Download - Brugada case-presentation
Case PresentationBy
Islam GhanemCardiologist
Think For A minute, You may Save A life
Rare case diagnosed in El Ansar hospital
The first time to see This
Rare SYNDROME
* 40 years old male patient, smoker, no HTN, no DM.
*Two years ago he had fainting attack, non typical chest pain.
*Misdiagnosed in Yemen as Cardiac Ischemia,,, Again 1 year ago misdiagnosed in Saudi Arabia.
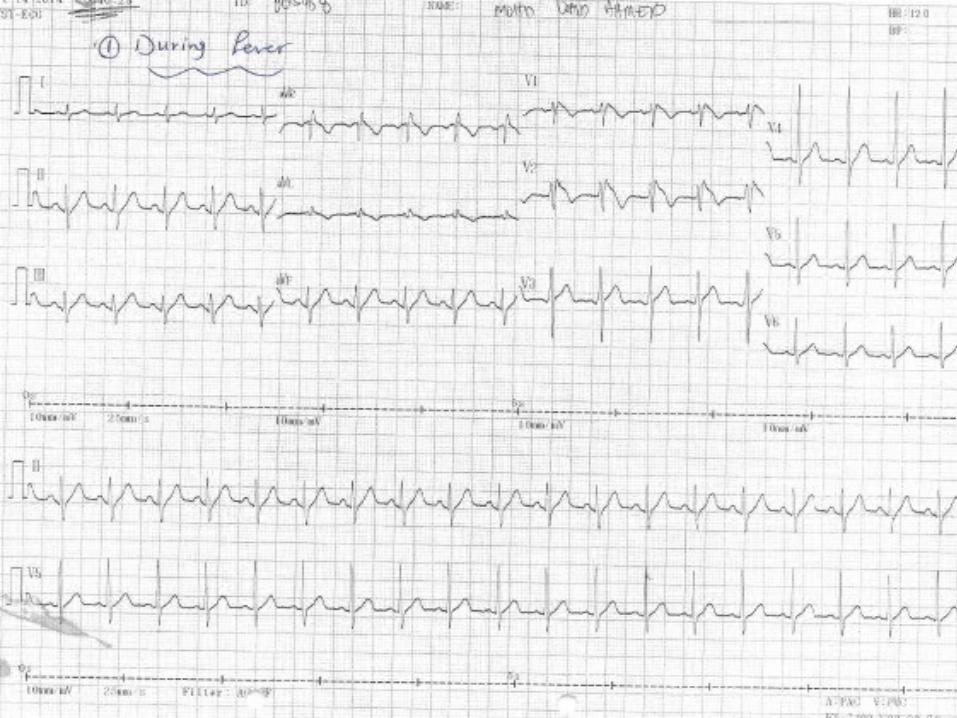
*He was admitted to our hospital with acute pneumonia.
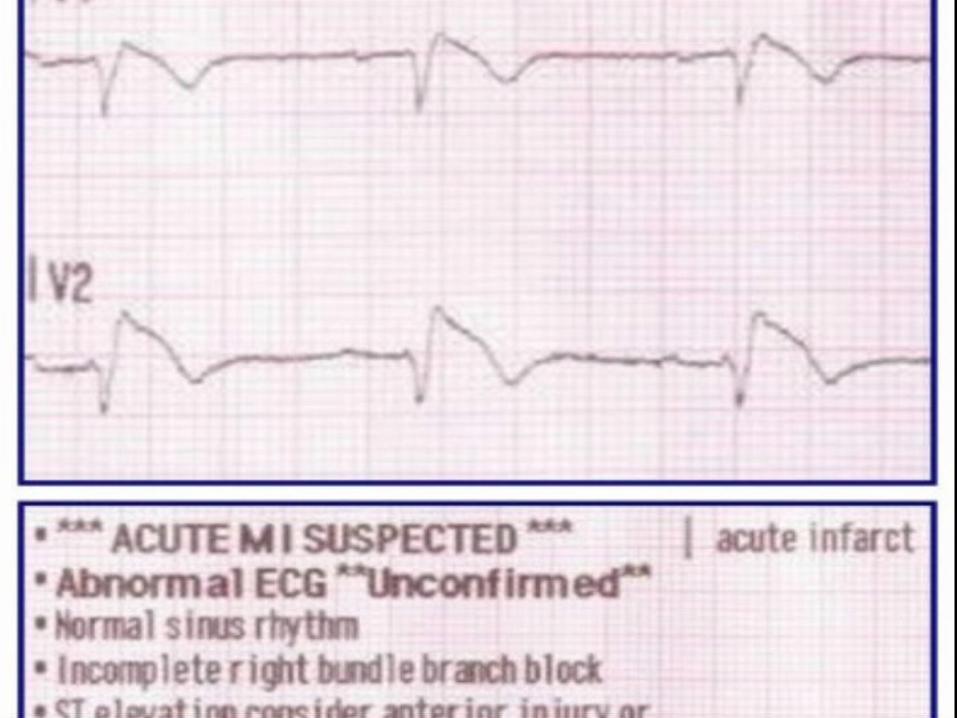
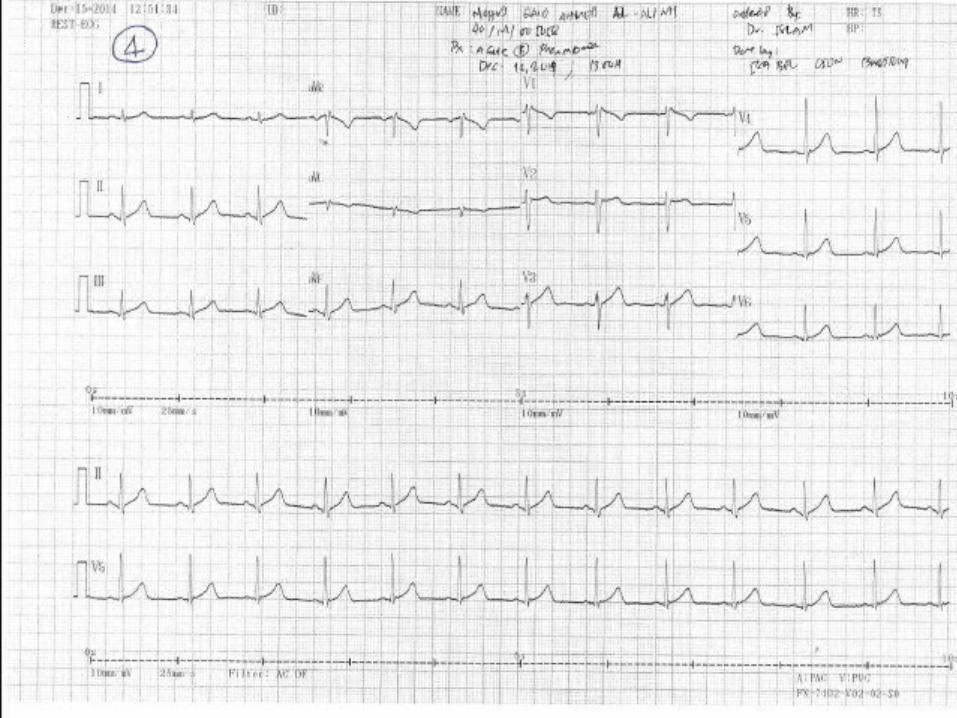
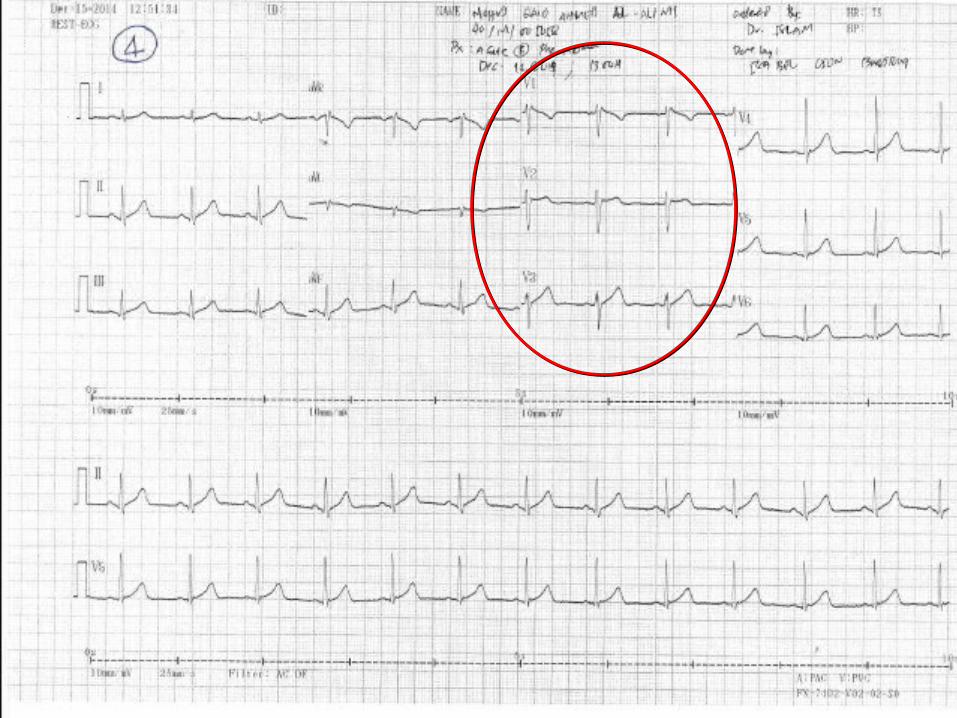
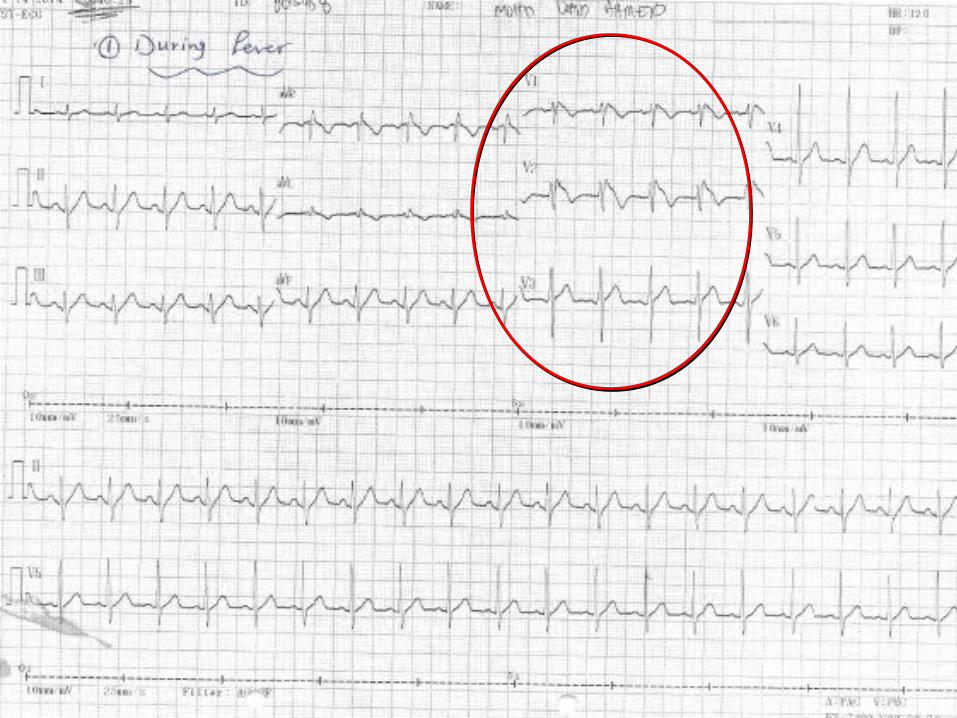
* Routine ECG was done and it was amazing (ST elevation!!!).

Brugada Syndrome
Brugada Syndrome
• Discovered by the Brugada brothers in 1992.
• Inherited defect of sodium channels (SCN5A gene).
• Epicardial area of the RV has repolarization abnormality.
• Prone to spontaneous Ventricular Arrhythmias.
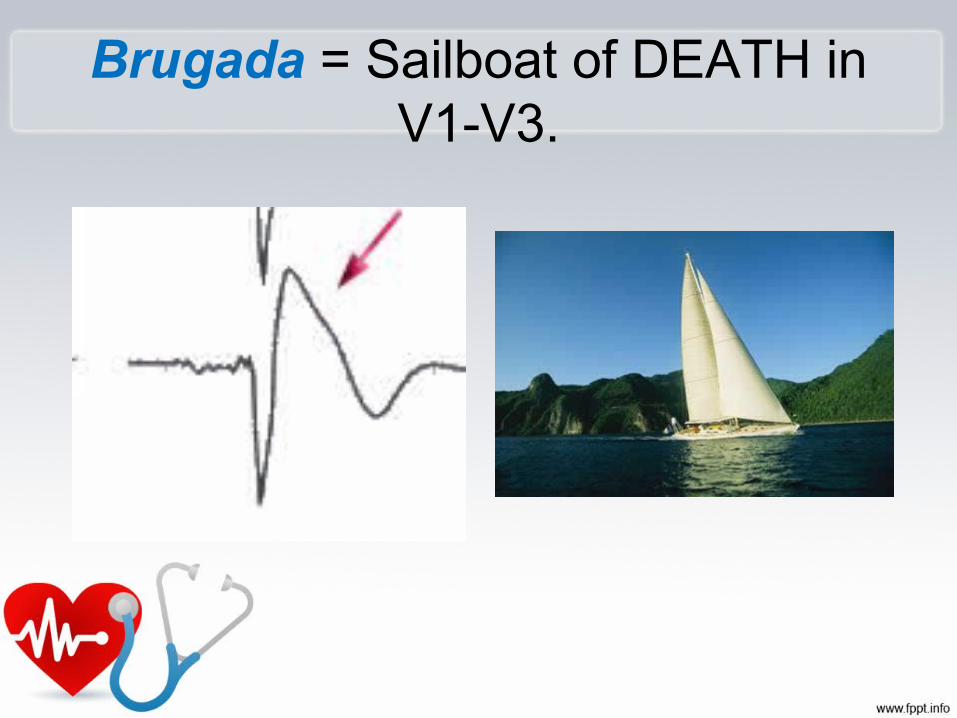
Brugada = Sailboat of DEATH in V1-V3.

Types
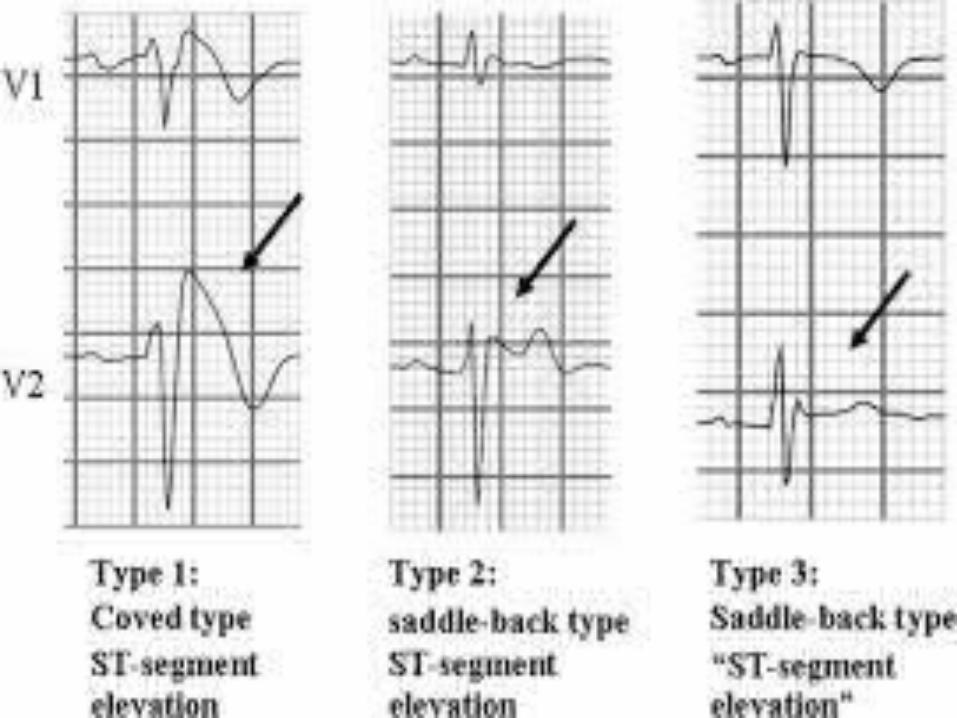
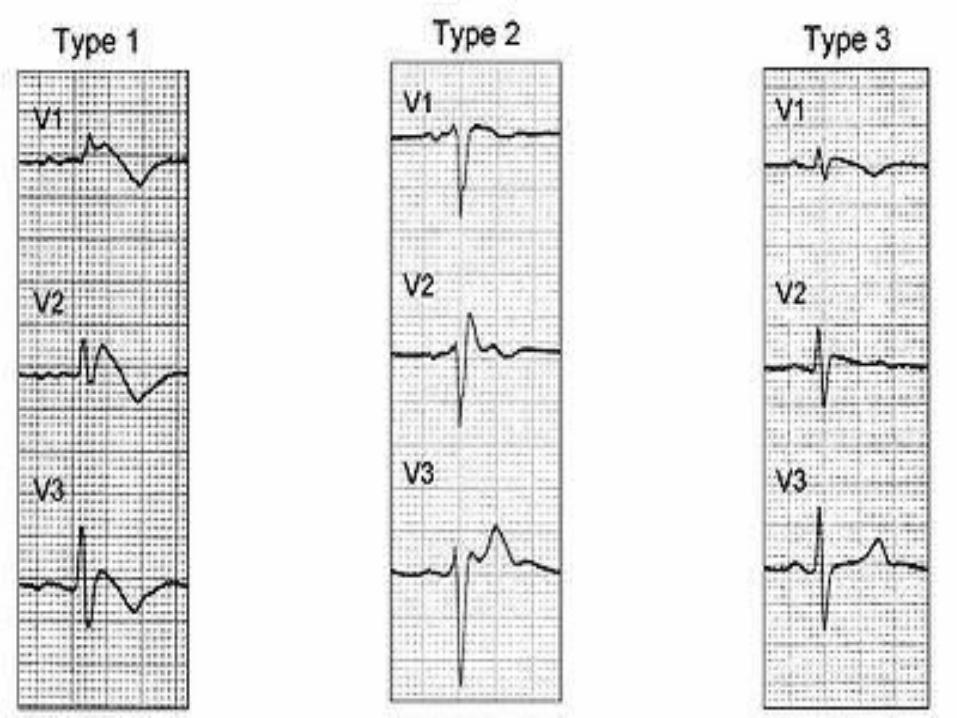
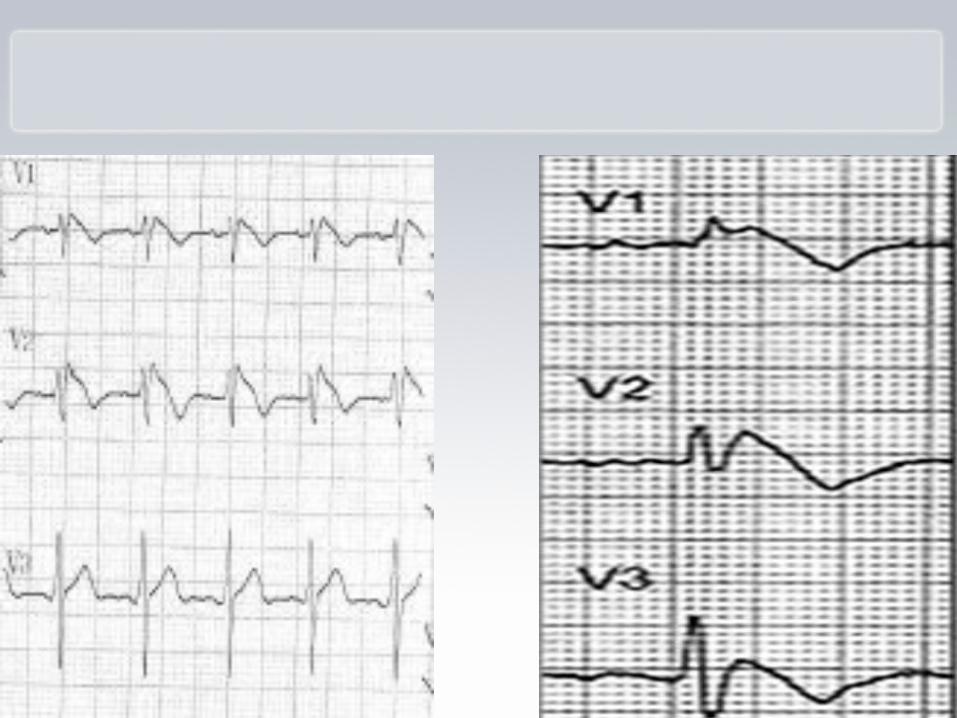
• Three ECG patterns of pseudo RBBB (incomplete or complete) with ST elevation in V1, V2, V3.
• Type I is diagnostic, but type II, III are suspicious and can be converted into type I with NA channel blocker (Ajmalin challenge test) or Fever or vagotonic stimulation.
Pathogenesis
• Genetics (Autosomal dominant)
• Loss of function mutations in SCN5A(3p21-24) coding for Alpha subunit of cardiac sodium channel
• The defective myocardial sodium channels reduce sodium inflow currents, thereby reducing the duration of normal action potentials.
• In addition, a prominent transient outward current, called I(to), in the right ventricular epicardium further shortens the action potential.
• This decrease in INa is thought to affect the right ventricular endocardium differently from the epicardium causing a voltage gradient during repolarization and the characteristic ST elevations on ECG.
Signs and symptoms*Syncope and cardiac arrest (due to ventricular arrhythmias: VT, VF): Most common clinical manifestations; in many cases, cardiac arrest occurs during sleep or rest, nightmares at night.*Asymptomatic, but routine ECG shows ST-segment elevation in leads V1-V3.

*Associated atrial fibrillation (20%).
*Fever: Often reported to trigger or exacerbate clinical manifestations, ECG appearance.
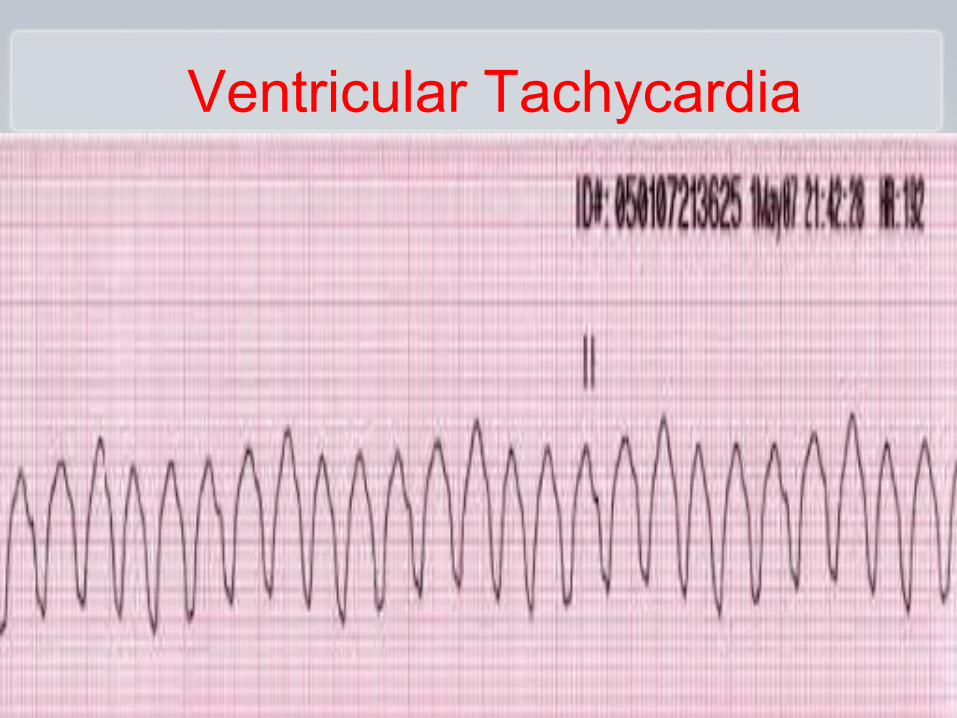
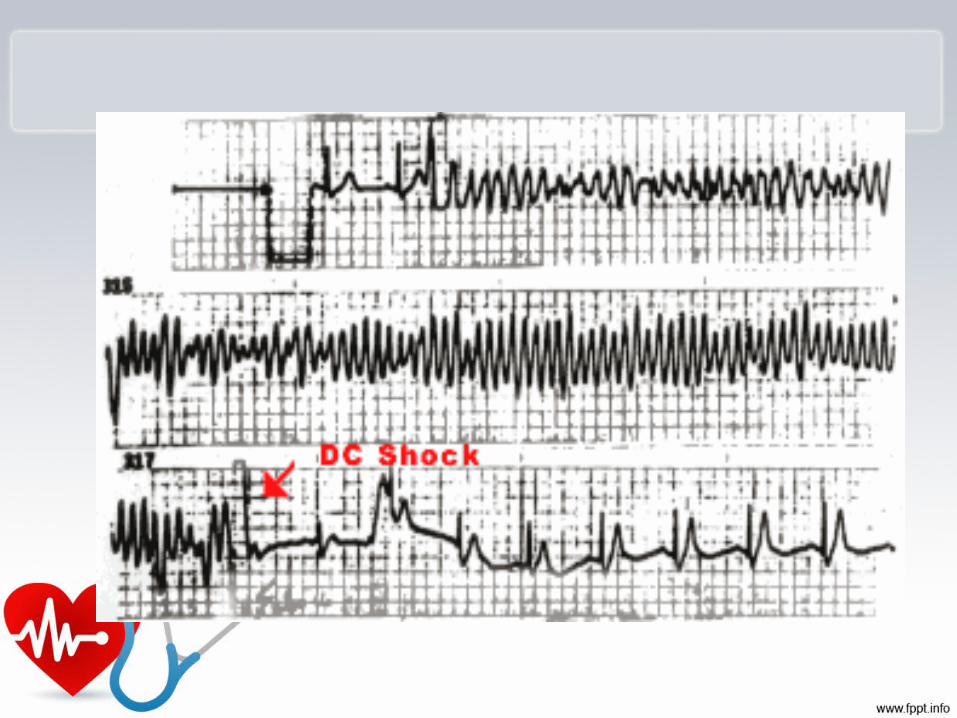
Ventricular Tachycardia
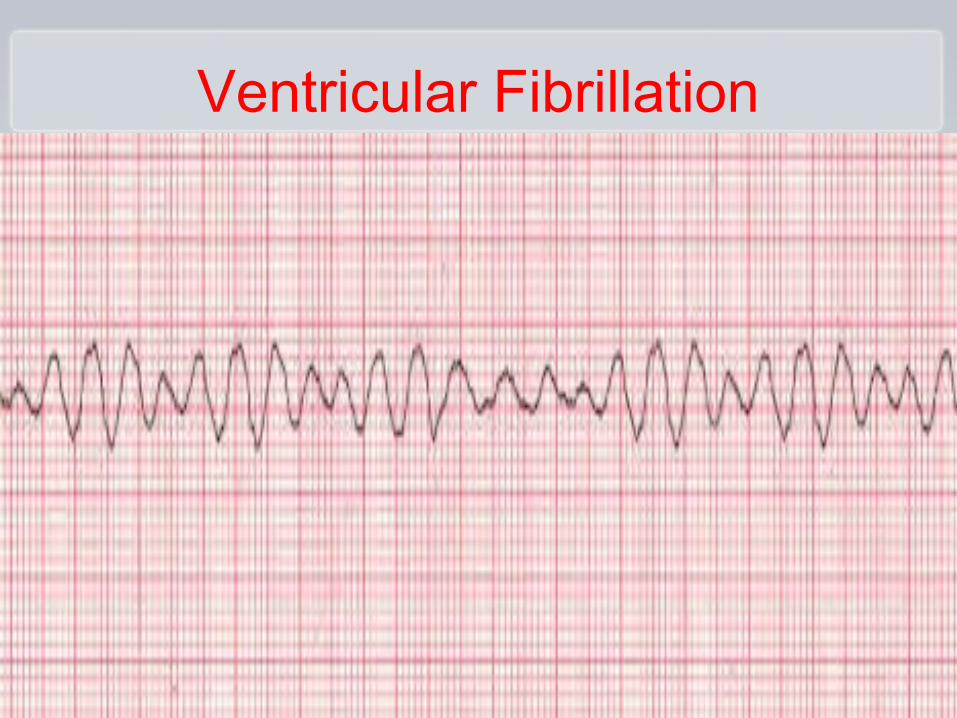
Ventricular Fibrillation
Diagnosis
*Most patients with Brugada syndrome have a normal physical examination. *12-lead ECG in all patients with syncope*Drug challenge with a sodium channel. blocker in patients with syncope without an obvious cause.
*Echocardiography.
*CK-MB and troponin levelsGenetic testing for a mutation in SCN5A.
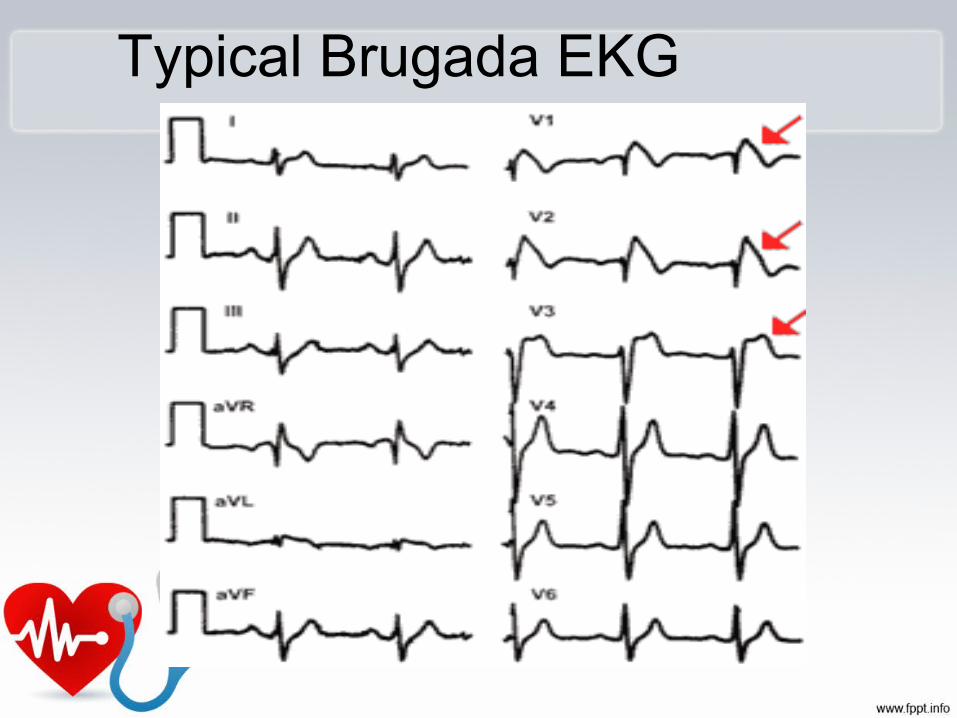
Typical Brugada EKG

Brugada Syndrome leads to ventricular arrhythmias.
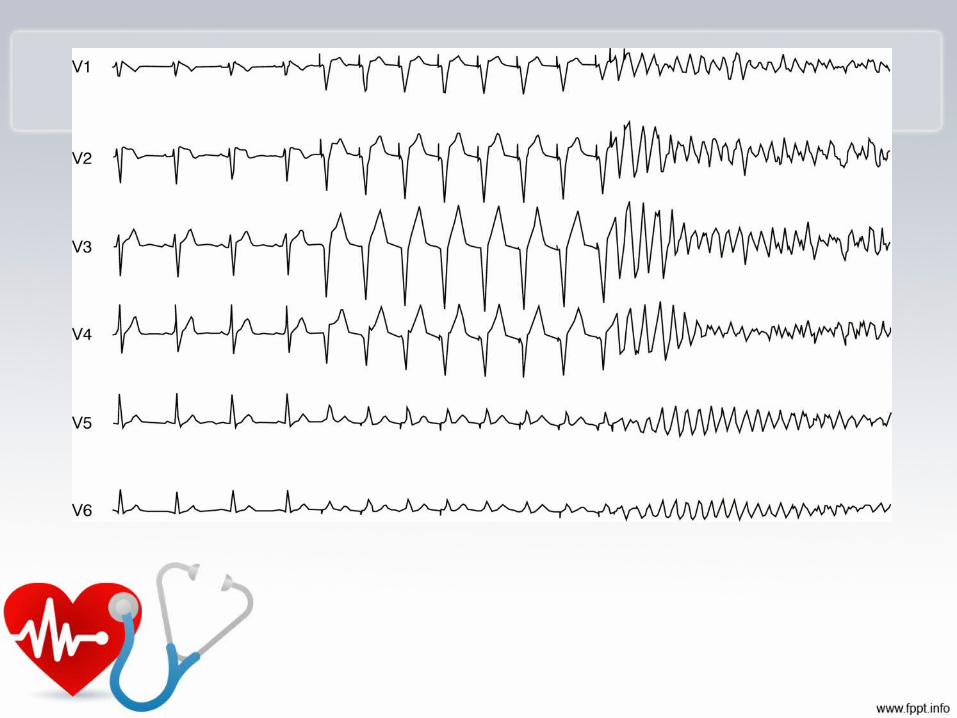
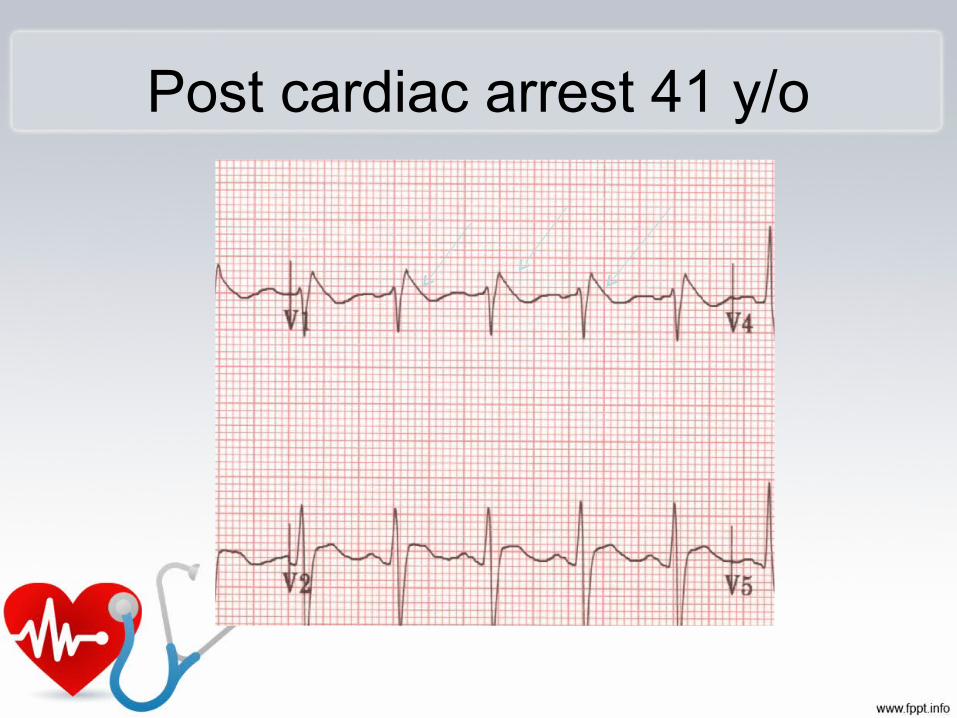
Post cardiac arrest 41 y/o

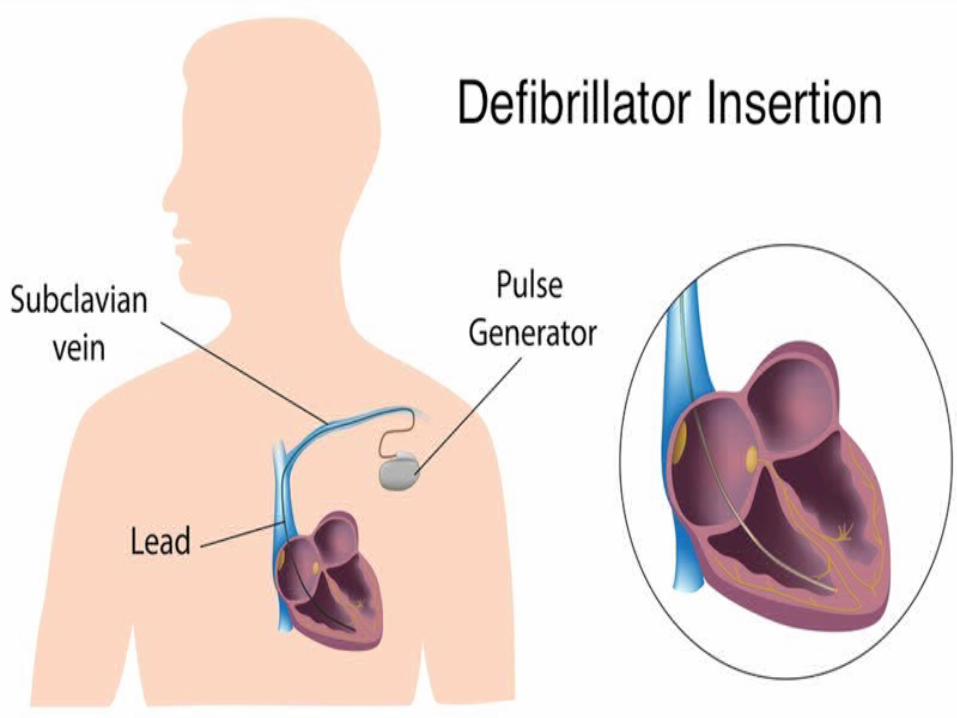
Management• Preventing sudden death(VT, VF) in
patients with Brugada syndrome through implantation of an automatic implantable
cardiac defibrillator (ICD).
* No pharmalogical treatment is
effective.

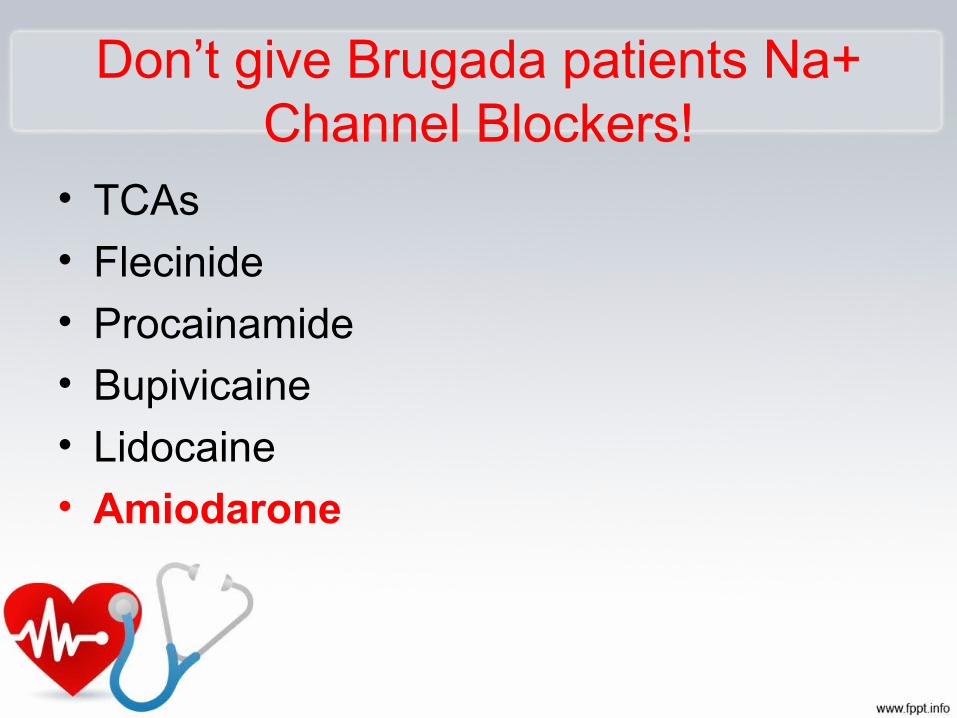
Don’t give Brugada patients Na+ Channel Blockers!
• TCAs
• Flecinide
• Procainamide
• Bupivicaine
• Lidocaine
• Amiodarone
Prognosis
• When a patient begins showing signs of Brugada Syndrome (syncope), mortality increases by 10% for every year Brugada is untreated.

Back to our patient
• *FEVER gave hand to us to diagnose him as it elicited the ECG appearance of BRUGADA (Converting it from type III into type I).


The patient was sent to a higher centre for ICD implantation
Sudden Cardiac Death in YoungCoronary artery anomalies, LAD bridge, CADPrimary electrical diseases:
WPW Long QT syndrome Catecholaminergic polymorphic VT Brugada syndrome Short QT syndrome Idiopathic VFNeurologic problems


T h a n k y o u







