
Baby Buddy: reducing health inequalities
through digital parenting support
Chair: Dr Ann Hoskins @HoskinsAnn
Discussant: Prof. Mitch Blair @blair_mitch Imperial College London
Alison Baum OBE @AlisonBaum Best Beginnings
Dr Adrienne Gordon @AdrienneOz University of Sydney
Dr Sam Ginja @SamuelGinja representing the BaBBLeS research team
Dr Nicola Crossland, University of Central Lancashire
Dr Nicos Middleton, Cyprus University of Technology
Panel Discussion
CBC Conference 2018 - Behaviour Change for Health: Digital and Beyond
Parallel Session 6, 11.35am-12.40pm Symposium
@BestBeginnings @CyUniTech @imperialcollege @UniofNewcastle @UCLan @Sydney_Uni
@BabyBuddyApp

Baby Buddy Symposium: reducing health inequalities through digital parenting support
CBC Conference 2018 - Behaviour Change for Health: Digital and Beyond
The role of co-creation in the development
and implementation of the Baby Buddy
app, a complex digital health intervention Alison Baum OBE, CEO, Best Beginnings
Shabira Papain, COO, Best Beginnings
Nilushka Perera, Evaluation & Impact Lead, Best Beginnings
@AlisonBaum @ShabiraPapain
@BestBeginnings @CyUniTech @imperialcollege @UniofNewcastle @UCLan @Sydney_Uni @BabyBuddyApp

Baby Buddy
Our purposeful public health intervention in
the guise of a fun mobile phone app
Using technology to empower parents,
support relationships, enhance conversations
and help parents maximise their:
own physical and mental health
child’s potential


Our VisionIs that all children in the
UK have the
best start in life
Our AimTo inform and empower
parents and professionals
to reduce inequalities in
child health outcomes

Infant Mortality Eg: a baby born @Birmingham is 4x more likely to die in infancy than a
baby born @Bath 7.2 per 1,000 births in Birmingham v 1.8 in Bath. Av: 4.3
Breastfeeding at 6-8 weeks Eg: a 6 wk old baby @Wandsworth is c.4x more likely to be
breastfed than baby of same age born @Knowsley Wandsworth=77.4% Knowsley=19.9%.
Av: 55%
Smoking on delivery Eg: a baby born @Blackpool is > 13x more likely to be born to a
mother who smokes than a baby born @Westminster Blackpool=27.2% Westminster=2.1%.
Ave: 10.7
Obesity at 4-5 years old Eg: a 4-5 year old @Barking&Dagenham is c. 3x more likely to be
obese than a child born @Richmond Barking&Dagenham=14.2% Richmond=5.5%. Ave:
9.5%
Dental decay Eg: children in Leicester are > 3x more likely to have had dental intervention
compared to children living in West Sussex Leicester=53.2% West Sussex=14.2%. Ave:
27.9%
Good development at end of Reception. Eg: almost 2x the number of children @Lewisham
Why are we bothering? Is this work a priority?

facebook/bestbeginningscharity | @bestbeginnings | www.bestbeginnings.org.uk
Pre-
conception
A child’s
3rd
birthday
Innovation Collaboration Evidence
Opportunity

facebook/bestbeginningscharity | @bestbeginnings | www.bestbeginnings.org.uk
Collaboration is key & it is why we are well
placed to develop & deliver Baby BuddyParents of all backgrounds
Other charities
Front-line professionals
Royal Colleges, other professional bodies
Government departments
Academics
Commissioners & other funders who fund us nationally AND locally
People in the public eye

Our three stage iterative approach
@BestBeginnings @BabyBuddyApp
@AlisonBaum #PowerOfCollaboration

July 11
First
funding
application
2011
Focus
groups
with
young
parents
2011
Baby Buddy
stakeholder
group
formed &
regular
meetings
begin
2012
Seed funding
to develop
Baby Buddy
prototype
Jan 13
Appreciative
enquiry
2012
GSTT co-
create &
plan Baby
Buddy
embedding
2012
Market
research
group/phone
/interview
Jun & July 13
Blackpool co-
create & plan
Baby Buddy
embedding
Tender process
for app developer
Dec 13
Big Lottery
Fund grant
awarded
Jan 14
Market
research
group/phone
/interview
June 14
Beta
testing
with over
500
parents
&
professio
nals
July 14
Soft launch
on app
stores
Nov 14
Official
launch
2014
Embedding
in
Bradford,
Lewisham,
Leicester,
M’brough
Dec 14
Baby
Buddy
Stakeholder
& Editorial
Meeting
2015
Embedding
gets
underway in
more areas
March 15
Baby Buddy
wins AXA
PPP Health
Tech & You
Award
People-driven digital health and wellbeing



@BestBeginnings @BabyBuddyApp
@AlisonBaum #PowerOfCollaboration


The Baby Buddy Content Pipeline
Video content received
Written content received
Content review
BB
Content review
Editorial Board
Content review ParentPanel
Content added to
Baby Buddy
approved approved approved
Parent feedback
Healthcare professional feedback

Endorsing Organisations:
The Department of Health and
Awards we’ve won:Finalist for:
@BestBeginnings @BabyBuddyApp
@AlisonBaum #PowerOfCollaboration
Best App
for Patients
& Carers

Baby Buddy and its 70+ mental health films is helping to change the
conversation about mental health and encouraging women get the
support they need when they need it.
We’re proud to
be part of
#HeadsTogether


#MaternalMHMatters
#PowerOfCollaboration
@HelloMag
@Heads_Together
@BabyBuddyApp
HELLO! Magazine

Our three stage iterative approach
@BestBeginnings @BabyBuddyApp
@AlisonBaum #PowerOfCollaboration
Our three stage iterative approach

SMT meeting ‘Making it Work’
‘What do You Think?’ workshop(Service Users)
‘Content & Co-Creation’ workshop(Resource Leaders)
Project report
‘The Plan in Practice’ workshop
Local Launch
‘Progress, support & sharing’ (4 month progress meeting)
Progress report
Embedding into local care-pathways
@BestBeginnings @BabyBuddyApp
@AlisonBaum #PowerOfCollaboration

Aylesbury
Blackpool
Bradford
Coventry
County Durham & Darlington
Cheshire West & Chester
East Sussex
Hillingdon
Hounslow
Nottingham
Norwich
Sites where Baby Buddy has been/is being embedded
locally & independent evaluation sites:Northumbria
Lambeth
Leeds
Leicester
Lewisham
Luton
Middlesbrough and Redcar & Cleveland
Solent
Warrington
West Sussex
Southwark
= Three data-collection sites of the DH funded North of England impact study – UCLAN
= Five data-collection sites of BIG funded evaluation – BaBBLes consortium led by UWE
@BestBeginnings @BabyBuddyApp
@AlisonBaum #PowerOfCollaboration

Our three stage iterative approach
@BestBeginnings @BabyBuddyApp
@AlisonBaum #PowerOfCollaboration
Our three stage iterative approach
@BestBeginnings @BabyBuddyApp
@AlisonBaum #PowerOfCollaboration

In-app data on uptake usage & feedback

Types of users registering up to 08/02/2018
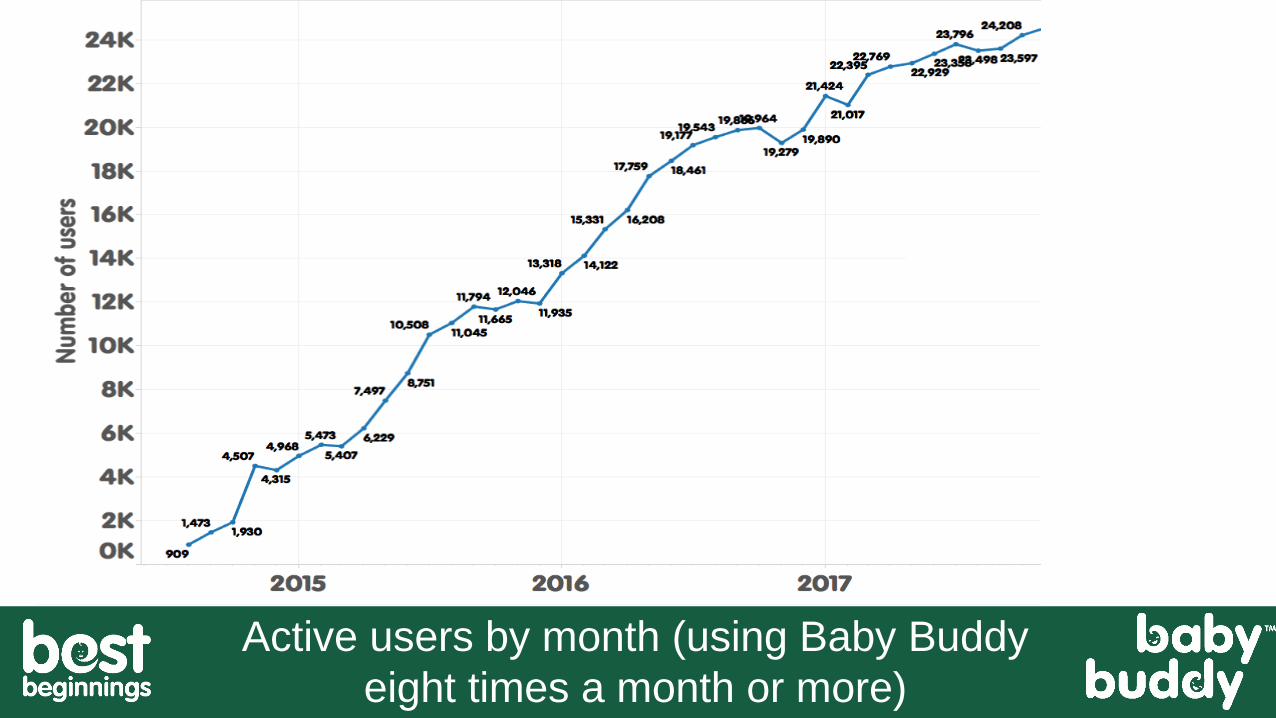
Active users by month (using Baby Buddy
eight times a month or more)

Confidence in the app knowing that the content has been extensively vetted by a
range of expert healthcare professionals with endorsements from an array of
organisations? 97%
Do you feel the Baby Buddy app would provide evidence-based/best practice-based
answers to questions that would be useful for parents-to-be or new parents? 94%
Recommend this app to parents-to-be or new parents with whom you work? 95%
Usefulness of the app for parents-to-be/new parents? 100%
Feedback from professionals using the Baby Buddy app up to
08/2/2018 completing the pop up surveys
@BestBeginnings @BabyBuddyApp
@AlisonBaum #PowerOfCollaboration

Pregnant women and new mums completing pop-up in-app
surveys to 31/08/17 report the following about Baby Buddy:
Easy to use (n=9757): >99%
Easy to understand (n=9707): >99%
Helps me get more out of my appointments (n=5549): 86%
Helps me look after my mental health (n=2,254): 87%
Helps me look after my physical health (n=2,277): 90%
Helps me feel closer to my baby (n=2955): 90%
Helps me feel more confident caring for my baby (n=2753): 98%
@BestBeginnings @BabyBuddyApp
@AlisonBaum #PowerOfCollaboration
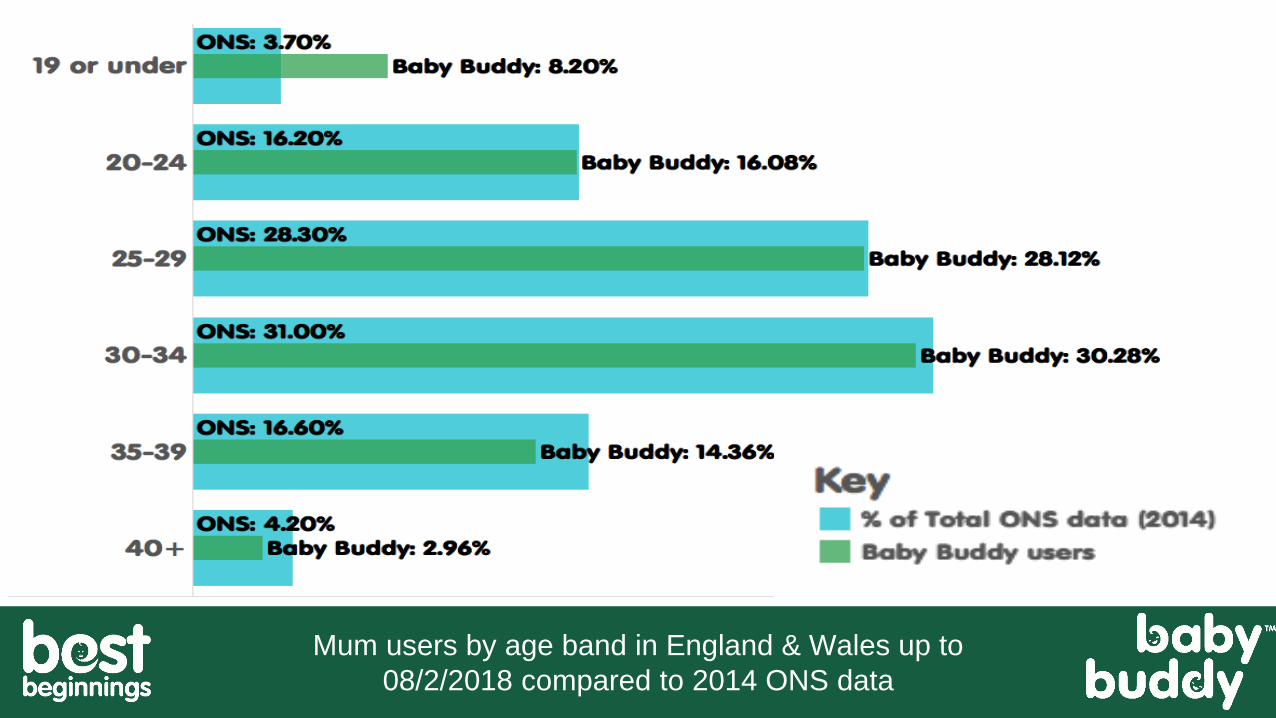
Mum users by age band in England & Wales up to
08/2/2018 compared to 2014 ONS data

Registrants of Baby Buddy by Ward in Leeds pre-embedding,
after first wave of embedding & again in Jan 2018

Baby Buddy sign-ups by local authority as a percentage to
its local birth cohort for six months (01/07/17-31/01/18)

We are working to secure funds to:
Increase awareness and downloads of current version through eg:
addition of more sharable content
Embed Baby Buddy within more areas across the UK
Collaborate to create international versions of Baby Buddy
Create Baby Buddy 2020 including:
more intuitive offering up of content
mood-tracking functionality
content for fathers & to support the couple relationship
interoperability
content for neonatal parents & those with multiples

Together we can make a
difference for future
generations
#PowerOfCollaboration
@bestbeginnings
@AlisonBaum

Baby Buddy Symposium: reducing health inequalities through digital parenting support
CBC Conference 2018 - Behaviour Change for Health: Digital and Beyond
Applying the Behaviour Change Wheel:
insights into the development of the
Breastfeeding Component of the Baby
Buddy App Dr Adrienne Gordon, Loretta Musgrave, Prof Caroline Homer
The University of Sydney
@AdrienneOz
@BestBeginnings @CyUniTech @imperialcollege @UniofNewcastle @UCLan @Sydney_Uni
@BabyBuddyApp

The University of Sydney Page 35
Breastfeeding - A healthy start to life
3
5

The University of Sydney Page 36
Breastfeeding - A healthy start to life
3
6
Victora CG, Bahl R, Barros AJ, Franca GV, Horton S, Krasevec J, Murch S, Sankar MJ, Walker N, Rollins NC et al:
Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387(10017):475-490.

The University of Sydney Page 37
Breastfeeding in UK
Bottom five countries after 12
months
Top five countries after 12
months
UK (0.5%) Senegal (99.4%)
Saudi Arabia (2%) The Gambia (98.7)
Denmark (3%) Malawi (98.3%)
Greece (6%) Guinea-Bissau (97.8%)
Canada and France (both 9%) Ethiopia (97.3%)
3
7
• 81% of mothers try breastfeeding
• 74% breastmilk for first feed
• 34% breastfeeding at six months
• 0.5% at 12 months
1 in 200 women breastfeeding at a year
Victora CG, Bahl R, Barros AJ, Franca GV, Horton S, Krasevec J, Murch S, Sankar MJ, Walker N, Rollins NC et al:
Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387(10017):475-490.

The University of Sydney Page 38
Rising use of smartphones in UK
Smartphone ownership in the UK 2012 – 2017 Statista

The University of Sydney Page 39
Smartphone as key information source
The rise of apps
– 5 Million apps available
– >165,000 medical and health apps
– Pregnant women high users of
Pregnancy Apps
– 73% use often in pregnancy
– 74% do not check validity of info
Ofcom Communications Market Report 2015, Statistia, 2017, Lupton 2016

Should we be App-rehensive?
• Validity and accuracy of information
• Equity
• Culturally appropriate
• Endorsement
• Stakeholder engagement
• Data privacy or security measures
• Concerns regarding pregnancy and fetal monitoring
• Health literacy
• Minimal high level evidence around efficacy
Lupton et al, 2016, Taki et al, 2015, Handley et al, 2016, Krishna et al, 2009,

The University of Sydney Page 41
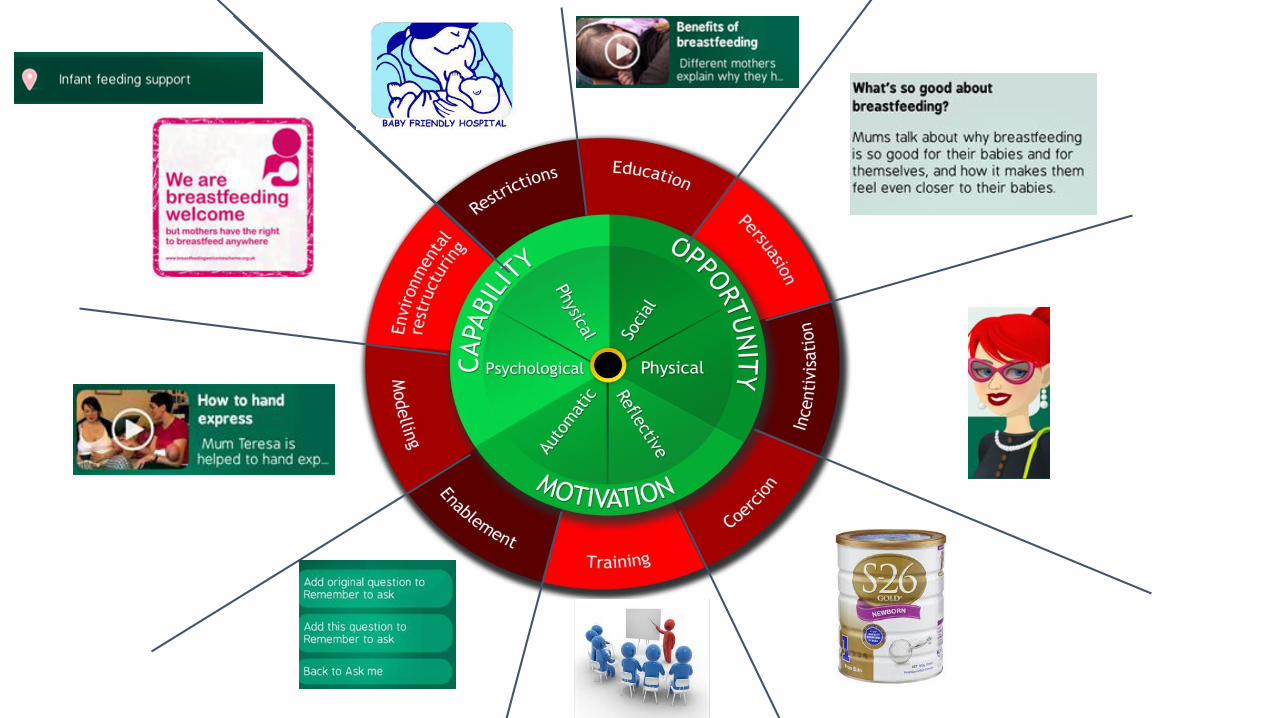
Aim– To systematically map the existing breastfeeding content of Baby Buddy
using the guidance for digital behaviour change interventions and the behaviour change wheel

The University of Sydney Page 42
Methods
– Information received from Best Beginnings about the development, context and activities undertaken with respect to breastfeeding component of Baby Buddy
– Application of APPEASE criteria for evaluation of DBCIs
– Breastfeeding component of Baby Buddy mapped to the Behaviour Change Wheel

From Bump to Breastfeeding Co-creation/Production Timeline
Driving change through collaboration
Mid-2007
4 nations
commit to
funding the
DVD
Aug 07
Market research
with parents
Sep 07
1st round table
meeting
Oct 07Filming begins Feb 08
Editing of DVD
Mar 08
Further
parental input
& 2nd round
table meeting
Mar 08Extra filming
Apr 08
Expert input
on final films
Nov 08
Official DVD
launch
July08
Baseline data
collected for
evaluation
Apr 09
Post intervention
evaluation begins
Oct 10
Evaluation
published
demonstrating
impact
Nov 10
films included within
DH/UNICEF/Start4Life
Breastfeeding Care
pathways
Over 2 million
copies distributed
2013
DH funded update
and re-voice

Context
DBCI Item Addressed Detail
Goals To inform and empower women of all socioeconomic
backgrounds to breastfeed for the first 6 months.
Opportunities Bump to Breastfeeding Resources, Key need secondary to UK
data, Smartphone use, Filmmaking, Big Lottery funding
Constraints Money, Time
Skills in tech – partnership with app developers
Staff – partnership with academic institutions for evaluation
Stakeholders Women, families, health professionals, colleges, health service
management, NHS
Collaborators Universities, app developers, other charities and pregnancy
support organisations
Risks Projected cost analysis, sustainability plan, staffing support
The University of Sydney Page 45
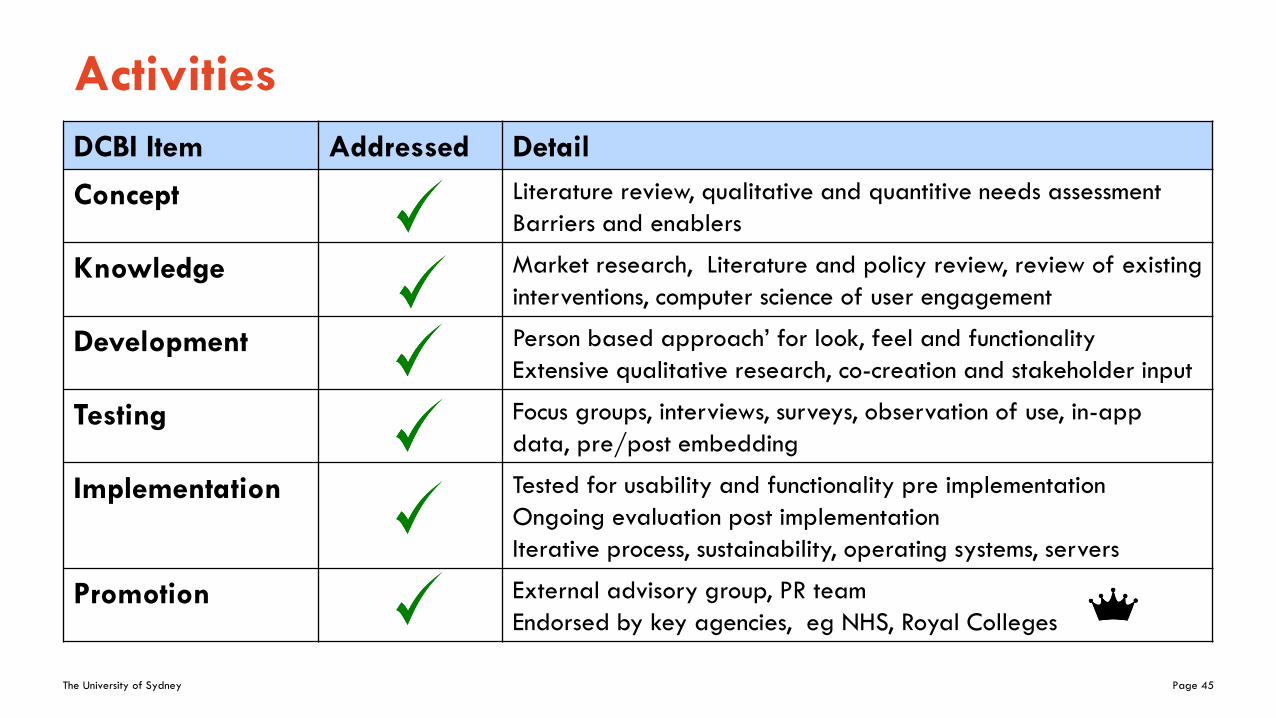
Activities
DCBI Item Addressed Detail
Concept Literature review, qualitative and quantitive needs assessment
Barriers and enablers
Knowledge Market research, Literature and policy review, review of existing
interventions, computer science of user engagement
Development Person based approach’ for look, feel and functionality
Extensive qualitative research, co-creation and stakeholder input
Testing Focus groups, interviews, surveys, observation of use, in-app
data, pre/post embedding
Implementation Tested for usability and functionality pre implementation
Ongoing evaluation post implementation
Iterative process, sustainability, operating systems, servers
Promotion External advisory group, PR team
Endorsed by key agencies, eg NHS, Royal Colleges

Focus on pre-conception to three years
Inform and empower parents to improve outcomes
Aim to reduce health inequalities in the UK
The University of Sydney Page 47
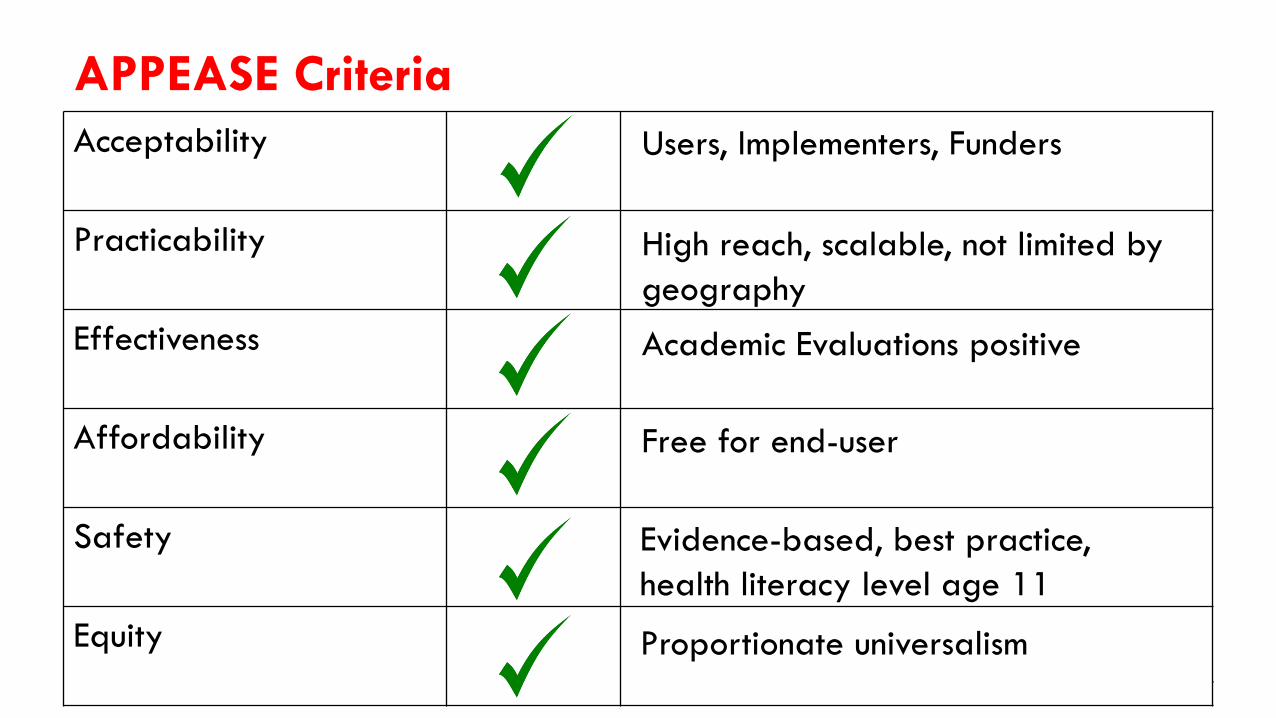
APPEASE Criteria
Acceptability
Practicability
Effectiveness
Affordability
Safety
Equity
Users, Implementers, Funders
High reach, scalable, not limited by
geography
Academic Evaluations positive
Free for end-user
Evidence-based, best practice,
health literacy level age 11
Proportionate universalism
The University of Sydney Page 48
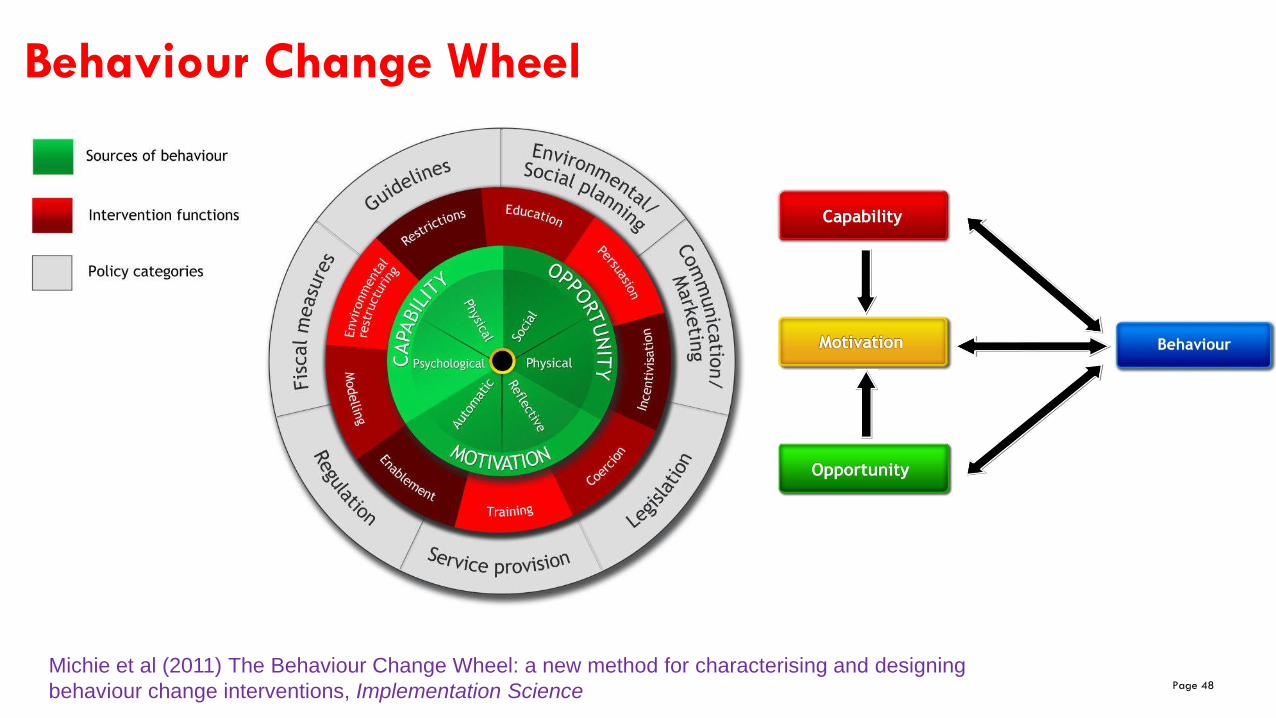
Behaviour Change Wheel
Michie et al (2011) The Behaviour Change Wheel: a new method for characterising and designing
behaviour change interventions, Implementation Science

The University of Sydney Page 49
Breastfeeding – understanding behaviour
Capability
Physical capabilitiy
Psychological capacity
1. Knowledge of how to attach and position the baby
2. Physical capability and skills to attach and position the baby
1. A lack of knowledge about the benefits of breastfeeding
2. Belief in ability to produce required amount of breast milk
3. Beliefs about the consequences of not breastfeeding
Motivation
Reflective motivation
Automatic motivation
1. Needing help with breastfeeding means there is a problem
2. Disappointment with self if unable to breastfeed
3. I don't need help - unrealistic optimism
1. Fear of failing at breastfeeds means offer bottle instead
2. Fear of being a bad mother
Opportunity
Physical opportunity
Social opportunity
1. Perception that breastfeeding is difficult due to the
unpredicatable nature of demand feeding
2. Provision of breastfeeding friendly social spaces

Breastfeeding – Intervention Functions

The University of Sydney Page 52
Breastfeeding – Policy Categories
Policy Categories
Service provision
Guidelines
Communication
Marketing
Links with evidence base, NHS Choices, current health
promotion campaigns

The University of Sydney Page 53
Conclusions
– Development of the breastfeeding component of Baby Buddy follows the principles on development of a DBCI and maps well to the BCW
– Using the structured process indicates room for improvement in future
– Evaluation of health outcomes will continue to inform Baby Buddy
– Ongoing input from stakeholders, key to relevance and sustainability
The University of Sydney Page 54
Take home messages
For the academics and researchers….– Retrospective application of BCW is possible and helpful
– Role for trials in DBCI to assess health outcomes
For practice and industry….– Sustainability of apps in competitive market
– Improved ability for consumer to assess app quality
Loretta Musgrave
Prof Caroline Homer
Dr Nathalie Kizirian
Alison Baum (UK)
Nilushka Perera (Sri Lanka)
The Team

Baby Buddy Symposium: reducing health inequalities through digital parenting support
CBC Conference 2018 - Behaviour Change for Health: Digital and Beyond
A cohort study to evaluate the
effectiveness of Best Beginnings Baby
Buddy phone app in EnglandDr Sam Ginja
Representing the BaBBLes research team
@BestBeginnings @CyUniTech @imperialcollege @UniofNewcastle @UCLan @Sydney_Uni
@BabyBuddyApp

Evaluation of Best Beginnings’ ‘Baby Buddy’ Phone App:
Bumps and Babies Longitudinal study (BaBBLeS)
Research team: Toity Deave (CI), Jane Coad (PI), Crispin Day (PI), Sally Kendall (PI), Raghu Lingam (PI);
Elizabeth Bailey, Samuel Ginja, Trudy Goodenough, Samantha Nightingale, Jane Smiddy,

https://www.bestbeginnings.org.uk/baby-buddy


Aim of the BaBBLeS cohort study
• Assess impact of the Baby Buddy app on maternal self-efficacy• Tool to Measure Parenting Self-Efficacy (TOPSE) (Bloomfield & Kendall, 2006)
• Secondary outcomes• Mental wellbeing
• Warwick-Edinburgh Mental Well-being scale (WEMWBS)
• Instructed use of the app
• Effect of outcome levels at 35 weeks gestation
Other measures
• Socio-demographic information
• Age, ethnic background, socio-economic deprivation (IMD), education, employment, relationship status
• Social support
• Multidimensional Scale of Perceived Social Support (MSPSS) (Zimet et al, 1988)
• Technology use
• Media and Technology Usage and Attitudes Scale (MTUAS) (Rosen et al 2013)
• Breastfeeding
• Intentions (baseline)
• Actual breastfeeding (post-birth)
• Childbirth experience
• Childbirth Experience Questionnaire (Dencker et al, 2010)
Methods• Design: Prospective cohort study
• Data collection time points:• 12-16 weeks gestation (baseline)• 35 weeks gestation• 3 months post-birth
• Participants: first-time mothers, aged 16+, able to provide consent
• Five recruitment sites in England• North West• West Yorkshire• West Midlands• London• East Midlands

Sample size calculation
• Aiming for ½ standard deviation difference on TOPSE scores between Baby Buddy users vs non-Baby Buddy users
• At 90% power % app download
Ratio* Total sample size (final sample)
12.5% 7 39214.3% 6 35016.7% 5 30620.0% 4 26525.0% 3 22833.3% 2 19250% 1 170
* Ratio of app users: non-app users

Participant pathway
Identified by booking at maternity unit –questionnaire pack given or sent in post
Invitation to participate, consent form and baseline questionnaire returned by post or online
Telephone Interviews, focus groups
Follow-up questionnaires
12
mo
nth
s

Baseline recruitment
62 (12.7%)
Inclusion: 16 yrs +, first-time mothers, 12-16 weeks gestation
Able to provide consent
488 women across all 5 sites
Site 4 Site 1 Site 3 Site 2 Site 5
66 (13.5%)
168 (34.4%)
53 (10.9%)
139 (28.5%)
Nested qualitative study from three sites: - 17 mothers interviewed- 20 healthcare professionals interviewed and took part in focus groups
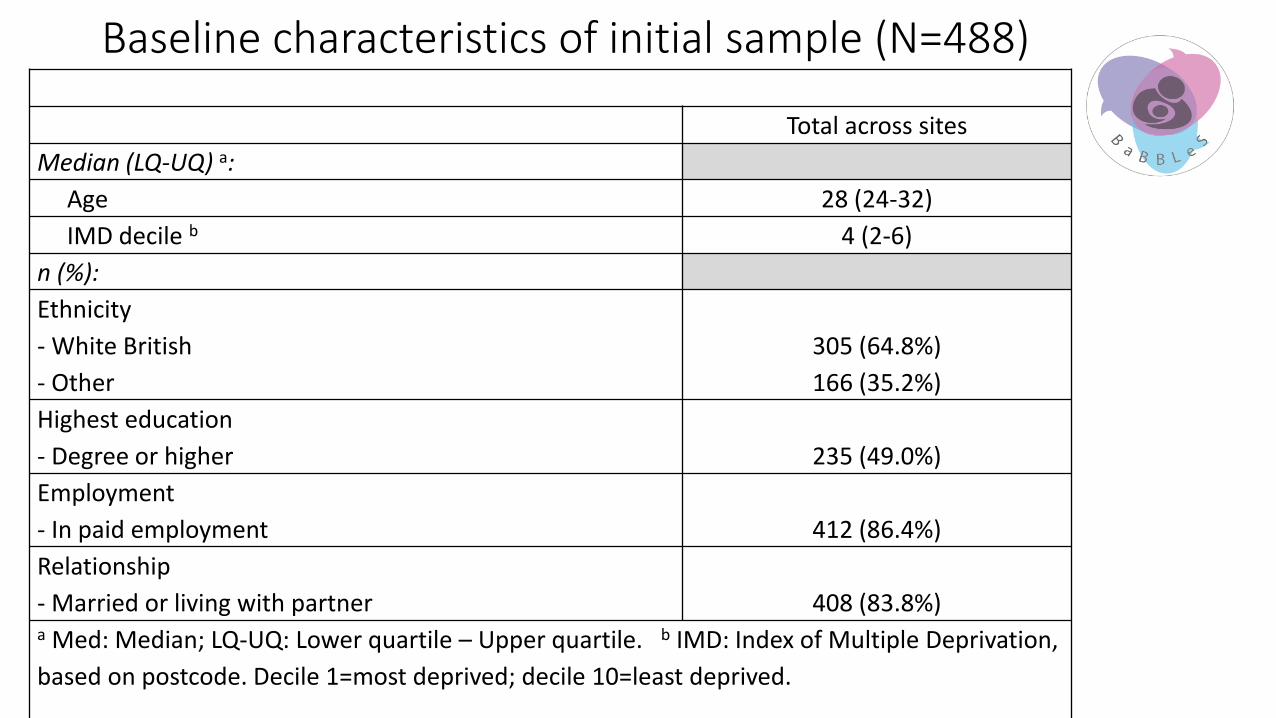
Baseline characteristics of initial sample (N=488)
Total across sites
Median (LQ-UQ) a:
Age 28 (24-32)
IMD decile b 4 (2-6)
n (%):
Ethnicity
- White British
- Other
305 (64.8%)
166 (35.2%)
Highest education
- Degree or higher 235 (49.0%)
Employment
- In paid employment 412 (86.4%)
Relationship
- Married or living with partner 408 (83.8%)a Med: Median; LQ-UQ: Lower quartile – Upper quartile. b IMD: Index of Multiple Deprivation,
based on postcode. Decile 1=most deprived; decile 10=least deprived.

Apps & Baby Buddy
Use of pregnancy and/or parenting apps at baseline
(N=488)
Variable n (%)
Uses and has used pregnancy/
parenting app(s)
355 (73.1%)
Uses or has used Baby Buddy app 51 (14.3%)

Challenges in evaluating app use
Challenge Action
Number of women using the app Recruit sufficient participants
Gaining access to in-app data Gain individual consent to look at specific app usage data
Matching in-app data with participants
Work with app developers re identifiers
Participants’ app usage Decide elements that constitute app usage
No data for time spent on app Number of elements used? Amount of usage?
Linking app usage to outcomes Compare high users with low users?

Thank you for your attention
Any questions?
Email: [email protected]
Chief investigator: [email protected]
Baby Buddy Symposium: reducing health inequalities through digital parenting support
CBC Conference 2018 - Behaviour Change for Health: Digital and Beyond
Evaluation of Best Beginnings
ResourcesDr Nicola Crossland, Dr Victoria Hall Moran & Dr Gill
Thomson
Maternal and Infant Nutrition & Nurture Unit
University of Central Lancashire
@BestBeginnings @CyUniTech @imperialcollege @UniofNewcastle @UCLan @Sydney_Uni
@BabyBuddyApp

North of England project
• Three sites in the North of England
• Best Beginnings parenting resources including Baby Buddy app embedded into care pathways

North of England project
• Three sites
• Embedding model
• Regional Facilitator from Best Beginnings working with stakeholders in each site over a six-month period
• Training workshops for senior staff and for nominated champions
• Resource Leaders
• Staff members working with pregnant and postnatal women
• Act as champions within their service
• Train colleagues

Aims of the evaluation
To understand how the embedding process worked
To identify barriers and facilitators
To understand women’s and professionals’ views
To look at the impact of the embedding and usage of the resources on
• breastfeeding rates.
• women’s attitudes and self-efficacy in relation to breastfeeding.
• parenting confidence
• mother–infant relationships
Evaluation design
Process evaluation study using:
• Observations of embedding workshops
• Interviews with key stakeholders (10 per site, 3 sites)
• Women’s survey (pre- and post-embedding) – >500 questionnaires per stage to women with a baby under 6 months
• Professionals’ survey (post-embedding) – distributed to maternity and early years staff

Survey participants
• Women (n=161 pre; n=192 post )• Most of the women who responded to the surveys were:• first-time mothers• aged 30+ years• White British• married/civil partnership/living with their partners• stayed in full-time education until 19+ years • employed in a paid capacity• No significant differences pre- and post-embedding
• Professionals (n=146 post)• 30+ years• female• White British

Key embedding facilitators
Resource Leaders
Awareness
Senior staffCommunication
between agencies
Feedback on app use
Fit with care pathways
• Yeah and I think it’s been received well by staff because it’s so easy to use the resources, because it fits in well with our care pathway, our booking appointments, we do talk about where to get information from so it’s a good opening into giving the leaflet that explains about the app, so I think it’s been well received by the staff and there hasn’t been any negativity about it being an added pressure. (Interview participant 6, Site Three)

Baby Buddy downloads
0
100
200
300
400
500
600
700
800
Site One Site Two Site Three
Number of Baby Buddy app registrations before and after embedding
Before embedding After embedding

Outcomes: Breastfeeding
The app reminds you about how important breastfeeding is and what a great thing you are doing for your baby.
(Women’s post-embedding survey 139, Site Three)
No statistically significant changes breastfeeding outcomes pre/post-embedding
Outcomes: Confidence
No change in women’s scores on the Parenting Sense of Competency Scale pre/post-embedding.
I love checking the app daily to see what hints/tips are there for today. It has given me ideas about my baby’s development and reassured me on numerous occasions. (Women’s post-embedding survey 156, Site Three)
I was amazed at how well the “Today’s Information” was matched to my baby's progress, it gave me confidence he was making good progress and gave me reassurance/new ideas. (Women’s post-embedding survey 26, Site One)
Outcomes: Relationships
There is a client who I knew previously, and she has had maternal mood concerns in the past which had affected how she interacted with her baby at times, and she hadn’t really before shown interest in the pregnancy. I talked about the App and she had actually gone on it and she had got a push notification which had said, it was something innocuous I know what it was it was about the baby’s growing nails and it wasn’t something that I would ever have thought of discussing with a mum-to-be. This had really caught her imagination so it was the right thing at the right time. She was much more engaged with the bump she was touching her bump she was talking about it. I just felt there was a whole attachment building already which could absolutely only be a positive thing for her but also for the baby, her mood had lightened which all together was wonderful.(Interview participant 27, Site Three)
Women in the post-embedding survey scored more positively on the Mother–Baby Bonding Scale than pre-embedding (p<0.01)

Strengths & limitations
• Study conducted across three sites giving comparative data
• In-depth interviews with stakeholders giving rich data
• Small number of survey respondents in women’s surveys
• Sociodemographic characteristics of women surveyed different to overall population
• Timing of the study captures only the early stages of the embedding process

Conclusions & recommendations
• Incorporating mobile phone app into maternity and early years care can be beneficial
• Needs:Sufficient numbers of motivated, senior Resource Leaders appointed early in the embedding
process
Senior staff on board
Maintain awareness among staff – keeping embedding on the agenda
Early introduction of the Baby Buddy app
Publicity to maintain awareness among women

Thank you

Baby Buddy Symposium: reducing health inequalities through digital parenting support
CBC Conference 2018 - Behaviour Change for Health: Digital and Beyond
Bringing Baby Buddy forward: assessing
cross-national transferability and co-creating a
web-based perinatal educational resource to
support the health professionals’ educational
role and enhance parental health literacy in
CyprusDr Nicos Middleton, Associate Professor Health Research
Methodology, Department of Nursing, School of Health Sciences,
Cyprus University of Technology
@BestBeginnings @CyUniTech @imperialcollege @UniofNewcastle @UCLan @Sydney_Uni
@BabyBuddyApp

“Baby Buddy – Forward” Key action: Cooperation for innovation. Strategic partnership: Adult Education
36 months: 1 Sept 2017 – 31 Aug 2020, Overall budget: ~ 350k euro
AIM: Bring the multi-award winning Baby Buddy (UK) forward
(1) assess cross-national relevance and transferability from high-resource to low-resource setting (Cyprus … and beyond)
(2) develop a modified educational resource & aid address learning needs of parents-to-be and support educational role of HP

CY context10000 birth/year: 70%-30% private-public split, different socio-demographic profile
2008-2015: C/S 60%, ~17% emergency (>30% public) Official MoH data
Bi-communal aspect, multi-cultural, high internet use (<30% reliable) Stylianou & Milioni 2016
Highly medicalized Hadjigeorgiou & Coxon. Midwifery 2014
Informed choice: physician dominance in communication Hadjigeorgiou et al Int J Childbirth 2012
Antenatal education Stylianides et al Int J Caring Sciences 2016
No Baby Friendly Hospitals Hadjiona et al Midwifery 2016
Exclusive breastfeeding: <20% 48 hours, <5% 6months Economou et al Public Health Nutr 2017
Postpartum depression: ~30% at 6 weeks; C/S, social gradient Stylianides et al Int J Caring Sciences 2016
Experience of labour: ~5.7 (SD 3.0) on a 1-10 VAS Stylianides et al unpublished PhD thesis 2015
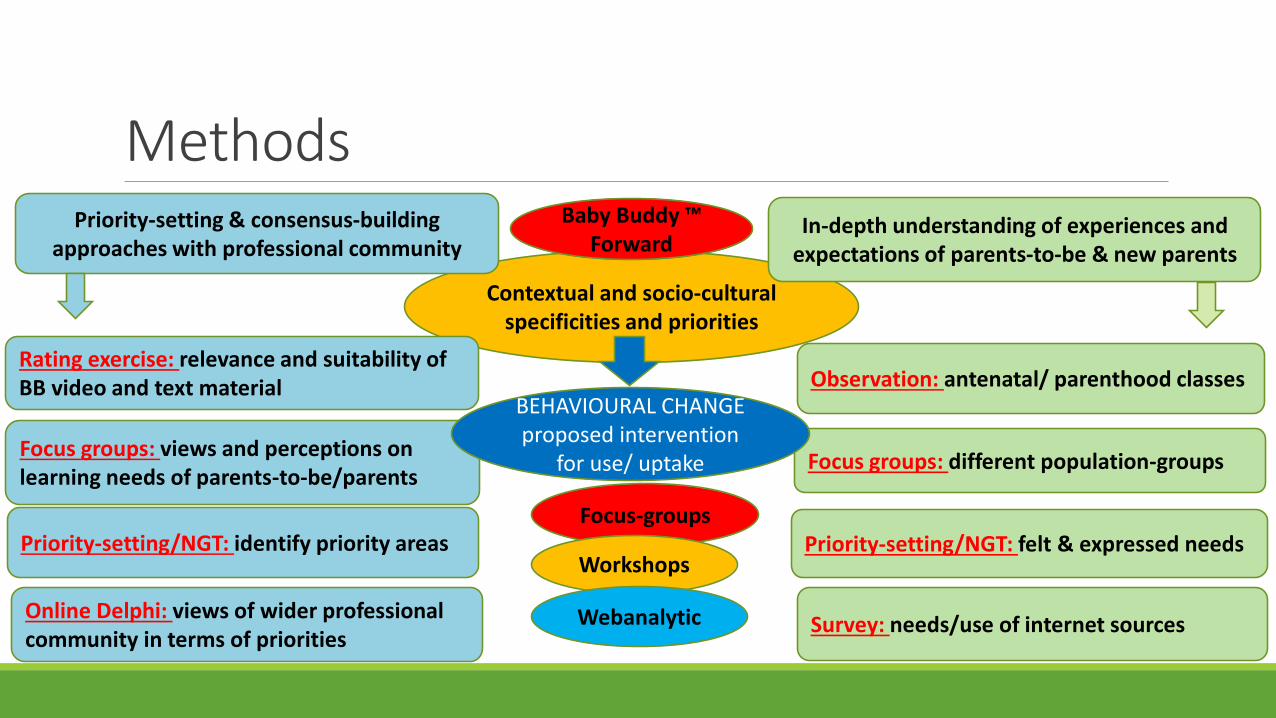
Contextual and socio-cultural specificities and priorities
MethodsPriority-setting & consensus-building
approaches with professional communityIn-depth understanding of experiences and
expectations of parents-to-be & new parents
Priority-setting/NGT: identify priority areas
Online Delphi: views of wider professional community in terms of priorities
Focus groups: views and perceptions on learning needs of parents-to-be/parents
Priority-setting/NGT: felt & expressed needs
Survey: needs/use of internet sources
Focus groups: different population-groups
Baby Buddy ™Forward
Rating exercise: relevance and suitability of BB video and text material
BEHAVIOURAL CHANGE proposed intervention
for use/ uptake
Focus-groups
Workshops
Webanalytic
Observation: antenatal/ parenthood classes


STRUCTURED PRIORITY-SETTING EXERCISE(Nominal Group Technique)
“If you had to prioritize a number of topics or issues that you feel have to be included in an antenatal or parenthood preparation educational programme, based on your experience with regards to the learning
needs of parents-to-be in Cyprus, which would you select??”
Educators/ Coordinators from all district hospitals (N=10)
Private sector: parenthood classes, NGOs, freelancers (N=7)
1st step: Silent generation of ideas
2nd step: Round-robin nominations
3rd step: Grouping of suggestions
4th step: Ranking and voting
Select top 5 and score on 1-5 importance scale

Public sector –Educators/Coordinators of antenatal classes
(Midwives/ Health Visitors, N=10, topics=26
Private sector –Parenthood classes, Support groups, NGOs, freelance
(multi-disciplinary, N=7, topics=25
Epidural (use of) 0 Medical interventions 0
Pain management/ Complimentary & Alternative 8
Exercise in pregnancy/postnatally 0 Exercise of infant and family 2
Family involvement/support 0 Services/ community support groups 1
Infant feeding/ Family meal planning 0 Weaning/ Introducing solids/ Long-term BF 5
Normal development of infant 0 Common illnesses & conditions 0
Nutrition in Pregnancy 0 Nutrition of infant and family 2
Partner relationships/Family changes 0 Partner Relationship/ Communication 3
Play/ Interaction with baby 0 Emotional needs of baby/newborn 15
Sex in pregnancy 0
Child accident prevention 1
Environmental health (pregnant mother & child) 1
Ultrasounds (understanding) 1
Immunizations 2 Immunizations 0
Physical and mental development of baby 2 Recognizing signs/needs of infant (crying) 2
Role of the father 2 Role of father 5
High & Low-risk pregnancy 3
Caring for the newborn (bath, massage) 4 Emotional needs of baby/newborn 15
Psychosomatic changes in pregnancy/postnatally 4 Medication use in pregnancy/BF 0
Family Planning 6
Health Promotion/ Well-being in pregnancy 6 Management of emotions/ emotional well-being 2
Potential obstacles during vaginal birth 7 Support in the prospect of C/S 0
Antenatal care/ Screening 8
Empowerment & Rights 13 Empowerment/ In touch with instinct/ Myths and stereotypes/ Culture 3
Psychoprophylaxis/ Breathing 26 Stages of labour/ practical choices 5
Breastfeeding 28 BF and supplements – when& how 0
Recognizing when baby’s hungry/full 8
Breastfeeding – intention and motivation 13
Obstacles in BF/ dealing with problems 16
Breastfeeding – position & techniques 17
Birth – experience/what to expect 32 Stages of labour/ practical choices 5

Public sector –Educators/Coordinators of antenatal classes
(Midwives/ Health Visitors, N=10, topics=26
Private sector –Parenthood classes, Support groups, NGOs, freelance
(multi-disciplinary, N=7, topics=25
Epidural (use of) 0 Medical interventions 0
Pain management/ Complimentary & Alternative 8
Exercise in pregnancy/postnatally 0 Exercise of infant and family 2
Family involvement/support 0 Services/ community support groups 1
Infant feeding/ Family meal planning 0 Weaning/ Introducing solids/ Long-term BF 5
Normal development of infant 0 Common illnesses & conditions 0
Nutrition in Pregnancy 0 Nutrition of infant and family 2
Partner relationships/Family changes 0 Partner Relationship/ Communication 3
Play/ Interaction with baby 0 Emotional needs of baby/newborn 15
Sex in pregnancy 0
Child accident prevention 1
Environmental health (pregnant mother & child) 1
Ultrasounds (understanding) 1
Immunizations 2 Immunizations 0
Physical and mental development of baby 2 Recognizing signs/needs of infant (crying) 2
Role of the father 2 Role of father 5
High & Low-risk pregnancy 3
Caring for the newborn (bath, massage) 4 Emotional needs of baby/newborn 15
Psychosomatic changes in pregnancy/postnatally 4 Medication use in pregnancy/BF 0
Family Planning 6
Health Promotion/ General well-being in pregnancy 6 Management of emotions/ emotional well-being 2
Potential obstacles during vaginal birth 7 Support in the prospect of C/S 0
Antenatal care/ Screening 8
Empowerment & Rights 13 Empowerment/ In touch with instinct/ Myths and stereotypes/ Culture 3
Psychoprophylaxis/ Breathing 26 Stages of labour/ practical choices 5
Breastfeeding 28 BF and supplements – when& how 0
Recognizing when baby’s hungry/full 8
Breastfeeding – intention and motivation 13
Obstacles in BF/ dealing with problems 16
Breastfeeding – position & techniques 17
Birth – experience/what to expect 32 Stages of labour/ practical choices 5
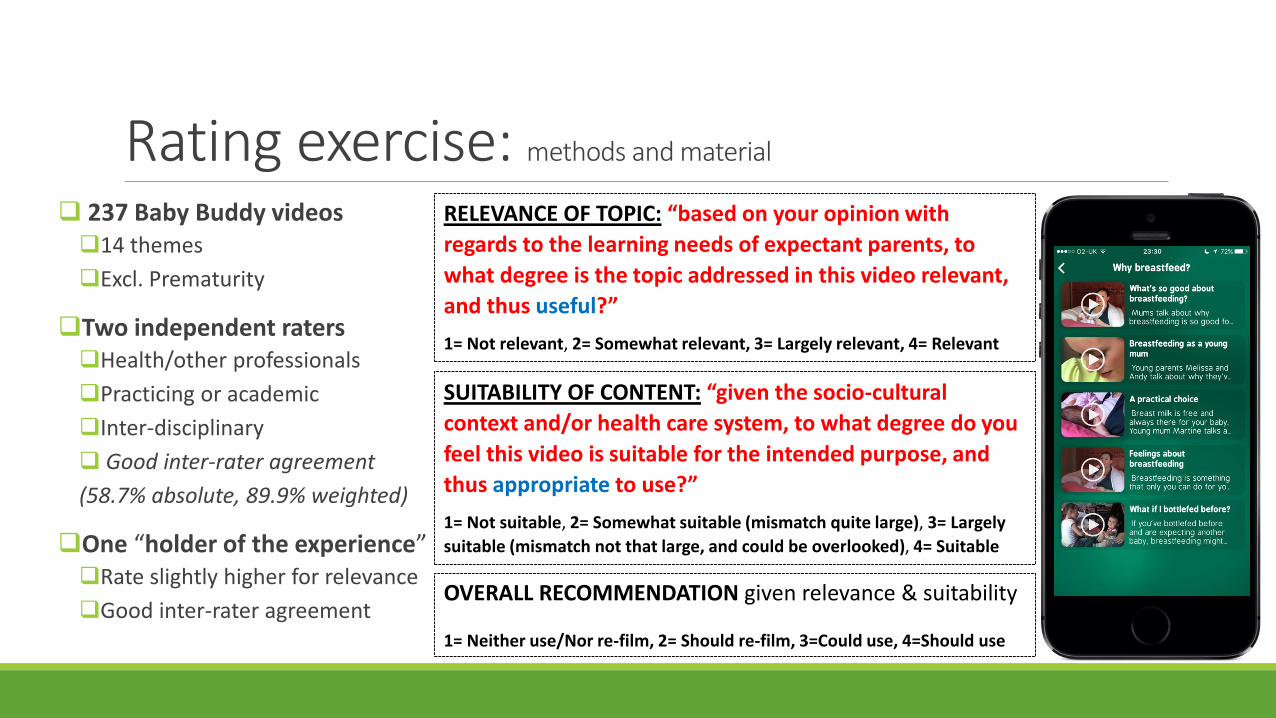
Rating exercise: methods and material
237 Baby Buddy videos14 themes
Excl. Prematurity
Two independent ratersHealth/other professionals
Practicing or academic
Inter-disciplinary
Good inter-rater agreement
(58.7% absolute, 89.9% weighted)
One “holder of the experience”Rate slightly higher for relevance
Good inter-rater agreement
RELEVANCE OF TOPIC: “based on your opinion with
regards to the learning needs of expectant parents, to
what degree is the topic addressed in this video relevant,
and thus useful?”
1= Not relevant, 2= Somewhat relevant, 3= Largely relevant, 4= Relevant
SUITABILITY OF CONTENT: “given the socio-cultural
context and/or health care system, to what degree do you
feel this video is suitable for the intended purpose, and
thus appropriate to use?”
1= Not suitable, 2= Somewhat suitable (mismatch quite large), 3= Largely
suitable (mismatch not that large, and could be overlooked), 4= Suitable
OVERALL RECOMMENDATION given relevance & suitability
1= Neither use/Nor re-film, 2= Should re-film, 3=Could use, 4=Should use

Classification of videos (number, %) in terms of relevance of topic to learning needs and suitability of content, based on the ratings of three independent raters (N=237)
RELEVANCE ≥3 =4
Group N (%) N (%)
Group 1:
High relevance
High agreement
176 (74.3%)
CVI-S UA
All 3 raters voted 4 101 (42.6%)
All raters ≥3
(and at least one voted 3)
75 (31.6%)
Group 2:
Relatively high
relevance
Not high agreement
49 (20.7%) At least 2 raters voted 4
(but at least one voted < 3)
23 (9.7%)
At least 2 raters ≥3
(but at least one voted <3)
26 (11.0%)
Group 3:
Relatively low
relevance
Not high agreement
10 (4.2%) Only one person voted ≥3 10 (4.2%)
Group 4:
Low relevance
High agreement
2 (0.8%) Nobody voted ≥3 2 (0.8%)
237 (100%) 237 (100%)
SUITABILITY ≥3 =4
Group N (%) N (%)
Group 1:
High suitability
High agreement
147 (62.0%)
CVI-S UA
All 3 raters voted 4 42 (17.7%)
All raters ≥3
(and at least one voted 3)
105 (44.3%)
Group 2:
Relatively high
suitability
Not high agreement
59 (24.9%) At least 2 raters voted 4
(but at least one voted < 3)
16 (6.8%)
At least 2 raters ≥3
(but at least one voted <3)
43 (18.1%)
Group 3:
Relatively low
suitability
Not high agreement
23 (9.7%) Only one person voted ≥3 23 (9.7%)
Group 4:
Low suitability
High agreement
8 (3.4%) Nobody voted ≥3 8 (3.4%)
237 (100%) 237 (100%)

Group 1:
High relevance
High agreement
Group 2:
Relatively high relevance,
Not so high agreement
Group 3:
Relatively low relevance,
Not high agreement
Group 4:
Low relevance
High agreement
TOTAL
Group 1:
High suitability
High agreementTotal= 135 (57.0%)
Across themes
Total = 12 (5.1%) 147
(62.0%)
Group 2:
Relatively high
suitability,
Not high
agreement
Total = 41 (17.3%) Total = 49 (20.7%)
90
(38.0%)
Group 3:
Relatively low
suitability, Not
high agreement
Group 4:
Low suitability
High agreement
TOTAL176 (74.3%) 61 (25.7%)
237
(100%)
• Healthcare system (e.g. family
nurse, home visits, MH services)
• CY reality (e.g. C/S, birth partner,
passive exposure, societal taboos)
• Socio-cultural mismatch (e.g.
dietary choices) and/or
• Contextualization (e.g. BF
challenges, Public, Exercise)
• Young parents/ teenage pregnancy
• Baby shower/celebration
• Social benefits: specific schemes
• Services: Gas/Air, water birth, home births
All > could use:
66.7%
At least one re-film/
Neither use, nor re-film:
95.9%
All should/could use:
83.0%
>1 rater, re-film:
80.5%
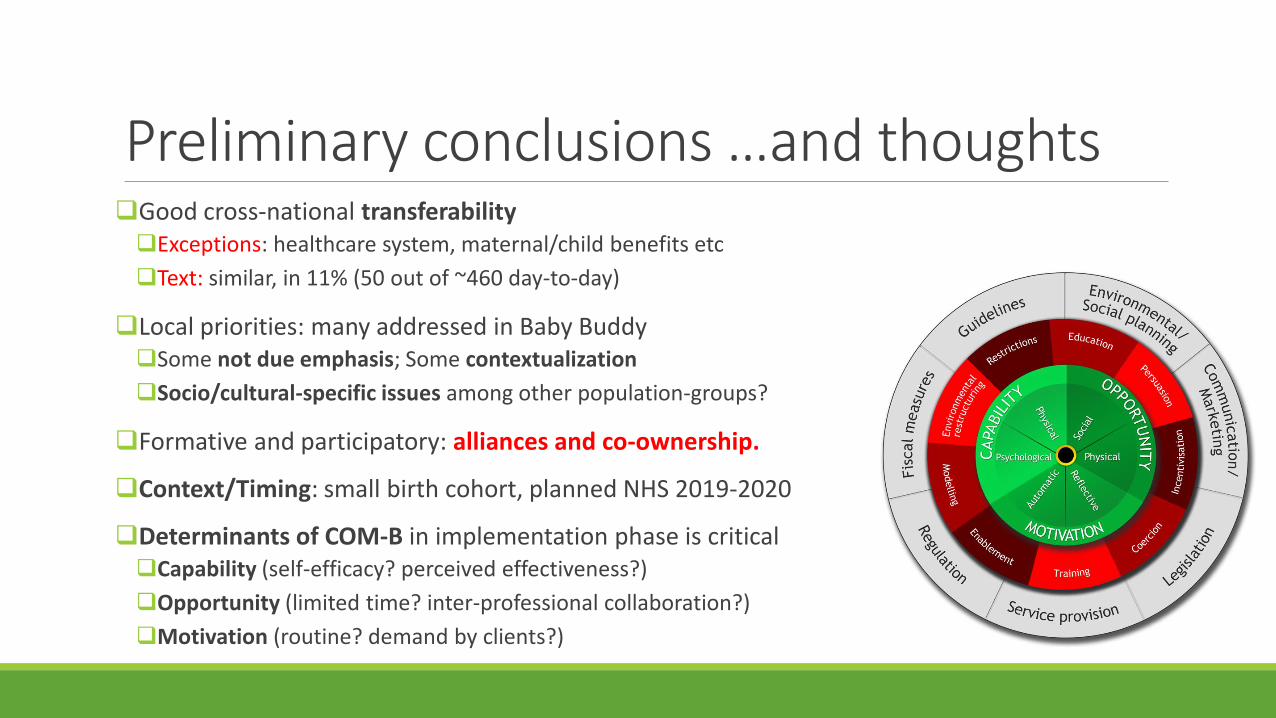
Preliminary conclusions …and thoughts Good cross-national transferability Exceptions: healthcare system, maternal/child benefits etc
Text: similar, in 11% (50 out of ~460 day-to-day)
Local priorities: many addressed in Baby BuddySome not due emphasis; Some contextualization
Socio/cultural-specific issues among other population-groups?
Formative and participatory: alliances and co-ownership.
Context/Timing: small birth cohort, planned NHS 2019-2020
Determinants of COM-B in implementation phase is criticalCapability (self-efficacy? perceived effectiveness?)
Opportunity (limited time? inter-professional collaboration?)
Motivation (routine? demand by clients?)

Impact: client-provider communication
“…I really enjoyed meeting everybody, that we were asked, that we were heard, we shared experiences, it makes us all better…” Midwife 3
“…opened up new avenues to move forward...today I am very excited.”
Midwife 5
“ I believe…it is through teamwork we can achieve much more. We are all different pieces of the same puzzle”
Pediatrician
“Inspirational” Doula
“I could stay here and talk for hours”
Lactation consultant
Top-down: Better-equipped
health professionals
Bottom-upWider reach and
demand for better care by better-informed users
Agent-ledenhanced role of NGO &academics as advocates
Dialogue platform for inter-professional
collaboration


Baby Buddy: reducing health inequalities
through digital parenting supportChair: Dr Ann Hoskins @HoskinsAnn
Discussant: Prof. Mitch Blair, Imperial College London, @blair_mitch
Alison Baum OBE, Best Beginnings, @AlisonBaum
Dr Adrienne Gordon, University of Sydney, @AdrienneOz
Dr Sam Ginga, representing BaBBLeS research team
Dr Nicola Crossland, University of Central Lancashire
Dr Nicos Middelton, Cyprus University of Technology
PANEL DISCUSSIONCBC Conference 2018 - Behaviour Change for Health: Digital and Beyond
Parallel Session 6, 11.45am-12.40am Symposium
@BestBeginnings @CyUniTech @imperialcollege @UniofNewcastle @UCLan @Sydney_Uni
@BabyBuddyApp

Participatory formative action research
Enrich content (local priorities and socio-cultural specificities)
Engage in priority-setting and consensus-building exercise among health professionals
Enhance relevance, appeal and reach via active consultation (Greek, Turkish, Arabic, Russian)
Research insights into experiences and expectations of parents-to-be/new parents
Develop policy recommendations on system change with decision-makers
“Complimentary” model of care (“as well” rather than “instead of”)
EDUCATIONAL RESOURCEand complimentary EDUCATIONAL AID
LEARNING NEEDS, PRIORITIES
EXPERTISE & EXPERIENCE
CO-OWNERSHIP CO-CREATIONCOLLECTIVE INTELLIGENCE









