon R, eds. Rheumatic fever.Washington, D.C.: American Registry of Pathology, 1999:485-497.
204. Majeed HA, Al-Doussary L, Moussa MM, Yusuf AR, Suliman AH. Office diagnosis and management ofgroup A streptococcal pharyngitis employing the rapid antigen detecting test. A 1-year prospective studyof reliability and cost in primary care centres. Ann Trop Pediatr 1993;13:65-72.
205. Wannamaker LW. Differences between streptococcal infections of the throat and of the skin. (Second oftwo parts). N Engl J Med 1970;282:78-85.
206. Stollerman GH. Rheumatic fever in the 21st century. Clin.Infect.Dis. 2001;33:806-814.207. Carapetis JR, Currie BJ, Mathews JD. Cumulative incidence of rheumatic fever in an endemic region: a
guide to the susceptibility of the population? Epidemiol.Infect. 2000;124:239-244.208. Schlesinger B. The relationship of throat infection to acute rheumatism in childhood. Arch Dis Child
1930;5:411-430.209. Glover JA. Incidence of rheumatic diseases. Lancet 1930;1:499-505.210. Collis WRF. Acute rheumatism and haemolytic streptococci. Lancet 1931:1341-1345.211. Sheldon W. On acute rheumatism following tonsillitis. Lancet 1931:1337-1341.212. Massell BF, Amezcua F, Pelargonio S. Evolving picture of rheumatic fever: data from 40 years at the House
of the Good Samaritan. JAMA 1964;188:287-294.213. Chamovitz R, Catanzaro FJ, Stetson CA, Rammelkamp CH. Prevention of rheumatic fever by treatment of
previous streptococcal infections 1:evaluation of benzathine penicillin G. N Engl J Med 1954;251:466-471.214. Brock LL, Siegel AC. Studies on the prevention of rheumatic fever: the effect of time of initiation of treatment
of streptococcal infections on the immune response of the host. J Clin Invest 1953;32:630-632.215. Anthony BF, Perlman LV, Wannamaker LW. Skin infections and acute nephritis in American Indian children.
Pediatrics 1967;39:263-279.216. Bisno AL, Pearce IA, Wall HP, Moody MD, Stollerman GH. Contrasting epidemiology of acute rheumatic
fever and acute glomerulonephritis. New England Journal of Medicine 1970;283:561-5.217. Kaplan EL, Anthony BF, Chapman SS, Ayoub EM, Wannamaker LW. The influence of site of infection on the
immune response to group A streptococci. J Clin Invest 1970;49:1405-1414.218. Stollerman GH, Lewis AJ, Schultz I, Taranta A. The relationship of the immune response to group A
streptococci to the course of acute, chronic and recurrent rheumatic fever. Am J Med 1956:163-169.219. Stollerman GH. Factors that predispose to rheumatic fever. Med Clin North Am 1960;44:17-28.220. Wannamaker LW. Differences between streptococcal infections of the throat and of the skin. (First of two
parts). N Engl J Med 1970;282:23-31.221. Stollerman GH. The relative rheumatogenicity of strains of group A streptococci. Modern Concepts of
Cardiovascular Disease 1975;44:35-40.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
43
222. Dillon HC, Jr, Reeves MSA. Streptococcal immune responses in nephritis after skin infection. Am J Med1974;56:333-345.
223. Colman G, Tanna A, Efstratiou A, Gaworzewska ET. The serotypes of Streptococcus pyogenes present inBritain during 1980-1990 and their association with disease. J.Med.Microbiol. 1993;39:165-178.
224. Widdowson JP, Maxted WR, Pinney AM. An M-associated protein antigen (MAP) of group A streptococci.J Hyg (Lond) 1971;69:553-64.
225. Maxted WR, Widdowson JP, Fraser CA, Ball LC, Bassett DC. The use of the serum opacity reaction in thetyping of group-A streptococci. J Med Microbiol 1973;6:83-90.
226. Rakonjac JV, Robbins JC, Fischetti VA. DNA sequence of the serum opacity factor of group A streptococci:identification of a fibronectin-binding repeat domain. Infect Immun 1995;63:622-31.
227. Molina AM, Coratza G, Musmanno RA, Figura N, Rossolini GM. Production of serum-opacity factor byStreptococcus pyogenes strains isolated from pharyngitis in children. Prevalence of “rheumatogenic” Mtypes among OF-negative strains. Eur J Epidemiol 1985;1:37-41.
228. Bessen DE, Fischetti VA. Differentiation between two biologically distinct classes of group A streptococciby limited substitutions of amino acids within the shared region of M protein-like molecules. J Exper Med1990;172:1757-1764.
229. Bessen DE, Jones KF, Fischetti VA. Evidence for two distinct classes of streptococcal M protein and theirrelationship to rheumatic fever. J Exp Med 1989;169:269-283.
230. Bessen DE, Veasy LG, Hill HR, Augustine NH, Fischetti VA. Serologic evidence for a Class 1 group Astreptococcal infection among rheumatic fever patients. J Infect Dis 1995;172:1608-1611.
231. Bessen DE, Sotir CM, Readdy TL, Hollingshead SK. Genetic correlates of throat and skin isolates of groupA streptococci. J Infect Dis 1996;173:896-900.
232. Bisno AL, Ofek I. Serologic diagnosis of streptococcal infection. Comparison of a rapid hemagglutinationtechnique with conventional antibody tests. Am J Dis Child 1974;127:676-81.
233. Popat KD, Riding WD. Acute rheumatic fever following streptococcal wound infection. Postgrad Med J1976;52:165-170.
234. Steer AC, Adams J, Carlin J, Nolan T, Shann F. Rheumatic heart disease in school children in Samoa.Arch.Dis.Child 1999;81:372.
235. Wiest LG. Problems of tropical dermatology in Ethiopia. Int J Dermatol 1977;16:506-511.236. Bisno AL. The concept of rheumatogenic and nonrheumatogenic group A streptococci. Streptococcal
diseases and the immune response 1980:789-803.237. Martin D, Sriprakash KS. Epidemiology of group A streptococcal disease in Australia and New Zealand. In: Asche
V, ed. Recent Advances in Microbiology. Melbourne: Australian Society for Microbiology, 1997:1-40.238. Hartas J, Goodfellow AM, Currie BJ, Sriprakash KS. Characterisation of group A streptococcal isolates
from tropical Australia with high prevalence of rheumatic fever: probing for signature sequences to identifymembers of the family of serotype 5. Microb.Pathog. 1995;18:345-354.
239. Bessen DE, Carapetis JR, Beall B, et al. Contrasting molecular epidemiology of group A streptococcicausing tropical and nontropical infections of the skin and throat. J Infect Dis 2000;182:1109-16.

44
GROUP A STREPTOCOCCUS
240. Pruksakorn S, Sittisombut N, Phornphutkul C, Pruksachatkunakorn C, Good MF, Brandt E. Epidemiologicalanalysis of non-M-typeable group A Streptococcus isolates from a Thai population in northern Thailand. JClin Microbiol 2000;38:1250-4.
241. Berrios X, Quesney F, Morales A, Blazquez J, Lagomarsino E, Bisno AL. Acute rheumatic fever andpoststreptococcal glomerulonephritis in an open population: comparative studies of epidemiology andbacteriology. J Lab Clin Med 1986;108:535-542.
242. Carapetis JR. PhD Thesis: Ending the heartache: the epidemiology and control of acute rheumatic feverand rheumatic heart disease in the Top End of the Northern Territory. Sydney: University of Sydney, 1998.
243. Majeed HA, Khuffash FA, Yousof AM, et al. The rheumatogenic and nephritogenic strains of the group Astreptococcus: the Kuwait experience. N Z Med J 1988;101:398-401.
244. Tewodros W, Muhe L, Daniel E, Schalen C, Kronvall G. A one-year study of streptococcal infections andtheir complications among Ethiopian children. Epidemiol.Infect. 1992;109:211-225.
245. Martin DR, Voss LM, Walker SJ, Lennon D. Acute rheumatic fever in Auckland, New Zealand: spectrum ofassociated group A streptococci different from expected. Pediatr.Infect.Dis.J. 1994;13:264-269.
246. Wannamaker LW, Ayoub EM. Antibody titers in acute rheumatic fever. Circulation 1960;21:598-614.247. Majeed HA, Khuffash FA, Sharda DC, Farwana SS, El-Sherbiny AF, Ghafour SY. Children with acute rheumatic
fever and acute poststreptococcal glomerulonephritis and their families in a subtropical zone: a three-yearprospective comparative epidemiological study. Int J Epidemiol 1987;16:561-568.
248. Koshi G, Benjamin V, Cherian G. Rheumatic fever and rheumatic heart disease in rural South Indian children.Bull World Health Organ 1981;59:599-603.
249. Poon-King T, Mayon-White RT, Harnaryan C, et al. Rheumatic fever and glomerulonephritis. In: Parker MT,ed. Pathogenic streptococci: proceedings of the VIIth International Symposium on Streptococci andStreptococcal Diseases held in September 1978. Surrey: Reedbooks, 1979:124-125.
250. Potter EV, Svartman M, Burt EG, Finklea JF, Poon-King T, Earle DP. Relationship of acute rheumatic feverto acute glomerulonephritis in Trinidad. J Infect Dis 1972;125:619-25.
251. Okoroma EO, Ihenacho HNC, Anyanwu CH. Rheumatic fever in Nigerian children. Am J Dis Child1981;135:236-238.
252. Ferguson GW, Shultz JM, Bisno AL. Epidemiology of acute rheumatic fever in a multiethnic, multiracialurban community: the Miami-Dade County experience. J.Infect.Dis. 1991;164:720-725.
253. da Silva CH. Rheumatic fever: a multicenter study in the state of Sao Paulo. Pediatric Committee—SaoPaulo Pediatric Rheumatology Society. Rev.Hosp.Clin.Fac.Med.Sao Paulo 1999;54:85-90.
254. Dillon HC, Jr. Post-streptococcal glomerulonephritis following pyoderma. Rev Infect Dis 1979;1:935-945.255. Haidan A, Talay SR, Rohde M, Sriprakash KS, Currie BJ, Chhatwal GS. Pharyngeal carriage of group C
and group G streptococci and acute rheumatic fever in an Aboriginal population. Lancet 2000;356:1167-1169.
256. Reid HFM, Bassett DCJ, Poon-King T, Zabriskie JB, Read SE. Group G streptococci in healthy school-children and in patients with glomerulonephritis in Trinidad. J Hyg Camb 1985;94:61-68.

A REVIEW OF THE TECHNICAL BASIS FOR THE CONTROL OF CONDITIONS ASSOCIATED WITH GAS INFECTIONS
45
257. al Sekait MA, al Sweliem AA, Tahir M. Rheumatic heart disease in schoolchildren in western district, SaudiArabia. J.R.Soc.Health 1990;110:15-6, 19.
258. Bassili A, Barakat S, Sawaf GE, Zaher S, Zaki A, Din Saleh EE. Identification of clinical criteria for group A-beta hemolytic streptococcal pharyngitis in children living in a rheumatic fever endemic area. J Trop Pediatr2002;48:285-93.
259. Barnham M, Thornton TJ, Lange K. Nephritis caused by Streptococcus zooepidemicus (Lancefield groupC). Lancet 1983;1:945-8.
260. Bateman AC, Ramsay AD, Pallett AP. Fatal infection associated with group C streptococci. J Clin Pathol1993;46:965-967.
261. Bisno AL, Collins CM, Turner JC. M Proteins of Group C Streptococci Isolated from Patients with Acutepharyngitis. J Clin Microbiol 1996;34:2511-15.
262. Jansen TL, Janssen M, de Jong AJ. Reactive arthritis associated with group C and group G beta-hemolyticstreptococci. J Rheumatol 1998;25:1126-30.
263. Turner JC, Fox A, Fox K, et al. Role of group C beta-hemolytic streptococci in pharyngitis: epidemiologic study ofclinical features associated with isolation of group C streptococci. J Clin Microbiol 1993;31:808-811.
264. Collins CM, Kimura A, Bisno AL. Group G streptococcal M protein exhibits structural features analagous tothose of Class I M protein of group A streptococci. Infect Immun 1992;60:3689-3696.
265. Campo RE, Schultz DR, Bisno AL. M proteins of group G streptococci: mechanisms of resistance tophagocytosis. J Infect Dis 1995;171:601-606.
266. Schnitzler N, Podbielski A, Baumgarten G, Mignon M, Kaufhold A. M or M-like protein gene polymorphismsin human group G streptococci. J Clin Microbiol 1995;33:356-63.
267. Geyer A, Schmidt KH. Genetic organisation of the M protein region in human isolates of group C and Gstreptococci: two types of multigene regulator-like (mgrC) regions. Mol Gen Genet 2000;262:965-76.
268. Proft T, Webb PD, Handley V, Fraser JD. Two novel superantigens found in both group A and group CStreptococcus. Infect Immun 2003;71:1361-9.
269. Sriprakash KS, Hartas J. Lateral genetic transfers between group A and G streptococci for M-like genesare ongoing. Microb Pathog 1996;20:275-285.
270. Navarre WW, Schneewind O. Surface proteins of gram-positive bacteria and mechanisms of their targetingto the cell wall envelope. Microbiol Mol Biol Rev 1999;63:174-229.
271. Franken C, Haase G, Brandt C, et al. Horizontal gene transfer and host specificity of beta-haemolyticstreptococci: the role of a putative composite transposon containing scpB and lmb. Mol Microbiol2001;41:925-35.
272. Kalia A, Bessen DE. Presence of streptococcal pyrogenic exotoxin A and C genes in human isolates ofgroup G streptococci. FEMS Microbiol Lett 2003;219:291-5.
273. Steer AC, Carapetis JR, Nolan TM, Shann F. Systematic review of rheumatic heart disease prevalence in childrenin developing countries: the role of environmental factors. J Paediatr Child Health 2002;38:229-34.
274. Alto WA, Gibson R. Acute rheumatic fever: an update. Am.Fam.Physician 1992;45:613-620.
46
GROUP A STREPTOCOCCUS
275. Cunningham MW. Autoimmunity and molecular mimicry in the pathogenesis of post-streptococcal heartdisease. Front Biosci 2003;8:s533-43.
276. Veasy LG, Hill HR. Immunologic and clinical correlations in rheumatic fever and rheumatic heart disease.Pediatr Infect Dis J 1997;16:400-7.
277. Figueroa F, Gonzalez M, Carrion F, et al. Restriction in the usage of variable beta regions in T-cells infiltratingvalvular tissue from rheumatic heart disease patients. J Autoimmun 2002;19:233-40.
278. Cunningham MW. Pathogenesis of group A streptococcal infections. Clin.Microbiol.Rev. 2000;13:470-511.