UK clinical perspective on treatment reviews of multiple
sclerosis therapiesAlasdair Coles
Neurologist, Cambridge, UK
Disclaimer
• Investigator on many Genzyme studies of alemtuzumab treatment of multiple sclerosis.
• Received honoraria and travel assistance for speaking on alemtuzumab from Genzyme.
• Received grant support from Genzyme.
• My institution (University of Cambridge) has received gifts from Genzyme.
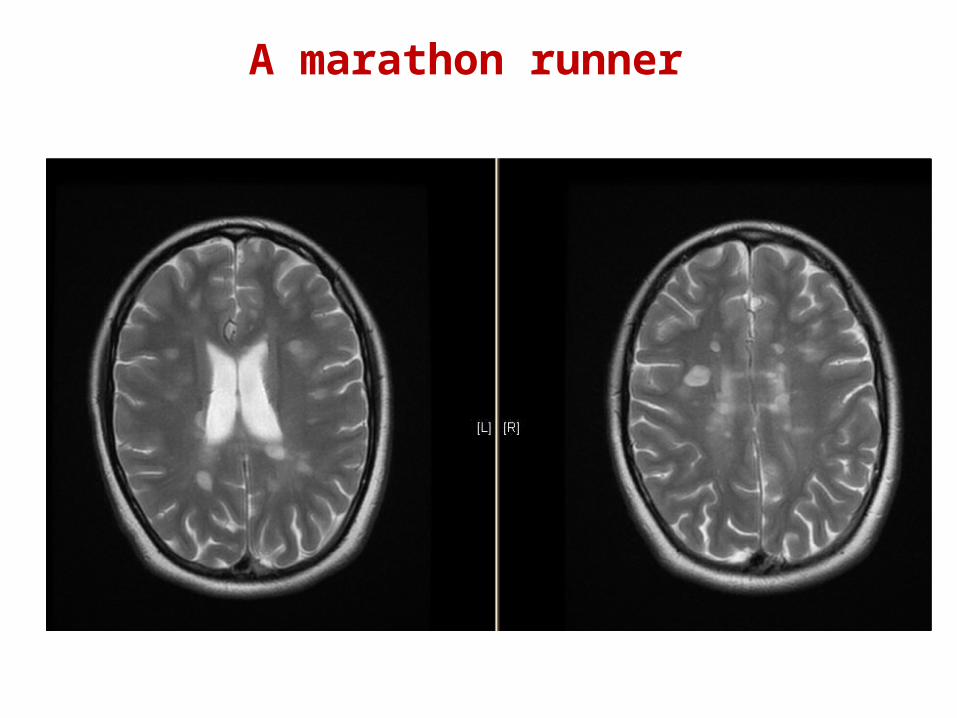
19 year old female law student and marathon runner
History18 months: ataxia, diplopia and headache 10 months: numb right big toe, tripping 4 months: burning sensation on right
shoulder1 month: diplopia, vertigo, numb right leg
for 2 weeks
EDSS 1.0
A marathon runner
A marathon runner
19 year old law student
Treatment
Started on interferon beta-1a SC.
2 months later: ascending numbness, weak legs then arms, then difficulty breathing, admitted to intensive care with quadraparesis. Steroids and plasma exchange. Good improvement over 6 weeks.
EDSS 2.5
A marathon runner

A marathon runner
RES: “rapidly evolving severe multiple sclerosis”• ≥ 2 disabling relapses in the previous year
AND• ≥ 1 gadolinium-enhancing lesions on brain
MRI Licensed indication for natalizumab in many regions
HAD: “high disease activity despite interferon-beta” • ≥ 1 relapse in the previous year on interferon-
beta• ≥ 1 gadolinium-enhancing MRI lesions or at
least nine T2-hyperintensive lesions on cranial MRI
Approved indication for fingolimod in many regions
What category of multiple sclerosis does she have according to NICE?
What evidence can guide switching from interferon to another drug ?
No RCT has compared switching to fingolimod versus natalizumab.
Sources of other evidence may be:• “real-life” databases• Indirect treatment comparison
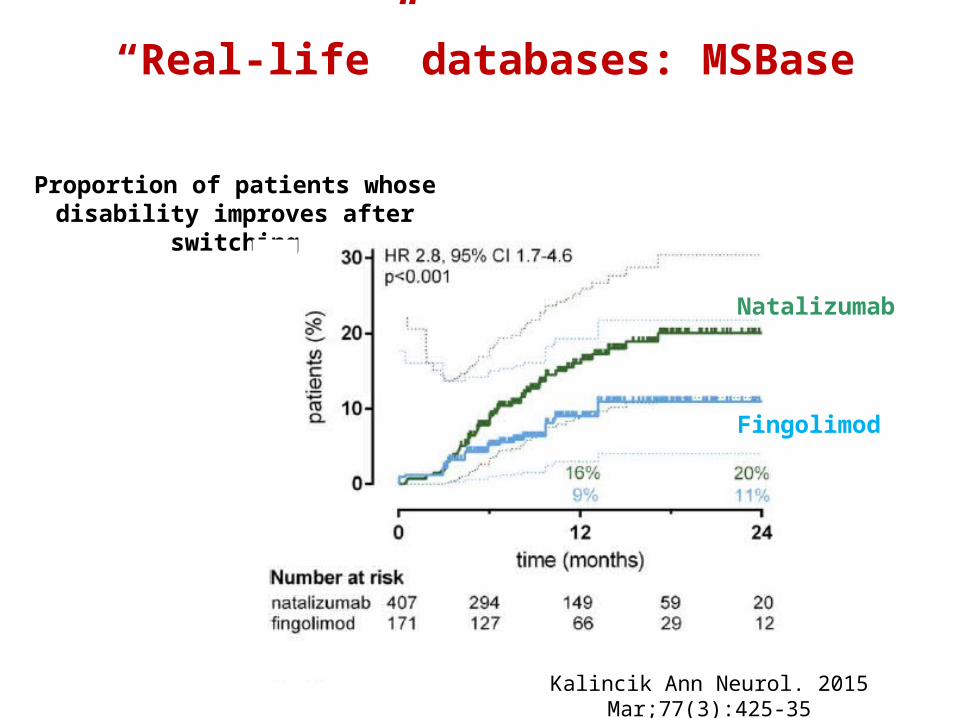
“Real-life” databases: MSBase
Proportion of patients whose disability improves after
switching
Kalincik Ann Neurol. 2015 Mar;77(3):425-35
Natalizumab
Fingolimod
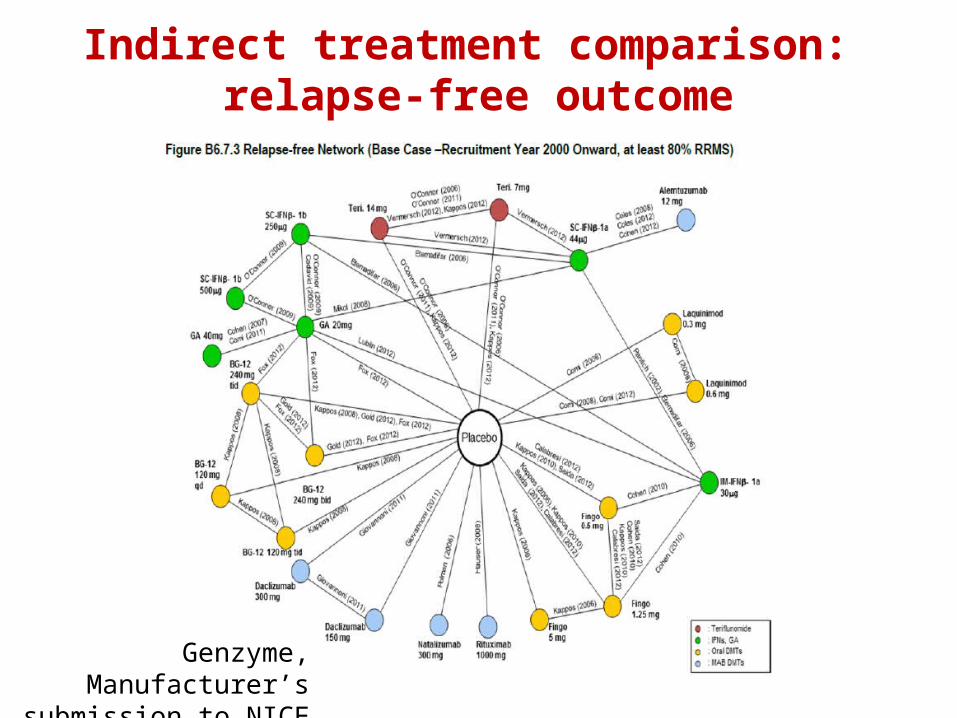
Indirect treatment comparison: relapse-free outcome
Genzyme, Manufacturer’s
submission to NICE 2014
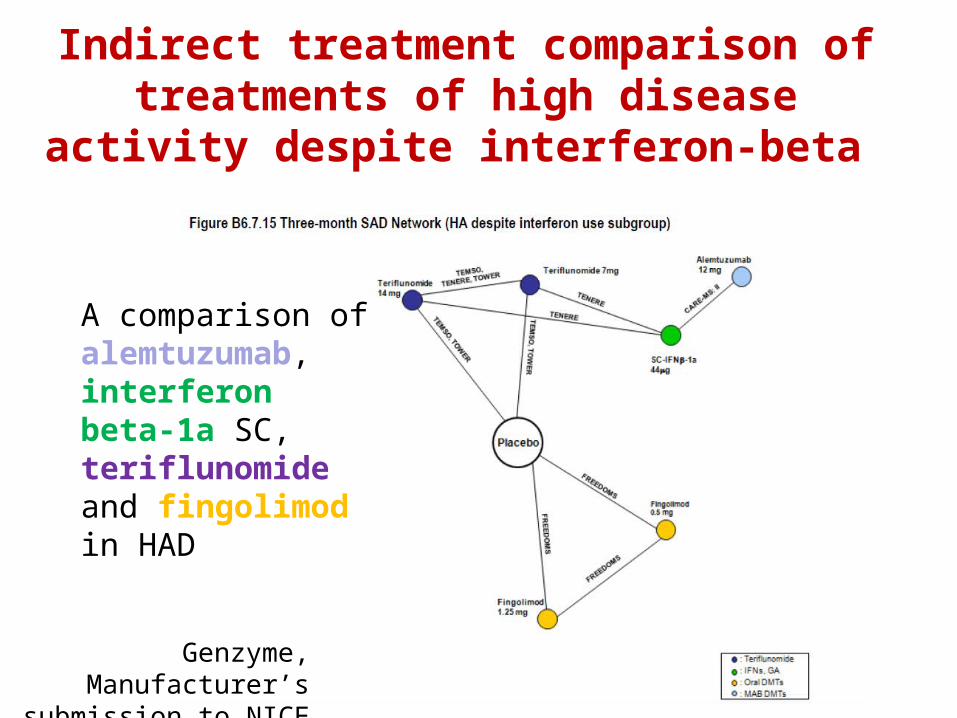
A comparison of alemtuzumab, interferon beta-1a SC, teriflunomide and fingolimod in HAD
Genzyme, Manufacturer’s
submission to NICE 2014
Indirect treatment comparison of treatments of high disease activity
despite interferon-beta
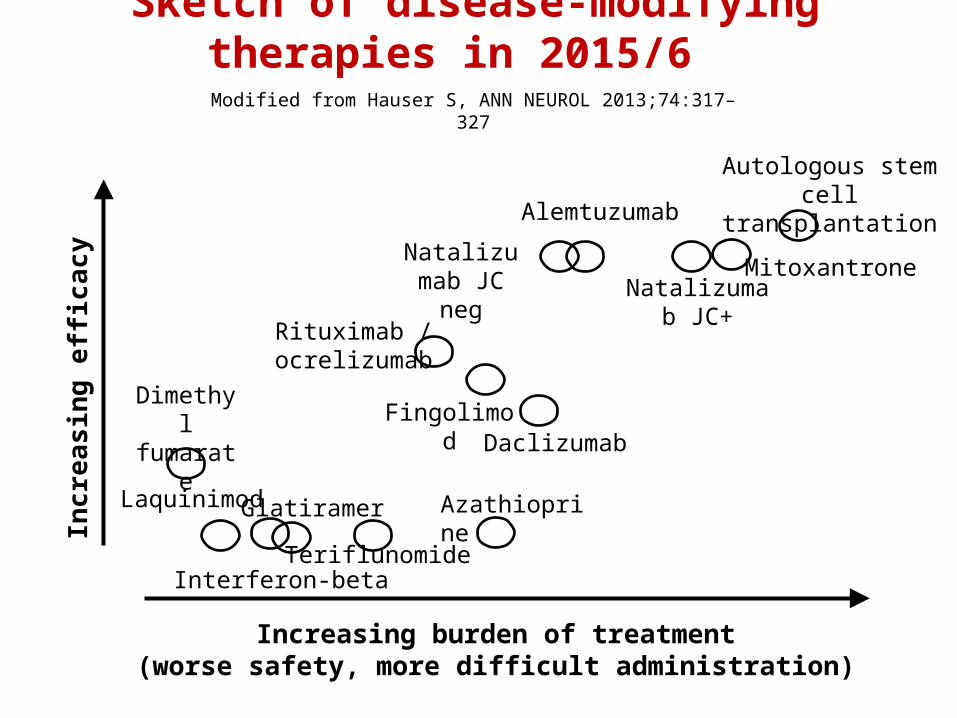
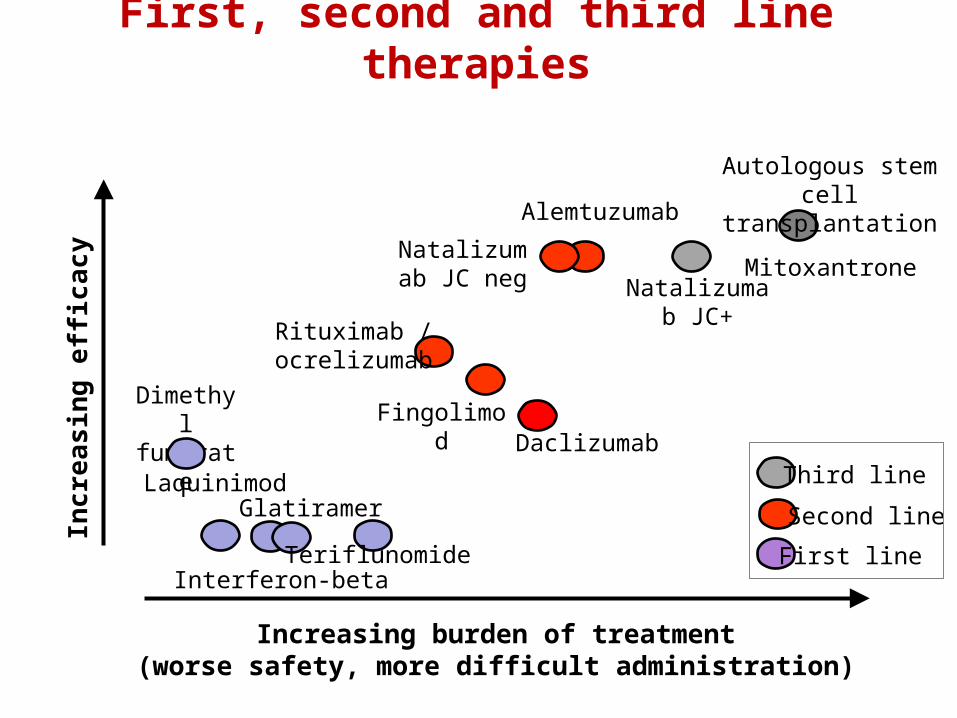
Incre
asin
g e
fficacy
Increasing burden of treatment(worse safety, more difficult administration)
Interferon-beta
Natalizumab JC+
Mitoxantrone
Fingolimod
Dimethyl fumarate
Autologous stem cell transplantation
Glatiramer
Sketch of disease-modifying therapies in 2015/6
Daclizumab
Modified from Hauser S, ANN NEUROL 2013;74:317–327
Laquinimod
Alemtuzumab
Natalizumab JC neg
Rituximab / ocrelizumab
Teriflunomide
Azathioprine
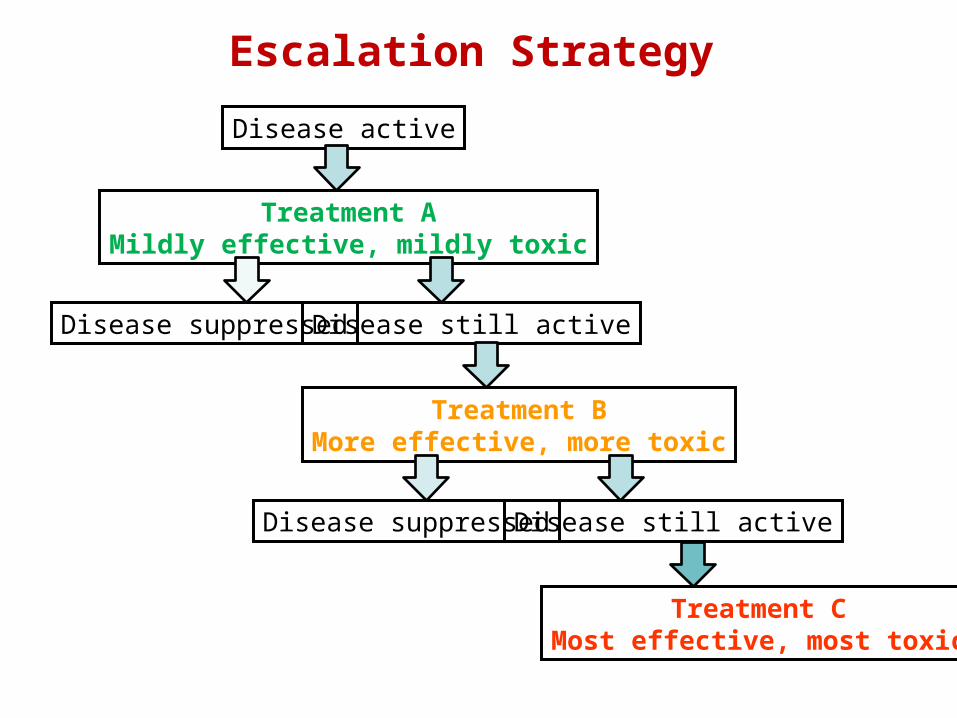
Treatment AMildly effective, mildly toxic
Disease active
Escalation Strategy
Disease suppressed Disease still active
Treatment BMore effective, more toxic
Disease suppressed Disease still active
Treatment CMost effective, most toxic
Incre
asin
g e
fficacy
Increasing burden of treatment(worse safety, more difficult administration)
Interferon-beta
Natalizumab JC+
Mitoxantrone
Fingolimod
Dimethyl fumarate
Autologous stem cell transplantation
Glatiramer
First, second and third line therapies
Laquinimod
Alemtuzumab
Natalizumab JC neg
Rituximab / ocrelizumab
Teriflunomide
Third line
Second line
First line
Daclizumab
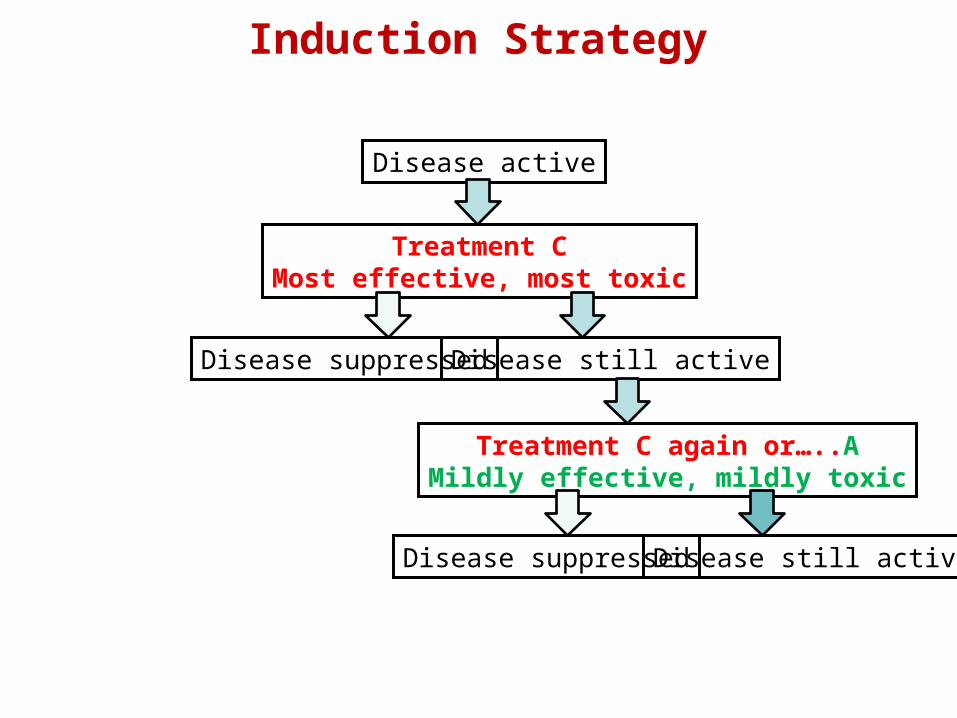
Treatment CMost effective, most toxic
Disease active
Induction Strategy
Disease suppressed Disease still active
Treatment C again or…..AMildly effective, mildly toxic
Disease suppressed Disease still active
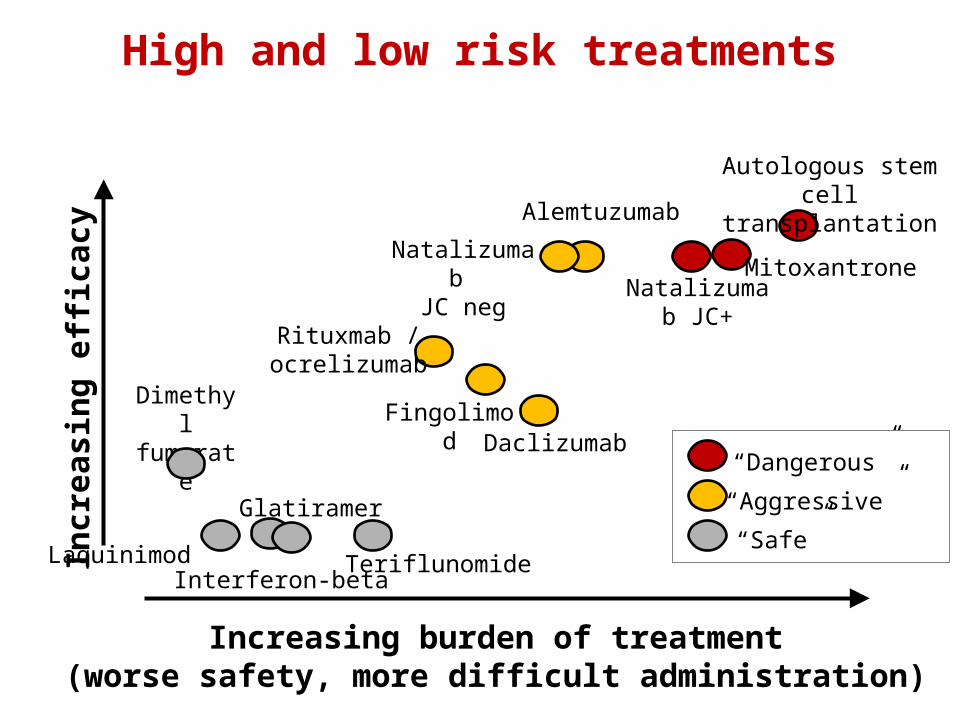
Incre
asin
g e
fficacy
Increasing burden of treatment(worse safety, more difficult administration)
Interferon-beta
Natalizumab JC+
Mitoxantrone
Fingolimod
Dimethyl fumarate
Autologous stem cell transplantation
Glatiramer
High and low risk treatments
Daclizumab
Laquinimod
Alemtuzumab
Natalizumab JC neg
Rituxmab / ocrelizumab
Teriflunomide
“Dangerous”
“Aggressive”
“Safe”
19 year old female law student and marathon runner
Attitude to illness: Very concerned to maintain intellectual level and run good marathon times.
Attitude to risk: “I am a high risk, high gain person”
Elected to receive alemtuzumab (in the UK)Received two cycles in 2003 and 2004.Since then has had one relapse and this triggered a further cycle of alemtuzumab. Continues to run marathons.
Back to our case
“Alemtuzumab is recommended as a possible treatment for people with active relapsing–remitting multiple sclerosis.”• European Medicines Agency, 2013
“We are very pleased to be able to recommend alemtuzumab for adults with relapsing-remitting multiple sclerosis. Evidence has shown that alemtuzumab is more effective and less expensive than current similar treatments for those with severe relapsing-remitting MS• National Institute for Health and Care Excellence
Chief Executive, Sir Andrew Dillon , 2014
UK approved use of alemtuzumab
Conclusion
• Rigid derivation of treatment guidelines from randomised controlled trials leads to unforeseen consequences.
• Indirect treatment comparisons and “real-lef” database studies answer questions not resolvable by RCTs
• Safety- conscious investigators and pharma tend to promote an escalation approach, which misses the opportunities of induction treatment.
• Detailed guidelines fail reduce the opportunity for physicians to adapt advice for individual patient factors, such as approach to risk.







