
Attachment and Psychotherapy: Implications from Empirical Research
Kenneth N. Levy, Ph.D.
Pennsylvania State Universityand
Joan and Sanford I. Weill Medical College of Cornell University
Early Development, Attachment, and Psychotherapy, Copenhagen, Denmark,
November 20th-22nd , 2008

Personality Disorders Institute (PDI)Joan and Sanford I. Weill Medical College of
Cornell University
• Otto F. Kernberg, MD, Director
• John F. Clarkin, PhD, Co-Director
• Frank Yeomans, MD• Armand Loranger, PhD • Paulina Kernberg, MD• Mark Lenzenweger, PhD
(Binghamton) • Eve Caligor, MD
• Ann Appelbaum, PhD• Monica Carsky, PhD• Catherine Haren, Psy.D.• Diana Diamond, PhD
(CUNY)• Pamela A. Foelsch, PhD• James Hull, PhD• Michael Stone, MD• Jill Delaney, M.S.W.

Laboratory for Research in Personality, Psychopathology, and Psychotherapy
• City University of New York– Kevin B. Meehan– Joseph S. Reynoso– Michal Weber– Komal Choksi
• Penn State– Lori N. Scott– Rachel H. Wasserman– Joseph E. Beeney– William D. Ellison
Funding and Support
• National Institute of Mental Health• Borderline Personality Disorder Research Foundation• National Association for Research in Schizophrenia and
Depression• American Psychoanalytic Association• International Psychoanalytic Association• Köhler Foundation • DeWitt Wallace Readers Digest Fund (Kernberg) • Department of Psychiatry, Weill Medical College• City University of New York, Dean’s Office• Research Foundation of the City University of New York • Pennsylvania State University• Social Science Research Institute

Attachment and Psychotherapy
• Although Bowlby was a psychiatrist. Psychoanalyst, and psychotherapist, much of the research on attachment theory has been carried out by developmental and social psychologists focusing on normative aspects of attachment.
• From its inception, however, Bowlby conceptualized attachment theory as relevant to both normal and psychopathological development.

Attachment and Psychotherapy
• Bowlby believed that attachment insecurity, although originally an adaptive set of strategies designed to manage distress, increases vulnerability to psychopathology, and can be linked to specific types of difficulties that arise.
• "the many forms of emotional distress and personality disturbance, including anxiety, anger, depression, and emotional detachment” (p. 5) which result from the disruption of those bonds

Attachment and Psychotherapy
• Bowlby also believed that attachment theory had particular relevance for psychotherapy.

Bowlby on Attachment and Psychotherapy
• The chief role of the therapist is “to provide the patient with a temporary attachment figure” (Bowlby, 1975, p. 191)
• the therapist’s first task is to “provide the patient with a secure base from which to explore both himself and also his relations with all those with whom he has made or might make, an affectional bond” (Bowlby, 1977; p. 421)

Bowlby: Five Key Tasks of Psychotherapy
• Establishing a secure base– which involves providing patients with a secure
base from which they can explore the painful aspects of their life by being supportive and caring;
• Exploring past attachments– which involves helping patients explore past and
present relationships, including their expectations, feelings, and behaviors;

Bowlby: Five Key Tasks of Psychotherapy
• Exploring the therapeutic relationship,– which involves helping the patient examine the
relationship with the therapist and how it may relate to relationships or experiences outside of therapy;
• Linking past experiences to present ones,– which involves encouraging awareness of how
current relationship experiences may be related to past ones;

Bowlby: Five Key Tasks of Psychotherapy
• Revising internal working models– which involves helping patients to feel, think,
and act in new ways that are unlike past relationships.

Bowlby: Five Key Tasks of Psychotherapy
• Revising internal working models– which involves helping patients to feel, think,
and act in new ways that are unlike past relationships.
• Providing a Safe Haven– Which to go in times of distress
• Can be a representational

Bowlby: Five Key Tasks of Psychotherapy
• Revising internal working models– which involves helping patients to feel, think, and
act in new ways that are unlike past relationships.
• Providing a Safe Haven– Which to go in times of distress
• Can be a representational
• Transference and countertransference dynamics (multiple contradictory IWM)
Attachment and Psychotherapy
• There are a number of ways that Attachment and Psychotherapy intersect– Attachment theory based interventions– Attachment organization as a moderator of outcome
(prognostic indicator)– Attachment organization as a prescriptive indicator– Psychotherapy process (therapist and patient in session
behaviors) as a function of attachment processes – Attachment organization as a moderator of
psychotherapy process– Change in attachment representations as outcome

Attachment Theory Based Interventions
• Many treatments implicitly use principles and techniques that are consistent with attachment theory – the establishment of a therapeutic alliance– the exploration of past and/or relational experiences,
the updating of self-views
• Until recently, few psychotherapies have been developed based directly on attachment theory principles

Attachment Based Child Interventions
• Baby Carrier Intervention (Ainisfeld et al., 1990)
• Home Visits (van den Boom, 1994)
• Intervention for high-risk pregnant women, (Korfmacher, Adam, Ogawa, & Egeland,1997)
• Watch, Wait, and Wonder (Cohen, Muir et al., 1999)
• Toddler-Parent Psychotherapy (Cicchetti, Toth, Rogosch, 1999; Toth et al., 2006)
• Circle of Security (Marvin, Cooper, Hoffman, & Powell, 2002; Hoffman et al., 2006)

Attachment Based Child Interventions
• Video Feedback Positive Parenting (Zeijl eta l., 2006)
• Prenatal Home Visits (Heinicke et al., 2006)
• Parent-Child Psychotherapy (Lieberman & Van Horn, 2004; Lieberman, Ippen, & Van Horn, 2006)

Ainisfeld et al., 1990: Attachment Security in SS
(n =46)

Attachment Based Adult Interventions
• Interpersonal Psychotherapy (IPT; Klerman, Weissman, Rounsaville, & Chevron, 1984)
• Mentalization Based Therapy (Bateman & Fonagy, 1999; 2001; 2008)
• Attachment Injury Resolution Model for Couples based Emotion Focused Psychotherapy (Johnson, 2004; Makinen & Johnson, 2006)

Bateman & Fonagy (1999)
• RCT of the effectiveness of 18 months of a non-manualized psychoanalytically oriented day hospitalization program compared with routine general psychiatric care for patients with BPD– significant improvement in depressive symptoms– better social and interpersonal functioning– significant decrease in suicidal and self-injurious acts– number of inpatient days
• Note:– TAU consisted of 2 hours of psychiatric care a month vs. 30
hours a week of PHP

Bateman & Fonagy (2008) Partial Hospital RCT: Patients at 5 yrs FU
0
10
20
30
40
50
60
70
80
90
Meet criteria(p<.0001)
No longeron
medication(p<.005)
Subsequenttreatment(p<.02)
Any suicideattempt(p<.001)
No self-harm
(p<.001)
MBT-PH TAU

Partial Hospital RCT: Patients at 5 yrs FU
0
2
4
6
8
10
12
14
16
18
20
totalscore(p<0.0001)
affectivedisturbance
(p<.01)
cognitivedisturbance
(p<.08)
impulsivity score(p<.001)
disturbedrelationship(p<.0.0003)
MBT-PH TAU

Partial Hospital RCT: % Attempting Suicide
0
10
20
30
40
50
60
70
80
90
100
Admission 12 months 24 months 36 months 48 months 60 months
Day Hospital
Control
*
* p < .05** p < .01*** p < .001
* ***
**
***
**
Follow -upTreatment
N=44NNT (18 months)=2.1NNT (36 months)=1.9NNT (60 months)=2.1
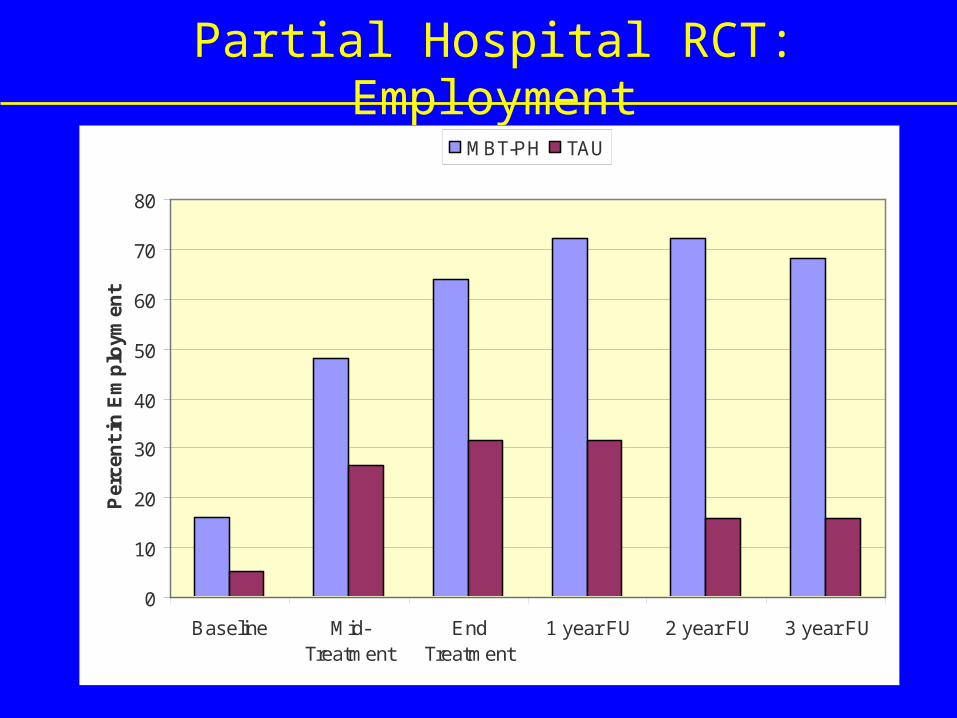
Partial Hospital RCT: Employment
0
10
20
30
40
50
60
70
80
Baseline Mid-Treatment
EndTreatment
1 year FU 2 year FU 3 year FU
Per
cen
t in
Em
plo
ymen
t
MBT-PH TAU

Partial Hospital RCT: GAF Scores
30
35
40
45
50
55
60
65
Baseline Endtreatment
18m FU 30 m FU 42 m FU
Mea
n G
AF
Sco
re
MBT-PH
TAU

Assessment of Attachment
• Adult Attachment Interview
• Reflective Function

Adult Attachment Interview • On the AAI individuals are asked to describe:
– Their parents generally, giving 5 adjectives with specific examples to back up general descriptions
– How parents responded when they were upset, ill, or in distress– The impact of early experience on current adult functioning
• The interview has the effect of “surprising the unconscious”
• Provides numerous opportunities for the speaker to elaborate upon, contradict or fail to support examples
• Can classify interviewees pattern of attachment as Secure, Preoccupied, Dismissive, Unresolved, or Cannot Classify

Assessment of Coherence (George, Kaplan, & Main, 1985)
• Coherence:– Quality—truthful, i.e., evidence for what was presented– Quantity—succinct, and yet complete– Relation—relevant to the topic at hand– Manner—clear and orderly
• Rated on 9 point scale, with 1= low coherence and 9 = high coherence, and score of 5 = cut-off for secure attachment
• Not related to IQ, or coherence of narrative discourse of non-attachment experiences (e.g., work)

Reflective Function
• The social cognitive and affective process of interpreting or making sense of behavior in oneself and others in terms of intentional mental states, such as desires, feelings, and beliefs.
• The capacity to reflect upon one’s own experience, whatever his or her attachment status.

Aspects of Reflective Function
• The explicit effort to tease out mental states underlying behavior– Accurate attributions of mental states to others.
• As suggested by differentiated views of events
• “My mother was good if I were physically hurt, except if she was frightened, then she wouldn’t be able to cope.”
– Recognition of diverse perspectives and points of view of the same event.
• “My mother had the habit of lifting her hand and slapping us, if we were naughty, or when she thought that we were naughty.”

Aspects of Reflective Function
• Recognizing the developmental aspects of mental states– Taking a developmental perspective
• “When we were little my father always seemed to have time for us and we would have so much fun together, but then as we got older he withdrew and had difficulty I think getting on with teenagers.”
• Mental states in relation to the interviewer – Acknowledging the separateness of minds
• “It must seem strange to you that I’m still upset, but it is almost exactly this time of year when the accident happened.”

Aspects of Reflective Function
• Awareness of the nature of mental states: – The opaqueness of mental states
• “I thought my mother felt resentful of us, but I’m not really sure if she felt that way herself” would be regarded as reflective whereas the statement, “One can never know what someone else thinks” would not.
– Awareness of the defensive nature of certain mental states:
• “You tend to blank things out that make you unhappy sometimes.”

Reflective Function(Fonagy, Target, Steele, Steele, 1998)
• The process of being able to reflect on experience and interpreting behavior in terms of intentional mental states, such as desires, feelings, and beliefs; represented by four dimensions:
– Awareness of the nature of mental states (“Well I think he felt obligated to do that because he felt guilty…”)
– Explicit efforts to tease out mental states underlying behavior (“…or at least that’s how it appeared, sometimes you feel different inside from how things appear.”)
– Recognizing developmental aspects of mental states (“It’s only as an adult that I understand this, as a child I was confused why he did that.”)
– Recognition of mental states in relation to the interviewer (“I’m not sure if that makes sense, should I explain further?”)

Reflective Function Scale (Fonagy, Target, Steele, Steele, 1998)
-1 Negative• Rejection, totally barren, grossly distorted, overly concrete,
unintegrated, or inappropriate RF
1 Disavowal, distorted/self-serving
3 Naive simplistic or over-analytic/hyperactive
5 Ordinary or inconsistent • model of mind is fairly coherent, but somewhat one dimensional
or simplistic
7 Marked
9 Exceptional • unusually complex, elaborate or original reasoning about mental
states



Correlation between Coherence and RF
• In non-clinical samples = .73 *** (Fonagy et al., 1991)
• In BPD sample pre-treatment = .48**
• In BPD sample post-treatment = .52**
• Note: *** significant at the .001 level.

Validity for RF
• Fonagy et al (1995) found that RF mediated the relationship between parental attachment security and infant attachment security in the SS.– insecurely attached parents with high RF were
more likely to have securely attached babies than insecurely attached parents with low RF.
Validity for RF
• Grienenberger, Kelly, & Slade, 2005 found that mother’s RF mediated the relationship between atypical maternal behaviors (e.g., affective communication errors, role/boundary confusion, intrusiveness) and attachment security in their infants.
Validity for RF
• Fonagy et al. (1996) found that among patients reporting abuse, those who scored low on RF were more likely to be diagnosed with BPD compared to those who were abused but scored high on RF. – Thus, high RF seems to be a possible buffer
against the development of BPD in individuals who have experienced abuse.

Wisconsin Card Sorting Task
• Measure of executive functioning,
• Specifically concept formation and the capacity shift attention (cognitive flexibility)
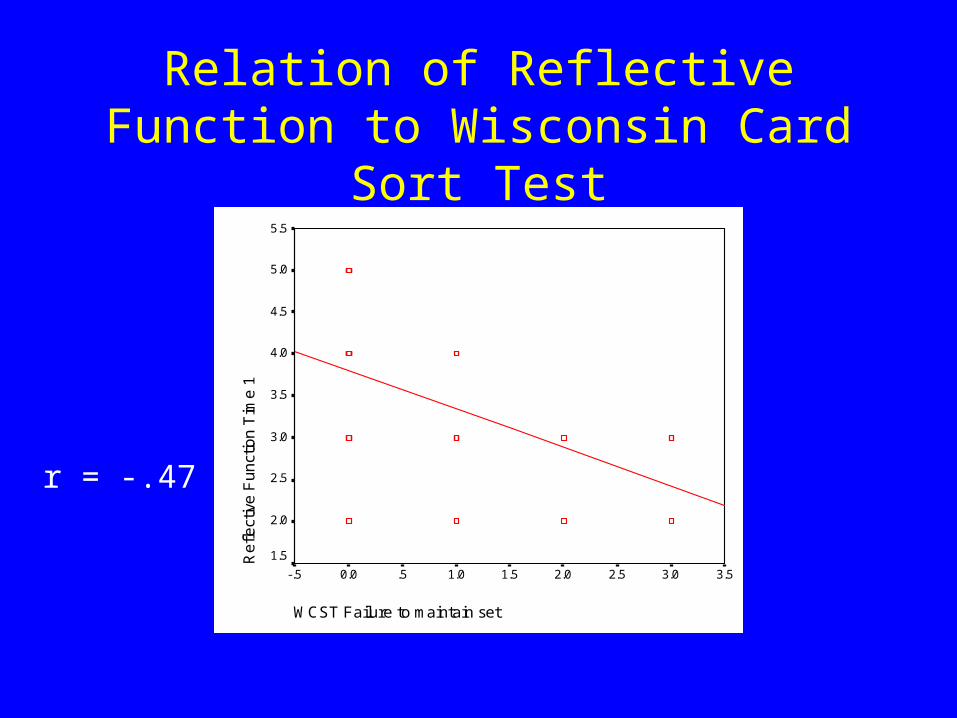
Relation of Reflective Function to Wisconsin Card Sort Test
WCST Failure to maintain set
3.53.02.52.01.51.0.50.0-.5
Re
flect
ive
Fu
nct
ion
Tim
e 1
5.5
5.0
4.5
4.0
3.5
3.0
2.5
2.0
1.5
r = -.47


3078

3078

1367


1637


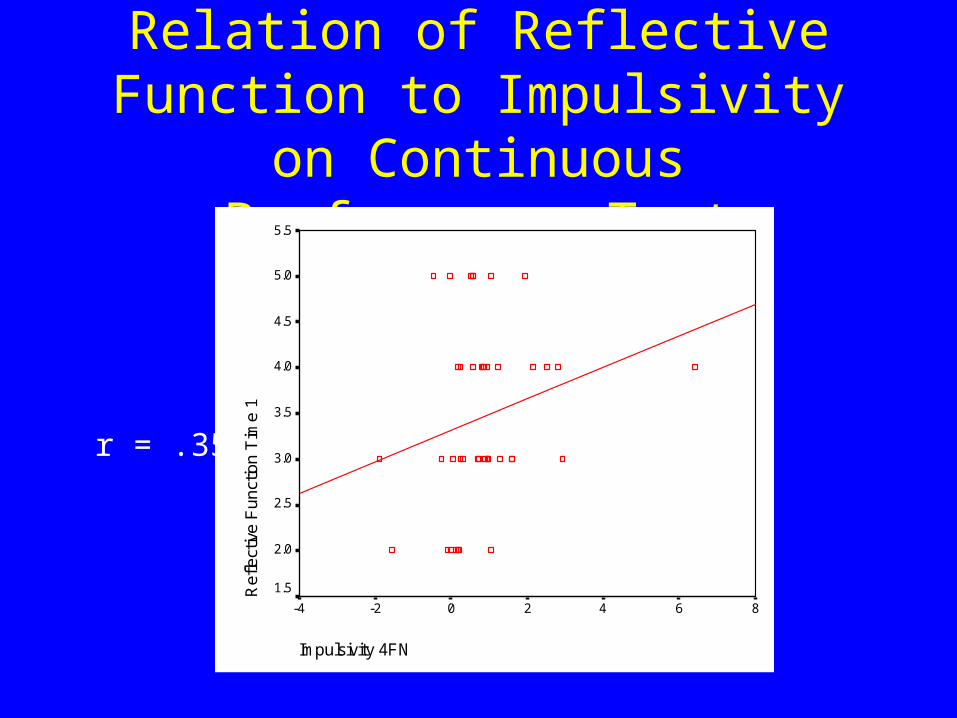
Relation of Reflective Function to Impulsivity on Continuous
Performance Test
Impulsivity 4FN
86420-2-4
Ref
lect
ive
Fun
ctio
n T
ime
15.5
5.0
4.5
4.0
3.5
3.0
2.5
2.0
1.5
r = .35
Attachment Moderates Likelihood of Being in
Psychotherapy
• Riggs et al. (2002) examined attachment and history of psychotherapy in 120 middle-class women. – dismissing women ↓ report a history of
psychotherapy– disorganized ↑ report a history of individual
psychotherapy – secure women ↑ report a history of couples
therapy.

Attachment as a Moderator of Outcome
• Dozier, 1990– Fs more cooperative with treatment– Ds associated with less help seeking, less self-disclosure, and
poorer treatment use
• Dozier, Cue, & Barnett, 1994; Tyrrell et al., 1999– Fs clinicians more likely to challenge patients’ own strategies
for relating – insecure clinicians tended to mirror the patients interpersonal
style– Better outcome when patient and therapist attachment
complementary vs. concordant.
Attachment as a Moderator of Outcome
• Fonagy et al., 1996– Ds attachment predicted better outcomes than E

∆ in GAF between Admission and Discharge as a Function of
Attachment
3641
25
31
20
36
051015202530354045
Admission Discharge
GA
F Sc
ore
F
E
Ds
Attachment as a Prescriptive Indicator
• McBride, Bagby, & Atkinson, 2006– attachment security moderate treatment
outcomes in a RCT of CBT and IPT for MDD– avoidant attachment predicted better response
to CBT than to IPT on all outcome measures, but anxious attachment did not predict different outcomes with the two treatments.

Attachment as an Outcome
• Fonagy et al., 1995
• Diamond et al., 2003; Levy et al., 2008
• Stovall-McClough & Cloitre, 2003
• Levy et al., 2006,
• Makinen and Johnson , 2006;
• Cicchetti et al., 1999; Toth et al., 2006
• Hoffman et al., 2006

Fonagy et al., 1995: Change in Security of Attachment (n =35)

Diamond et al., 2003: Change in Security of Attachment (n =10)

Change in Coherence and RF as a Function of Time: Pre-Post
Study
2.7
3.58
3.05
4.4
00.5
11.5
22.5
33.5
44.5
5
Yr. Prior Tx. Year
CoherenceRF
Coherence Paired t-test = -2.86, p < .02; RF paired t-test = -6.38, p < .001Levy et al., 2008

Stovall-McClough & Cloitre, 2003: Change in Unresolved
Status (n =18)

BPDRF-PDI RCTOverall Study Aims
To assess the efficacy of Transference Focused Psychotherapy (TFP) and Supportive Psychotherapy (SPT) compared with Dialectical Behavioral Therapy (DBT) for patients with Borderline Personality Disorder (Clarkin, Levy,
Lenzenweger, & Kernberg, 2004, Journal of Personality Disorders)

BPDRF-PDI RCTOverall Study Aims and Design
Examine efficacy of Transference Focused Psychotherapy Randomized 90 patients to one of three treatments: TFP, DBT,
and Supportive Psychotherapy (SPT) Experienced treatment cell leaders, experienced trained
therapists, supervised weekly• Patients clinically referred, highly comorbid (77% hx of MDD,
55% anxiety disorder, 33% eating disorder, and 38% substance use disorder), and highly traumatized (28% severe sexual abuse and ~50% some sexual abuse)
(Clarkin, Levy et al., 2004; 2007; Levy et al., 2006)

Treatments
Transference Focused Psychotherapy– Uses a treatment contract to set the frame and assist in the
containment of acting out behaviors, stipulates a sequence of treatment phases for interventions, emphasizes analysis of the transference for the integration of disparate representational models.
Dialectical Behavior Therapy (DBT) – emphasizes a balance between acceptance and change, skills
training in the context of validation Supportive Psychodynamic Psychotherapy (SPT)
– eschews transference interpretation and places primary emphasis on strengthening adaptive defenses; forming an alliance, providing reassurance and advice

Transference Focused Psychotherapy
• Modified Psychoanalytic Psychotherapy • Specifically for personality disorders• Structured twice weekly outpatient treatment• Based on Otto Kernberg’s Object Relations Model• Primary goal:
– reduce symptomatology and self-destructive behavior through integration of representations of both self and other (resolution of identity diffusion or stated differently the accomplishment of identity consolidation)

Overview of the TFP Treatment Model
• During the first year of treatment, TFP focuses on a hierarchy of issues:– Begins with a treatment contract
• the containment of suicidal and self-destructive behaviors• the various ways of interfering with the treatment
– In session, therapist follows dominant affect– Identifies and explicates recapitulation of dominant
object relational patterns, as they are experienced and expressed in the here-and-now of the relationship with the therapist (conceptualized as a transference relationship).
– Not about reconstructing childhood experience

Therapeutic Techniques
• Clarification– Of the patients subjective experience
• Confrontation– Tactfully pointing out discrepancies between what the patient
is saying at one time and another or between what they are saying and doing or saying and expressing
• Transference Interpretation– The therapist’s timely, clear, and tactful interpretations of the
dominant, affect-laden themes and patient enactments in the here and now of the transference, are hypothesized to integrate polarized self- and object representations.

Proposed Mechanisms of Therapeutic Change
• Integration of self concept• Integration of concept of significant
others• Integration of previously dissociated or
split off affect states with the result that affective experiences become enriched and modulated

Increased Differentiation and Integration
• Ability to think more flexibly and benevolently
• Impaired representations become transformed through new experiences
• Relationships:– infused with less aggression
– greater capacity for intimacy,
– increased coherence of identity,
– reduction in self-destructive behaviors,
– general improvement in functioning

Therapist Patient Sets frame via contract Experiences safe haven to express self
↓
Expression of affect includes actions and
interactions based on implicit OR dyads
Observes the action without judging or reacting
Tries to understand/explicate the OR underlying the actions, using
1 – Clarification
2 - Confrontation
3 – Interpretation Increases reflection
(these appeal for reflection &
address obstacles to it)
Further reflection, with Progress toward
increased contextualization integration
Increased modulation of affects

Telephone Inquires
(n = 337)
(294 clinical referrals, 28 non-
clinical, 15 not known)
Declined Interview
(n = 130)
Interviewed
(n = 207)
Refused Randomization
(n = 19)
Randomized
(n = 90)
TFP
(n = 31)
DBT
(n = 30)
SPT
(n = 29)
Met Criteria
Offered Randomizing
(n = 109)
Loss of Eligibility
(n = 0)
Did Not Meet Criteria
(n = 98)
Reason n
Did not meet BPD Criteria 30
Age 21
Substance Dependent 9
Concurrent Treatment 6
IQ 3
Bipolar Disorder 8
Eating Disorder 4
Psychotic Disorder 8
Scheduling Conflict 1
Dropped out 8
Levy, Critchfield, & Clarkin, in preparation

Treatment Cell Leaders
• Treatment cell leaders were very experienced in the modality that they were supervising
• Many years of experience practicing in their respective treatments
• Many years supervising in their respective treatments
• Acknowledged as nationally known experts• Published on their treatments
Therapists
• In each condition:– Chosen by treatment cell leader – Experienced practitioner in respective modality– Supervised weekly and monitored for
adherence and competence– Generally senior therapists, although ranged
from recent graduates to those with 30 years of experience

Patient Demographic Characteristics
• 90 Patients (83 Women and 7 Men)
• Mean Age = 30.9 (S.D. = 7.85)
• Marital status: – 7 (7.7%) Married, 11 (12.2%) Living with partner, 40 (44.4%) Divorced, 21 (23.3%) In
relationship
• Education:
– 4-year college degree (any college) 32.2% (63.3%)
• Employment:– Employed (fulltime) 64.4% (33.3%)
• Ethnicity/Race: – 67.8% Caucasian, 10.0% African-American, 8.9% Hispanic, 5.6% Asian, 3.3 %
mixed ethnicity/race, 4.4% other

Patients Represented a Seriously Disturbed Cohort
• All clinically referred• Highly comorbid (77% hx of MDD, 55% anxiety
disorder, 33% eating disorder, and 38% substance use disorder)
• Highly traumatized (28% severe sexual abuse and ~50% some sexual abuse)
• A third of the patients began cutting by age 12• Not selected based on intelligence or
analyzability!
TFP Outcome• Primary Outcome Variables
– Significant improvement in TFP and DBT; but not in Supportive:
• Suicidality – Significant improvement in TFP and SPT
• Anger and Impulsivity– Significant improvement only in TFP group:
• Assault• Secondary Outcome Variables
– Significant improvement in all three groups:• Depression, Anxiety, Social Relations, GAF
– Significant improvement only in TFP group:• Irritability

Distribution of 5-Category Attachment Status Time 1
5%15%
30% 32%
18%
0%
20%
40%
60%
80%
100%
Time 1
SecurePreoccupiedDismissingUnresolvedCannnot Classify
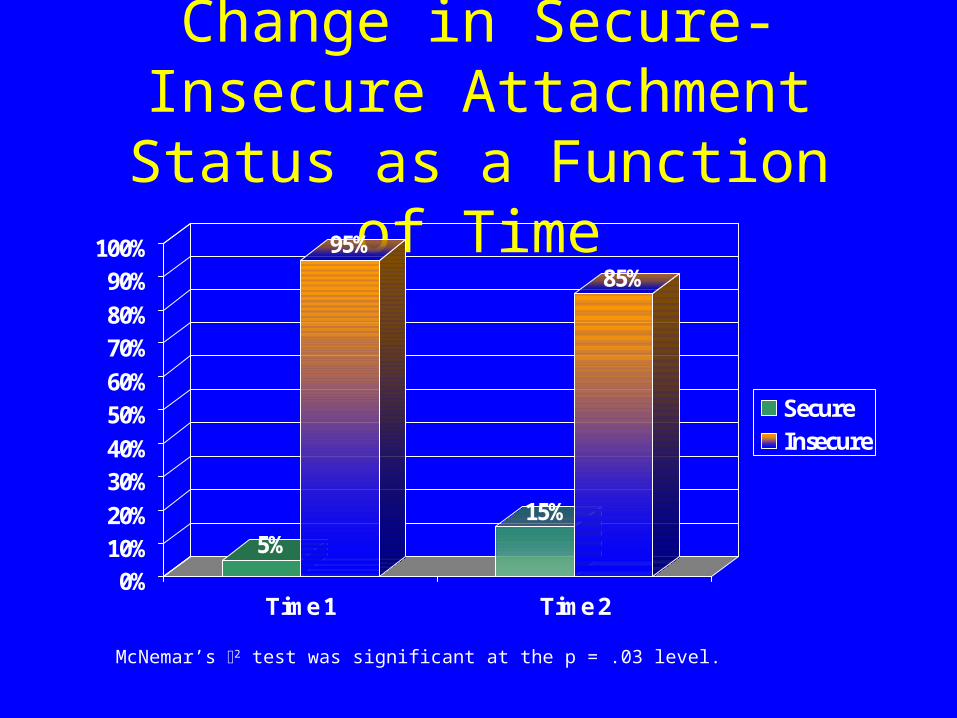
Change in Secure-Insecure Attachment Status as a Function
of Time
5%
95%
15%
85%
0%10%20%
30%40%
50%60%
70%80%
90%100%
Time 1 Time 2
SecureInsecure
McNemar’s 2 test was significant at the p = .03 level.

Change in Coherence as a Function of Time and Treatment
2.5
2.7
2.9
3.1
3.3
3.5
3.7
3.9
4.1
4.3
4.5
Coherence T1 Coherence T2
TFPDBTSPT
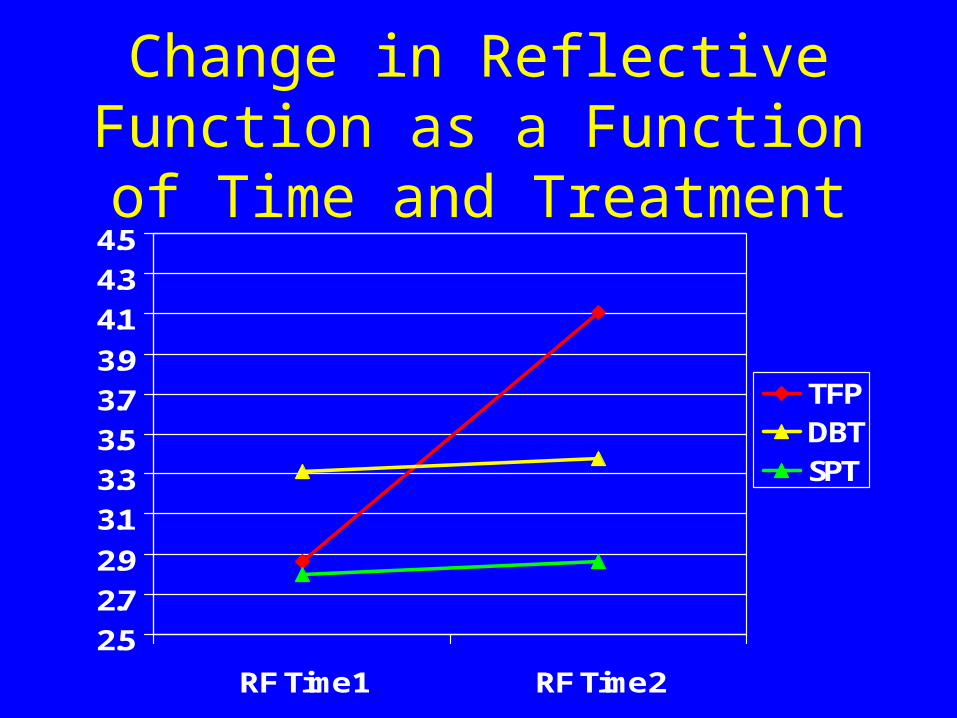
Change in Reflective Function as a Function of Time and
Treatment
2.5
2.7
2.9
3.1
3.3
3.5
3.7
3.9
4.1
4.3
4.5
RF Time 1 RF Time 2
TFPDBTSPT

Change in Resolved-Unresolved Attachment Status as a Function
of Time
67%
33%
79%
21%
0%10%
20%30%
40%50%
60%70%
80%90%
100%
Time 1 Time 2
ResolvedUnresolved

Dropout as a Function of Treatment Condition and Reflective Function
• Survival Analysis – Treatment Condition and RF as covariates
• Is there differential dropout across treatments as a function of RF?– e.g., are patients with low RF retained better in
certain treatments?
• RF at three levels:– Severely Impaired, Impaired, Average

Survival analysis on the Dropout criterion with Tx Condition and RF
• RF moderates relationship between Treatment Condition and Dropout– Average: When RF was within the average range, there were no
significant differences across treatments with respect to dropout• TFP = SPT = DBT
– Impaired: Significantly more dropout for individuals in DBT than TFP (Wilcoxon Statistic=.4.61, df=1, p<.03) and SPT (Wilcoxon Statistic=8.81, df=1, <.003).
• TFP<DBT=SPT
– Severely Impaired RF: Significantly more dropout in DBT than TFP (Wilcoxon Statistic=3.82, df=1, p<.05), while the differences between SPT and other treatments were non-significant.
• TFP<DBT, SPT ns

Dropout in Average RF Group

Dropout in Impaired RF group

Dropout in Severely Impaired Group

Specific Aspects of TFP that may Increase Mentalizing
• Focus on the object relation dyads– Explore mental state of other and self– The nature of mental states– Reduces rigidity about knowledge of other
peoples minds – Model and encourage patient to think about
mental states– Move beyond empathizing by also offering a
different, yet experientially appropriate representation (contingent and marked)
Specific Aspects of TFP that may Increase Mentalizing
• Clarification– Initiates self-exploration– Identifies differences in perspective
• Confrontation– Bids for self-reflection– Brings into awareness disparate information
and illustrates the defensive nature of certain mental states

Specific Aspects of TFP that may Increase Mentalizing
• The Transference Interpretation– timely, clear, and tactful interpretations of the
dominant, affect-laden themes and patient enactments in the here and now of the transference
• Mentalization emotion-laden content• Awareness of the defensive nature of certain mental states• Assists patient in elaborating on emotional state that may
have led to the enactment
• are hypothesized to integrate polarized representations of self and others

Clinical Observations
• Cannot Classify– E/Ds
• Derogations in angry preoccupied passages
– Pseudo Secures (F/E/Ds or Ud/F)• Mildly coherent in the provision of believable episodic
memories, but may show below threshold idealization, derogation, lack of recall, passivity, or angry preoccupation
• however, episodic memories are often belied by a self-serving quality with positive wrap-ups, lack of true valuing of relationships, and show little evidence compassion, affection, forgiveness, or freshness characteristic of secure narratives

Clinical Observations
• Cannot Classify– Time 1 CCs that move to E or D at Time 2
– Time 1 Es or Ds that move to CC at Time 2
• E classifiable transcripts with split representations– E1/E2
• passive, self-blaming passages (helpless/passive/avoidant)
• Angry preoccupied parent-blaming passages (hostile/controlling)

Clinical Observations
• Lyons-Ruth’s Hostile/Helpless distinction• Severe Splitting
– Rapid oscillations of object relation dyads– Splitting between caregiver– Mention of trauma at beginning of interview or
during five adjectives but no mention of it later in interview when topic is brought up by interviewer
– Idealization or denigration of interviewer

Clinical Observations
• Psychic Equivalence – Interview process or questions experienced as
the equivalent of past traumatic experiences

Therapist RF and Patient RF
• We assessed RF in our therapist in the small pre-post study using a modified patient-therapist AAI.
• Therapist RF re: patient generally high
• However, it did vary within therapist as a function of patient (but not patient RF!)
• Therapist tended to have lower RF with their Ds patients

Clinical Illustration
• Single, 32 year old, unemployed female• Many unsuccessful treatments• Over a number of years, increasingly isolated
in her apartment, gaining weight, rarely bathing
• Poor interpersonal relations rationalized because of her ethnic background
• No sexual relations ever, except 1 attempt by boyfriend leading to formal rape charges
Clinical Illustration
• Occasional self-cutting
• 3 brief hospitalizations; diagnosis Bipolar Disorder
• Background: Middle daughter in highly educated family; prestigious and dominant but tough father; master’s degree educated; series of jobs destroyed by interpersonal relations; not working for last few years

Clinical Illustration
• On the AAI:– CC/Ds2 (devaluing of attachment
experiences/derogating)/E2 (angry/conflicted)– RF = -1

Clinical Illustration
• Treatment: Controlling, dominant, dismissing therapist’s comments
• Condition for treatment: back to work, accepted after prolonged struggle
• Interpretation of relationship between hostile, grandiose, arrogant object and victim threatened with abandonment
• Generalization of this relationship to all interpersonal conflicts interpreted consistently
• Patient’s reflection on relationship with father coincident with emergence of positive transference while re-establishing relations with men

Clinical Illustration
• At the completion of one-year of treatment– Interested in apparently appropriate men; however,
relationships often unrequited– Volunteering in a occupational area that she thought
she might be interested– Taking non-matriculated graduate classes– Independent study evaluations: advance from
Reflective Functioning score of -1 to 6 by end of first year of therapy
– Medication: low dose of Neurontin at beginning, tapered off during year of treatment

Clinical Illustration
• At one-year follow-up– Effective improvement in work and
interpersonal relations– Good sexual relations with stable boyfriend– Attending graduate school in area consistent
with interests and capacities– Occasional struggles with feelings during times
of stress (she had a cancer scare)

Clinical Illustration
• At three-year follow-up– Continued improvement in work and
interpersonal relations• Married; good sexual relations; trying to get
pregnant• Working in high-level job consistent with her
interests and intellectual capacities
– Medication free– Affect: generally happy

Mentalization, Mindfulness, and Integrated Representation
• Slightly difference foci.
• Very similar in their hypothesized relationship to attentional control and affective instability.
• Allows appropriate distance (as opposed to defensive distance) from events, thoughts, and feelings.

Mentalization, Mindfulness, and Integrated Representation
• Thoughts, feelings, and events are not seen concretely or experienced literally as a rigid reality, but are experienced implicitly and sometimes explicitly as symbolic representations of experience, which one has some control over (i.E., One can shift one’s attention or think differently about an event).
• Events remain in perspective and lose their re-traumatizing capacity.

Thank YouFor more information please e-mail me at [email protected] and
visit the Laboratory for Personality, Psychopathology, and Psychotherapy website at http://levylab.psych.psu.edu
Also visit the Personality Disorders Institute website at
www.borderlinedisorders.com







