Adjuvant Chemotherapy in Older Adults with Lung Cancer
Ajeet Gajra MD FACP
Upstate Cancer Center,
SUNY Upstate Medical University
Syracuse, NY
Introduction: Early Stage NSCLC • More older adults safely undergo surgery given improved
surgical techniques and peri-operative care
• Cisplatin-based adjuvant chemotherapy (ACT) is standard of care in early stage resected NSCLC though no trials specific to older adults
• The evidence is limited to:– Sub-group analyses of studies in age-unselected populations– Retrospective analyses from population databases
• It is challenging to administer cisplatin to older adults

Adjuvant Chemotherapy in Older Adults with NSCLC: Questions
1. What proportion of older adults receive surgery for stage I-IIIA NSCLC?
2. What is the representation of elderly in ACT trials?(IALT, JBR, ANITA and CALGB 9633/ LACE)
Example of database studies: SEER, Ontario, VA
3. Decision making in the clinic
4. Is carboplatin as good as cisplatin?
5. Is some chemotherapy better than none i.e. chemotherapy dose?
7. Can Geriatric Assessment help?
Surgical Treatment of Early Stage NSCLC
The Impact of Age
Surgical Treatment of NSCLC in Older Adults
• How often are older adults offered curative
surgery compared to younger patients?
• Is the Overall Survival the same amongst
older adults treated with curative surgery as
younger patients?
• What about lung cancer specific survival?
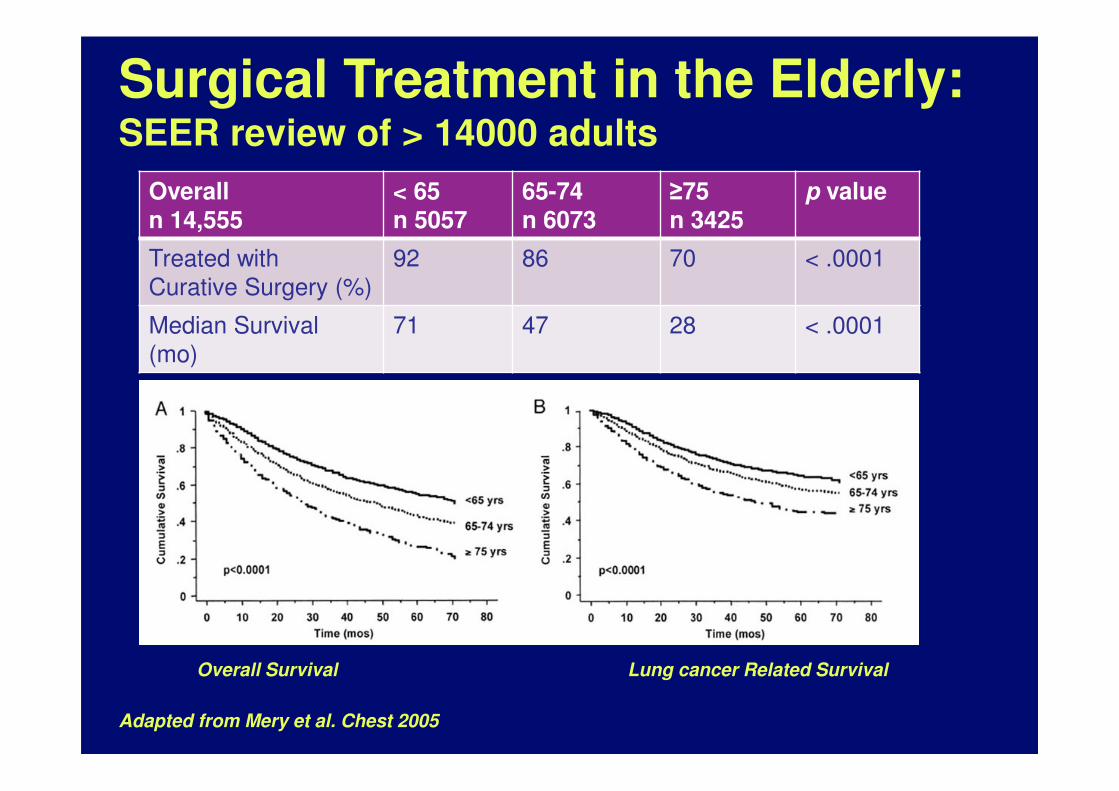
Surgical Treatment in the Elderly:SEER review of > 14000 adults
Overalln 14,555
< 65n 5057
65-74n 6073
≥75n 3425
p value
Treated with
Curative Surgery (%)
92 86 70 < .0001
Median Survival
(mo)
71 47 28 < .0001
Adapted from Mery et al. Chest 2005
Overall Survival Lung cancer Related Survival
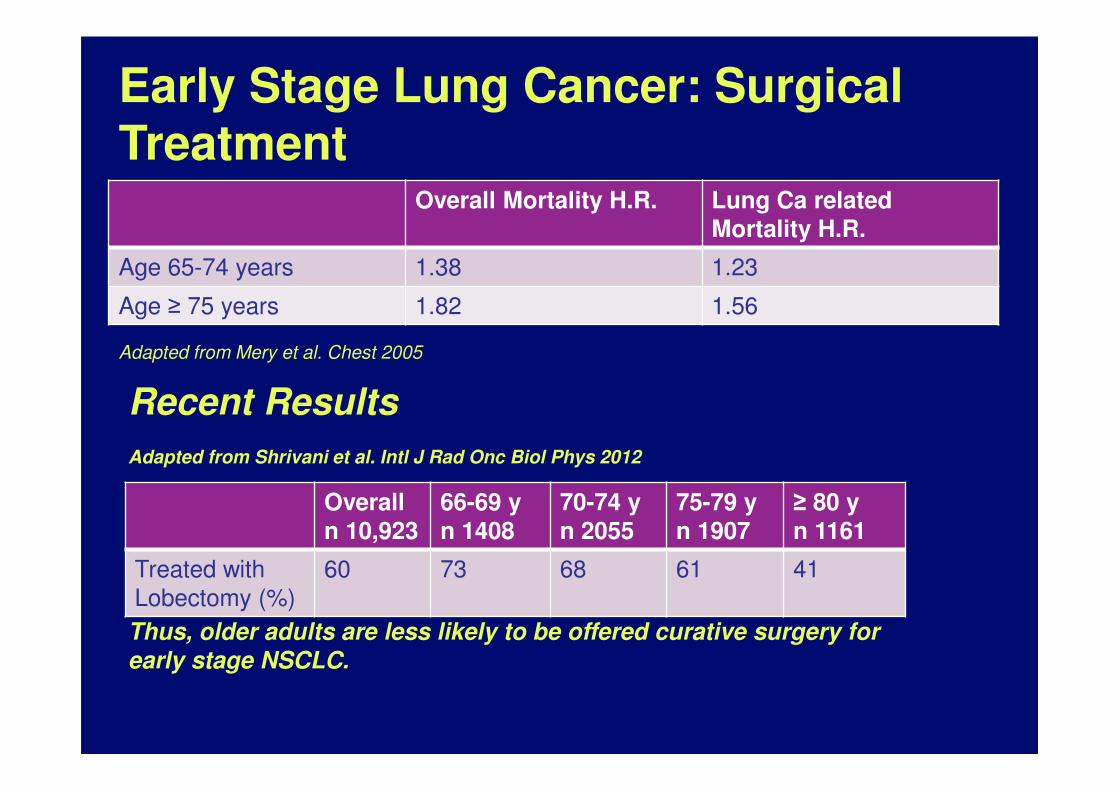
Early Stage Lung Cancer: Surgical Treatment
Overall Mortality H.R. Lung Ca related Mortality H.R.
Age 65-74 years 1.38 1.23
Age ≥ 75 years 1.82 1.56
Overalln 10,923
66-69 yn 1408
70-74 yn 2055
75-79 yn 1907
≥ 80 yn 1161
Treated with
Lobectomy (%)
60 73 68 61 41
Recent Results
Adapted from Shrivani et al. Intl J Rad Onc Biol Phys 2012
Adapted from Mery et al. Chest 2005
Thus, older adults are less likely to be offered curative surgery for
early stage NSCLC.
“But my surgeon said they got it all so why do I need chemo…?”
“….but they even got the lymph nodes that the cancer traveled to!”
“Surgeons can cut out everything
except cause.”
Herbert M. Shelton
Adjuvant Chemotherapy in Stage I-III NSCLC
Data from Prospective Randomized Clinical Trials
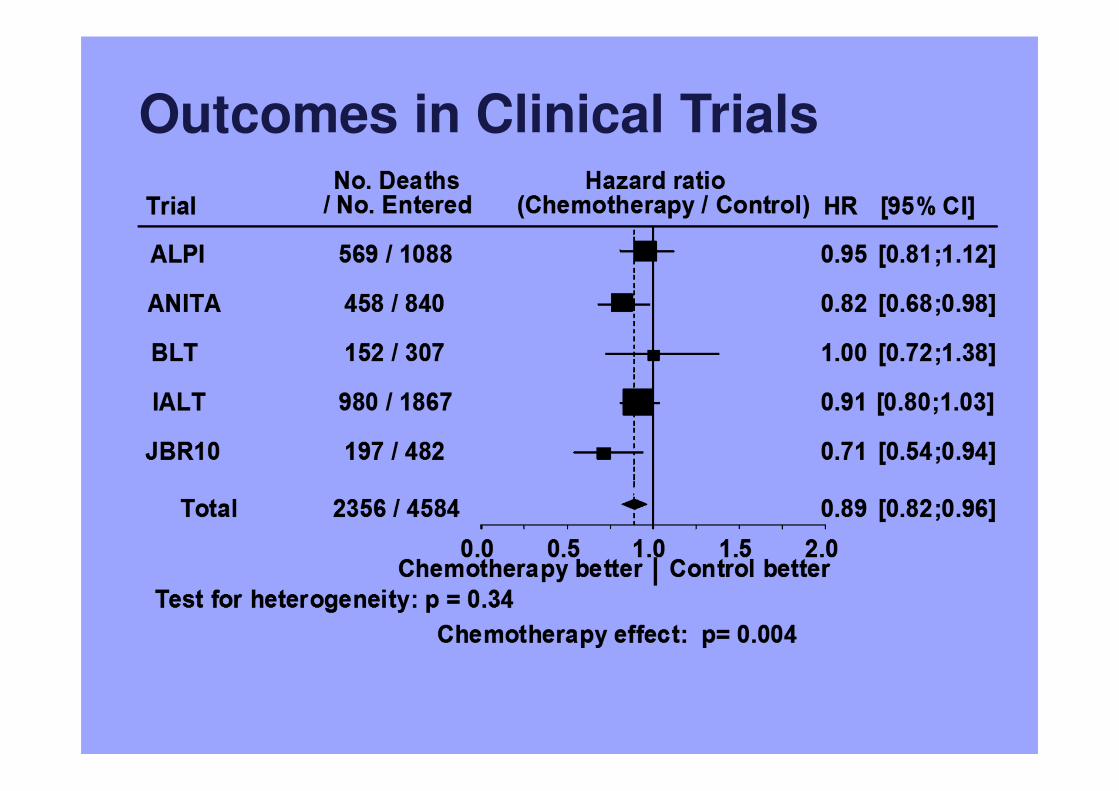
Outcomes in Clinical Trials
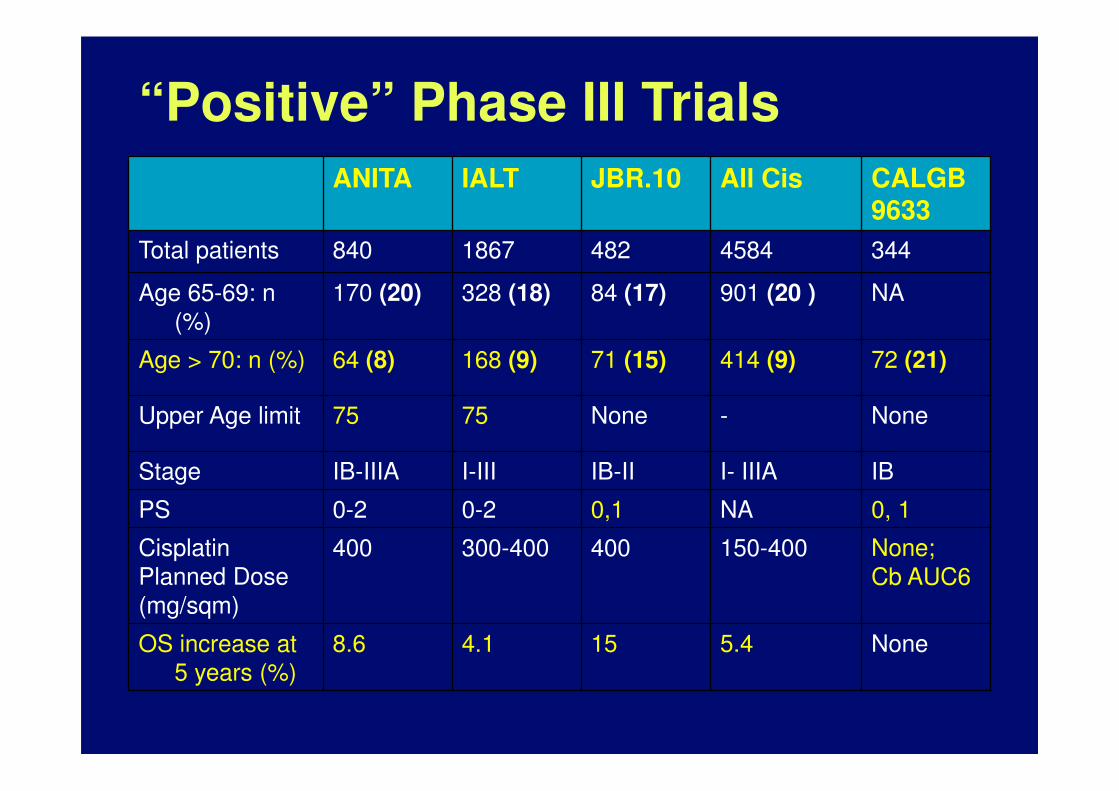
“Positive” Phase III Trials
ANITA IALT JBR.10 All Cis CALGB9633
Total patients 840 1867 482 4584 344
Age 65-69: n
(%)
170 (20) 328 (18) 84 (17) 901 (20 ) NA
Age > 70: n (%) 64 (8) 168 (9) 71 (15) 414 (9) 72 (21)
Upper Age limit 75 75 None - None
Stage IB-IIIA I-III IB-II I- IIIA IB
PS 0-2 0-2 0,1 NA 0, 1
Cisplatin
Planned Dose
(mg/sqm)
400 300-400 400 150-400 None;
Cb AUC6
OS increase at
5 years (%)
8.6 4.1 15 5.4 None
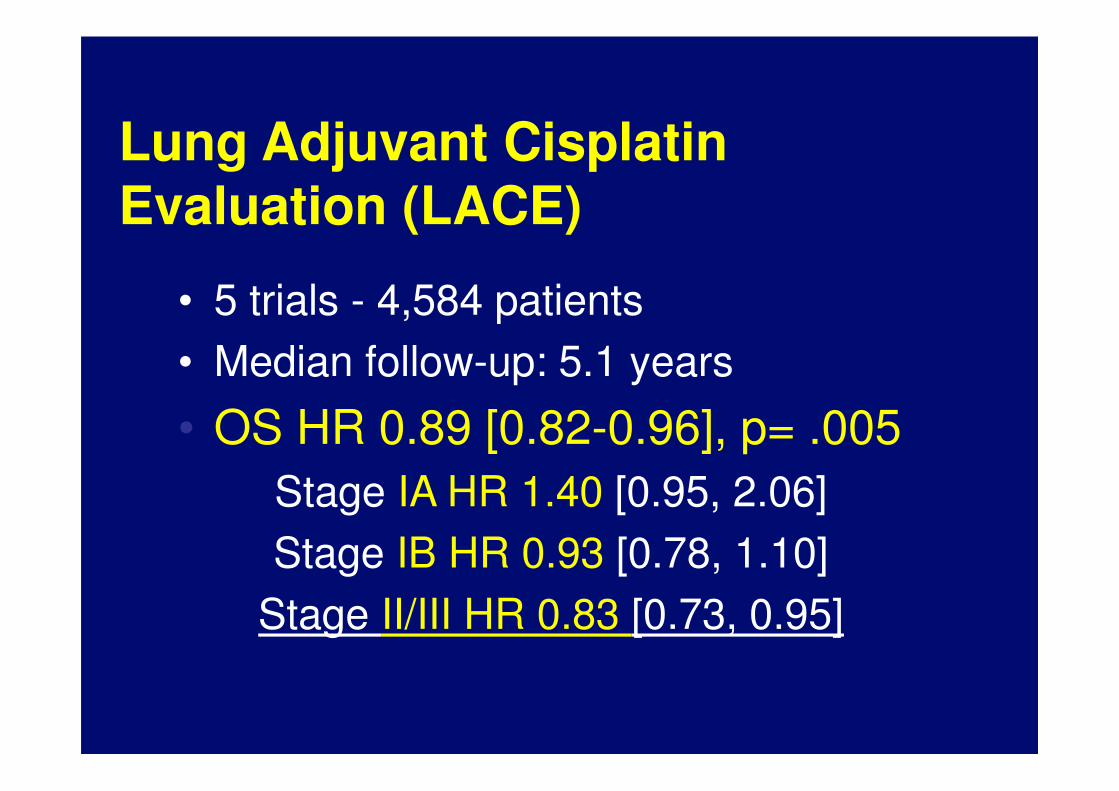
Lung Adjuvant Cisplatin Evaluation (LACE)
• 5 trials - 4,584 patients
• Median follow-up: 5.1 years
• OS HR 0.89 [0.82-0.96], p= .005
Stage IA HR 1.40 [0.95, 2.06]
Stage IB HR 0.93 [0.78, 1.10]
Stage II/III HR 0.83 [0.73, 0.95]
““As to diseases, make a habit of two things —to help, or at least, to do no harm…”
Hippocrates
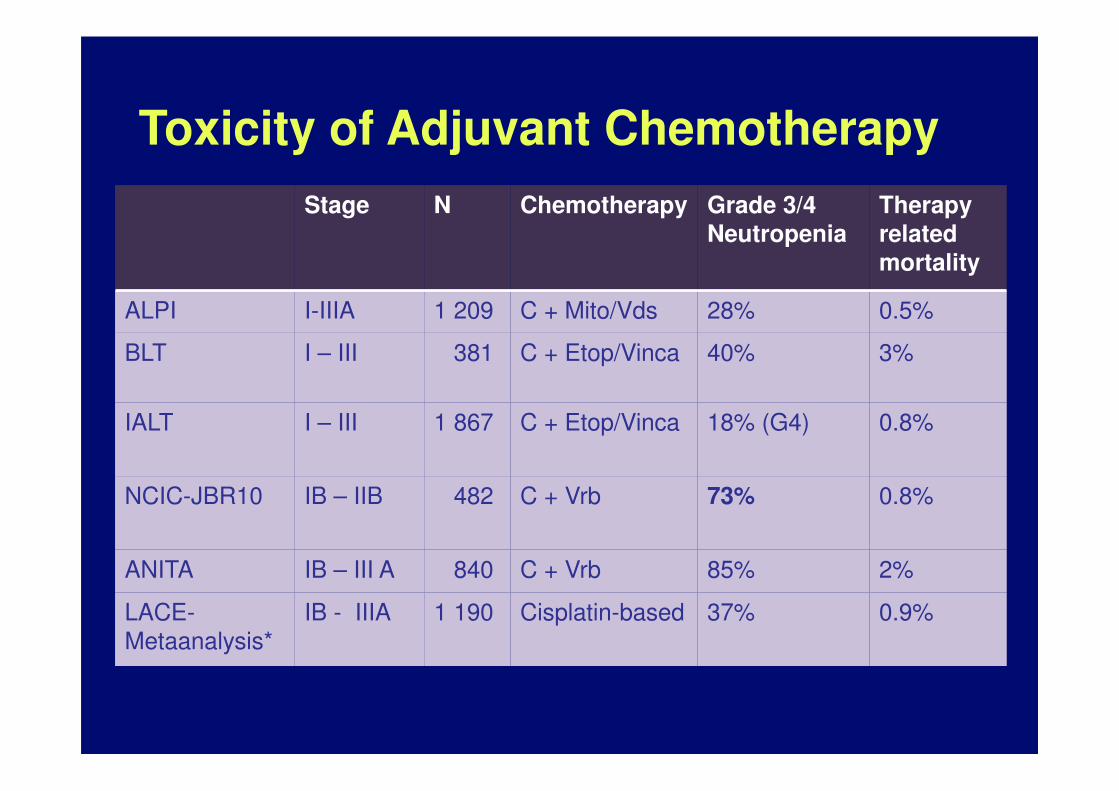
Toxicity of Adjuvant Chemotherapy
Stage N Chemotherapy Grade 3/4 Neutropenia
Therapy related mortality
ALPI I-IIIA 1 209 C + Mito/Vds 28% 0.5%
BLT I – III 381 C + Etop/Vinca 40% 3%
IALT I – III 1 867 C + Etop/Vinca 18% (G4) 0.8%
NCIC-JBR10 IB – IIB 482 C + Vrb 73% 0.8%
ANITA IB – III A 840 C + Vrb 85% 2%
LACE-
Metaanalysis*
IB - IIIA 1 190 Cisplatin-based 37% 0.9%
Adjuvant Trials in NSCLC: Summary
• No trials specific to older adults to date
• Older adults are under-represented in existing trials
– JBR.10- 15%
– LACE – 9%
• Older adults may be at significant risk of chemotherapy toxicity
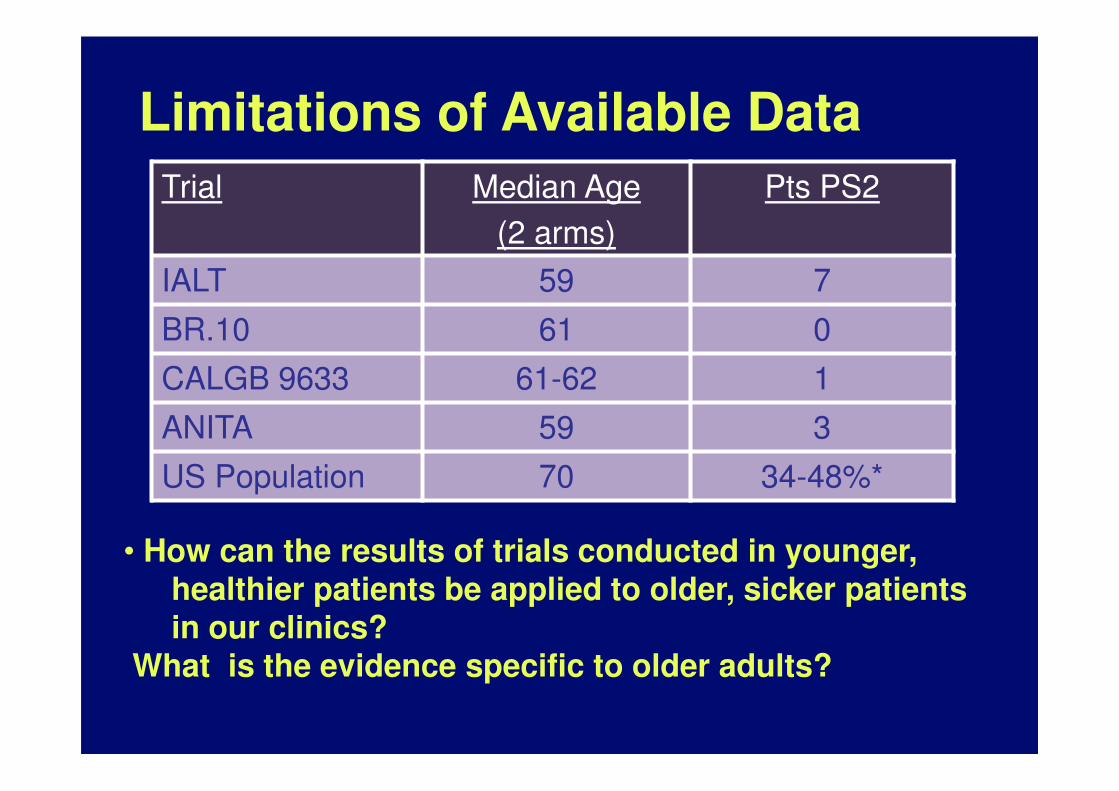
Limitations of Available Data
Trial Median Age
(2 arms)
Pts PS2
IALT 59 7
BR.10 61 0
CALGB 9633 61-62 1
ANITA 59 3
US Population 70 34-48%*
• How can the results of trials conducted in younger, healthier patients be applied to older, sicker patients in our clinics?
What is the evidence specific to older adults?
In the absence of PRCTs specific to older adults
Post-hoc Subset Analyses
JBR.10
LACE
Population Database studies
SEER
VA Cancer Registry
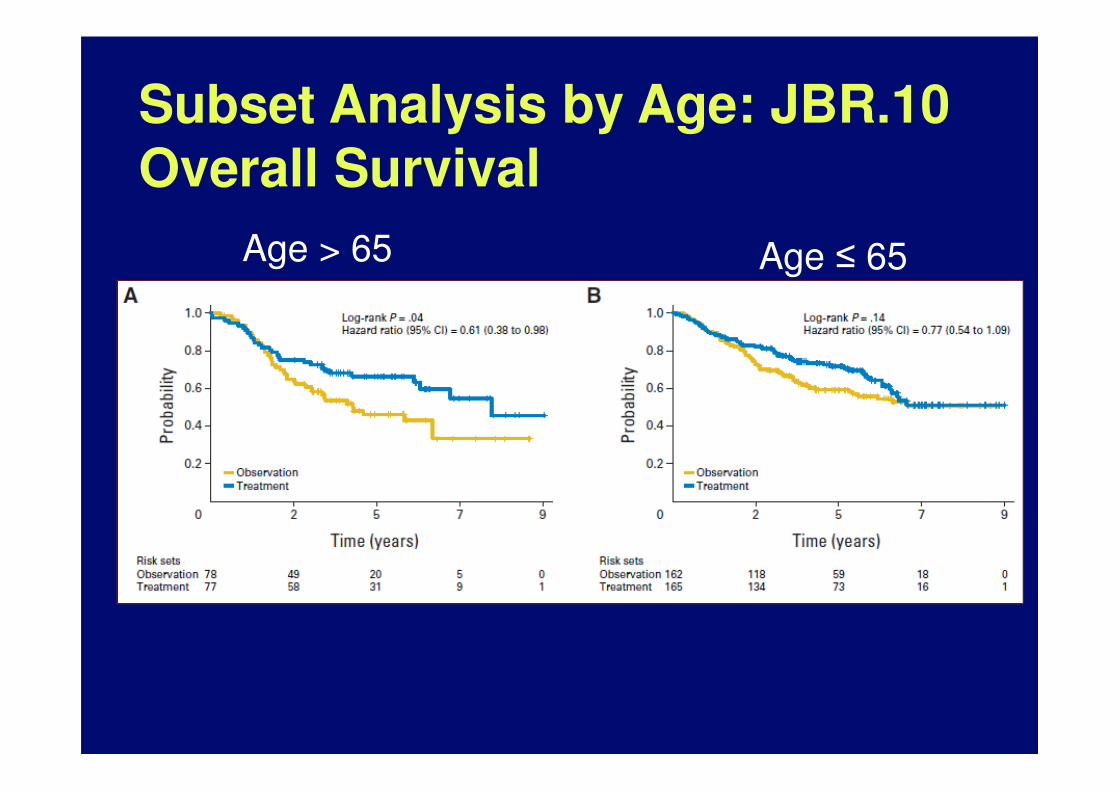
Subset Analysis by Age: JBR.10Overall Survival
Age > 65 Age ≤ 65
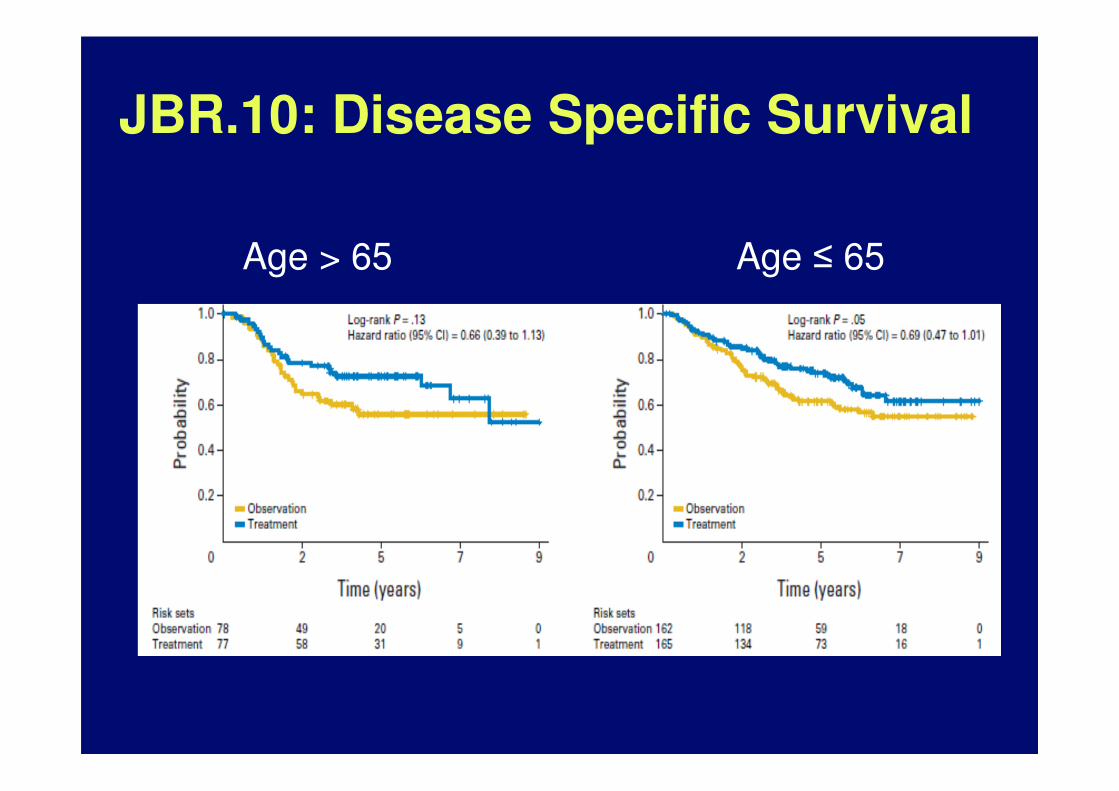
JBR.10: Disease Specific Survival
Age > 65 Age ≤ 65
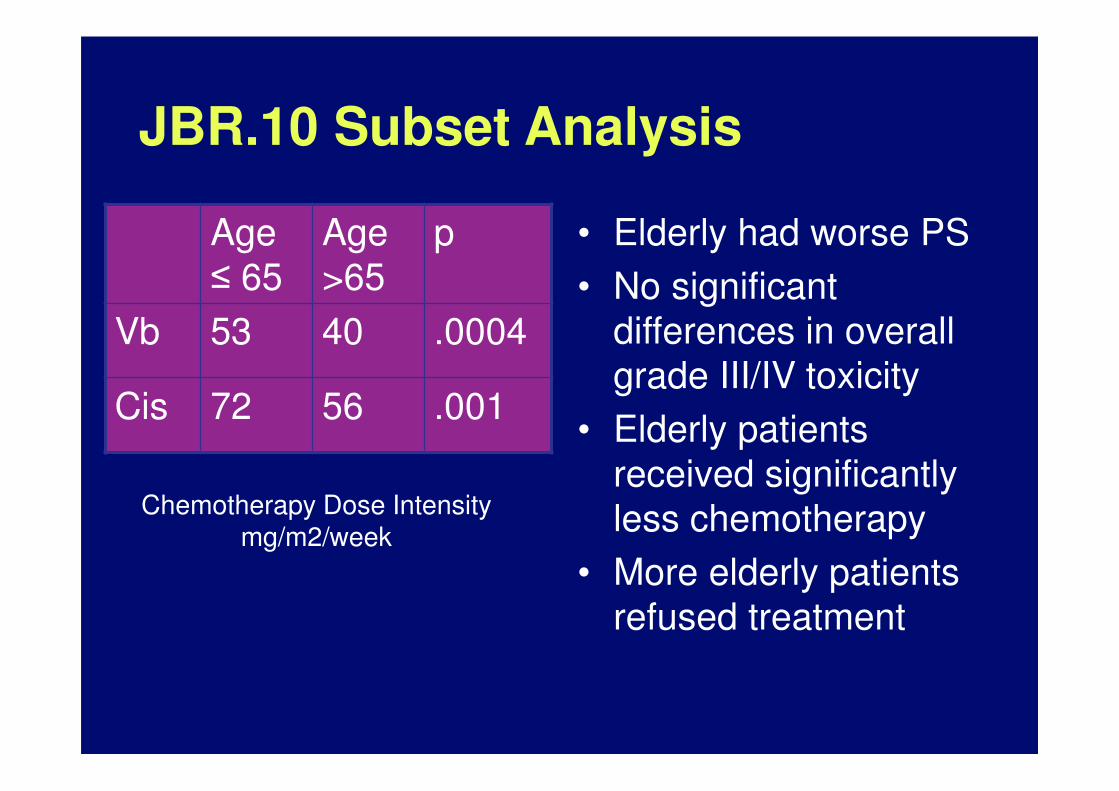
JBR.10 Subset Analysis
• Elderly had worse PS
• No significant
differences in overall
grade III/IV toxicity
• Elderly patients
received significantly
less chemotherapy
• More elderly patients
refused treatment
Age
≤ 65
Age
>65
p
Vb 53 40 .0004
Cis 72 56 .001
Chemotherapy Dose Intensity mg/m2/week
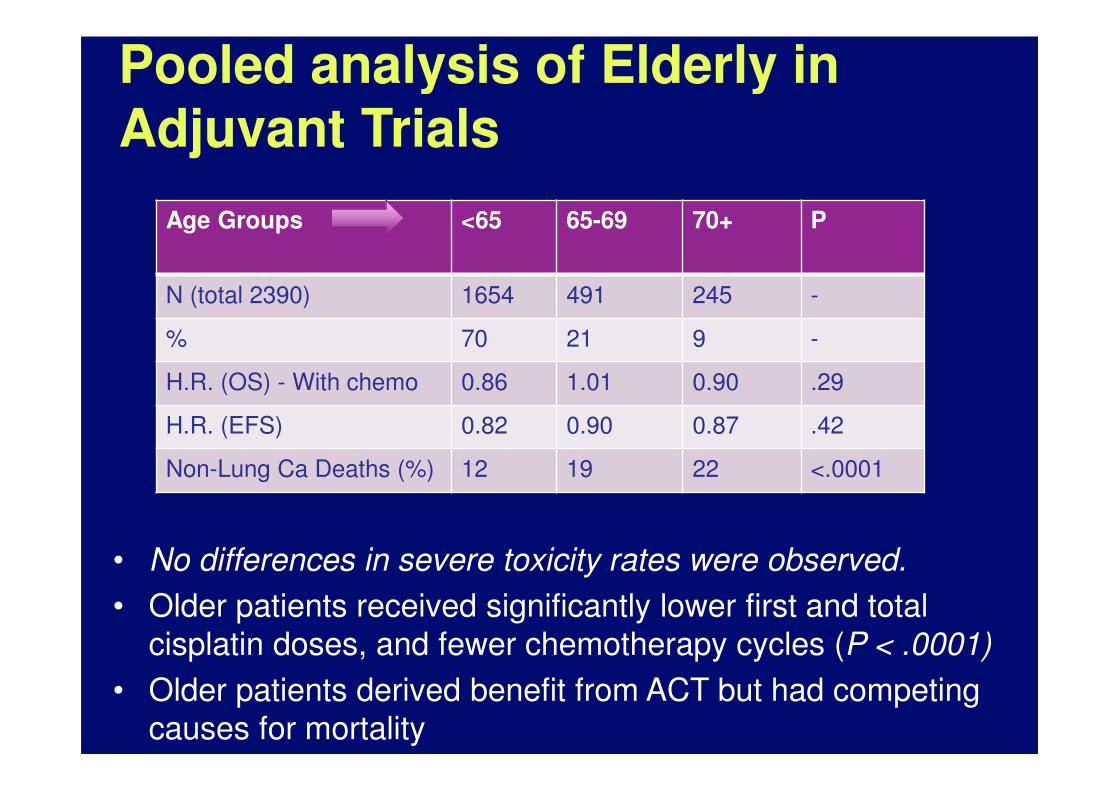
Pooled analysis of Elderly in Adjuvant Trials
• No differences in severe toxicity rates were observed.
• Older patients received significantly lower first and total
cisplatin doses, and fewer chemotherapy cycles (P < .0001)
• Older patients derived benefit from ACT but had competing
causes for mortality
Age Groups <65 65-69 70+ P
N (total 2390) 1654 491 245 -
% 70 21 9 -
H.R. (OS) - With chemo 0.86 1.01 0.90 .29
H.R. (EFS) 0.82 0.90 0.87 .42
Non-Lung Ca Deaths (%) 12 19 22 <.0001
Population Database Studies
SEER Database
Veterans Administration Cancer Registry
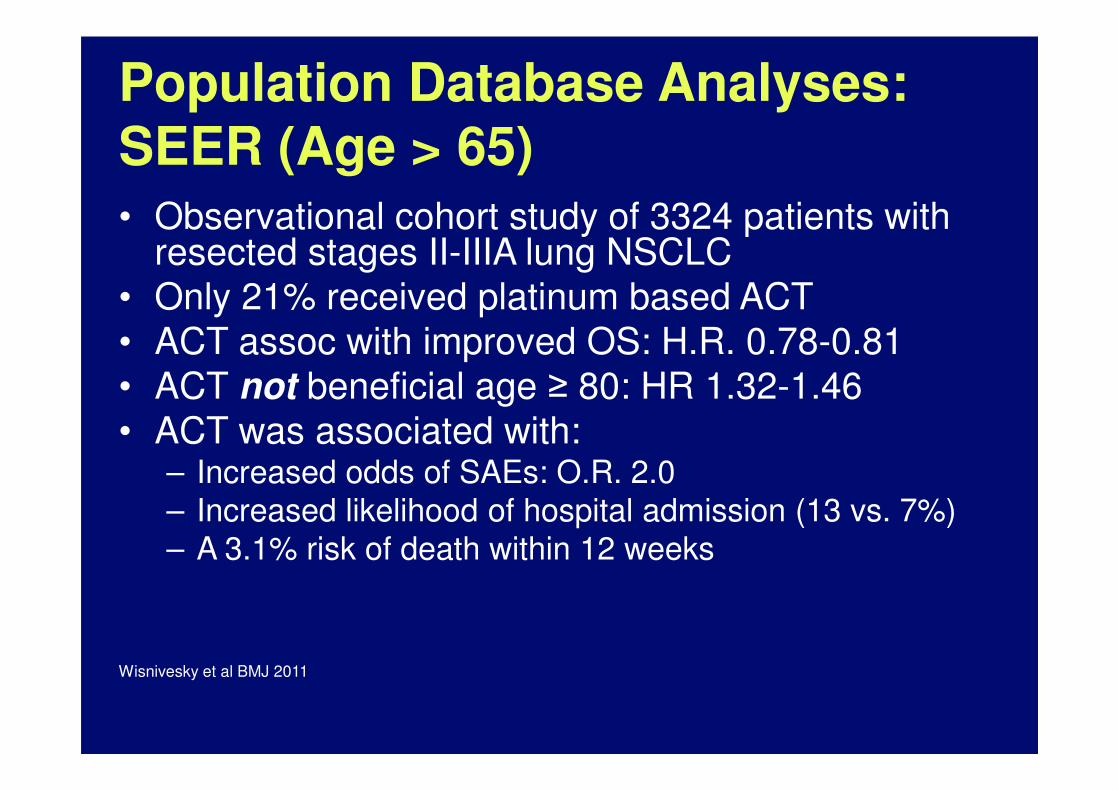
Population Database Analyses: SEER (Age > 65)
• Observational cohort study of 3324 patients with resected stages II-IIIA lung NSCLC
• Only 21% received platinum based ACT
• ACT assoc with improved OS: H.R. 0.78-0.81
• ACT not beneficial age ≥ 80: HR 1.32-1.46
• ACT was associated with:– Increased odds of SAEs: O.R. 2.0
– Increased likelihood of hospital admission (13 vs. 7%)
– A 3.1% risk of death within 12 weeks
Wisnivesky et al BMJ 2011
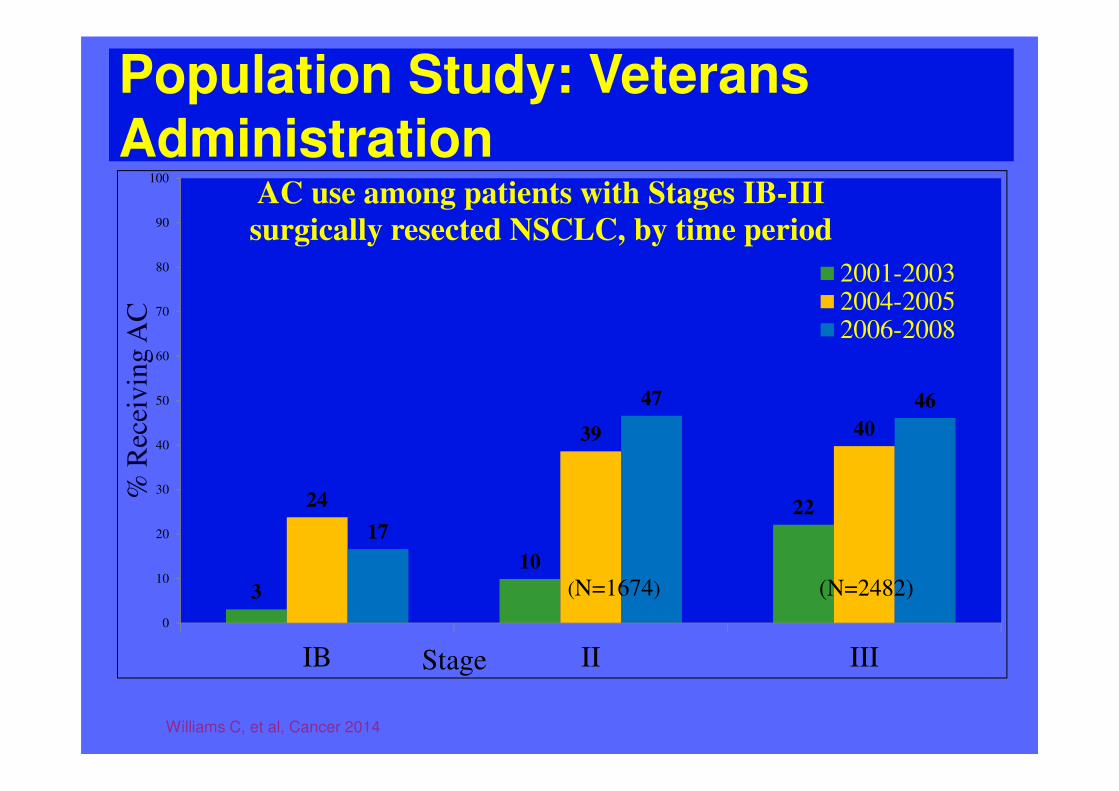
Population Study: Veterans Administration
Williams C, et al, Cancer 2014
3
10
2224
39 40
17
47 46
0
10
20
30
40
50
60
70
80
90
100
IB II III
% R
ecei
vin
g A
C
Stage
AC use among patients with Stages IB-III
surgically resected NSCLC, by time period
2001-20032004-20052006-2008
(N=1674) (N=2482)
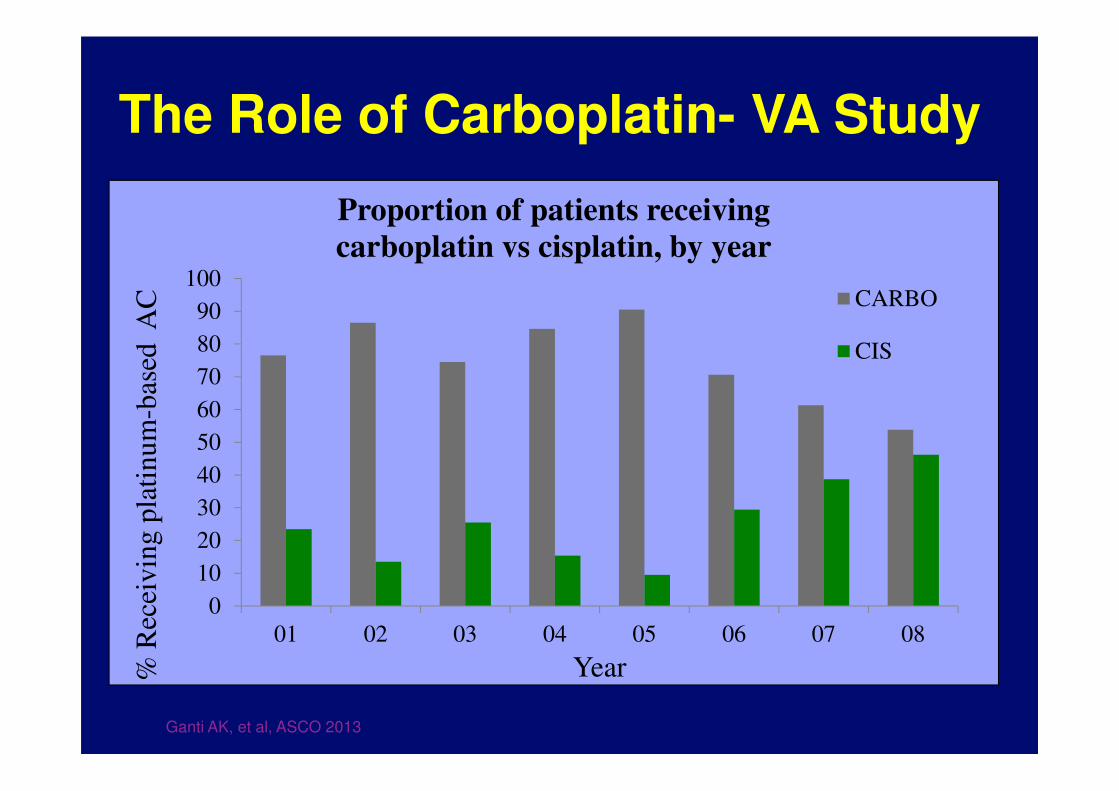
The Role of Carboplatin- VA Study
0
10
20
30
40
50
60
70
80
90
100
01 02 03 04 05 06 07 08
% R
ecei
vin
g p
lati
nu
m-b
ased
AC
Year
Proportion of patients receiving
carboplatin vs cisplatin, by year
CARBO
CIS
Ganti AK, et al, ASCO 2013
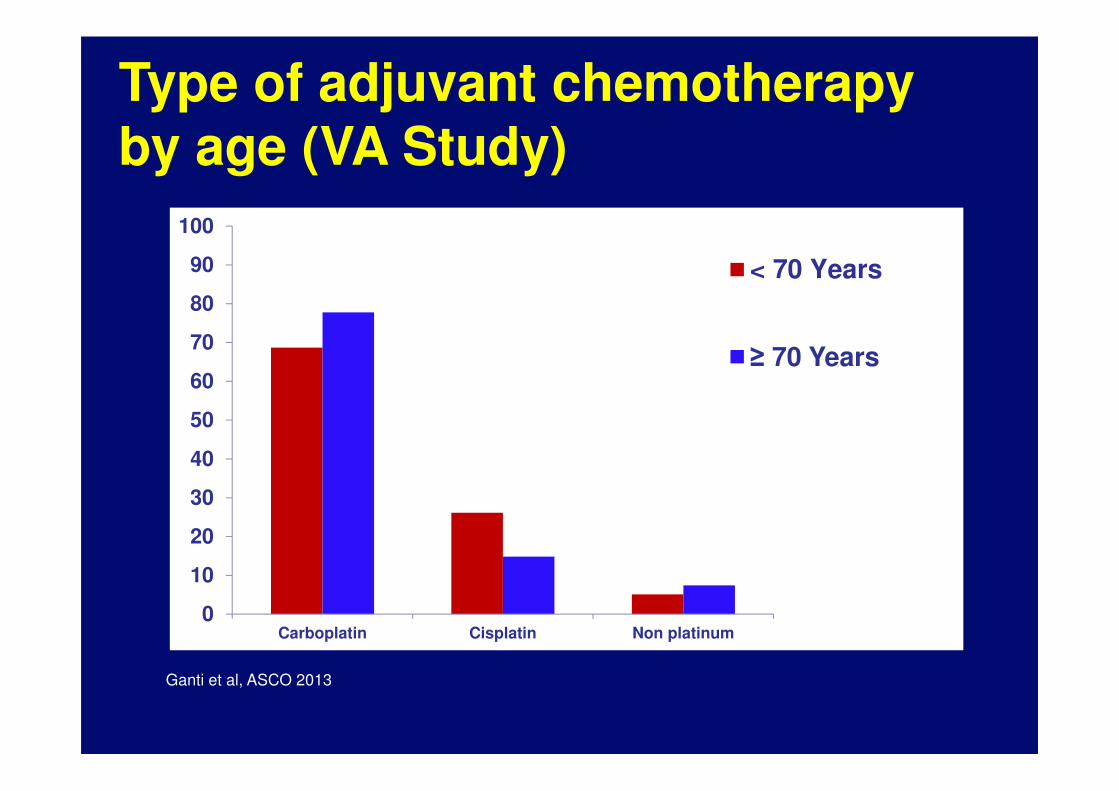
Type of adjuvant chemotherapy by age (VA Study)
Ganti et al, ASCO 2013
0
10
20
30
40
50
60
70
80
90
100
Carboplatin Cisplatin Non platinum
< 70 Years
≥ 70 Years
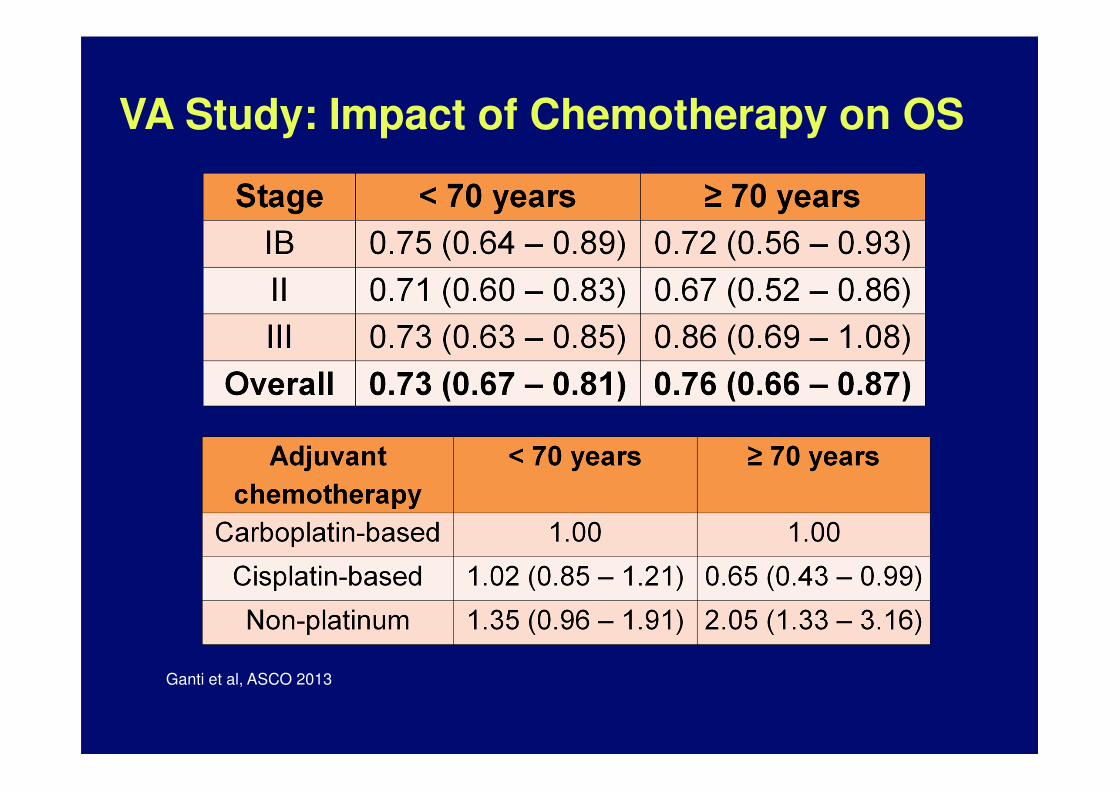
VA Study: Impact of Chemotherapy on OS
Ganti et al, ASCO 2013
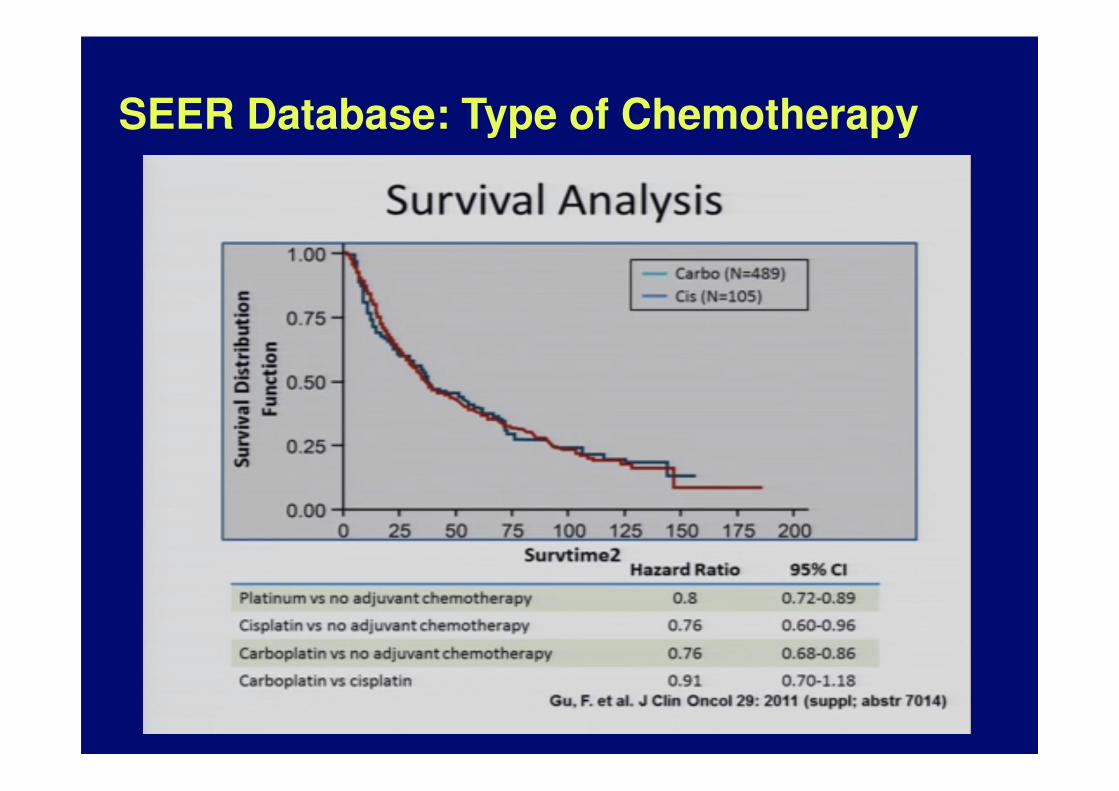
SEER Database: Type of Chemotherapy
Conclusions by authors:

Chemotherapy dose
• Even though older adults tolerate and receive lower doses, they still derive benefit
• Need to develop definitive guidelines for chemotherapy dose modification in older adults
Decision-making in the Clinic
• Communication is key
• Consider medical, psychological, and social issues: – Pain, impaired breathing, or fatigue from thoracotomy. – Debility due to smoking-related illness– Depression – Lung cancer related social stigma– Nicotine withdrawal – Social support- family, friends, caregivers.
• The elderly, are more susceptible to the toxic adverse effects of chemotherapy.
• More likely to die of something other than lung cancer than a younger patient with similar stage disease
• What are their goals for themselves?
“Isn’t it a bit unnerving that doctors
call what they do “practice”?”
George Carlin
A GA-based approach
Can Geriatric Assessment help identify those at greatest risk of
chemotherapy toxicity?
Ideal Tool to Risk Stratify
• Identification of vulnerable older adult
• To stratify by toxicity risk for cytotoxic therapy
• Outcomes depend on not just age but other
factors:
• Comorbidity,
• Physiologic function,
• Nutrition
• Functional status
• Social support
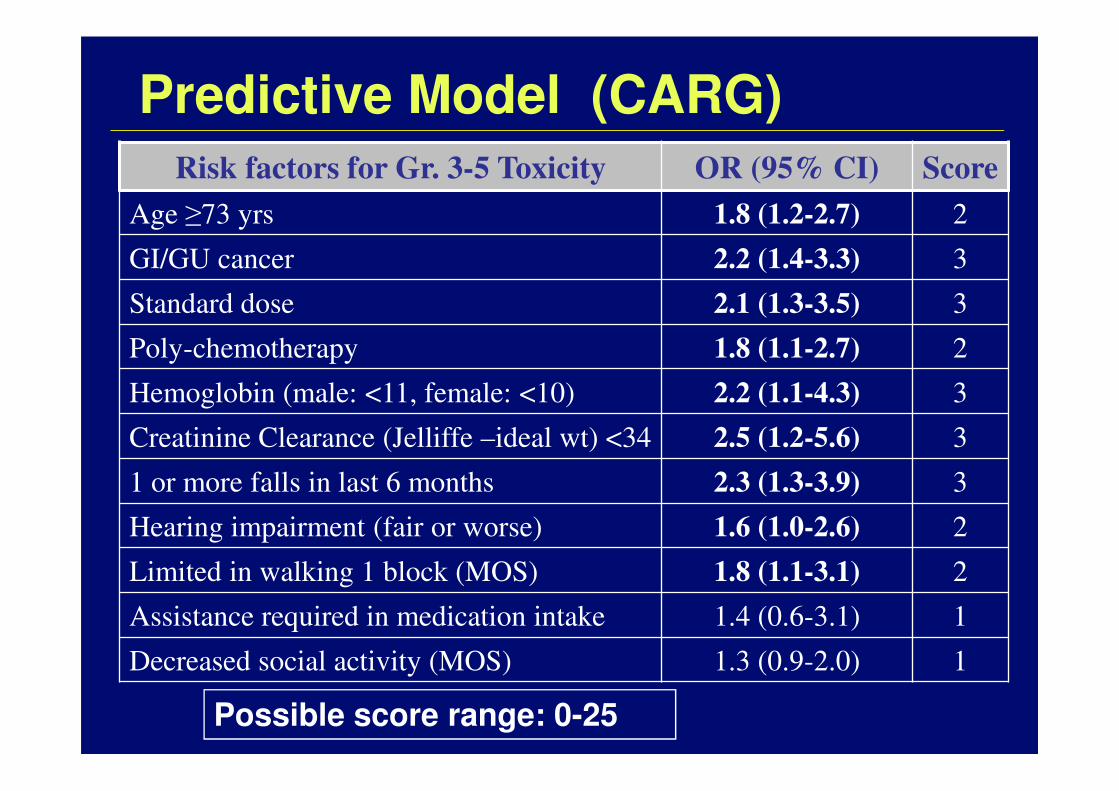
Predictive Model (CARG)
Risk factors for Gr. 3-5 Toxicity OR (95% CI) Score
Age ≥73 yrs 1.8 (1.2-2.7) 2
GI/GU cancer 2.2 (1.4-3.3) 3
Standard dose 2.1 (1.3-3.5) 3
Poly-chemotherapy 1.8 (1.1-2.7) 2
Hemoglobin (male: <11, female: <10) 2.2 (1.1-4.3) 3
Creatinine Clearance (Jelliffe –ideal wt) <34 2.5 (1.2-5.6) 3
1 or more falls in last 6 months 2.3 (1.3-3.9) 3
Hearing impairment (fair or worse) 1.6 (1.0-2.6) 2
Limited in walking 1 block (MOS) 1.8 (1.1-3.1) 2
Assistance required in medication intake 1.4 (0.6-3.1) 1
Decreased social activity (MOS) 1.3 (0.9-2.0) 1
Possible score range: 0-25
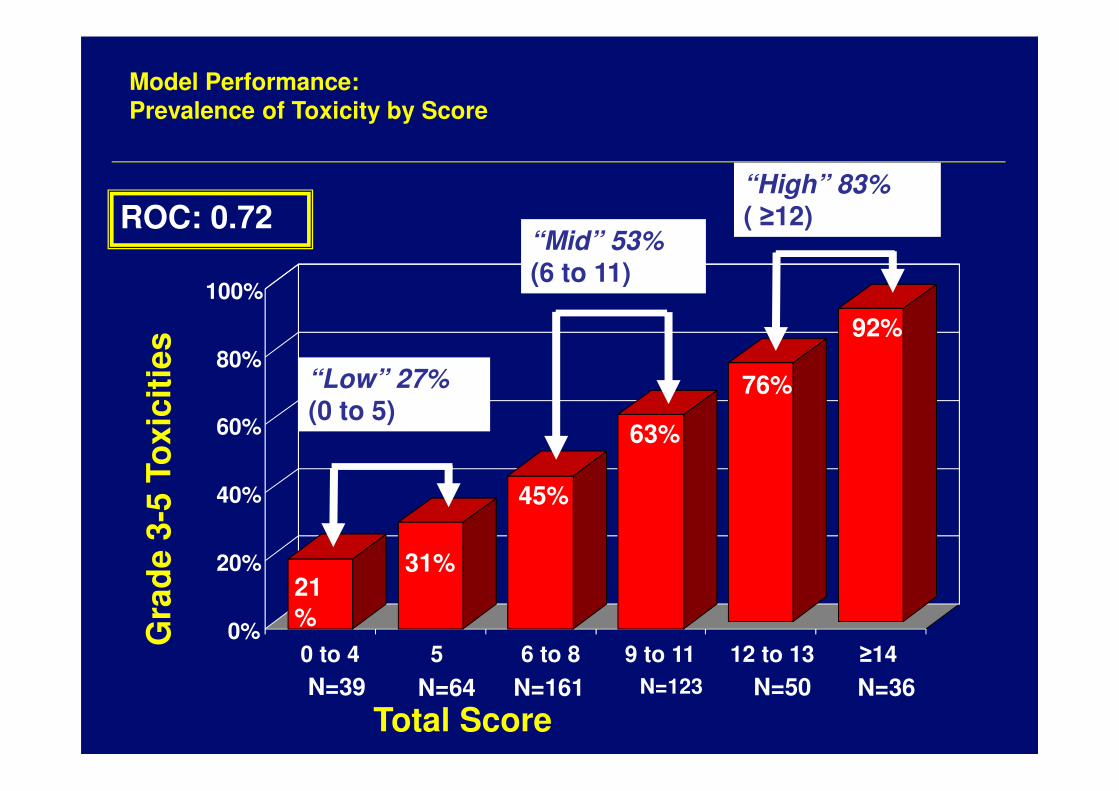
Model Performance:Prevalence of Toxicity by Score
Gra
de
3-5
To
xic
itie
s
Total ScoreN=39 N=64 N=123 N=36N=50N=161
0%
20%
40%
60%
80%
100%
0 to 4 5 6 to 8 9 to 11 12 to 13 ≥14
“Low” 27%(0 to 5)
31%21%
“Mid” 53%(6 to 11)
45%
63%
“High” 83%( ≥12)
76%
92%
ROC: 0.72
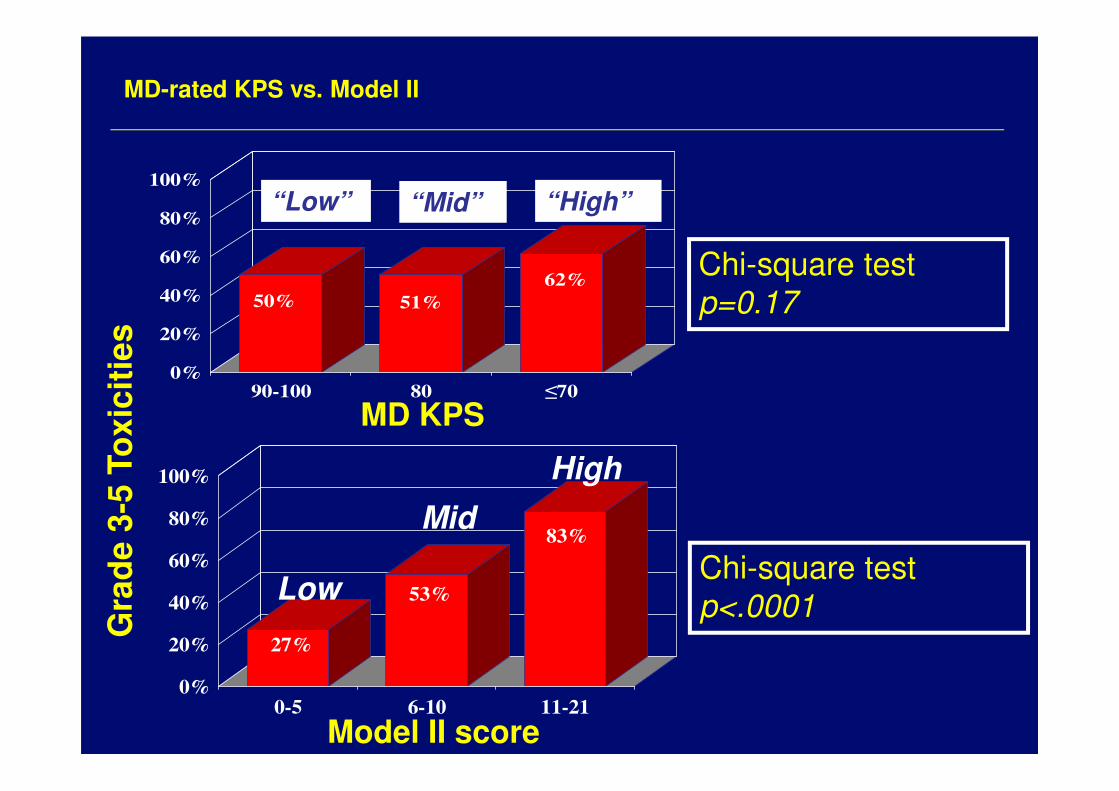
MD-rated KPS vs. Model II
50% 51%
62%
0%
20%
40%
60%
80%
100%
90-100 80 ≤70
“Low” “High”“Mid”
Chi-square test
p<.0001
Chi-square test
p=0.17
27%
53%
83%
0%
20%
40%
60%
80%
100%
0-5 6-10 11-21
Low
Mid
High
Gra
de
3-5
To
xic
itie
s
Model II score
MD KPS
Future Directions
• Use of GA to guide adjuvant treatment. – While the “fit elderly” may be offered the same therapies as
younger patients, for the vulnerable elderly, alternative treatment strategies need to be explored.
• Study the role of non-cisplatin based regimens in the older adults
• Lower dose and altered schedule of cisplatin
• Care of octagenerarians offers particular challenges. – No evidence thus far that ACT offers benefit.
– It is vital to discern the goals and expectations of the individual
Conclusions
– Assess interest in adjuvant chemotherapy.
– While absolute improvement in OS is 5.4% based on
meta-analysis, the magnitude of benefit it is likely lower
for older adults.
– If the patient is interested and at low risk for
chemotherapy toxicity consider cisplatin based therapy.
– If the patient has contraindication to cisplatin, consider
carboplatin based therapy.
– Data do not support the use of adjuvant chemotherapy
in those over age 80 years.
“The art of medicine consists of
amusing the patient while nature cures
the disease.”
― Voltaire
Thank You







