Anesthesia Awareness
Update on Fire Safety Issues in the Operating Room
Haven’t We Been Here Before?
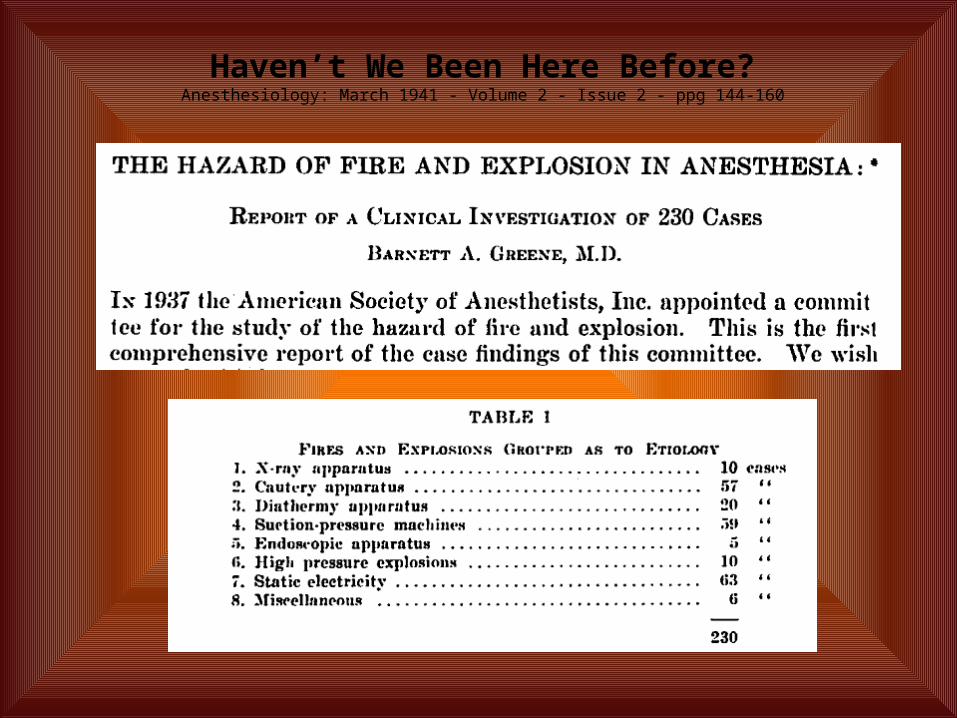
Haven’t We Been Here Before?Anesthesiology: March 1941 - Volume 2 - Issue 2 - ppg 144-160
Armour and Burtnett

Haven’t We Been Here Before?Electrical Burns During Laparoscopy
JAMA1973;226(12):1465
Intraabdominal Fire during Laparoscopic Cholecystectomy
Anesthesiology: October 1995 - Volume 83 - Issue 4 - pp 871-874
Airway Fire during Tracheostomy: Extubation May Be Contraindicated
Anesthesiology: December 1998 - Volume 89 - Issue 6 - p 1576–1578
Renewed Interest or Recurrence of Old Problem
AANA Journal August 2004Vol. 72, No. 4

Practice Advisory for the Prevention and Management of Operating Room Fires ASA Task Force On Operating Room Fires
EducationOR Fire DrillsPreparationPreventionManagement
Inquiring minds want to know.

Operating Room Fire Victim Awarded $1.3 Million in Ohio Medical Malpractice Lawsuit
Mole removed (2006)Trial in April 2009.

Before Post-burn
Woman Accidentally Set On Fire During C-Section
Haaretz newspaper reported. (2008)
OR Fire Occurs in Absence of Oxygen Enriched Environment: A Case ReportAPSF Volume 23, No. 1, Spring 2008
Obese adult patient Femoral distal bypass graft under GETAAlcohol-based solution may have
saturated skin folds over time producing vapors under the drapes.
A sterno-like fire burned the patients' leg after the vapors were exposed to the electrocautery.

Woman Sues Tulsa Doctor For Being Set On Fire During Surgery
NewsOn6-KOTVTulsa, OKMay 29, 2010

Post Accident (12/09) March 2010

Cathy Lake's mother, Catherine Reuter, 74, suffered second- and third-degree burns
Cleveland Clinic reports six operating room fires in past year, three patients injured.
The Cleveland Plain DealerMay 01, 2010

Dr. Toby Cosgrove, Cleveland Clinic CEO On April 30, officials at the
Cleveland Clinic confirmed that six fires had broken out in Clinic operating rooms in the 12-month period that ended in March.
“Patients suffered ‘superficial burns’ in three of the fires,” they said. "And no one was harmed in the other three.”

Dr. Toby Cosgrove, Cleveland Clinic CEO
“the three injured patients suffered superficial burns that resulted from ignition of flammable skin-preparation or other chemicals used during surgery.
Each of the six fires,” the hospital explained, “was started by an electrocautery device…”
How Are You To Know?
Where’s The Data?
HAC payment provision - July 2008
Foreign Object Retained After Surgery
Air Embolism Blood Incompatibility Stage III and IV Pressure
Ulcers Falls and Trauma
◦ Fractures◦ Dislocations◦ Intracranial Injuries◦ Crushing Injuries◦ Burns◦ Electric Shock
Manifestations of Poor Glycemic Control
Catheter-Associated Urinary Tract Infection
Vascular Catheter-Associated Infection
Surgical Site Infection◦ Coronary Artery Bypass Graft
(CABG) - Mediastinitis◦ Bariatric Surgery ◦ Orthopedic Procedures
Spine, Neck, Shoulder, Elbow Deep Vein Thrombosis/Pulmonary
Embolism ◦ Total Knee Replacement◦ Hip Replacement
Adverse Events in Hospitals: Public Disclosure of Information About Events Deputy Inspector General for Evaluation and Inspection, March 2008
State Adverse EventAgency for Healthcare Research and Quality(AHRQ)
Patient Safety OrganizationsCMS
Data Collecting Organizations
25 states and DC have reporting systems
72 PSOs
AHRQ creating and will maintain Network of Patient Safety Databases. (2012)

“Smart people learn from their mistakes.
Wise people learn from the mistakes of others. “
Norm Brodsky

APSFVideo

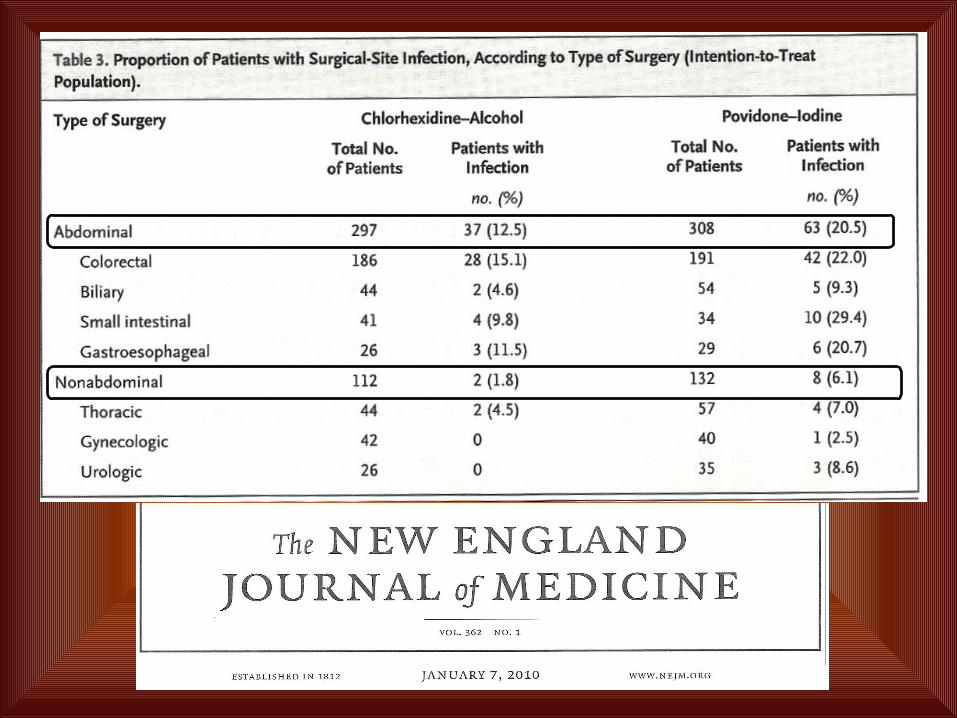
The ChloraPrep Advantage Rapid acting: Rapidly kills microorganisms versus free iodine,
which requires two minutes to begin antimicrobial activity. Persistent: Maintains antimicrobial activity for at least 48
hours compared to two hours for free iodine. Broad spectrum: Effective against microorganisms including
gram-positive and gram-negative bacteria, Methicillin-resistant Staphylococcus aureus (MRSA), Vancomycin-resistant Enterococci (VRE), Clostridium difficile, Acineobacter, and most viruses and fungi.
Active in protein-rich biomaterials: Remains active in the presence of blood, serum and other protein-rich biomaterials unlike traditional iodophors, which are neutralized.
Garcia R, Mulberry G, Brady A, Hibbard JS. Comparison of ChloraPrep and Betadine as preoperative skin preparation antiseptics. Poster presented at: 40th Annual Meeting of the Infectious Disease Society of America; October 25, 2002.

Characteristics of Antiseptics
Reviews in Obstetrics and Gynecology 2009 Fall; 2(4):212-221.


Br J Surg. 1976 Dec;63(12):981-3.Inflammable antiseptics and theatre fires.Briscoe CE, Hill DW, Payne JP
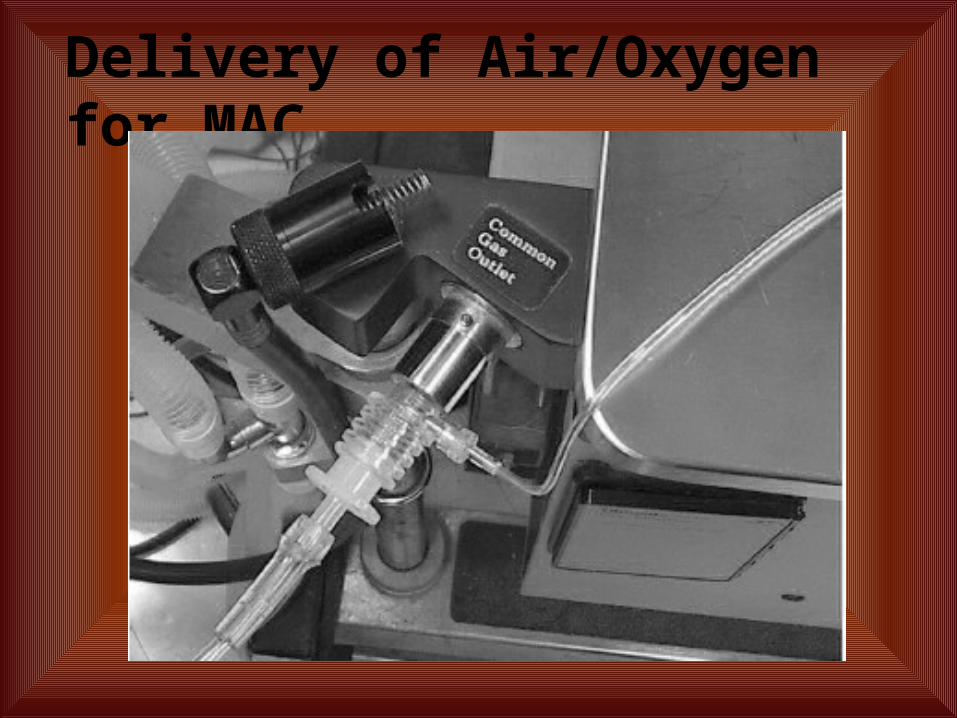
Delivery of Air/Oxygen for MAC
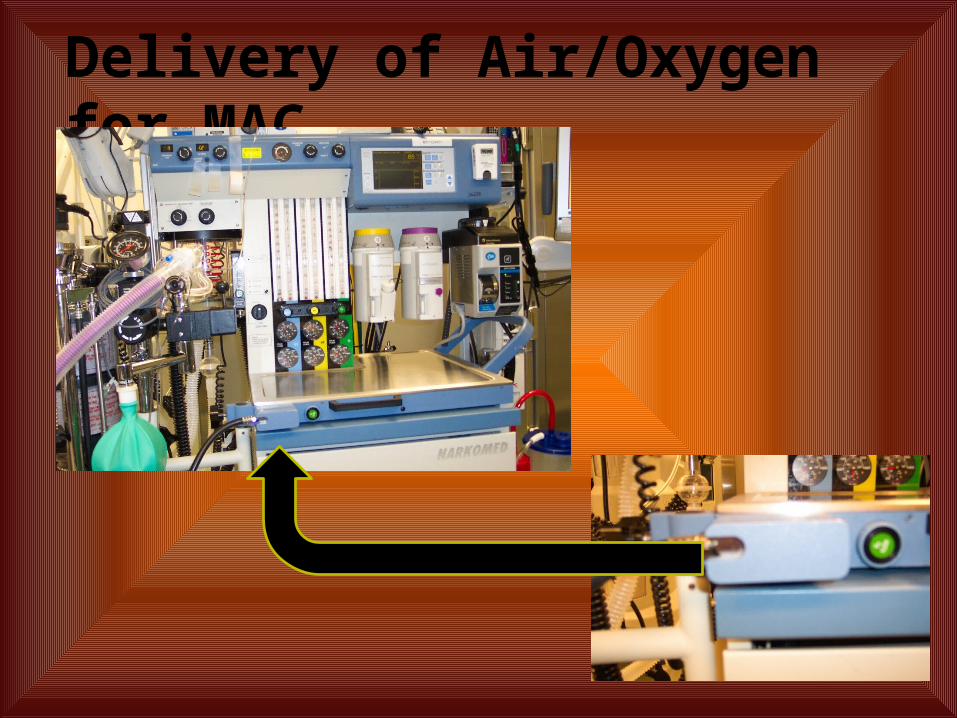
Delivery of Air/Oxygen for MAC

Delivery of Air/Oxygen for MAC
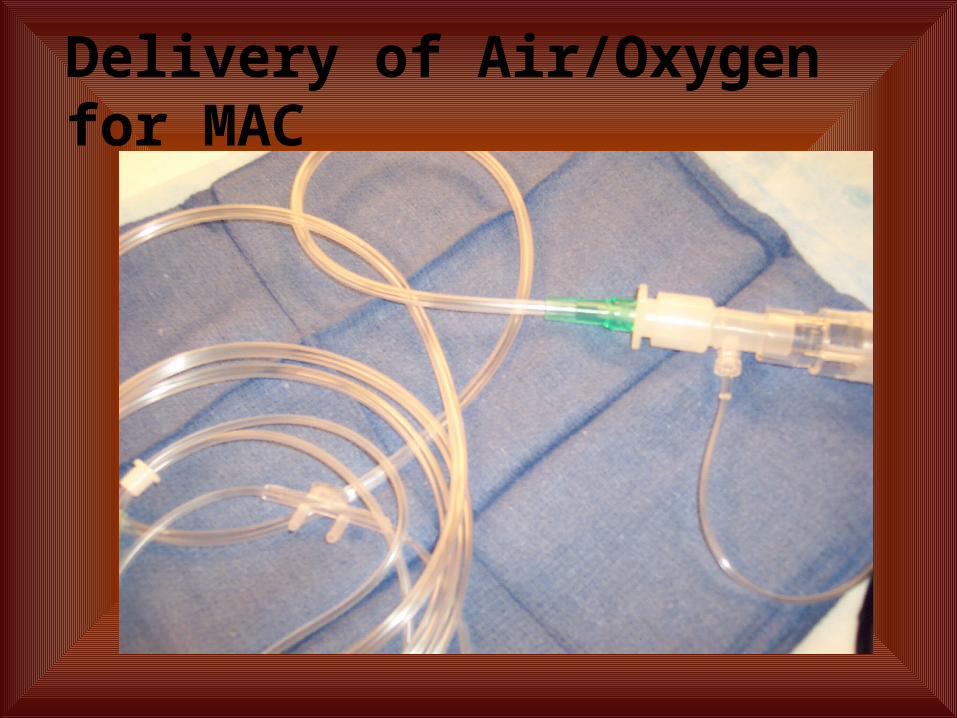
Delivery of Air/Oxygen for MAC

Delivery of Air/Oxygen for MAC

Flow Rates and FiO2
Oxygen Air FiO21 1 0.611 3 0.411 5 0.341 7 0.310.5 3 0.320.3 3 0.28

Prevention Thru Communication
Does potential exist?◦Alcohol-based prep◦FiO2 > 21%
◦ElectrocauterySteps taken to minimize
potential?◦No tenting of drapes◦Air flush or suction
Roles should potential become reality.◦Who does what
References Fires in the Operating Room and Intensive Care Unit: Awareness is the Key to Prevention, Rajnish Prasad,
MD, Zenaide Quezado, MD, Arthur St. Andre, MD, and Naomi P. O’Grady, MD; Anesth Analg 2006;102:172–4.
Joint Commission on Accreditation of Healthcare Organizations. Sentinel Event Alert. Issue 29, June 24, 2003.
ECRI. A clinician’s guide to surgical fires. Health Devices 2003;32:5–24. ECRI. Fires from oxygen use during head and neck surgery. Health Devices 1995;24:155–6. Barker SJ, Polson JS. Fire in the operating room: a case report and laboratory study. Anesth Analg
2001;93:960–5. Briscoe CE, Hill DW, Payne JP. Inflammable antiseptics and theatre fires. Br J Surg 1976;63:981–3. Bruley ME, de Richemond AL. Supplemental oxygen versus latent alcohol vapors as surgical fire
precursors. Anesth Analg 2002;95:1464. Wolf GL, Sidebotham GW, Lazard JL, Charchaflieh JG. Laser ignition of surgical drape materials in air, 50%
oxygen, and 95% oxygen. Anesthesiology 2004;100:1167–71. Aly A, McIlwain M, Duncavage JA. Electrosurgery-induced endotracheal tube ignition during tracheotomy.
Ann Otol Rhinol Laryngol 1991;100:31–3. Macdonald AG. A brief historical review of non-anaesthetic causes of fires and explosions in the operating
room. Br J Anaesth 1994;73:847–56. ECRI. Improper use of alcohol-based skin preps can cause surgical fires. Health Devices 2003;32:441–3. https://www.ecri.org/Press/Pages/Preventing_Surgical_Fires.aspx Department of Health & Human Services. Memorandum Report: Adverse Events in Hospitals: Public
Disclosure of Information about Events. March 12, 2008







