
Bed Management and Escalation Policy v4
Policy No: OP33
Version: 4.0
Name of Policy: Bed Management and Escalation Policy
Effective From: 28/09/2015
Date Ratified 17/07/2015
Ratified PQRS Committee
Review Date 01/07/2017
Sponsor Director of Nursing, Midwifery and Quality
Expiry Date 16/07/2018
Withdrawn Date
Unless this copy has been taken directly from the Trust intranet site (Pandora) there is no assurance that
this is the most up to date version
This policy supersedes all previous issues

Bed Management and Escalation Policy v4 2
Version Control
Version Release Author/Reviewer Ratified
by/Authorised
by
Date Changes
(Please identify
page no.)
1.0
Jan 2006
TFP Jan 2006
2.0
Sept 2008
Divisional
Managers
SafeCare
Council
Sept 2008
3.0
August
2010
Divisional
Managers
SafeCare
Council
11/10/2009
4.0 08/10/2010 CC Divisional
Manager
SafeCare
Council
11/10/2009
5.0
28/09/2015
Pam Naylor PQRS
Committee
17/07/2015

Bed Management and Escalation Policy v4 3
CONTENTS Page
1 Introduction .................................................................................................................................. 5
2 Policy scope .................................................................................................................................. 5
3 Aim of policy ................................................................................................................................. 5
4 Duties (Roles and responsibilities) ............................................................................................... 5
4.1 Board of Directors ........................................................................................................... 5
4.2 Chief Executive ................................................................................................................ 6
4.3 Director on Call ............................................................................................................... 6
4.4 Associate Directors .......................................................................................................... 6
4.5 Service Line Managers ..................................................................................................... 6
4.6 Medical Staff .................................................................................................................... 6
4.7 Bed Managers .................................................................................................................. 6
4.8 Matrons ........................................................................................................................... 7
4.9 Night Site Manager .......................................................................................................... 7
4.10 Ward Sister/Charge Nurse ............................................................................................... 7
4.11 Accident and Emergency Sister/Charge Nurse and Clinical Lead .................................... 7
4.12 Members of Staff ............................................................................................................. 7
5 Definitions .................................................................................................................................... 7
6 Main Body of the policy ................................................................................................................ 8
6.1 Normal Working .............................................................................................................. 8
6.2 Bed management process ............................................................................................... 9
6.2.1 Bed Meetings ......................................................................................................... 9
6.2.2 Bed State ............................................................................................................... 9
6.2.3 Patient’s Awaiting Admission ................................................................................ 9
6.2.4 The Flight Desk ...................................................................................................... 9
6.3 Early Supported Discharge and Alternatives to Admission ............................................. 9
6.4 ‘Boarding’ of Patients ...................................................................................................... 10
6.5 Trigger levels and escalation ........................................................................................... 11
6.5.1 Alert Levels (NEEP) ................................................................................................ 11
6.5.2 Triggers for Escalation .......................................................................................... 11
6.5.3 Action Cards ........................................................................................................... 11
6.6 Requesting and receiving Patients Divert from other Trusts .......................................... 12
6.6.1 Requesting a Divert ............................................................................................... 12
6.6.2 Receiving a Divert .................................................................................................. 12
6.6.3 Durham .................................................................................................................. 12
6.7 Ambulance Handover Delays ......................................................................................... 12
6.8 Winter Resilience Plan ..................................................................................................... 12
7 Training ......................................................................................................................................... 12
8 Equality and diversity ................................................................................................................... 13
9 Monitoring compliance with the policy ....................................................................................... 13
10 Consultation and review ............................................................................................................... 13
11 Implementation of policy (including raising awareness) ............................................................. 13
12 Associated Policies ....................................................................................................................... 13
13 Appendices ................................................................................................................................... 13

Bed Management and Escalation Policy v4 4
APPENDICES
Appendix 1: QE Quick Triggers for Alert Levels ................................................................................... 14
Appendix 2: North East Escalation Plan (NEEP) ................................................................................... 15
Appendix 3: ED Specific Triggers and Actions ...................................................................................... 32
Appendix 4: ECCA Escalation Triggers and Actions ............................................................................ 33
Appendix 5: Action Cards .................................................................................................................... 36
- Actions for the Bed Managers ............................................................................... 36
- Actions for Duty Matron (Cover 7.30am – 5pm) ................................................... 38
- Actions for the Duty Matron (Cover 5 - 8.30pm) .................................................. 41
- Actions for the Service Line Manager and Senior Manager on Call ...................... 42
- Actions for the Senior Manager on Call from 5pm and Weekends ....................... 44
- Actions for the Senior Manager on Call from 5pm ................................................ 45
- Actions for the Acute Response Team Band 7 Role (Cover 20:00pm – 08:00am) 46
- Actions for the Director on Call ............................................................................. 48
- Action for the Medical Teams, Consultants and Clinical Leads ............................. 50
Appendix 6: Standard Operating Procedures ...................................................................................... 52
- Monitoring A&E Ambulance Handover Breaches
- Escalating A&E Ambulance Handover Breaches
Appendix 7: Winter Resilience Plan ..................................................................................................... 53

Bed Management and Escalation Policy v4 5
Bed Management and Escalation Policy
1. Introduction
This policy aims to provide clear operational guidance for bed management and escalation and
incorporates the escalation status, bed capacity and emergency trigger points and associated
action’s required in response to operational pressures. This will provide a safe operating
framework for staff and reduce the levels of risk for patients.
Maintaining flow of patients through the Trust is key to maximising bed availability in order to
effectively manage fluctuations in workload. As a key principle Gateshead Health NHS Foundation
Trust will not close to emergency admissions. When hospital resources are stretched e.g. shortage
of beds, exceptionally high attendances in the Accident and Emergency Department hospital
remains the safest place for seriously ill people. Closure of the hospital will only be on the
instruction of the Director on Call and will result in the declaration of a Major Incident.
2. Policy Scope
This policy applies to all members of staff of Gateshead Health NHS Foundation Trust. The policy
recognises that not all staff groups in all disciplines will have direct involvement in bed
management and escalation, however all members of staff have a responsibility to support this
policy.
3. Aim of the Policy
This policy aims to provide clear guidance to those directly involved in bed management and
escalation; the establishment of an effective policy and framework which will contribute to the
following:
• Early identification of capacity problems
• Proactive rather than reactive response
• Concise and clear actions
• Defined responsibilities
This policy will enable the Trust to deal effectively with fluctuations in demand and capacity so that
it can manage associated risk within acceptable limits. The policy is designed to mitigate the risk of
further escalation and ensures an appropriate response from key staff members to contribute to a
reduction in escalation status.
The policy aims to ensure that every emergency admission is allocated a bed within four hours and
no elective admission is cancelled because of lack of bed availability. Effective communication and
teamwork is crucial to the implementation of this policy requiring regular dialogue with nursing
staff, medical staff and managers.
The policy aims to maintain high standards of patient safety, patient experience and performance
against key waiting time and quality standards of care.
4. Duties (Roles and Responsibilities)
4.1 Board of Directors
The Trust Board is responsible for ensuring that there is a robust system of Corporate
Governance within the organisation. This includes having a systematic process for the
development, authorisation and management of policies.

Bed Management and Escalation Policy v4 6
4.2 The Chief Executive
The Chief Executive is ultimately responsible for ensuring effective Corporate Governance
within the organisation and therefore supports the Trust wide implementation of this
policy.
4.3 Director on call
The Director on Call is responsible for setting up Gold Command at NEEP 5, to support with
diverts where required and to facilitate discussions with regards to Ambulance queuing in
exceptional circumstances.
4.4 Associate Directors
Associate Directors are responsible for ensuring that the systems and processes are in place
so that this Policy is implemented effectively within the individual Business Units. They are
responsible for developing the annual corporate winter plan.
4.5 Service Line Managers
Service line Managers are responsible for ensuring that systems are in place so the Bed
Management and Escalation Policy is implemented effectively within individual service
lines:
• Ensuring systems are in place to manage patient access effectively
• To ensure day-to-day capacity is available for the individual specialty
• To ensure a forward thinking and planning approach for the provision of patient
care services.
• Making the decision to open extra beds or a ward if the trigger level of bed
availability within the Trust is not achieved.
• Participate in Senior Manager on call rota escalating issues to the Director on Call
as required.
When Senior Manager on Call work with the Bed Manager / Night Site Manager and Duty
Matron to ensure effective use of beds is maintained and that patients are not kept in
Accident and Emergency for any longer than necessary.
4.6 Medical Staff
Medical staff are responsible for ensuring that the elements of the SAFER bundle are
implemented. This includes ensuring that discharge planning arrangements are robust and
in line with the Trust Discharge Policy (OP13) including setting a discharge date for all
patients. In addition, collaborating with the ward nursing team to identify patients who are
appropriate to be ‘boarded’ to other specialties if required; organising additional ward
rounds during periods of Escalation at NEEP 4; fast tracking assessments in Accident and
Emergency as appropriate and explore alternatives to admission (e.g. rapid access to the
next available clinic).
4.7 Bed Managers
Bed Managers are responsible for:
• Operational responsibility for the daily management of beds
• Ensuring that an up to date bed state and record of patients waiting for admission
is maintained
• Co-ordination of information for presentation at bed meetings
• Escalation of any potential problems to the Duty Matron
• Completion and delivery of Flight Deck information to NEAS.

Bed Management and Escalation Policy v4 7
4.8 Matrons
The Matron’s role is to proactively action issues identified within their area of
responsibility. They are available to provide support and advice to the ward team and to
support the team in the management of effective discharge. They will provide support and
advice to ward staff when they experience difficulty in identifying patients suitable for
boarding.
The Duty Matron will facilitate and coordinate bed meetings and actively manage within
this policy escalating to the Service Line Managers, Associate Directors as set out in
appendix 5.
4.9 Night Site Manager
The Night Site Manager is responsible for the overnight site management of the hospital
and delivery of services and ensuring any issues are escalated to the Service Line Manager
on call.
4.10 Ward Sister/Charge Nurse (delegated to Nurse in Charge)
The Ward Sister/Charge Nurse is responsible for ensuring staff understand the Bed
Management and Escalation Policy and the Discharge Policy. They will work proactively
with the medical staff to ensure the elements of the SAFER bundle are implemented to
identify patients who are ready for discharge, appropriate for boarding and ensuring staff
understand that at times wards will be expected to:
• Take boarders
• place boarders in an appropriate part of their ward following an infection control
risk assessment
• Move staff to another area to support the delivery of clinical care
The ultimate responsibility for providing accurate bed state updates rests with the Ward
Sister/Charge Nurse (or nominated deputy). This is best facilitated by keeping Medway as
up to date as possible with changes in patient movement and all wards should be working
to achieve this on a 24 hour basis. They must keep the appropriate Matron aware of any
concerns about staffing and/or the implementation of this policy.
4.11 A&E Co-ordinator and Clinical Lead
The A&E Co-ordinator and Clinical Lead are responsible for ensuring that the person ‘in
charge’ is identified on each shift to provide regular updates on current occupancy, and
expected admissions and discharges over the next 2 to 4 hours. The A&E co-ordinator in
charge of each shift is responsible for reporting to the Duty Matron any patient who has
been in the department for 2.5 hours, for whom there is no imminent plan and who looks
like they will be in the department over 4 hours unnecessarily, and efforts made to ensure
a safe and effective plan is put in place.
4.12 All members of staff are required to support this Policy whether or not they are directly
affected by bed management and escalation.
5. Definitions
Escalation
Escalation, for the purpose of this Policy identifies when there are increasing levels of demand in
the Emergency Department/Emergency Assessment Unit and/or lack of bed capacity and specific
responses are required.
Boarder
This term may be used when a patient is residing on a ward outside their admitting specialty.

Bed Management and Escalation Policy v4 8
Action cards
Key staff members have action cards (within this policy) which provide them with actions that they
should undertake at a particular escalation status level.
North East Escalation Plan (NEEP)
NEEP is a common language used by all hospital and community organisations in the North East to
identify the levels of activity pressure and escalation across the area. In producing this document
the Trust has aligned this Policy to the North East Surge and Escalation Framework (Appendix 2).
SAFER Bundle – The SAFER bundle is a set of recommended good practice actions to be taken on a
daily basis to support good patient flow.
S – Senior review of all patients before mid-day
A – All patients to have an expected date of discharge
F – Flow of patients, wards to pull patients from assessment units to wards before 10am
E – Early discharge, 33% of patients from base wards to be in discharge lounge with to take out
(TTO’s) medications and letter before mid-day
R – Review of all patients with extended length of stay (10-14 days) to have a management plan
Gold Command
Gold Command is introduced at NEEP Level 5, or at NEEP 4 to prevent NEEP 5 status being reached.
This involves a decision being made by the Director on Call in liaison with the Senior Manager on
Call. Identified staff will be required to report to a designated area to oversee all actions in respect
of escalation. This is part of our major incident plan.
HALO
The Hospital Ambulance Liaison Officer (HALO) is a member of staff from the North East Ambulance
Service who works very closely with the A&E Co-ordinator to support the levelling of activity across
the local area.
The Flight Deck
Is a series of metrics submitted by Trusts from across the Region to the North East Ambulance
Service (NEAS). The metrics include:
• NEEP status
• Empty bed numbers including critical care, surgery, medicine and maternity
• Are there any diverts in place
• Are there any bed closures
• Length of waits to be seen in A&E
The information collected is then shared across the Region. The NEAS use this information to
facilitate decisions on diverts and deflections.
6. Main Body of the policy
6.1 Normal Working
Normal working is how the Trust operates on a day to day basis to ensure NEEP level 1 (see
appendix 1). All Trust employees are required to actively contribute to the timely and safe
care of patients and implementation of the SAFER bundle.

Bed Management and Escalation Policy v4 9
6.2 Bed management process
Every morning there is a report and bed state email handover from the Night Site Manager
to key personnel and a verbal handover to the Duty Matron and Bed manager.
6.2.1 Bed meetings
Bed meetings are held at 9am, 1pm and 4.30 pm with Business unit staff. Frequency
of meetings may change when the Trust is on NEEP 3 & 4 at the discretion of the
Duty Matron.
6.2.2 The Bed State
Throughout the day the bed state will be updated using the bed monitoring
proforma. This will include:
• Number of empty beds by ward, specialty, male/female and side wards.
• Number of patients expected to be discharged that day.
• Number of patients ‘boarded out’ or awaiting transfer to other hospital
sites.
• Number of beds occupied by patients awaiting arrangements for discharge
and the reasons for these delays.
• Number of patients waiting for isolation facilities.
• Potential patients who will be ready to come out of Critical Care the next
day.
• Number of electives due to come in the next day.
• Numbers of in-patients admitted following an agreed Durham divert.
It is the responsibility of ward staff to provide accurate and timely information.
6.2.3 Patients Awaiting Admission
The Bed Manager will be informed of patient admissions and demand for beds by
the Nurse Co-ordinator in A&E, waiting list managers, member of staff taking GP
referral calls and Matrons.
All patients arriving by ambulance will arrive at the ambulance entrance and will be
streamed (initial assessment and directed to appropriate care setting) by the A&E
co-ordinator. GP referrals will be streamed direct to EAU unless there is no capacity
(in which case they will be streamed to appropriate pathway in EAU), unless they
require immediate resuscitation, or can be appropriately managed in Majors.
6.2.4 The Flight Deck
Information to be submitted three times a day at 11am, 4pm and 8pm by the Bed
Manager.
6.3 Early Supported Discharge and Alternatives to Admission
Several services have been developed to provide an alternative to hospital admission and
support early discharge:
• All specialist nurses – work to provide early supported discharges and prevent
unnecessary admissions where appropriate.
• CROP team can facilitate a discharge and provide interim support whilst awaiting
more formal care packages to start.
• Rapid Response Domiciliary Care Team
• Gateshead Immediate Care Team

Bed Management and Escalation Policy v4 10
A site wide Multi-Disciplinary meeting takes place every day at 12.30pm to identify patients
who are awaiting discharge and to ensure all actions are in place to help people to be
discharged from hospital.
6.4 ‘Boarding’ of Patients
When bed pressures continue is may be necessary to ‘board’ patients to another ward. In
the context of this policy, a ‘boarder’ is defined as ‘a patient residing on a ward outside
their admitting specialty’. The boarding of patients should be avoided as far as possible.
However, there are times when such activity becomes a necessary part of managing
emergency admissions and maintaining a supply of appropriate beds. The decision to
board patients will be co-ordinated by the Duty Matron. While there are no protected beds
within the hospital all beds that are planned for elective admissions later that day or the
following day should be last in line to board to.
The clinical teams on the base wards remain responsible for identifying patients that are
suitable to be moved elsewhere.
It is acknowledged that, at times, there will be no patients that are deemed suitable. Under
these circumstances the clinical teams will be expected to make decisions based on their
professional judgement, to identify patients to move.
In the event of patients being ‘boarded’ the Named Nurse or nurse in charge will explain
this to the patients and relatives, if possible, in a manner appropriate to the patient’s
individual needs accessing the support of the interpretation services or support worker if
required.
If the relatives are not present it is the responsibility of the Named Nurse or nurse in charge
to notify the ‘next of kin’ / ‘person to notify’ of the patient’s transfer and ensure that this is
documented.
The Bed Manager will liaise with the Matron from the Division to which patients are
boarded at the regular bed meetings. The Bed Manager should inform the appropriate
wards of the arrangements to transfer or ‘board’ a patient. As stated above Ward Staff on
the transferring ward will remain responsible for providing necessary clinical detail to
facilitate arrangements. When it is necessary to board from one specialty to another it is
best practice to allocate a single bay to accommodate the patients from the boarding
specialty whenever possible. Advice must be sought from the Infection Prevention and
Control Team for any patient/s with a known or suspected infection.
The boarding of patients should take place between the hours of 09:00 and 22:00 each day
wherever possible. Only in exceptional circumstances will the moving of patients occur
outside these hours or during protected mealtimes. No patient should, during their stay, be
boarded out more than once. This does not include any subsequent transfer to the care of
another Consultant or Specialty, for a clinical need, or repatriation to original base ward in
exceptional circumstances.
The dignity and quality of care given to the patient will be maintained throughout the
transfer or ‘boarding’ process (OP29). Staff must use their professional judgment when
attempting to move patients who would be clearly distressed by the move e.g. patients
with learning difficulties or there is knowledge that the family have raised strong concerns.
When patients are boarded out from the specialty, which would normally receive the
admission, it becomes the responsibility of the receiving ward and patient’s consultant
team to ensure they receive the same standard of care. Junior medical teams on receiving

Bed Management and Escalation Policy v4 11
wards are expected to support the care of patients who have been moved from their base
ward. If needed, advice can be sought from the specialty Matron.
Circumstances such as skill mix, infection status on the receiving ward should be taken into
consideration.
The numbers of patients boarded into different specialties will be reported on a daily basis
through the SITREP report in line with DH guidance.
When transferring (either within Gateshead Health NHS Foundation Trust or to another
hospital / organisation) ‘boarding’ or receiving a patient all nursing documentation must be
updated.
It is the responsibility of the Named Nurse to make an assessment of the patient’s needs to
determine if an escort is required to accompany / stay with the patient when they are being
transferred to another ward, department or site within Gateshead Health NHS Foundation
Trust in line with the Internal Transfer/Escort Policy (OP84)
6.4 Trigger levels and Escalation
6.5.1 Alert Levels (NEEP)
The following alert levels will be used to help communicate the escalation status
and guide people to the correct actions. This is based on a number scale that
reflects the level of risk to patient safety and the extent to which patient
experience may be compromised (as outlined below).
6.5.2 Triggers for escalation
Appendix 1 Trigger/alert levels are identified in (quick reference guide).
Appendix 2 outlines the Trust NEEP levels and escalation framework agreed by
Trust Board in line with North East Surge and Escalation Framework
Appendix 3 local triggers for Accident & Emergency
Appendix 4 local triggers Emergency Assessment Unit
Please refer to guidance, when appropriate, for actions specific to other
departments – Maternity, Critical Care Escalation Plans.
6.5.3 Action cards
The Action cards highlight actions to be taken by key individuals in the event of
increasing pressure and when triggers are causing any concern.
To patient safety and experience
Moderate
Risk
3
Low Risk
2
High
Risk
4
Service
Failure
6
Low Risk
1
Critical
5

Bed Management and Escalation Policy v4 12
Following the identification in a rise in the Escalation/NEEP Alert levels within the
NEEP escalation framework and local triggers for Accident & Emergency (Appendix
3) and Emergency Assessment Unit (Appendix 4), actions identified in the suite of
Action Cards (set out in appendix 5) will be followed by all key personnel.
6.6 Requesting and Receiving Diverts from other Trusts
6.6.1 Requesting a Divert
When the Trust is at NEEP 4 the Trust may need to request a divert to another
hospital. The requirement to consider this should be escalated by the Duty Matron
or Service Line Manager to Associate Director during office hours or Senior
Manager on Call to Director on Call out of hours. The regional divert policy should
be consulted in relation to this.
6.6.2 Receiving a Divert
• Any request to receive a divert should be made to a Service Line Manager in
Medicine (in hours) or Senior Manager on Call out of hours .
• Discussion should then take place with the on site team which may include
Bed Manager, Duty Matron, SLM, Consultant in charge of A&E, A&E nurse
co-ordinator before making a decision to accept patients.
• It is advised a fixed number of patients to accept should be agreed with a
built in review rather than a time period. Close monitoring is required to
assess the impact on our internal patient flow.
• Refer to North East Divert Policy (NEAS- May 2015)
• Escalate or further discuss with Associate Director (in hours) or Director on
Call (out of hours).
6.6.3 Durham
• We currently have an agreement with Durham CCG with regards to diverts
– refer to NDCCG Local Divert Policy (June 2015). This will be a NEAS direct
contact to the Service Line Manager in medicine (in hours) or Senior
Manager on Call (out of hours). Discussion with Associate Director (in
hours) or Director on Call (out of hours) can take place if required.
• When making decisions to request or accept a divert the Flight Deck
information may be of some help.
• Patient level details are required for Durham diverted patients in order to
ensure they are correctly logged on Medway.
6.7 Ambulance Handover Delays
Queuing of ambulances at A&E should be avoided whenever possible and proactive
management is required to ensure kept to a minimum. Appendix 6 outlines key actions to
be taken and how ambulance handover delays should be monitored.
6.8 Winter Resilience Plan
Every year additional measures are put in place for the winter months. Appendix 7 outlines
the current Winter Resilience Plan.
7. Training
Training with regards to this policy will take place at Site Training days, at Matron and Ward
Manager days, the Service Line Manager forum and the Central Management team time out.

Bed Management and Escalation Policy v4 13
8. Equality and diversity
The Trust is committed to ensuring that, as far as is reasonably practicable, the way we provide
services to the public and the way we treat our staff reflects their individual needs and does not
discriminate against individuals or groups on any grounds. This policy has been appropriately
assessed.
9. Monitoring Effectiveness of this Policy
To ensure the effectiveness of this policy the following indicators will be monitored:
• Number of 4 hour A&E waits
• Number of 12 hour A and E breaches
• Number of black (over 1 hour) Ambulance handover delays.
• Number of Ambulance handover delays above 30 minutes
• Number of diverts to other hospitals requested
• Number of cancelled operations as a result of bed pressures
10 Consultation and review
A Kaizen event was held with a number of stakeholders including Medical Staff, in order to engage
a broad spectrum of staff in the development of this policy. This was followed up with a series of
discussions to finalise actions. The implementation and effectiveness of the policy will be reviewed
through Performance Board Reports and annually at the Annual Winter Review event.
11 Implementation of policy (including raising awareness)
The policy will be implemented immediately and awareness will be raised at Matron /Ward
Manager Away Days, SLM forum, CMT time out, and Consultants’ meetings.
12. Associated Policies
This policy must be read in conjunction with the following Gateshead Health NHS Foundation Trust
Policies:
• Privacy and Dignity:
• Infection Prevention and Control Policies (IC1 – 26)
• Safeguarding Patients’ Privacy & Dignity (OP29)
• Patients’ Access Policy (OP12)
• Discharge Policy (OP13)
• Resuscitation Policy (RM27a and RM27b)
• Records Management Policy (OP10)
• Critical Care Escalation Policy
• Maternity and Special Care Baby Unit Escalation Policy
13 Appendices

Bed Management and Escalation Policy v4 14
Level A&E (see Appendix 3) EAU (see Appendix 4) Back of House
1 • Business as Usual • Business as Usual • Business as Usual
2
• 1 patient spending more than 4 hours in the
ED (avoidable)
• 1 resus space and 1 majors space
• Time from DTA to admission 1-2 hours
• 1-2 ambulance handovers > 15 minutes
• Pts on trolley >8hrs
• 0 cubicle availability 0-
1hrs
• Beds not available to receive non elective patients (ie less than one male
and one female bed available for each non elective receiving areas)
• Insufficient capacity identified in bed meeting for TCIs either medicine or
surgery
• Between 1 – 5 outliers in other specialties
• No critical care bed immediately available
• Ward staffing below agreed levels by 1 – 3 nursing staff across the site and
is judged to present a low risk to patient safety
3
• Multiple patients spending more than 4
hours in the ED (avoidable)
• 0 resus spaces and 0 majors spaces
• Time from DTA to admission 2-4 hours
• 4-8 patients stacking in the ED awaiting
admission
• 2 ambulance handovers > 15 minutes
• Pts on trolley >12hrs
• 0 cubicle availability
between 1-4hrs
• Insufficient capacity to accommodate non clinically urgent TCIs in either
medicine or surgery
• 5 – 14 outliers
• No critical care bed available and no plan in place for one to become
available in the next four hours
• Ward staffing is below agreed levels by 4 – 6 nursing staff across site and is
judged to present a moderate risk to patient safety
4
• Multiple patients spending significantly
longer than 4 hours in the ED
• No capacity to receive patients
• Time from DTA to admission >4 hours
• >8 patients stacking in the ED awaiting
admission
• Ambulances queuing to handover
• Pts on trolley >24hrs
• 0 cubicle availability
>4hrs
• Insufficient capacity to accommodate TCIs in either medicine or surgery
who are clinically urgent
• >15 outliers in other specialties
• Ward staffing is below agreed levels by 7+ nursing staff across site
• No critical care bed available, no place in place for one to become available
in the next four hours and no scope for escalation of critical care capacity
5
• Pts on trolley >36hrs
• 0 cubicle availability
>8hrs
• Negative bed state in either medicine or surgery with escalation areas open
& continued A&E/EAU triggers
• Ward staffing is below agreed levels by 7+ nursing staff across the site and
is judged to present a high risk to patient safety
6 • •
QE TRIGGERS FOR ALERT LEVELS (Quick Reference Guide) Appendix 1

15
*ED consultant when present in the ED. ED middle grade at other times.
Surge and Escalation Framework for : GATESHEAD HEALTH NHS FOUNDATION TRUST
Version number: 3.0 Date created: July 2015 Author: Pam Naylor
Glossary of Terms/Abbreviations:
NEEP – North East Escalation Plan NEAS: North East Ambulance Service NECS: North East Commissioning Service
DEP – Department Escalation Plan REAP: Regional Escalation Action Plan DM: Duty Matron
NECS: Clinical Commissioning Group AD: Associate Director ED: Emergency Department
OOH: Out of Hours DOC: Director on Call CD: Clinical Director
SMOC: Senior Manager on Call ART: Acute Response Team
Trigger Level Action Communication Command and control Impact Implications?
• What needs to
have happened
(actual), or be
about to
happen
(prospective
trigger)?
• Are these
internal
organisational
triggers, or
external ones
i.e. across the
NECS?
• NHS North East
Escalation Plan
(NEEP) level
• Description of
what is happening
in the organisation
or service at this
level
• What will be done to
mitigate the raised level
of pressure as a result of
moving to this level?
• Who by? When?
Where?
• What will be
communicated
intra and/ or inter
organisationally?
• Who by? When?
• What command and
control
arrangements will
be in place?
• Who has the
authority and
responsibility to
trigger?
• When and where
will it be triggered?
• Are these different
in hours and out of
hours?
• Expected
impact of
these
actions
• Any
implications
of these
actions on
other
organisations
Appendix 2

16
Surge and Escalation Framework for : Gateshead Health NHS Foundation Trust
Version number: 3.0 Date created: July 2015 Author: Pam Naylor Glossary of Terms /Abbreviations: NEEP – North East Escalation Plan NEAS: North East Ambulance Service NECS: North East Commissioning Service ED: Emergency Department DEP – Department Escalation Plan REAP: Regional Escalation Action Plan CD: Clinical Director DM: Duty Matron NECS: Clinical Commissioning Group AD: Associate Director ART: Acute Response Team SMOC: Senior Manager on Call OOH: Out of Hours DOC: Director on Call
Trigger Level Action Communication Command and control Impact Implications?
• What needs to have happened (actual), or be about to happen (prospective trigger)?
• Are these internal organisational triggers, or external ones i.e. across the NECS?
• NHS North East Escalation Plan (NEEP) level
• Description of what is happening in the organisation or service at this level
• What will be done to mitigate the raised level of pressure as a result of moving to this level?
• Who by? When? Where?
• What will be communicated intra and/ or inter organisationally?
• Who by? When?
• What command and control arrangements will be in place?
• Who has the authority and responsibility to trigger?
• When and where will it be triggered? • Are these different in hours and out
of hours?
• Expected impact of these actions
• Any implications of these actions on other organisations
• The Trust is operating at “normal service” 16 beds funded for winter contingency are available at NEEP level 1
Influencing factors (changes to the following):
• Premises • Workforce • IT • Resources, assets, utilities
and supplies
• Surge in demand
• Queuing ambulance
NEEP 1
Normal (white)
NOTE –PROVISIONAL DATA- STILL MODELLING
G& Acute Baseline:
Total beds available - 603
Of which is core bed stock – 442 ( in Winter)
Acute - 442
Maternity – 16 Paediatrics - 8
Of which are
• The organisations plans are in place for winter, escalation and surge.
• Daily operational meeting with clinical team within surgical business unit to assess elective for the day and capacity for emergency admissions.
• The Patient Flow Co-ordinator, DM and ARTOOH must monitor and report any surges in activity and report to DM’s and SLM’s if their Directorate is under pressure prior to or at the daily patient flow meetings.
• Patient flow meetings to be attended by the on call manager and
• A copy of the organisation winter plan communicated to NECS.
• Trust winter plan and escalation plan available on intranet site.
• Participate in the daily situation reporting (11am) during the winter monitoring months published on the winter planning and surge management website.
• Participate in daily teleconferencing during the winter reporting period chaired by North of
• Operational Patient Flow meetings x 3 daily - See bed meeting standard operating procedure.
• The patient flow co-ordinator with the Duty M has overall responsibility for managing the surge and capacity within the organisation
• Overnight this responsibility lies with ARTOOH and Senior Manager on Call
• Communication with AD/DOC as required.
•
• May be able to offer mutual aid to other organisations.

17
escalation beds -
Critical care capacity - 12
Level 1 -
Level 2 - 6
Level 3 - 6
High dependency unit – 6 (Level 2)
Average daily A&E attendances
Monday - 332
Tuesday - 298
Wednesday - 280
Thursday - 281
Friday - 271
Saturday - 310
Sunday - 325
Ambulatory care capacity – 10 patients
Average daily Acute admissions
Monday - 83
Tuesday - 79
alert any issues to the Director on Call via the telephone or E mail.
• Bed Predictions to be used at Bed Meetings..
• Action planning must follow the patient flow meetings and an action plan developed for evening/overnight.
• The Ward Manager/ senior nurse is responsible for 24/7 staffing cover for their area concerns must be raised through the Matron and the SLM if necessary.
• Late staffing issues to be highlighted at Patient Flow Meetings and resolution facilitated by Duty Clinical Matron.
• Patients identified for discharge to be taken to the discharge lounge as early as possible in the day even if the relatives are attending to take home.
• Test escalation areas are fit for purpose i.e. alarms and equipment are in good working order
• ED Co-ordinator to front all majors/resus triage.
• Board rounds on all wards.
• SAFER bundle principles in place
S – Senior review of all
England Commissioning Support Unit on behalf of the CCG.
• Flight deck information complete at 11am, 4.30pm and 8pm.
• Any escalation of NEEP levels to be communicated to the on call NECS Manager via the teleconference or directly.
• The organisations internal infrastructure Director/Senior Manager on Call system in place.
• Patient Flow Team presence on site 8am – 8pm 7 days a week.
• Duty Matron on site 8am-8pm 7 days a week
• SMOC • Daily analysis of
ED 4 hour breaches with issues communicated to relevant specialties,
• Daily Discharge facilitation meetings.
• The organisations internal on call

18
Wednesday - 74
Thursday - 74
Friday - 78
Saturday - 62
Sunday - 60
Average daily discharges required (Acute)
Monday - 80
Tuesday - 88
Wednesday - 83
Thursday - 78
Friday - 90
Saturday - 52
Sunday - 40
Average length of stay –
Elective (minus Daycase) – 3.5
Non-Elective – 5.0
During NEEP level 1, the organisation will be providing a full elective
patients before mid-day
A – All patients to have an expected day of discharge
F – Flow of patients, wards to pull patients from assessment unit to wards before 10am
E – Early discharge – 33% of patients from base wards to be in discharge lounge until TTO’s and letter before mid-day
R – Review all patients until extended length of stay (10-14 days) to have a management plan.
infrastructure is in place
• Weekly operational delivery group meetings
• Regular winter / surge planning meetings

19
programme:
Average daily electives required
Monday - 111
Tuesday - 127
Wednesday - 123
Thursday - 126
Friday - 112
Saturday - 25
Sunday - 7
Consideration to be given to the following Triggers to activate NEEP level 2
Three or more of the following indicators are hit.
INDICATORS
A&E
• 1 patient spending more than
4 hours in the ED (avoidable)
• 1 resus space and 1 majors
space
• Time from DTA to admission
1-2 hours
• 1-2 ambulance handovers >
15 minutes
NEEP 2 Concern
(green)
ALL ACTIONS AT NEEP 1 IN PLACE
Command and control - communications
• At the teleconferences NEAS/OOH via NECS to be informed of growing pressures within the Acute Trust
• Duty Matron to request additional matron, SLM support and support services representation at bed meetings.
• Team briefed of capacity issues all matrons/senior nurses to attend their respective areas to assess and to actively create capacity;
• Inform Communications
All communication within NEEP 1 will have been activated
All command and control actions in NEEP 1 will have been activated.
• Impact on
• May not be able to offer mutual aid.
• May not be able to attend external meetings
• May impact on NEAS
• Risks to KPI’s

20
EAU
• Pts on trolley >8hrs
• 0 cubicle availability 0-1hrs
Back of House
• Beds not available to receive
non elective patients (ie less
than one male and one
female bed available for each
non elective receiving areas)
• Insufficient capacity identified
in bed meeting for TCIs either
medicine or surgery
• Between 1 – 5 outliers in
other specialties
• No critical care bed
immediately available
• Ward staffing below agreed
levels by 1 – 3 nursing staff
across the site and is judged
to present a low risk to
patient safety
• No critical care beds available
at present and no movement
identified in the next few
hours.
Team of Escalation and ask for appropriate screen saver launch.
• Critical Care network to be informed if no beds and none imminent.
Ambulance queuing/ demand on A&E department
• ED Co-ordinator or ED Senior Dr
fronting triage
• Senior decision makers to front all services (minors and majors category) e.g. Consultant in Ambulatory care
• Ensure ED is adequately staffed with a transfer nurse and porters.
• Mobilisation of additional resources to assist with transfer of patients.
• Duty matron to liaise with A&E co-ordinator and consultant to activate A&E escalation plan.
Bed availability
• Identify patients to be moved to different speciality wards.
• Discuss with Bed Manager opening and staffing additional escalation beds
• Test escalation areas are fit for purpose i.e. alarms
• Early comms out to clinical teams re pressure being experienced..
• Enhanced liaison with co-ordinator on A&E & EAU.
• Communication to NECS & other organisations on teleconference call..
• Flight deck information complete at 11am, 4.30pm and 8pm.
Matron/SLM other commitments
• May impact on staff being able to attend meetings.

21
and equipment are in good working order
• Request additional consultant led patient reviews on all wards to identify patients suitable for discharge.
• Patients identified for discharge to be taken to the discharge lounge as soon as possible even if the relatives are attending to take home.
• Delays with discharge letter and pharmacy to be identified and to be given priority following discussion with medical teams to be coordinated by Ward Teams / Duty Matron.
• Community on call manager to liaise with Trust on call manager to ensure appropriate discharge and continuing to support patients within their own home to avoid unnecessary admissions.
• Elective teams to risk assess the continuity of the elective activity.
• Matron / SLM for elective care, Women’s and Children’s’ services and perioperative service manager to liaise with booking team to review lists of TCIs for the following day.
• Consideration of elective work in relation to back up for Critical Care
• Command and control will be as at NEEP 1.
• Consider SLM/SMOC presence at patient flow meetings if potential to escalate to NEEP 3.

22
• Identify 2 potential boarders on each ward by 1pm Patient Flow meeting.
Workforce
• At the discretion of Duty Matron the following to be in attendance at Patient Flow Meetings or contact made with: Clinical Support Services
Domestic Monitoring
IPC Nursing Team
Discharge Nurses
Ensure Staff Breaks are coordinated to allow sufficient flexible rest periods.
Consideration to be given to the following Triggers to activate NEEP level 3
Three or more of the following indicators are hit.
TRIGGERS
A&E
• Multiple patients
spending more than 4
hours in the ED
(avoidable)
• 0 resus spaces and 0
NEEP 3 Pressure
(amber)
Expectation that all actions from NEEP 2 have been considered and implemented. All available capacity opened and patients boarded
Command and control - communications
• At teleconference and through the SITREP report escalation of NEEP level to the NECS manager/ CCG on-call manager out of hours • Inform Communications
All communication within NEEP 1 and 2 will have been activated .
All command and control actions in NEEP 1 and 2 will have been activated.
• Impact on Matron/SLM/ AD other commitments
• Impact on study leave attendance
• Impact on meeting attendance
Risks to:
• Elective activity • KPI’s • Normal service
delivery
May impact on:
• NEAS • Ability to
repatriate from other hospitals
• Will have great difficulty in offering mutual aid

23
majors spaces
• Time from DTA to
admission 2-4 hours
• 4-8 patients stacking in
the ED awaiting
admission
• 2 ambulance handovers
> 15 minutes
EAU
• Pts on trolley >12hrs
• 0 cubicle availability
between 1-4hrs
Back of House
• Insufficient capacity to
accommodate non
clinically urgent TCIs in
either medicine or
surgery
• 5 – 14 outliers
• No critical care bed
available and no plan in
place for one to become
available in the next
four hours
• Ward staffing is below
agreed levels by 4 – 6
nursing staff across site
and is judged to present
a moderate risk to
patient safety
• No critical care beds
available and no
potential movement
identified over the next
few hours with difficulty
Team of Escalation for a bulletin to go to all staff re NEEP levels
• Director on call and Associate Director be informed of escalation to NEEP level 3
• Team briefed of capacity issues all matrons/senior nurses and SLM’s to attend their respective areas to assess and to actively create capacity;
• Request from NEAS pre-alert of all ambulances attendance to EAU if A&E under pressure
• Consider requesting HALO
• Critical Care network to be informed if no beds and none imminent by Critical Care
• Identify hot spots/process/patient flow pressure points for individual Directorates to be reported to the Patient Flow Team.
• Elective
Ambulance queuing/ busy A&E department
• Senior decision makers to front all services - minors and majors category
• Physician of the day/week to assist with assessment of patients in A&E for suitability of referral or discharge
• Patient flow co-ordinator
• DM to trigger NEEP 3.
• May need to request mutual aid from elsewhere.

24
transferring level 3
patients out because
regional position has
worsenend.
• Physician of the day/week to contact all medical consultants via voice bleep to advise of increased escalation
• Physician of the day/week to attend Bed Meetings to gain full briefing
• Physician of the day/week to consider moving junior staff to support pressure areas
• Physician of the day/week to ensure all sub specialty referrals are seen early in the day
• Physician of the day/week to consider cancelling elective activity for the afternoon and following day
• Refer to A&E escalation plan
Bed availability
• Additional escalation beds to be opened as documented in the winter plan.
• Additional consultant led patient reviews on all wards to identify patients suitable for discharge.
• Review of delayed discharges and accelerate discharge plans where possible involving Social Services and other relevant organisations.
to inform ward teams of increasing pressure.
• Patient flow co-ordinator to inform DM of increasing pressure.
• DM/ART OOH to inform SLM/SMOC of increasing pressure
• Voice over - bleep voice alert to all medical consultants to inform of escalation to NEEP 3. (See medical team action card in Escalation Policy.)
• Flight deck information complete at 11am, 4.30pm and 8pm
• DM to co-ordinate additional patient flow meetings when required.
• SLM/SMOC to attend 9am patient flow meetings.
• SMOC to attend additional patient flow meetings where required.
• SLM/SMOC to keep AD/DOC informed of situation.

25
• Request acceleration of patients waiting repatriation to other hospitals.
• Wards to prioritise the patients for radiology / scanning and pharmacy if this is all they are waiting for before they are discharged and to ensure Patient Flow Team informed.
• Ask Estates if there are any works that can be expedited should that free up bed capacity
• Consider a porter being assigned to patient flow Manager at a weekend
• Acute Care physician to be aware of potential (additional Consultant or Junior Medical support to be co-ordinated through the Medical Business Unit.
• Clinical Matrons and SLM’s to assist discharge co-coordinator/matrons/patient flow co-ordinator to influence all wards to encourage movement of discharged patients to the discharge lounge
• ACCEEP Critical Care plan will be triggered as per the regional ACEEP network agreement
• Daily Critical care command and control meetings will take place and plan for daily management of the

26
situation/pressures. • Community On Call
Manager will continue to liaise with Trust On Call Manager to ensure appropriate support for discharge and continuing to support patients within their own home to avoid unnecessary admissions.
• Consider additional weekend sessions for ultrasound and or CT as required
Workforce
• Review rotas with a view of cancellation of study leave based on individual assessment of both course and staff.
• Assess study leave – Business Units to identify case by case leave which can be cancelled and benefits provided to own or other areas.
• Close liaison with Nurse Bank – requesting additional bank staff where appropriate.
• Consider use of Practice Development Team Nurses / Specialist Nurses/ART to support ward areas.
• Consider the appropriateness of staff that are sent to help out on the ward. Ensure Staff Breaks are

27
coordinated to allow sufficient flexible rest periods.
Consideration to be given to the following Triggers to activate NEEP level 4
Three or more of the following indicators are hit.
• All actions from NEEP level 3 implemented with no significant improvement with capacity
• Critical Care patients exceed the physical bed spaces available of 17.
TRIGGERS
A&E
• Multiple patients spending
significantly longer than 4
hours in the ED
• No capacity to receive
patients
• Time from DTA to admission
>4 hours
• >8 patients stacking in the ED
awaiting admission
• Ambulances queuing to
4 NEEP
Severe Pressure
(red)
Expectation that all actions from NEEP 3 have been considered and implemented. All available capacity opened and patients boarded
Cancellation of all electives with the exception of priority 1.
Command and control - communications
• Continue managing situation as a surge and escalation incident.
• Through the daily teleconference and SITREP report escalation of NEEP level to the NECS manager/ CCG on-call manager out of hours
• Inform Communications Team of escalation
• Director on call to be informed of escalation to NEEP level 4
• Consider calling additional local teleconference with CCG, Local Authority, Community Services and NEAS
• At NEEP level 4 designated Director on Call, AD’s, and SLM’s to
All communication within NEEP 1,2 and 3 will have been activated.
• AD/DOC is to be kept informed of situation by SLM/SMOC
• DM/ART OOH to
All command and control actions in NEEP 1,2 and 3 will have been activated.
• Impact on Matron/SLM/ AD other commitments
• Impact on study leave attendance
• Impact on meeting attendance
• The need to cancel routine work will impact on KPI’s and reputation.
• Financial cost of additional resource brought in.
Risks to:
• Elective activity • KPI’s • Normal service
delivery
May impact on:
• NEAS • Neighbouring
Trusts • Ability to
repatriate from other hospitals
• Will not be able to offer mutual aid to other organisations.
• Will need to request mutual aid from other organisations.

28
handover
EAU
• Pts on trolley >24hrs
• 0 cubicle availability >4hrs
Back of House
• Insufficient capacity to
accommodate TCIs in either
medicine or surgery who are
clinically urgent
• >15 outliers in other
specialties
• Ward staffing is below agreed
levels by 7+ nursing staff
across site
• No critical care bed available,
no place in place for one to
become available in the next
four hours and no scope for
escalation of critical care
capacity
report to Gold Command. Activation of their Business Continuity Plans with regard to cancellation of elective procedures and continuity of core services.
• NEAS/OOH via NECS to be informed of growing pressures within the Acute Trust by the daily teleconference and SITREP
• Team briefed of capacity issues all matrons/senior nurses and SLM’s to attend their respective areas to assess and to actively create capacity
• Continued communication with NEAS re: pre-alert of all ambulances attendance to EAU
• Continued communication with Critical care network if no beds and none imminent
Ambulance queuing/ busy A&E department
• Senior decision makers to front all services - minors and majors category
• Physician of the day/week to assist with assessment of patients in A&E for suitability of referral or discharge
• Additional consultant to be commandeered to support the on call Consultant to be co-ordinated by the
ensure SLM/SMOC aware of situation and to request on-site presence when necessary.
• SLM/SMOC to request DOC to seek mutual aid.
• Flight deck information complete at 11am, 4.30pm and 8pm.
• SLM/SMOC to escalate to AD/DOC the need for setting up Gold Command.
• DOC to assess situation with SMOC and determine if on-site presence is required.

29
Medical Director • Request mutual aid from
neighbouring organisations in accordance with the Mutual Aid Policy
Bed availability
• Consider opening additional beds.
Produce list of potential elective cancellations which have been assessed on a case by case basis.
Cancellation of all electives with the exception of priority 1. Must take place when organisation at NEEP 4.
• Review of medical outpatients to be undertaken with potential to cancel non urgent outpatient appointments to free up medical consultants to attend ward rounds.
Workforce
• Assess study leave – Business Units to identify case by case leave which can be cancelled and benefits provided to own or other areas.
• Close liaison with Nurse
.

30
Bank – requesting additional bank staff where appropriate.
• Consider use of Practice Development Team Nurses / Specialist Nurses/ART to support ward areas.
• Consider the appropriateness of staff that are sent to help out on the ward. Ensure Staff Breaks are coordinated to allow sufficient flexible rest periods.
Consideration to be given to the following Triggers to activate NEEP level 5
Three or more of the following indicators are hit.
TRIGGERS
EAU
• Pts on trolley >36hrs
• 0 cubicle availability >8hrs
Back of House
• Negative bed state in either
medicine or surgery with
escalation areas open &
continued A&E/EAU triggers
• Ward staffing is below agreed
levels by 7+ nursing staff
across the site and is judged
to present a high risk to
patient safety
NEEP 5
Critical
(purple)
• ACTIVATION OF MAJOR INCIDENT PLAN (as per policy)
All communication within NEEP 1,2,3 and 4 will have been activated.
• On activation of major incident plan all stakeholders identified within plan will establish communications through command and control
All command and control actions in NEEP 1,2,3 and 4 will have been activated.
• Gold command at SHA
• Silver command NECS and Trusts
• Bronze command Trust
For discussion consideration of impact on:
• mental health • Primary Care
(via NECS) • Neighbouring
Trusts • Community
Directorate • GPs
• Risks to Targets
• Normal service delivery
• Elective activity

31
NEEP 6
Potential Service
Failure
(black)
• CONTINUE WITH MAJOR INCIDENT/BUSINESS CONTINUITY PLANS SIMULATNEOUSLY WITH STAND BY TO INITIATE RECOVERY PHASE ( as per policy)
• As NEEP level 5 • As NEEP level 5
For discussion consideration of impact on:
• mental health • Primary Care
(via NECS) • Neighbouring
Trusts • Community
Directorate • GPs
• Risks to Targets • Normal service
delivery • Elective activity

32
ED ED Specific Triggers ED Co-ordinator Actions ED Senior Doctor* Actions
Level 1
• functioning safety and 4 hour target consistently being delivered
• <40 patients in the ED
• 1 resus space and >2 majors spaces
• Time from DTA to admission < 1 hour
• No delays with ambulance handovers
• Adequate staffing in the ED
• Normal working practice
• Maintain lines of communication with duty
matron and bed manager
• Review staffing for next 24 hours
• Normal working practice
• Consider attending EAU handover at 8pm to touch
base
Level 2
At least
three
triggers to
be present
to trigger
this level
• 1 patient spending more than 4 hours in the ED (avoidable)
• 40-50 patients in the ED
• Influx of patients arrived or expected (>10 in 1 hour)
• 1 resus space and 1 majors space
• Patients waiting >2 hours to see a doctor
• Time from DTA to admission 1-2 hours
• 1-2 ambulance handovers > 15 minutes
• Borderline staffing in the ED
• Redeploy nurses to high pressure ED areas
• Alert EAU co-ordinator and request attendance to
jointly look at board, see if any patient can be
moved immediately
• Alert duty matron and request support in
addressing the delays in moving patients to
EAU/wards
• Address any nursing staffing shortfalls
• Redeploy doctors to high pressure ED areas
• Ensure that ED patients have early senior review
• Contact registrar or consultant of specialty teams if
there is a delay (>30 minutes) from specialty teams to
see patients in the ED
• Address any ED medical staffing shortfalls
• Re-triage all patients to potentially re-allocate to
different work streams
• Liaise with EAU consultant
Level 3
At least
three
triggers to
be present
to trigger
this level
• Multiple patients spending more than 4 hours in the ED (avoidable)
• 50-60 patients in the ED
• >10 pts arrived in ED per hour over 3 consecutive hours
• 0 resus spaces and 0 majors spaces
• Maximum of 4 in holding corridor
• Time from DTA to admission 2-4 hours
• 4-8 patients stacking in the ED awaiting admission
• 2 ambulance handovers > 15 minutes
• Significant staffing shortages in the ED
• As above plus:
• Request nursing staff support from other
departments
• Liaise with duty matron to identify specialty help
that could be utilised in the ED
• Clinical staff on non-clinical duties to support
patient care
• Minor injuries shift lead to look at ED queue to
see what could be pulled through to them
• Reception staff to inform patients on arrival of
waiting time
• Refer to Ambulance Handover SOP – Appendix 6
• As above plus:
• Identify patients that could safely be moved directly to
EAU/SSU/wards
• Re-review patients ? can patient go home rather than
admission
• Refer to Ambulance Handover SOP – Appendix 6
Level 4
At least
three
triggers to
be present
to trigger
this level
• Multiple patients spending significantly longer than 4 hours in the ED
• >60 patients in the ED
• >10 patients arrived in ED per hour over 4 consecutive hours
• No capacity to receive patients
• Time from DTA to admission >4 hours
• >8 patients stacking in the ED awaiting admission
• Ambulances queuing to handover
• Inadequate staffing in the ED
• As above plus:
• Create additional majors capacity by utilising
minors pods
• Utilise additional resus capacity
• Refer to Ambulance Handover SOP – Appendix 6
• As above plus:
• Clinical staff on non-clinical duties to support patient
care
• Consider curtailing WIC work and utilising cubicles
• Refer to Ambulance Handover SOP – Appendix 6
Appendix 3 ACCIDENT & EMERGENCY LOCAL ESCALATION PLAN

33
ECCA ESCALATION PLAN
ECCA Triggers for Alert levels ECCA Specific triggers ECCA Co-ordinator Actions ECCA Senior Doctor’s Actions
Level 1
• Business As Usual
• Ensure minimum of 3
spaces available at all
times
• Good flow of patients in
and out of department
• No delays with discharges
• Adequate staffing levels
achieved
• Normal working practice
• Maintain lines of communication with ED Co-ordinator, SSU Co-
ordinator, duty matron, emergency bed manager and Acute Physician
• Liaise with bed manager, SSU / ACC co-ordinator to plan to create space
• Normal working practice
Level 2
• <5 patients in
admissions requests
list on Medway
• potential limited space on
ECCA
• Staffing in line with
planned safe staffing levels
• Co-ordinator ensures spaces available to accommodate ALL impending
admission requests – transfers and discharges performed in a timely
manner and directs nursing staff and doctors to complete paperwork in
real time
• Actual staffing levels are suitable for department to function without
assistance from elsewhere
• Address any medical staffing issues
Level 3
• > 5 patients in
admissions requests
list on Medway with
limited space on
ECCA to
accommodate
• No current capacity for
patient requiring a bed
GP or A&E
• Greater than 5 patients
awaiting nurse assessment
As above plus
• If expected GP referral, Co-ordinator reads GP letter and assesses if
immediate bed required or suitable for ACC or ‘holding corridor’
• If suitable for ACC, co-ordinator contacts ACC Nurse in charge via vocera
and requests a transfer upstairs – staff member assigned to transfer
• If bed immediately required then identifies a patient to move elsewhere
– base ward /ACC/SSU and liaises with bed managers to locate available
space
• If bed not immediately required , assigns a staff member to ‘holding
corridor’ and performs a set of obs to ensure patient safety
• Co-ordinator contacts SSU co-ordinator and ACC nurse in charge via
vocera to assess if any staff could be released to supervise ‘holding area’
– if not then escalates to duty matron
• Duty matron to attend ECCA and assess
• Co-ordinator escalates to duty matron
• Duty matron attends ECCA and discusses situation with co-ordinator
• Duty matron and co-ordinator looked at staffing levels of all areas on
ECC via electronic staffing grid and staff requested from other areas to
help complete nurse assessments
• Duty matron to temporarily take over Co-ordinator role to free up co-
ordinator to nurse assess
As above plus
• Should A&E have x1 ambulance
delay then Acute Physician should
meet up with A&E Consultants and
identify patients to pull through
• Ensure medics are aware of joint /
shared roles and responsibilities to
assist with assessments of patie
Appendix 4

34
• Greater than 5 ECCA
patients awaiting junior
doctor clerking
• Greater than 5 patients
awaiting Consultant review
• Staffing levels below
planned levels and actual
levels are causing a backlog
in nursing assessments
taking place
• Co-ordinator escalates to Acute physician and duty matron and
discussion to take place with Acute physician from SSU
• Co-ordinator to contact duty matron and then to liaise with Acute
Physician for ECCA and Physician of the day from SSU
• ECCA co-ordinator to liaise with SSU &ACC co-ordinator’s and also A&E
co-ordinator to discuss staffing levels across the floor and then staffing
moved to where deficit is showing – duty matron informed as to
potential staff movement
• If ECCA bottleneck or potential –
ask wards with 3 or more doctors
present to send someone to ECCA
to assist with clerking – ask on call
doctors due to start at 5 pm to
leave base wards and attend ECCA
earlier
• Acute Physician contacts Dr’s Scott
/ Naryanan to request additional
consultant support – out of hours
patients can be moved to base
wards without a Consultant review
/ providing a registrar or band 7
from ART has reviewed patient. A
list should be made of such
patient’s on Friday / Saturday
nights for weekend Consultant
doing ward rounds on Saturday &
Sunday to review the patients’ on
the base wards the following day.
Base ward nurses should ensure
that if they are concerned about a
patient, ECCA are informed so that
the patient can be prioritised to be
seen.
Level 4
• > 5 patients in
admissions requests
• No space available in
‘holding area’ and no beds
available for immediate
As above plus
• EAU co-ordinator liaises with A&E co-ordinator to negotiate potential
space in majors until space in ECCA is available recognising the patient
MUST be filtered back through ECCA when space created.

35
list on Medway with
NO space on ECCA to
accommodate
transfer and patient arrives
into ambulance area who
requires ECCA
• Inadequate staffing in ECCA
despite attempts to be self
sufficient across ECC
• ECCA co-ordinator contacts duty matron who will liaise with bed
managers to assist with base wards identifying suitable space as quickly
as possible. A transfer list will be compiled from ECCA patients,
identifying who is ready to move first.
• SSU co-ordinator contacted to identify any patients who could wait in
ACC and release a bed then a suitable ECCA patient to transfer up
without review / clerk for this to be performed on SSU (in hours)
• ECCA co-ordinators to liaise with duty matron nd emergency bed
managers to request staff movements from other areas of the Trust i.e.
Clinical staff on non- clinical duties to support patient care

36
KEY PERSONNEL ACTION CARDS
Actions for the Bed Managers
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
Handover from the ART Team Undertake all actions identified
at Level 1
Undertake all actions identified
at Level 1
Undertake all actions identified
at Level 1
Support Gold Command
Walk around the wards to
establish bed status
Work closely with the Duty
Matron and Service Line
Manager
In liaison with the Duty Matron
and Service Line Manager
identify patients to be moved to
other areas
Ring around the wards to
establish the nurse staffing
levels
Work closely with the Duty
Matrons to identify critical care
potential
Ensure patients requiring
repatriation are identified at the
bed meetings and included in the
action plan
Take all decisions to admit, eg
GP referrals or admissions from
clinics, outliers and repatriations
Attend the bed meetings - 9.30
am, 1.30 and 4.45 pm and take
the information relating to bed
status. Email bed status after
the bed meetings
Identify predicted/potential
discharges across the site
Work closely with coordinators
on EAU, ED and short stay -
coordination in terms of what is
coming in
Appendix 5

37
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
Monitor patients in ED - coming
up to three or four hours -
working with ED Coordinator to
establish a plan
Collect the Boarders List
Communicate regularly with
Duty Matron
Handover to the Acute Response
Team (ART) at 8pm
Monitor and consider who is on
call – Vascular
In liaison with the Duty
Matron/Service Line Manager
manage the elective admissions
ensuring identification of beds
required for next day admissions
In liaison with the Duty Matron
and SLM ensure that all beds are
open
Work with Ward Managers to
identify patients for specialty
wards
Keep wards informed of current
NEEP status

38
Actions for the Duty Matron (Cover 7.30 am – 5.00 pm)
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
All actions included in Business
as Usual (BAU)
Ensure completion of all Level 1
/BAU actions
Ensure completion of all Level 2
actions
Review ensure plans are in place
to de-escalate to level 3
In liaison with the Director on
Call and the Senior Manager on
call instigate Gold Command
Participate in handovers with
ART team lead at 07.30
Review & ensure plans are in
place to de-escalate to level 1
Review & ensure plans are in
place to de-escalate to level 2
Cancel all non-clinically urgent
elective surgery in discussion
with SMOC/SLM’S/ Director on
Call
Call in all staff identified in this
Policy who have Action Cards
Chair and co-ordinate bed
meetings at 9.30, 1.30 and 4pm
as per agreed Standard
Operational Procedure (Appendix
1a)
Co-ordinate response to
increasing pressures across the
Trust
Initiate communication with
senior clinicians/Consultants to
expedite review of patients
Review forward staffing plans. In
conjunction with SMOC consider
cancellation of planned non-
clinical time / training for front
line staff and backfill onto areas
under pressure
Consider cancelling all outpatient
activity to provide additional
ward input in discussion with
SMOC / Director on Call
Continue to work with Gold
Command
Take lead in ensuring actions
from bed meetings are
completed
In liaison with ED co-ordinator
and Consultant activate ED
escalation plan – Appendix 3
Contact Nurse Bank to request
additional bank staff into areas
under pressure where
appropriate
Discuss with SMOC request for
mutual aid
Request site presence and
support of SMOC if not already in
attendance
Agree SITREP with Service Line
Manager in Medicine by 10am.
Discuss any escalation to Level 2
with SMOC
Request additional resources to
assist with transferring patients
to maintain patient flow
Chair and co-ordinate more
frequent bed meetings as
required
Discuss with SMOC / Director on
Call potential need to escalate to
level 5 and instigation of gold
command.
Raise any issues with Senior
Manager on Call or SLM by
EXCEPTION ONLY
Request additional Matron, SLM
support and Support Services
representation at bed meetings if
required
Consider request for mutual aid
with SMOC if appropriate
Request additional Consultant
led patient reviews for all
specialities under pressure to
In conjunction with SMOC
develop plan for drafting in
additional medical staff to
support areas under pressure

39
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
identify patient suitable for
discharge
Will be required to act as first
point of contact for requests for
mutual aid from other Trusts
with ED co-ordinator / Lead
Consultant and advise SMOC /
Director on Call
Escalate issues regarding delayed
discharges of medically fit
patients to SLM’s within Business
Units or SMOC
Discuss with SMOC and Director
On Call any agreement in
escalation to Level 4 with
review/agreement of plan
Redeploy nurses from non-ward
based areas.
In conjunction with Ward /
Department Managers, 1104 and
1200 Bleep holders identify
patients for boarding using
boarding criteria tools
Consider extended opening and
use of discharge hospitality
lounge
Required to act as first responder
in event of adverse / serious
untoward incident e.g. missing
patients, serious drug incidents,
MAJAX
Agree with SMOC the planned
order of escalation into other
wards / departments as set out
in the winter plan.
Appendix 7
Request Site Presence of Senior
Manager on Call if needed.
May be required to act as a first
point of contact for press
enquires and discuss with SMOC
/ Director on Call
Discuss with SLM’s / SMOC any
agreement in escalation to Level
3 with review/agreement of plan
Opening and staffing of
escalation beds / areas based
upon speciality requirements /
pressures
Discuss potential request for
mutual aid within specialities
with ED Consultant and SMOC
In conjunction with ward /
department managers ensure
that proactive discharge planning
is occurring e.g. EDD, discharge
plans, working with DLT / social
services
Communicate closely with SMOC
in hours and where necessary
escalate any issues causing
concern
Discuss with SMOC and Director
on Call any agreement in
escalation to Level 4 with review
/ agreement of plan

40
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
Agree communication plan for
evening with Senior Manager on
Call at 4.30pm bed meeting – NB
reporting should be by
EXCEPTION ONLY
Ensure completion of all Level 1
/BAU actions
In liaison with Surgical
Consultants, SLM’s and Theatres
prioritise elective admissions and
consider cancellation of non-
urgent cases.
Communicate closely with SMOC
and where necessary escalate
any issues causing concern
Participate in handover with ART
team lead at 20.00
Review & ensure plans are in
place to de-escalate to level 1
Where required provide
handover to Duty Matron for
following day via email or
telephone call
Co-ordinate response to
increasing pressures across the
Trust
In liaison with ED co-ordinator
and Consultant activate ED
escalation plan
Request site presence of SMOC
as necessary
Communicate closely with SMOC
out of hours and where
necessary escalate any issues
causing concern

41
Actions for the Duty Matron (Cover 5 - 8.30 pm)
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to patient
safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
All actions included in BAU Ensure completion of all Level 1
/BAU actions
Ensure completion of all Level 2
actions
Request site presence and
support of SMOC if not already in
attendance
In liaison with the Director on
Call and the Associate Director
for the Business Unit instigate
Gold Command
Agree communication plan for
evening with Senior Manager on
Call at 4.30pm bed meeting – NB
reporting should be by
EXCEPTION ONLY
Continue with identified Duty
Matron actions 07.30-17.00
Continue with identified Duty
Matron actions 07.30-17.00
Call in all staff identified in this
Policy who have Action Cards
Participate in handover with ART
team lead and Senior Manager on
Call at 20.00
Request site presence of SMOC
as necessary
Request site presence of SMOC as
necessary
Where required provide
handover to Duty Matron for
following day via email or
telephone call
Discuss with SMOC any
agreement in escalation to
Level 3 with review/agreement
of plan
Discuss request for mutual aid
within specialities with ED
Consultant and SMOC
May be required to act as first
point of contact for PALS and
Complaints
Communicate closely with
SMOC out of hours and where
necessary escalate any issues
causing concern
Discuss with SMOC and Director
on Call any agreement in
escalation to Level 4 with review /
agreement of plan
Required to act as first responder
in event of adverse/serious
untoward incident e.g. missing
patients, serious drug incidents,
MAJAX
Ensure completion of all Level 1
/BAU actions
Communicate closely with SMOC
and where necessary escalate any
issues causing concern
May be required to act as a first
point of contact for press
enquires and discuss with SMOC /
Director on Call

42
Actions for the Service Line Manager and Senior Manager on Call
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
SMOC to attend 4pm bed
meeting for handover into the
evening
Review and ensure plans are in
place to de-escalate to Level 1
Review and ensure plans are in
place to de-escalate to Level 2
Review and ensure plans are in
place to de-escalate to Level 3
Consider launching Gold
Command in discussion with
Associate Director and Director
on Call
Consider requests for mutual aid
with A&E/EAU co-ordinators.
Discuss with DoC if required
Agree and support as required
mobilisation plan for escalation
into the designated Escalation
areas
Initiative communications with
senior clinicians to expedite
review of patients
Cancel non-urgent elective work Site presence required
Contact ARTOOH between 9-
11pm for current situation
Discuss with Duty Matron/ART
escalation to Level 3 with
review/agreement of plan
In liaison with Duty Matron and
Surgical Consultants prioritise
elective admissions identifying
those who may be able to
attend as same day admissions
Site presence required
Handover issues to SMOC 9am at
weekends
Attend complex discharge
meeting (12.30 pm in the Agile
area) and support Duty
Matron/Patient flow in
accelerating all potential
discharges
SLM presence
Proactively inform CCG of
position and mitigating actions
Point of contact for press
enquiries, discuss with Director
on Call (all levels)
Consider cancelling of some
non-urgent elective work
Instigate requests for mutual aid
following discussion with DoC
Discuss with Matron/ART
escalation to L2
Agree and support as required
mobilization plan for escalation
into identified areas
Contact Local Authority and
Social Care with a view to
commissioning additional
community beds to accelerate
discharges
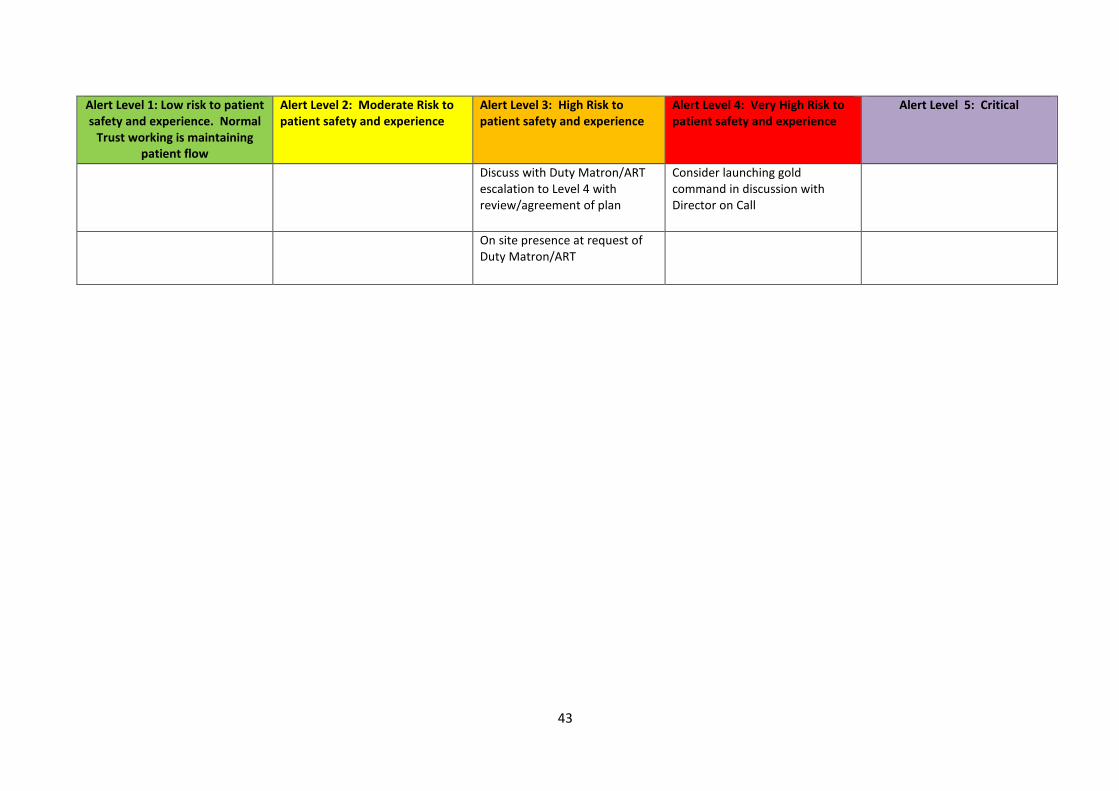
43
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
Discuss with Duty Matron/ART
escalation to Level 4 with
review/agreement of plan
Consider launching gold
command in discussion with
Director on Call
On site presence at request of
Duty Matron/ART

44
Actions for Senior Manager on Call from 5pm and weekends
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
Participate in handover with
Duty Matron at 8 pm
Consider site presence at request
of Duty Matron/ART
Participate in 8 pm Handover
Meeting
Discuss with Director on Call
request for mutual aid
In liaison with the Director on
Call and the Duty Matron Unit
instigate Gold Command
Appropriate handover to Senior
Manager on Call 9 am Saturday
and Sunday
Discuss with Duty Matron/ART
escalation to Level 3 with review
and agreement of plan
At 9 am on a Saturday and
Sunday Senior Manager to Senior
Manager On Call telephone
handover
Consider launching Gold
Command in discussion with
Director on Call
Site presence required
Consider requests for mutual aid
with A&E/EAU coordinators and
Duty Matron/ART and advise
Director on Call for decision (at
all levels)
In liaison with the Duty Matron
devise and implement a plan to
reduce further risk
On site presence Site presence required
Point of contact for press
enquiries, discuss with Director
on Call (at all levels)
Consider site presence at request
of Duty Matron/ART
Discuss with Director on Call
request for mutual aid
Discuss with Duty Matron/ART
escalation to Level 4 and inform
Director on Call with
review/agreement of plan
Point of contact for press
enquiries – liaise with Director on
Call relating to these

45
Actions for the Senior Manager on Call (from 5 pm)
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
Participate in handover with
Duty Matron at 8 pm
Consider site presence at
request of Duty Matron/ART
Participate in 8pm handover
meeting
Discuss with Duty Matron/ART
escalation to Level 4 and inform
Director on Call with
review/agreement of plan
In liaison with the Director on
Call and the Duty Matron Unit
instigate Gold Command
Appropriate handover to Senior
Manager on Call 9 am Saturday
and Sunday
Discuss with Duty Matron/ART
escalation to Level 3 with review
and agreement of plan
At 9am on a Saturday and
Sunday Senior Manager to
Senior Manager on Call
telephone handover
Point of contact for press
enquiries – liaise with Director
on Call relating to these
Site presence required
Consider requests for mutual aid
with A&E/EAU coordinators and
Duty Matron/ART and advise
Director on Call for decision (at
all levels)
In liaison with the Duty Matron
devise and implement a plan to
reduce further risk
On site presence
Point of contact for press
enquiries, discuss with Director
on Call (at all levels)
Consider site presence at
request of Duty Matron/ART
Discuss with Matron/ART
escalation to Level 2

46
Actions for the Acute Response Team Band 7 Role (Cover 20:00pm – 08:00am)
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
Joint handover with the Bed
Manager and Duty Matron
Identify potential outliers, plan
to potentially transfer to other
specialties
Report escalation of NEEP level
to the Senior Manager on call
Undertake all Levels 1, 2 and 3 Constant communication with
Duty Manager, Director on Call
Agree overall alert status level
for the Trust
Transfer outlier to given wards
in a timely manner ,preferably
before 22:00
Working with Senior Manager on
Call
Identify any areas for
intervention or where extra
resource is required and agree
and arrange
A&E clinician, and Consultants on
Call
Establish any Staffing issues Ensure ECC is adequately staffed
with a transfer nurse and porters
Liaise with Ward Teams to
identify all patients who can be
transferred to non- medical
wards
Preparation of escalation areas
to open ensuring adequate staff
for overnight but also plans to
staff these areas for the morning.
Support Gold Command
Looking at predicted/potential
discharges across the site
Keeping in close touch with the
EAU coordinator and A & E
coordinator to enable prediction
of patient flow
If possible to allocate help from
other departments to support
ECC with Transfers
Contact the Medical Lead to gain
additional input from the medical
staff
Emergency list of elective
patients and telephone numbers
to prepare for potential
cancellation of procedures.
Monitoring patients in ED -
coming up to three or four hours
- working with the ED
Coordinators
In liaison with A&E activate the
A&E Escalation Plan (see
Appendix 3)
Ensure that all beds are open and
utilised
Staff to be prepared to inform
patients that there may be
decisions made to discharge
those patients whose elective
surgery is planned for the next
day
Collect a Outliers List from base
wards
Consider opening and staffing
additional escalation beds
Work with medical teams and
nursing staff to identify further
discharges for am
Contact should be made with
Duty Manager and Director on
call for support and guidance
potential requests for divert.

47
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
Communication with EAU and
Short Stay to establish if any
patients can be transferred to
other specialty wards as outliers
In the Request additional
consultant led patient reviews on
all wards to identify patients
suitable for discharge
To collect data regarding elective
admission in each area and
ensure this is communicated to
Bed Managers and Duty Matron
in am
Ensure any decision relating to
divert is discussed with Senior
Manager on Call, Director on call
A&E Clinician, A &E coordinator.
Looking at predicted/potential
discharges across the site
Ensure all identified patients for
discharge have plans in place to
ensure speedy transfer to the
Discharge Lounge for the
opening in the am
Liaise with all high patient flow
areas frequently including areas
such as Critical Care , Maternity ,
Theatres and Paediatrics
regarding acuity and dependency
of patients
Visit all Wards and identify areas
which may be struggling
including visiting A&E
Coordinating response to
increasing pressures across the
site
Communication across the site to
advise all areas and staff who are
on duty.
Communication in am to Bed
Manager and Duty Matron
Facilitation of conversations
between clinicians to ensure that
the patient flow continues
Electronic Morning report to be
sent with relevant information
Contact Senior Manager on Call
following regarding bed status
early evening
Communication in am to Bed
Manager and Duty Matron
Electronic Morning report to be
sent with relevant information
regarding trust Status and Issues
overnight

48
Actions for the Director on Call
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
Business as usual Business as usual Expect an update from Senior
Manager on Call re current status
and plans in place
Site presence may be required
following discussion with the
SLM On Call
Following discussion with the
Senior Manager on Call
Implement Gold Command’ –
site presence required
Respond to any issues escalated Support with any issues as
needed
SMOC will make decisions re
receiving diverts but may require
advice/support
Establish base in Bed Bureau for
Gold Command
Support with Mutual Aid
requests from our Trusts to
others
If we are receiving a divert
ensure this is discussed with
SMOC, A&E Consultant and
Co-ordinator and Duty Matron
Set up Control Team
• Medical Director
• Associate Director
• Duty Matron/ARTOOH
• Senior Manager on Call
• Bed Manager
• A&E Consultant or
representative
• Consultant Physician on Call
• Consultant Surgeon on Call
Use Flight Deck information to
aid decisions re from whom to
contact re Mutual Aid
Check all non-urgent elective
activity is cancelled as
appropriate
Plan of action to be developed
- To include releasing clinical
staff from non-clinical duties
- Cancel all but essential
elective activity
- Re direction Walk-in activity
from A&E Minors
Prepare to support requests for
diverts from other Trusts – refer
to Flight Deck information
- Agree communications plan
- Discussion with
CCG/NECS/Local Authority/
Community Services Lead

49
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
Contact NEAS Duty Manager to
notify the position at the Trust
and advise the Trust is looking to
divert elsewhere Advise NEAS of
any agreements made with
regards to diverts
Prepare to request divert to
other Trusts
Consider communication with
CCG/NECS/ Local Authority/
Community Services Leads if
situation is ongoing and
burdening NEEP 5

50
Actions for the Medical Teams, Consultants and Clinical Lead
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
Ward Consultant/Medical Team
Actions (standard expected
practice):
Business as usual
Lead Consultant in speciality
communicates the situation and
actions required. Consultants in
teams with inpatients, and with
the relevant ward manager/s.
Once communication is received
from designated bed
manager/coordinator ensure this
is communicated to all medical
consultants via voice bleep
Once communication is received
from designated bed
manager/coordinator ensure this
is communicated to all medical
consultants via voice bleep
Once communication is received
from designated bed
manager/coordinator ensure this
is communicated to all medical
consultants via voice bleep
Support Gold Command – on site
presence required
Ensure daily consultant or SpR
ward round in the morning as
per SAFER Flow Bundle:
Discuss with other consultants in
sub-speciality AND ensure a
consultant-led or SPR led ward
round takes place on the base
ward in the morning
Where possible attend bed
meeting(s) to get full briefing
Attend bed meeting(s) to get full
briefing
If above not possible ensure SpR-
led ward round with report to
consultant
Liaise with Business Unit Lead to
check on medical staffing levels
within the department and
identify any potential gaps
Liaise with the Business Unit
Lead or deputy to re-deploy
medical staff if needed
S – Senior Review – Aim for
senior review of all patients on
base wards by midday
Ensure every patient has an
‘early’ discharge plan with
criteria for nurse-led discharge
documented if appropriate
Check that all actions above have
been taken and review as
necessary
Contact colleagues to discuss if
any support is needed to ensure
above actions are completed
o Aim to see potential
discharges after
sick/unstable patients
Highlight patients waiting for
social services sort out and
medically fit on Medway and to
ward manager
Update duty matron by
telephone
Discuss cancelling elective
activity with sub-speciality
colleagues and divisional team

51
Alert Level 1: Low risk to patient
safety and experience. Normal
Trust working is maintaining
patient flow
Alert Level 2: Moderate Risk to
patient safety and experience
Alert Level 3: High Risk to
patient safety and experience
Alert Level 4: Very High Risk to
patient safety and experience
Alert Level 5: Critical
o Hand Over Form (HOF)
completed real time
Liaise with AC if there are any
inpatients on your ward suitable
for this pathway
If junior staffing levels allow
consider offering help to other
areas like EAU
o Identify patients likely to go
home the following day and
update EDD for all patients
Contact other sub-speciality
consultants by phone if any
patients on the ward are waiting
for another consultant’s opinion
(includes on EAU & SSU)
Ensure all sub-speciality referrals
are seen early in the day
A – All patients should have an
EDD
Consider cancelling elective
activity for the afternoon and
following day if possible
o Aim to set EDD within 24
hours of arrival on base ward
o Communicate this date to
patient and relatives/carers

52
Standard Operating Procedure
Monitoring A&E Ambulance Handover Breaches
• A&E Co-ordinator to monitor handover breaches on designated proforma
• Proforma to be scanned and sent to Pam Naylor / Chris Wright on a daily basis by Night
Site at 4.00am with 4 hour breach sheet
• Night Site Team and Bed Managers, during the day, to detail on bed report
o Number of Ambulance Handover delays 15-30 minutes
o Number of Ambulance Handover delays 30-60 minutes
o Number of Ambulance Handover delays over 1 hour (black breaches)
• NEAS provides the electronic information about Ambulance Handover delays to our
Information Department
• Information Department to send this information to Chris Wright / Pam Naylor for
validation against the proforma completed by A&E Co-ordinator
• Number of Ambulance Handover delays performance and subsequent action planning to
be discussed at monthly Emergency Care Service Line meeting attended by Senior staff
within the service
• Issues / concerns to be escalated to Associate Director
Appendix 6

53
Standard Operating Procedure
Escalating A&E Ambulance Handover Breaches
• A&E Co-ordinator to monitor capacity in Department against expected arrivals
• If capacity is not sufficient to meet expected demand contact Bed Manager to inform
and further assess nature and origin of patients coming in to decide plan for movement
of patients requiring admission
• If no patients deemed ready to move A&E Co-ordinator and Bed Manager to speak to
shop floor Consultant and agree most suitable to be moved
• If not able to create immediate capacity due to pressure on EAU spaces, A&E Co-
ordinator/ Bed Manager to contact Duty Matron / Night Site to initiate plans for freeing
up beds
• Any Ambulance Handover waits that have gone above 15 minutes A and E Co- ordinator
to contact Bed Manager and Duty Matron / Night Site if not already involved. Discussion
to also take place with Senior Doctor.
• Any waits above 30 minutes, Duty Matron / Night Site to attend, if not involved already,
and liaise with Co-ordinator and Senior Doctor to agree plans
• Senior Manager on Call to be informed if breaches above 30 minutes are anticipated.
SMOC to check all appropriate escalation actions across the patient pathways and above
actions have taken place. Work with on- site teams to develop on- going plan- consider
opening additional capacity, requesting mutual aid (use Flight Deck information to help
inform).
• SLM/ SMOC to be informed if any black breaches (over 1hr) anticipated.
• If anticipated to be an on- going situation SMOC to discuss the situation with the
Ambulance service to flag the pressures. SMOC to contact Associate Director/ Director
on Call to advise of situation and further discuss request of Mutual aid/ on- going plans.
• If any black breaches occur Duty Matron / Night Site and SLM / SMOC to write report to
outline events and to record any learning. This should be submitted to Associate
Directors with SLMs and Matrons copied in for discussion at Business Unit Boards and at
Board to Board meetings.
Appendix 6







