Download - Cadth 2015 b4 remote robot cadth

Using Remote Presence Robots to
Improve Access to Care for People
with Low Back Pain
Stacey Lovo Grona, MSc, Brenna Bath, PhD, Luis Bustamante, MSc, Ivar Mendez, PhD,
Background
• Robots successfully used for medical assessments in a northern Inuit community in Newfoundland (Mendez et al., 2013)
• Now being used clinically in remote Northern Saskatchewan by the Department of Surgery, U of S.
• Innovative and emerging health care trend.
• Not yet used for PT service delivery anywhere in the world despite affordability and flexibility.
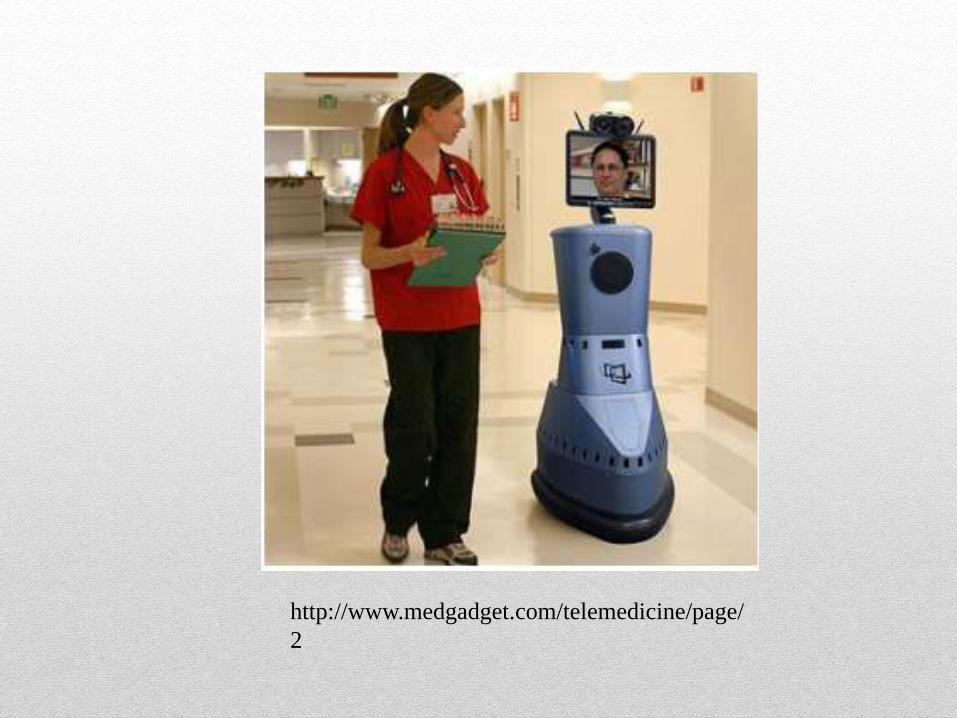
http://www.medgadget.com/telemedicine/page/
2

Background
• Chronic low back disorders (CLBD) are the leading
cause of morbidity worldwide, compared to 289 other
disease and conditions, considering years lived with
disability! (Vos et al., 2012)
• People with CLBD use more than double the health
system dollars than a comparable population without
back disorders (Mapel et al., 2004).

• 20% of Canadians have chronic back disorders (CBD) for
more than 6 months at a time.
• PT’s are rarely included in primary care teams, yet they
have very much to offer in terms of managing chronic low
back disorders.

PT and Management of
Back Pain
• Experienced PT’s have higher levels of knowledge in
managing back pain than physician interns, residents,
and all physicians except orthopedic surgeons (Childs et
al., 2005).
• Bath et al. (2012) found no significant difference
between PT’s and an orthopedic surgeon regarding
diagnostic categorization of people with chronic low
back disorders.

• People living in rural or remote regions are 30% more
likely to have CBD (Bath et al. 2014), however, access to
physical therapy (PT) services is limited.
• Lack of appropriate health care is thought to be a reason
for the higher rates of chronic health conditions in rural
areas (Allen, 1996 and Grimmer, 1998).
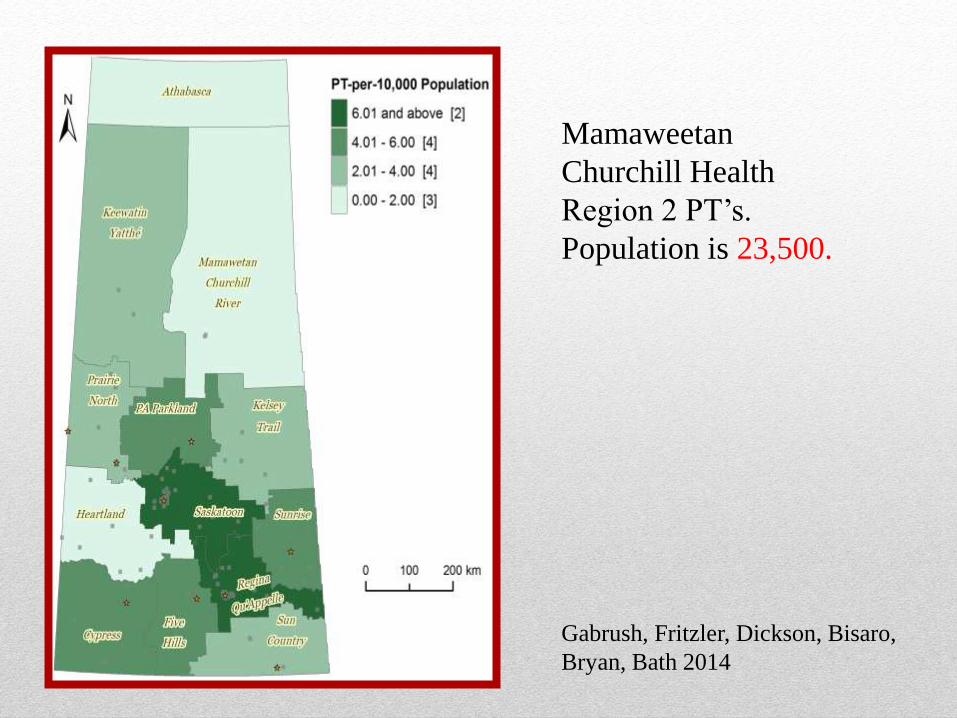
Gabrush, Fritzler, Dickson, Bisaro,
Bryan, Bath 2014
Mamaweetan
Churchill Health
Region 2 PT’s.
Population is 23,500.
Residents of remote Northern areas frequently seek care
for back disorders in urban centers.
• Time away from work, home and family
• Lengthy periods of travel, difficult road conditions
• Barrier to early assessment and appropriate follow-up

A New Model of Care is
Needed
RP-7 Remote Presence Robot
• In Touch Health, Santa Barbara, CA
• Class II medical device, US FDA
• Mobility – the PT can move around the patient with the robot to evaluate important aspects such as posture, movement quality and control.
• Realistic head / screen movements
• Excellent camera, audio and visual functionalities

RP-7 Remote Presence
Robot
• Functionalities:
• Regular and zoom camera control
• Microphone and speaker volume
• Mirrored screen (operator can demonstrate TO patient what
he/she is looking at by drawing or highlighting on the
screen)
• Approximate size of a person
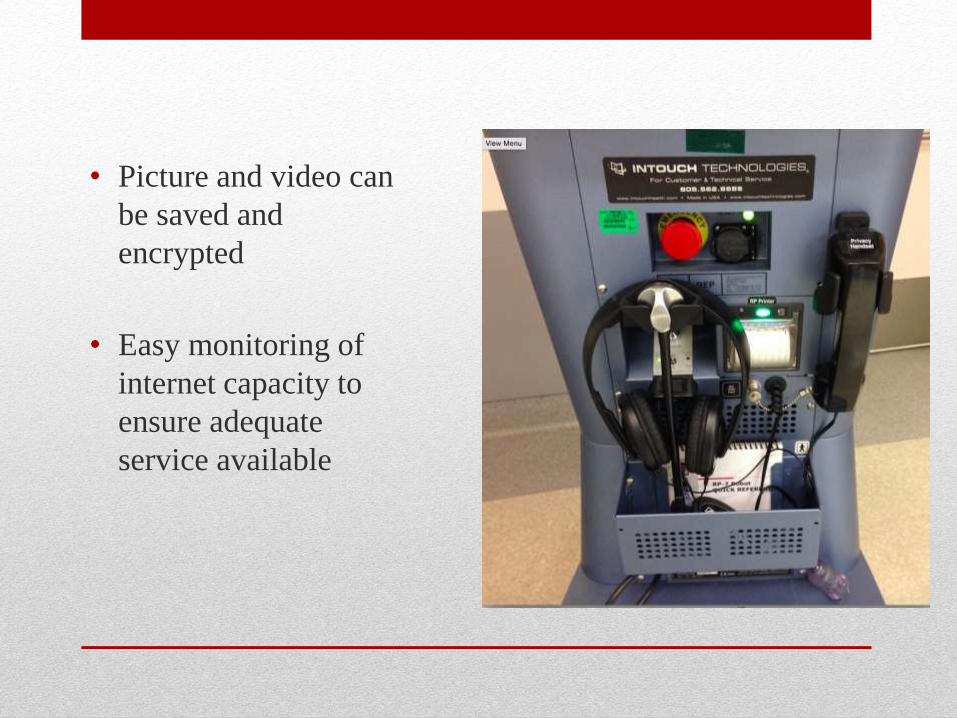
• Picture and video can
be saved and
encrypted
• Easy monitoring of
internet capacity to
ensure adequate
service available

• Set-up Considerations:
• Pre-clinical testing (light, audio to ensure most pleasing
appearance and sound)
• Earphones for privacy
• Privacy handset
• Printer
Research Question
• What is the feasibility of using remote
presence robots for a distance physical
therapy assessment of chronic low back
pain?

Research Details
• Approved by the University of Saskatchewan Biomedical Ethics Board 15-16. Case study design.
• Preparation and consultation with Indigenous community to ensure respectful research protocol.
• Data: Sociodemographic information, clinical information, depression and fear avoidance questionnaires, patient satisfaction and patient/practitioner experience interviews

Model of Care
• Interprofessional Team and Videoconferencing Pilot
• NP involvement with patient, urban PT joining from a distance
• Interprofessional role clarification and revision of traditional
spinal triage assessment

• Participant Selection:
• 18-80 years
• >3 months bothersome back or leg pain
• Not presently receiving PT, nor covered by WCB/SGI
• Recruitment: via NP appointed in charge of study by
Indigenous community
• NP training

• Interprofessional Assessment:
• Subjective History
• Medical history, medications, imaging results, weight and history of chronic illness
• Special questions: thecal pressure, neurological symptoms, bowel/bladder and sensation, use of steroids, history of RA, coagulation issues.
• Objective Exam
• Active Mobility
• Neurological Tests: key muscles, reflexes, upper motor neuron testing and sensory testing
• Neural Mobility Tests
• Special Tests:

Education Provided
• Use of mirrored screen to display educational
information:
• Back biomechanics and occupational hygiene
• Anatomy and pathology of back injuries
• Exercise examples
• Postural education
• Stages of tissue healing and expectations for recovery
• Next steps
• Findings:
• Subjective: post-surgical discectomy and laminotomy
• Objective: active range of motion limitations, poor control of posture and core musculature, neural mobility restrictions
• Follow-up
• 1 week later via robot
• Review and progression of exercise, explanation of next steps.
• Referral to closest in person PT for hands on treatment.

Results
• Awaiting following up semi structured interview and
questionnaires.
• SLR improved to normal in 1 week
• In one month goal of 10,000 steps per day achieved.
• Client was very pleased with education and ability to
begin exercises, as well as information on back safety and
expectations









