
Emergency Department (ED) Discharge to Die Pathway

How the pathway began
• National Statistics/Data (as previously mentioned by Dr Crede)
• Negative Personal and Professional experiences – Frustrated through own personal experience that patients ended up in ED when could have stayed home – felt need for a turnaround, discussed at appraisal
• Desire to respect patients dignity and dying wishes
• CQC recommendations • Initial Start date 2014

First Steps
• Initial meetings held with representatives from
• Palliative Care
• Front Door Response Team (FDRT)
• Emergency Dept. (Jayne and John)

Next Steps (3 year process) • Regular feedback meetings
• Obstacles that arose: • DNAR Forms – Yorkshire Ambulance Service brought in
• New Lorenzo system – District Nursing, Intensive Home Nursing brought in
• Pink Cards/pre-emptive medications – District Nursing, Pharmacy, Intensive Home Nursing brought in
• Availability of staff
• Initial pathway designed
• Further implementation issues identified
• Alterations made and pathway finalised
• This led to a 3 year process

Pathway

PATIENT IDENTIFIED TO BE IN THE LAST HOURS TO DAYS OF LIFE AND WISHES
TO DIE IN THEIR PLACE OF CHOICE
EMERGENCY DEPARTMENT DISCHARGE TO DIE IN HOURS PATHWAY. 0800-2000HRS
MEDICAL /NURSING STAFF USE SBAR GUIDANCE TO DISCUSS DYING WITH PATIENT AND THOSE
IMPORTANT TO THEM AND AS PART OF THE DISCUSSION ENSURE THEY KNOW:
THE LIKELY SCENARIO AS THEY ARE DYING I.E WHAT TO EXPECT
THERE MAY NOT BE PROFESSIONAL CARER SUPPORT AVAILABLE IMMEDIATELY. FRONT DOOR
RESPONSE TEAM WILL TRY TO SECURE CARERS AND DISTRICT NURSES (DNs) WILL VISIT IN
EMERGENCY. CHECK THAT FAMILY CAN COPE UNTIL CARERS AVAILABLE. AND IF THEY CANNOT
DELAY THE DISCHARGE
THAT IF PATIENT DIES IN THE AMBULANCE THEY WILL BE RETURNED TO ED (NOT HOME)
TO PHONE THE DNs IF THE PATIENT BECOMES SYMPTOMATIC AT HOME
WHEN THE PATIENT DIES NOT TO PHONE FOR AN AMBULANCE, PHONE THE DN OR GP
ENSURE A DNACPR IS COMPLETED AND DISCONTINUE SHEWS AND ROUTINE OBSERVATION
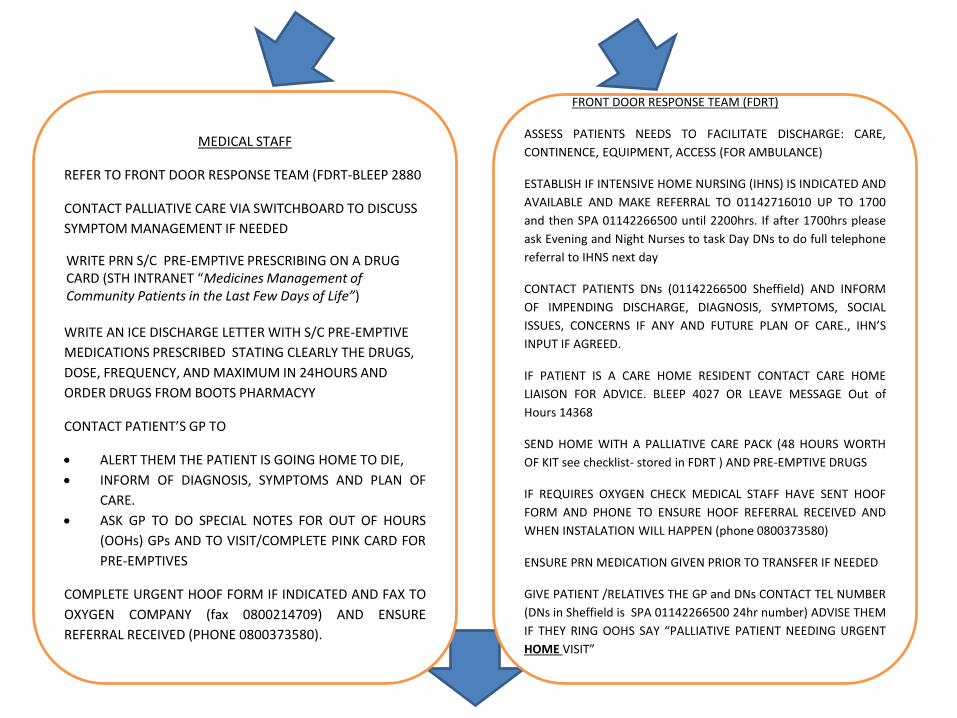
MEDICAL STAFF
REFER TO FRONT DOOR RESPONSE TEAM (FDRT-BLEEP 2880
CONTACT PALLIATIVE CARE VIA SWITCHBOARD TO DISCUSS
SYMPTOM MANAGEMENT IF NEEDED
WRITE PRN S/C PRE-EMPTIVE PRESCRIBING ON A DRUG CARD (STH INTRANET “Medicines Management of Community Patients in the Last Few Days of Life”)
WRITE AN ICE DISCHARGE LETTER WITH S/C PRE-EMPTIVE
MEDICATIONS PRESCRIBED STATING CLEARLY THE DRUGS,
DOSE, FREQUENCY, AND MAXIMUM IN 24HOURS AND
ORDER DRUGS FROM BOOTS PHARMACYY
CONTACT PATIENT’S GP TO
ALERT THEM THE PATIENT IS GOING HOME TO DIE,
INFORM OF DIAGNOSIS, SYMPTOMS AND PLAN OF
CARE.
ASK GP TO DO SPECIAL NOTES FOR OUT OF HOURS
(OOHs) GPs AND TO VISIT/COMPLETE PINK CARD FOR
PRE-EMPTIVES
COMPLETE URGENT HOOF FORM IF INDICATED AND FAX TO
OXYGEN COMPANY (fax 0800214709) AND ENSURE
REFERRAL RECEIVED (PHONE 0800373580).
FRONT DOOR RESPONSE TEAM (FDRT)
ASSESS PATIENTS NEEDS TO FACILITATE DISCHARGE: CARE,
CONTINENCE, EQUIPMENT, ACCESS (FOR AMBULANCE)
ESTABLISH IF INTENSIVE HOME NURSING (IHNS) IS INDICATED AND
AVAILABLE AND MAKE REFERRAL TO 01142716010 UP TO 1700
and then SPA 01142266500 until 2200hrs. If after 1700hrs please
ask Evening and Night Nurses to task Day DNs to do full telephone
referral to IHNS next day
CONTACT PATIENTS DNs (01142266500 Sheffield) AND INFORM
OF IMPENDING DISCHARGE, DIAGNOSIS, SYMPTOMS, SOCIAL
ISSUES, CONCERNS IF ANY AND FUTURE PLAN OF CARE., IHN’S
INPUT IF AGREED.
IF PATIENT IS A CARE HOME RESIDENT CONTACT CARE HOME
LIAISON FOR ADVICE. BLEEP 4027 OR LEAVE MESSAGE Out of
Hours 14368
SEND HOME WITH A PALLIATIVE CARE PACK (48 HOURS WORTH
OF KIT see checklist- stored in FDRT ) AND PRE-EMPTIVE DRUGS
IF REQUIRES OXYGEN CHECK MEDICAL STAFF HAVE SENT HOOF
FORM AND PHONE TO ENSURE HOOF REFERRAL RECEIVED AND
WHEN INSTALATION WILL HAPPEN (phone 0800373580)
ENSURE PRN MEDICATION GIVEN PRIOR TO TRANSFER IF NEEDED
GIVE PATIENT /RELATIVES THE GP and DNs CONTACT TEL NUMBER
(DNs in Sheffield is SPA 01142266500 24hr number) ADVISE THEM
IF THEY RING OOHS SAY “PALLIATIVE PATIENT NEEDING URGENT
HOME VISIT”
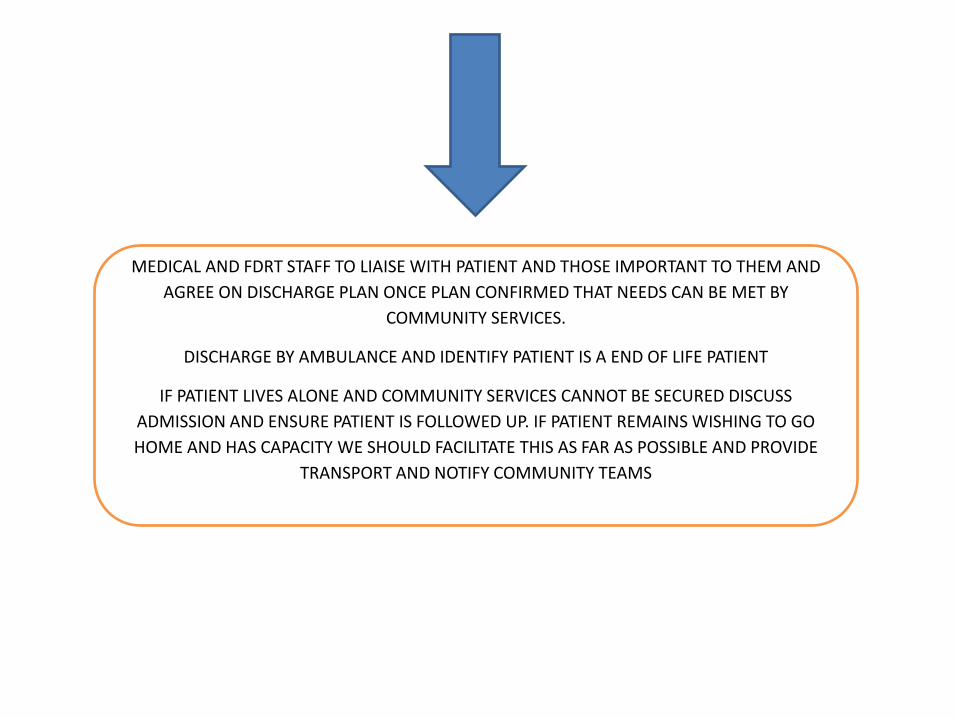
MEDICAL AND FDRT STAFF TO LIAISE WITH PATIENT AND THOSE IMPORTANT TO THEM AND
AGREE ON DISCHARGE PLAN ONCE PLAN CONFIRMED THAT NEEDS CAN BE MET BY
COMMUNITY SERVICES.
DISCHARGE BY AMBULANCE AND IDENTIFY PATIENT IS A END OF LIFE PATIENT
IF PATIENT LIVES ALONE AND COMMUNITY SERVICES CANNOT BE SECURED DISCUSS
ADMISSION AND ENSURE PATIENT IS FOLLOWED UP. IF PATIENT REMAINS WISHING TO GO
HOME AND HAS CAPACITY WE SHOULD FACILITATE THIS AS FAR AS POSSIBLE AND PROVIDE
TRANSPORT AND NOTIFY COMMUNITY TEAMS

DISCHARGE TO DIE OUT OF HOURS PATHWAY EMERGENCY DEPT. (AFTER 2000HOURS/WEEKENDS)
PATIENT IDENTIFIED TO BE IN THE LAST
HOURS TO DAYS OF LIFE AND WISHES TO
DIE IN PLACE OF CHOICE
MEDICAL/NURSING STAFF USE SBAR GUIDANCE TO DISCUSS DYING WITH PATIENT AND THOSE
IMPORTANT TO THEM. AS PART OF THE DISCUSSION ENSURE THEY KNOW:
THE LIKELY SCENARIO AS THEY ARE DYING I.E WHAT TO EXPECT
THAT IF PATIENT DIES IN THE AMBULANCE THE PATIENT WILL RETURN TO EMERGENCY DEPT. (NOT
HOME)
THERE MAY NOT BE PROFESSIONAL CARER SUPPORT AVAILABLE IMMEDIATELY. ED WILL TRY TO SECURE
CARERS AND DISTRICT NURSES (DNs) WILL VISIT IN EMERGENCY. CHECK THAT THEY CAN COPE UNTIL
CARERS AVAILABLE. AND IF THEY CANNOT DELAY THE DISCHARGE
TO PHONE THE DISTRICT NURSE IF PATIENT BECOMES SYMPTOMATIC AT HOME
WHEN THE PATIENT DIES NOT TO PHONE FOR AN AMBULANCE, PHONE THE GP/DISTRICT NURSE
ENSURE A DNACPR IS COMPLETED AND DISCONTINUE SHEWS AND ROUTINE OBSERVATION

MEDICAL/NURSING STAFF
REFER TO FRONT DOOR RESPONSE (FDRT-BLEEP 2880 (UP
UNTIL 2000)
CONTACT PALLIATIVE CARE ON CALL SPR VIA SWITCHBOARD
TO DISCUSS SYMPTOM MANAGEMENT IF NEEDED
WRITE s/c PRN PRE-EMPTIVE PRESCRIBING ON A DRUG CARD (STH INTRANET “Medicines Management of Community Patients in the Last Few Days of Life”)
CONTACT OUT OF HOURs GP COLLAB. (01143051412) TO
ALERT THAT THE PATIENT IS GOING HOME TO DIE
INFORM OF DIAGNOSIS, SYMPTOMS and PLAN OF CARE
AND REQUEST THEY ADD THIS INFO AS A SPECIAL NOTE
TO PATIENTS RECORDS.
ASK THE OOHs GP TO VISIT ED TO COMPLETE PINK
CARD FOR PRE-EMPTIVE DRUGS AND SUPPLY PRE-
EMPTIVE DRUGS FROM THE GP COLLABORATIVE DRUG
CUPBOARD (PALLIATIVE PACK)
COMPLETE URGENT HOOF FORM (ON INTRANET) IF
INDICATED AND FAX TO AIR PRODUCTS (fax 0800214709)
AND PHONE TO ENSURE REFERRAL RECEIVED (0800373580).
ED NURSING TEAM (FDRT BEFORE 1800)
ASSESS PATIENTS NEEDS TO FACILITATE DISCHARGE (CARE, CONTINENCE,
EQUIPMENT, ACCESS (FOR AMBULANCE)
CONTACT PATIENTS DISTRICT NURSES (01143051460) AND INFORM OF
IMPENDING DISCHARGE, DIAGNOSIS, SYMPTOMS, SOCIAL ISSUES,
CONCERNS IF ANY AND FUTURE PLAN OF CARE. IHN’S INPUT IF AGREED.
IF A CARE HOME PATIENT CONTACT CARE HOME DIRECTLY TO INFORM THE
PATIENT IS RETURNING. LEAVE MESSAGE FOR CARE HOME LIAISON TEAM
TO F/U NEXT DAY ext. 14368
ESTABLISH IF INTENSIVE HOME NURSING IS AVAILABLE AND MAKE
REFERRAL IF INDICATED. TEL 01142716010 UP TO 1700hrs AND THEN SPA
01143051460 UNTIL 2200hrs (if referred to IHNS after 1700hrs please ask
Evening and Night Nurses to task Day DNs to do full telephone referral to
IHNS next day
SEND HOME WITH A PALLIATIVE CARE PACK (48 HOURS WORTH OF KIT see
checklist) and PRE-EMPTIVE S/C DRUGS AND PINK CARD IF GP COLLAB
VISITED
IF REQUIRES OXYGEN CHECK MEDICAL STAFF HAVE SENT HOOF FORM AND
PHONE TO ENSURE HOOF REFERRAL RECEIVED AND WHEN INSTALATION
WILL HAPPEN (0800373580)
ENSURE PRN MEDICATION GIVEN PRIOR TO TRANSFER IF NEEDED
GIVE PATIENT/RELATIVE THE GP and DNs CONTACT TEL NUMBER (DNs in
Sheffield is SPA 01143051460 24hr number) AND IF THEY NEED TO RING
ADVISE THEY SAY “PALLIATIVE PATIENT NEEDS AN URGENT HOME VISIT”
SEND HOME PINK CARD AND DRUGS IF OOHS GP VISITED EDD

MEDICAL AND ED NURSING STAFF TO LIAISE WITH PATIENT AND
THOSE IMPORTANT TO THEM AND AGREE ON DISCHARGE PLAN
DISCHARGE BY AMBULANCE AND IDENTIFY PATIENT IS AN END OF
LIFE PATIENT

Reflection on how pathway worked
• Approximately 20 people have been discharged from the Emergency Department using the pathway.
• “Patients have the right to express their wishes about
where they would like to receive care and where they want to die. People who are approaching the end of life are entitled to high-quality care, wherever they're being cared for.” – ‘End of Life Care’ - NHS.UK
• Scenario

Patient Scenario
• Mr T presented to A&E with a 1 day history of dizziness, vertigo, photophobia and nausea on examination was found to have positive nystagmus Ct head showed a further right frontal haemorrhagic infarct. Initially was for transfer to the RHH stroke unit but Mr T declined this transfer and wanted to return home to die as he was in the terminal stage of his illness
• Mr T had a current diagnosis of a poorly differentiated adenocarcinoma of unknown primary with mid–line nodal disease. This was diagnosed following a stroke and a MI which prompted further investigations due to Mr T’s young age, long term prognosis was poor and for palliative support and care.
• Mr T was referred to FDRT for a fast track palliative discharge using the new palliative care pathway; an assessment was completed identifying Mr T’s care and equipment needs
• Referral made to Intensive home nursing for end of life care • Equipment hospital bed , etc. ordered from BRC • Referral made to DNS for palliative care and management of driver which was set up in ED • Liaised with GP/DN both verbally and electronically to inform that this gentleman was being sent
home to die • Obtained pre-emptive drugs and pink card • Comfort box given • A priority ambulance was organised due to being end of life • Using the pathway enabled team working throughout all professionals and services, using the
pathway enabled a timely save and smooth discharge meeting all the patients’ needs and wishes of not to be in hospital and die in his own home
• The discharge of Mr T that was successful and he was discharged home with the support of community services to die in his own home with his family.

Plan for the future
Apr-
Sept
Oct-
Mar
Grand
Total
NGH A&E 3 12 15
NGH AMU 173 234 407
NGH Frailty Unit 20 56 76
NGH Surgical Assessment
Centre 53 62 115
Grand Total 249 364 613
Pts Contacts Average
Hospital LOS
1909 11733 19.7 Pts Average Hospital
LOS
440 10.3
Patients seen within first 24 hours of admission March 2017 – March 2018 - ED Patients seen by Consultant
Plan to work alongside Palliative Care Consultants to reduce length of stay
HST Data - All Contacts HST Data - Seen On Day/ Next Day Of Hospital Admission
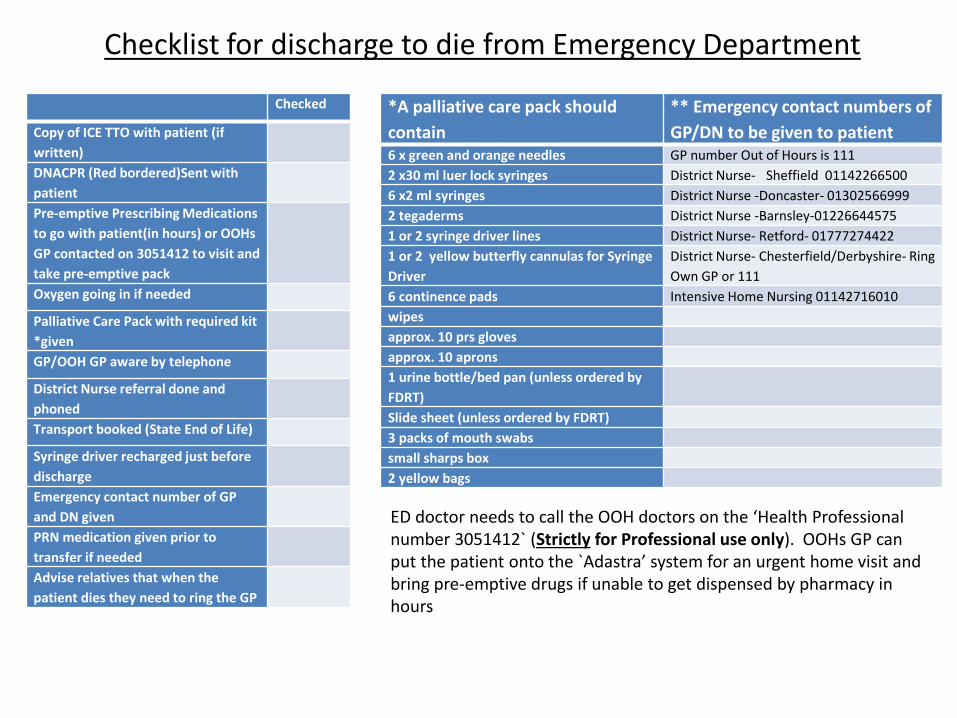
Checklist for discharge to die from Emergency Department
Checked
Copy of ICE TTO with patient (if
written)
DNACPR (Red bordered)Sent with
patient
Pre-emptive Prescribing Medications
to go with patient(in hours) or OOHs
GP contacted on 3051412 to visit and
take pre-emptive pack
Oxygen going in if needed
Palliative Care Pack with required kit
*given
GP/OOH GP aware by telephone
District Nurse referral done and
phoned
Transport booked (State End of Life)
Syringe driver recharged just before
discharge
Emergency contact number of GP
and DN given
PRN medication given prior to
transfer if needed
Advise relatives that when the
patient dies they need to ring the GP
*A palliative care pack should
contain
** Emergency contact numbers of
GP/DN to be given to patient 6 x green and orange needles GP number Out of Hours is 111
2 x30 ml luer lock syringes District Nurse- Sheffield 01142266500
6 x2 ml syringes District Nurse -Doncaster- 01302566999
2 tegaderms District Nurse -Barnsley-01226644575
1 or 2 syringe driver lines District Nurse- Retford- 01777274422
1 or 2 yellow butterfly cannulas for Syringe
Driver
District Nurse- Chesterfield/Derbyshire- Ring
Own GP or 111
6 continence pads Intensive Home Nursing 01142716010
wipes
approx. 10 prs gloves
approx. 10 aprons
1 urine bottle/bed pan (unless ordered by
FDRT)
Slide sheet (unless ordered by FDRT)
3 packs of mouth swabs
small sharps box
2 yellow bags
ED doctor needs to call the OOH doctors on the ‘Health Professional number 3051412` (Strictly for Professional use only). OOHs GP can put the patient onto the `Adastra’ system for an urgent home visit and bring pre-emptive drugs if unable to get dispensed by pharmacy in hours







