
1
Oregon’s EMS SystemOregon’s EMS System

2
Objectives
Describe the environment in which the first
‘ambulances’ responded
Identify the first volunteer ambulance
Identify the agency that was tasked,
through Legislation, with developing the
Emergency Medical Services

3
Objectives State when Legislation was passed to
develop Oregon’s Trauma System
List the Oregon Revised Statutes and Oregon Administrative Rules that outline the responsibilities of Oregon’s EMS Office
List three things an EMT can do to assist the EMS Office in providing service to him/her

4
Objectives
State the difference between Level 1, Level 2, Level 3 and Level 4 Trauma Hospitals in Oregon
List three reportable actions defined in OAR 333-265-0160
Identify three functions of the Medical Director

5
Way Back
Napoleonic War
– Horse drawn wagons
Civil War
NYC 1869
1899 – The first
motorized ambulance
– Chicago

6
In the beginning…
1913 – Ben C. Buck started the nation’s first private ambulance service in Portland, Oregon
1918 – Mr. Buck donated one of the few motorized ambulances used in WW-I
1920 – First volunteer ambulance service, Roanoke, Virginia
1942 – Buck Ambulance became the first to carry oxygen as standard equipment

7
More Recent CPR, 1960s
– Dr. Leonard Rose, Cardiac Tech
8% WWI, 4.5% Korea,
2% Vietnam Accidental Death & Disability, The Neglected
Disease of American Society, 1966
1966 – DOT – EMS

America’s deaths from influenza were greater than the number of U.S. servicemen
killed in any war
0
100
200
300
400
500
600
700
800
900
Civil WWI 1918-19 WWII Korean Vietnam
War Influenza War War
Thousands

9
Historical PerspectiveCivilian Evolution
• Civilian evolution varied from Civilian evolution varied from region to region in U.S.region to region in U.S.
• Rural areas – UndertakersRural areas – Undertakers Fire departments and volunteer Fire departments and volunteer
ambulance replaced funeral ambulance replaced funeral directorsdirectors
• Urban areasUrban areas Hospital-basedHospital-based Fire departmentsFire departments Police departmentsPolice departments Independent ambulance Independent ambulance
companiescompanies

10

11
More Modern Times
1973-82 Title 12 Grants
– $12 million to Oregon
June 30, 1981
1987 Trauma System
1989 BME OHD- Now DHS-EMS
12
State EMS Office(DHS, Emergency Medical Services and Trauma Systems)
Statutory responsibility– Oregon Revised Statutes Chap. 682, 431
– Oregon Administrative Rules Chap. 333-200, 250, 255, 260, 265, Chap. 847
State EMS office
State EMS Committee– Subcomm. EMT Cert. and Discipline
STAB, ATAB

13
State EMS Office
Charge – minimum standards– FR– EMTs– Ambulance vehicles– Ambulance services– Trauma hospitals
Certification, CME Accreditation process

14
State EMS Office
Be nice to them Do your research Start locally Read, then follow directions Know your responsibilities Document, conduct business in writing Don’t shop for answers

Things in the works!• “Certification” of First Responders
• Revision of Oregon EMT-Intermediate Curriculum (rethinking)
• ACEP/OHD-EMS Supervising Physician Course
• 40 Hour Oregon Version DOT National Standard EMS Instructor Course
• National Registry Exam
• Manage Grant Programs
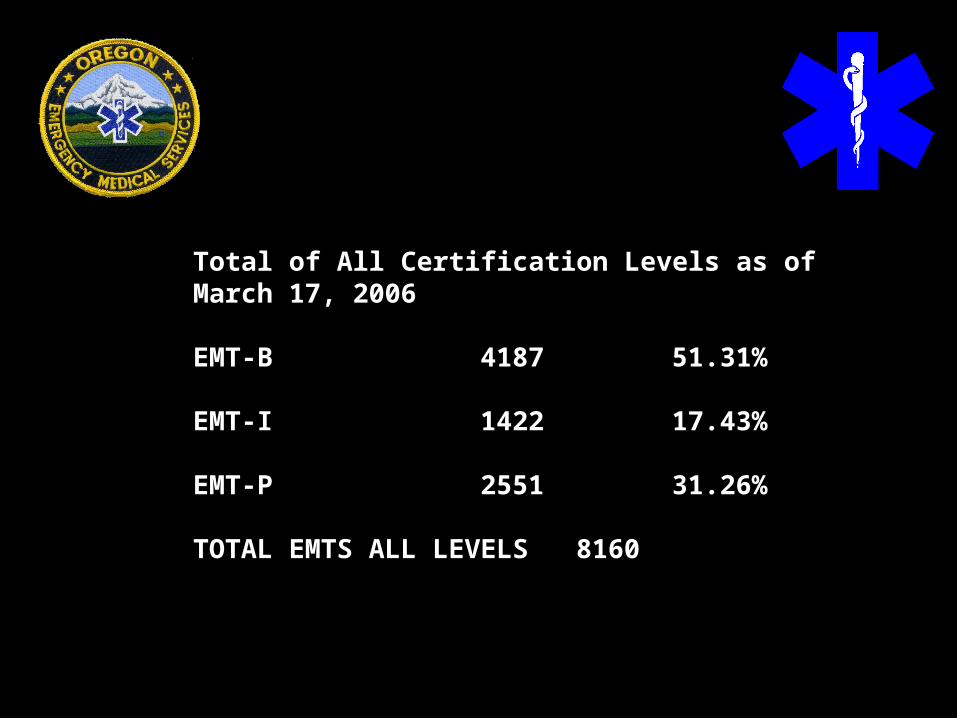
Total of All Certification Levels as of March 17, 2006
EMT-B 4187 51.31%
EMT-I 1422 17.43%
EMT-P 2551 31.26%
TOTAL EMTS ALL LEVELS 8160

Oregon’s EMTs All Levels by ZIP code

Oregon’s EMT-Basics by ZIP code
4075
51.23%of total EMTs

Oregon’s EMT-Intermediates by ZIP code
1472
18.51%of total EMTs

Oregon’s Paramedics by ZIP code
2407
30.16% of total EMTs

Statewide ALL EMS Agencies
N = 654

Statewide Transport Agencies
N = 136

Statewide Non-transport Agencies
N = 518

25
Trauma Section
State wide trauma system
Hospital designation 1-4
Data gathering
Triage criteria
911 System

Revised 3/20/02
Oregon Trauma System Hospitals
Revised: 1/23/04
3
1
2
4
III
IV
1. Legacy Emanuel Hospital & Health Center, Portland2. Oregon Health & Science University, Portland
3. Good Samaritan Regional Medical Ctr., Corvallis4. Sacred Heart Medical Center, Eugene5. St. Alphonsus Regional Medical Center, Boise, ID *6. St. Charles Medical Center, Bend7. SW Washington Medical Center, Vancouver, WA *
8. Bay Area Hospital, Coos Bay9. Columbia Memorial Hospital, Astoria10. Good Shepherd Medical Center, Hermiston11. Grande Ronde Hospital, La Grande12. Holy Rosary Medical Center, Ontario13. McKenzie-Willamette Hospital, Springfield14. Mercy Medical Center, Roseburg15. Merle West Medical Center, Klamath Falls16. Mid-Columbia Medical Center, The Dalles17. Peace Harbor Hospital, Florence18. Pioneer Memorial Hospital, Prineville19. Providence Hood River Memorial Hospital, Hood River20. Providence Medford Medical Center, Medford21. Rogue Valley Medical Center, Medford22. Salem Hospital, Salem23. Samaritan Albany General Hospital, Albany24. Samaritan Lebanon Community Hospital, Lebanon25. St. Anthony Hospital, Pendleton26. St. John Medical Center, Longview, WA *27. St. Mary Medical Center, Walla Walla, WA *28. Three Rivers Community Hospital, Grants Pass29. Tillamook County General Hospital, Tillamook30. Walla Walla General Hospital, Walla Walla, WA *31. Willamette Valley Medical Center, McMinnville
32. Ashland Community Hospital, Ashland33. Blue Mountain Hospital, John Day34. Central Oregon Community Hospital, Redmond35. Coquille Valley Hospital, Coquille36. Curry General Hospital, Gold Beach37. Harney District Hospital, Burns38. Lake District Hospital, Lakeview39. Lower Umpqua Hospital, Reedsport40. Mountain View Hospital, Madras41. Pioneer Memorial Hospital, Heppner42. Providence Newberg Hospital, Newberg43. Samaritan North Lincoln Hospital, Lincoln City44. Samaritan Pacific Communities Hospital, Newport45. Santiam Memorial Hospital, Stayton46. Silverton Hospital, Silverton47. St. Elizabeth Health Services, Baker City48. Sutter Coast Hospital, Crescent City, CA49. Wallowa Memorial Hospital, Enterprise50. West Valley Community Hospital, Dallas
Level I
Level II
Level III
Level IV
* ID WA Designated
30

TOTRAUMAHOSPITAL
VITAL SIGNS & LEVEL OF CONSCIOUSNESS:Systolic blood pressure <90 mmHg; orRespiratory distress with rate<10 or >29; or Airway management required; orGlasgow Coma Scale <12
ANATOMY OF INJURY:Penetrating injury of the head, neck, torso, or groin; orAmputation above the wrist or ankle; orSpinal cord injury with limb paralysis; orFlail chest; orTwo or more obvious long-bone (humerus/femur) fractures.
YES→MANDATORYTRAUMA SYSTEM ENTRY
MECHANISM OF INJURY:Death of a same car occupant; orEjection of patient from an enclosed vehicle; orHeavy extrication time >20 minutes.
TRIAGE CRITERIA AND DECISION SCHEME

NO↓
HIGH ENERGY TRANSFER SITUATIONS:Falls >20 feet; orPedestrian hit at 20 mph or thrown 15 feet; orRollover; orMotorcycle, ATV or bicycle crash; orSignificant impact or intrusion into occupant space of vehicle.
YES
→DISCRETIONARYTRAUMA SYSTEM ENTRY
These criteria shall cause a high index of suspicion that a patient may have sustained a severe injury. Trauma system entry for patients meeting two or more of these criteria is strongly encouraged.
CO-MORBID FACTORS:Extremes of age <5 or >55 years; orPatient with bleeding disorder or patient on anticoagulants; orMedical illness: cardiac or respiratory disease, insulin-dependentdiabetes, cirrhosis, or morbid obesity; orPregnancy; orImmunosuppressed patients; orPresence of intoxicants.

29
Prehospital Standards
Reporting criteria (ORS 682.220(4)) Applications and recertification. Backgrounds E-4 The nasty stuff
– Sexual assault elderly– Walking around in sox– Diverting drugs to owner– Convicted double homicide

30
Medical Directors
Under BME Standing orders (protocols) Advocate, training Scope of Practice
– Don’t violate
Only under an agency's protocols Teamwork

Questions??







