Skeletal Muscle Movements Health History Inspection Palpation
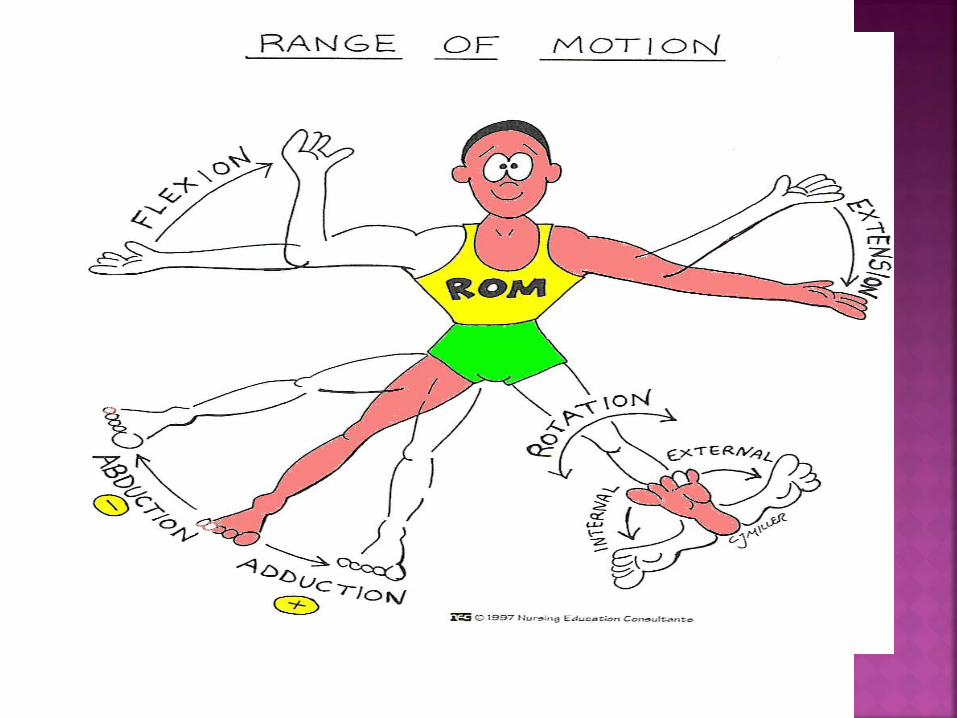
Flexion – bending a limb at the joint Extension – straightening a limb at a joint Abduction – moving a limb away from the
midline (-) Adduction – moving a limb to the midline
(+) Internal rotation – turning a body part
toward the midline External rotation – turning a body part
away from the midline
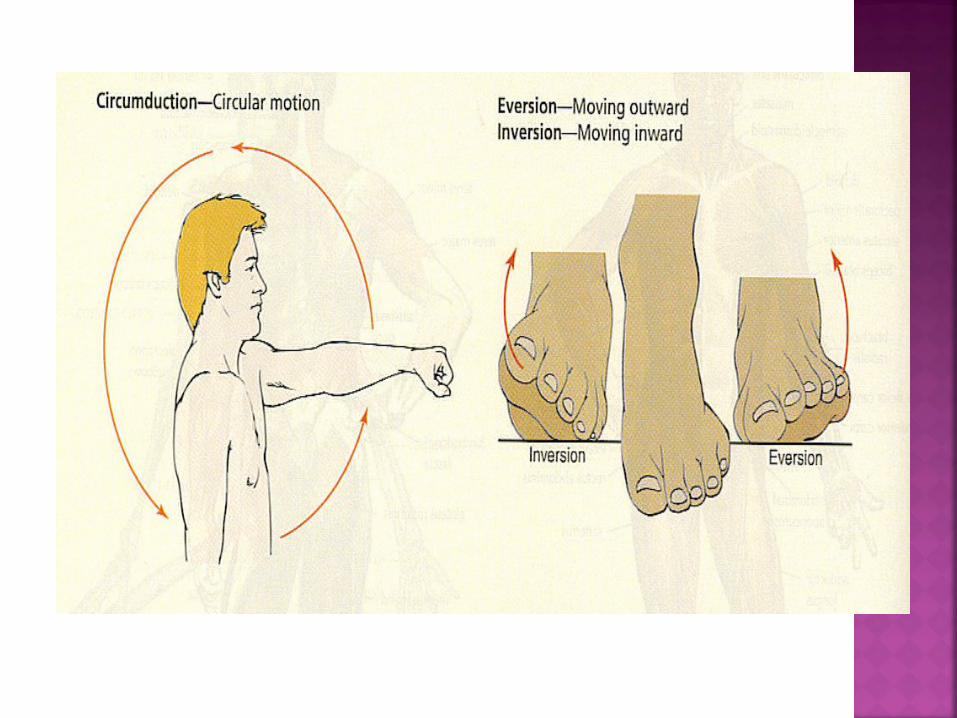
Pronation – turning the palm downward Supination – turning the palm upward Inversion – moving the foot inward Eversion – moving the foot outward Circumduction – moving the arms in a
circular motion
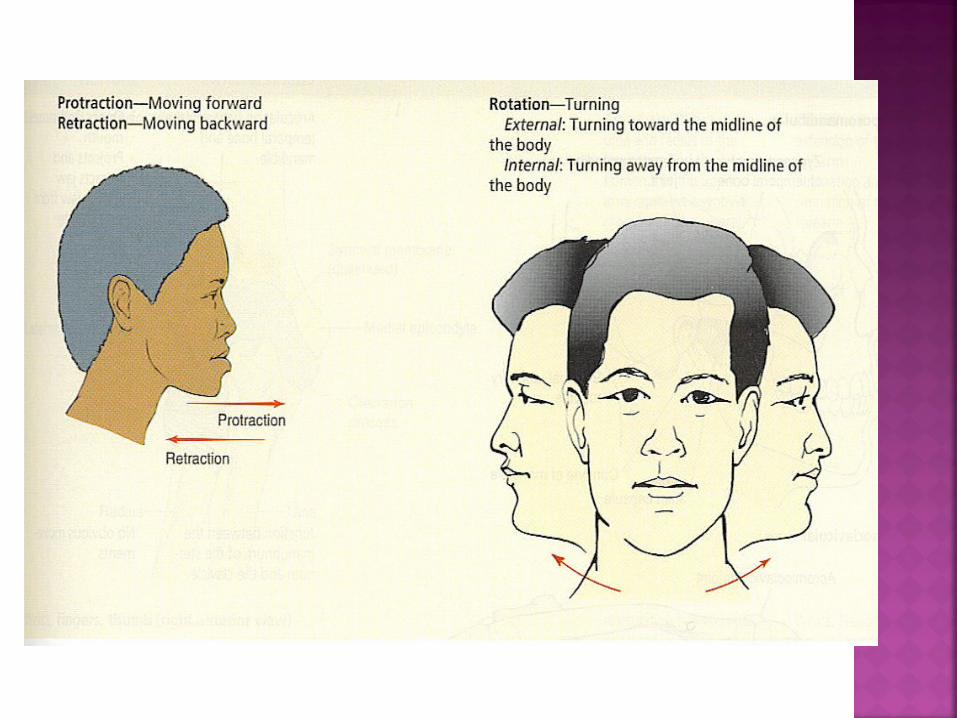
Rotation – moving the head around a central axis
Protraction – moving a body part forward
Retraction – moving a body part backward
Elevation – raising a body part Depression – lowering a body part

Joints – any pain, stiffness, swelling, heat, redness. Evaluate ROM
Muscles – any pain/cramps, muscle strength/weakness
Bones – any pain, deformity, trauma Functional assessment – performance
of ADL’s Self-care behaviors – Exercise, weight
gain/loss, current meds, disability

Infants and Children Birth history Achieved motor development milestones Any broken bones or deformities Check for dislocation of hip – Ortolani’s maneuver
Adolescents Scoliosis screen Sports participation, warms-up, special
equipment Elderly
Hx. of falls, mobility, weakness, ability to perform ADL’s

With a (+) Ortolani’syou will hear a click andfeel the femur shift
Gait – should be smooth, rhythmic and coordinated
Symmetry, alignment, size - of body parts
Any swelling, masses, deformities or atrophy
ROM – should be smooth without clicking
Joints, muscles, bony articulationsAny heat, tenderness, swelling or masses
ROMActiveActive-assistedPassive
Muscle strength: should be (=) bilaterallyGrade strength 0-5 scale – Table pg. 641
Active ROM – Client performs unassisted Active Assisted ROM – Nurse helps client
with ROM exercises Passive ROM –nurse must perform all
ROM. It is useful to prevent atrophy, contractures and promote joint mobility. Does not increase muscle strength.
**Stop and reestablish correct body alignment for a client who experiences pain or cramping with ROM.
Inspection – observe for swelling Palpation
Open mouth Normal opening 3-6 cm, or 3 fingers
Move side to sideStick out lower jawClench teeth
Note size, strength Provide resistance to chin, assesses CN V

InspectionCheck alignment of head and neckSpine should be straight and head erect
PalpationPalpate spinous processes,sternomastoid, trapezius andparavertebral muscles. Should be firm,without tenderness or spasms.
Muscle strengthPlace hand against side of head or jawline.

Extension 0°
Hyperextension 55°
Flexion 45°
Lateral bending 40°
Rotation 70°

InspectionVertical alignment and symmetrySpine should be straight with hipsand shoulders of (=) height.Leg length discrepancy
PalpationSpinous processesParavertebral muscles
Have client touch toesFlexion 75-90°
Bend sidewaysLateral bending 35°
Bend backwardHyperextension 30°
Twist shoulders to one side and then the otherRotation 30°
Inspection Compare posteriorly and anteriorly
Palpation Place one hand on shoulder Palpate for muscle spasms, atrophy, swelling,
heat or tenderness Muscle Strength
Have client shrug shoulders against resistance
Tests CN XI – Spinal accessory
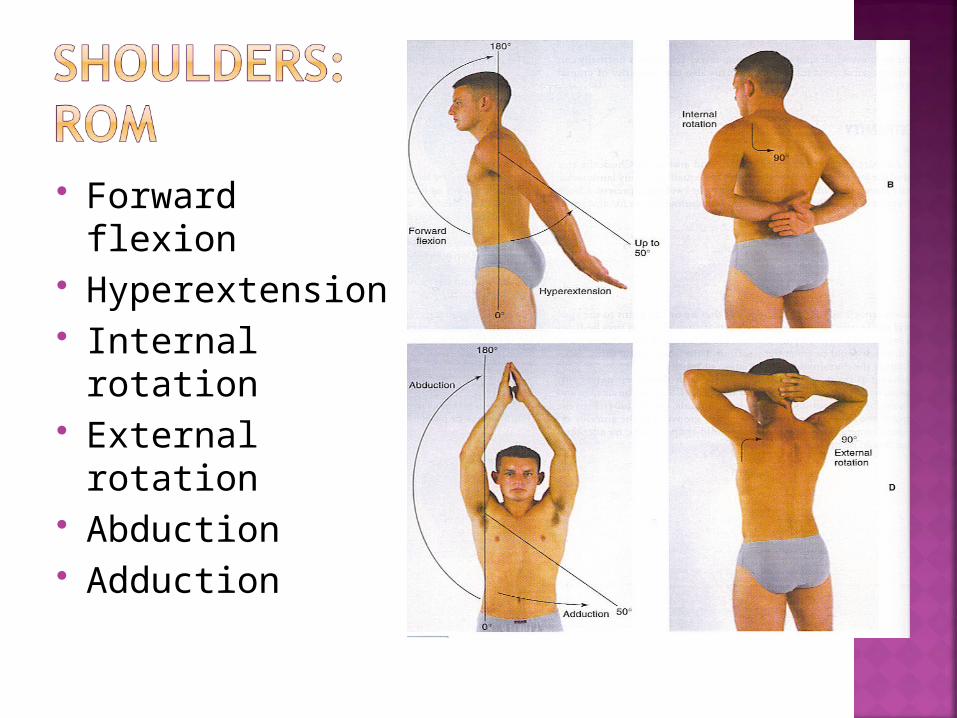
Forward flexion Hyperextension Internal rotation External rotation Abduction Adduction
Inspection Palpation Muscle strength
Apply resistance to forearm ROM
Pronation –palm downSupination – palm up

Inspection Palpation
Include wrist, metacarpal joints

Resistance Carpal Tunnel
Syndrome Phalen’s Test
Acute flexion Numbness or burning
with CTS Tinel’s Sign
With direct percussion of median nerve, burning and tingling occurs with CTS

Inspection Palpation Muscle strength
With hand on thigh have client push upward
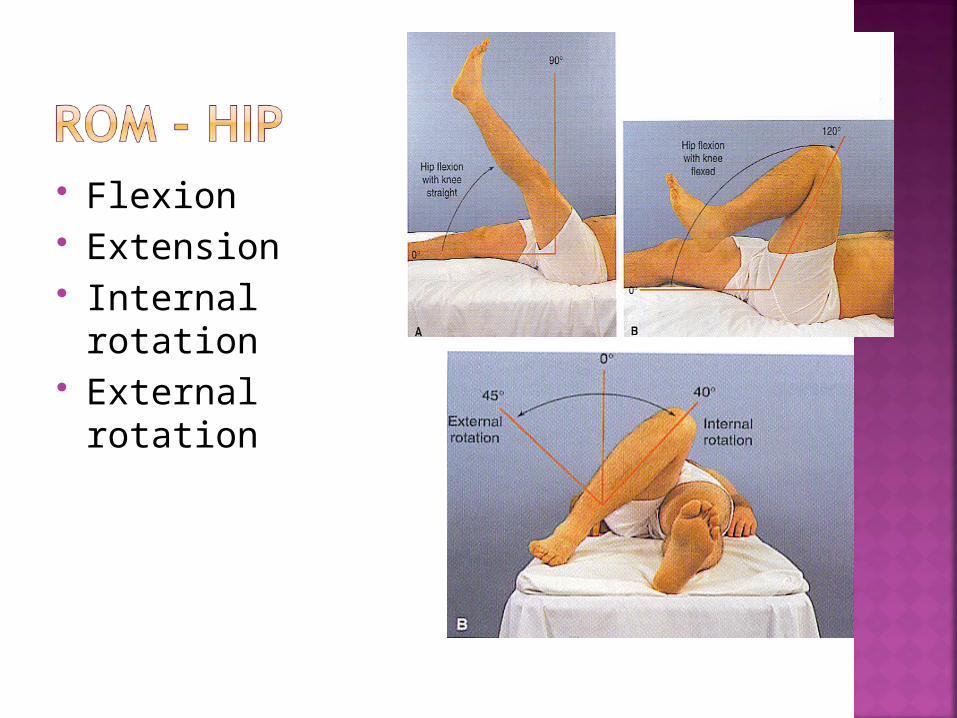
Flexion Extension Internal rotation External rotation
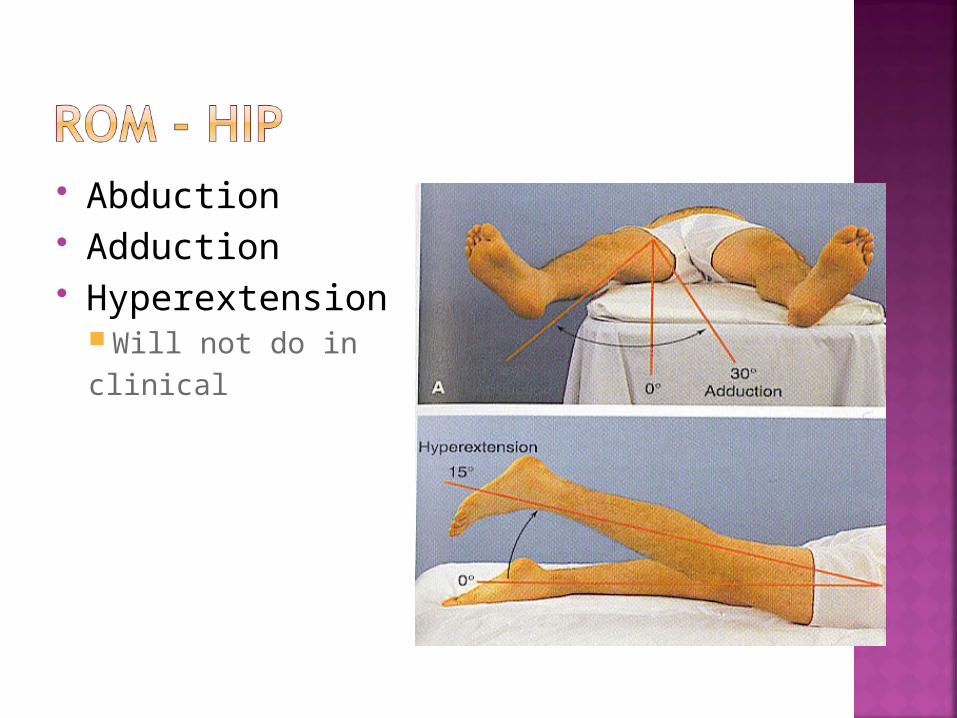
Abduction Adduction Hyperextension
Will not do inclinical

Flexion Extension Hyperextension
InspectionAnkle and Metatarsals
Palpation Muscle Strength
Dorsiflex and plantar flex foot against resistance

Dorsiflexion Plantar flexion Eversion Inversion

![Palpation [Kompatibilitási mód]](https://cdn.vdocument.in/doc/165x107/61bd103e61276e740b0ef9f7/palpation-kompatibilitsi-md.jpg)





