
Ellie Campbell DO Campbell integrative Family Medicine
Revolution Practice, LLC
CMT Conference Oct 2018

1) History and Definition of Integrative and Functional Medicine
2) Root Cause Resolution and the role of antecedents, triggers and
mediators
3) Tools for the exam room: the functional medicine matrix and timeline
4) Putting it all together! Concierge medicine and Functional Medicine :
an opportunity for improved patient outcome and revenue
5) The Scholarship Program in concierge care
6) Resources to learn, implement and share functional medicine
2 © Ellie Campbell 2018

© Ellie Campbell 2018 3
1995-2014 USA 17.141%

© Ellie Campbell 2018 4

© Ellie Campbell 2018 5

© Ellie Campbell 2018 6
By comparison, AUSTRALIA spent 9.422% of GDP and ranks
#3 for men and # 7 for women in life expectancy and CANADA
10.45 % #8 for men and #10 for women
USA
life expectancy #31

Is it ETHICAL to continue to practice in
a broken system that spends too much
money and gets such poor outcomes
compared to the rest of the world???
Or is it time for a
PARADIGM REVOLUTION?
© Ellie Campbell 2018 7

© Ellie Campbell 2018 8

© Ellie Campbell 2018 9

A system of diagnosis
followed by an
algorithmic approach
to a treatment
© Ellie Campbell 2018
10

© Ellie Campbell 2018 11

The IF the primary driver of chronic disease is the complicated interaction between
genes, activities of daily living (lifestyle), and the environment, DRIVEN BY INFLAMMATION THEN our allopathic paradigm addresses these very poorly.
© Ellie Campbell 2018
12

© Ellie Campbell 2018 13
Integrative medicine -A holistic medical discipline which takes into account
• the lifestyle habits of a patient.
• treat the whole person rather than just the disease.
• mind, body, and soul of a patient are taken into consideration to promote healing and well-being.
Integrative medicine is a combination of modern healthcare
practices for Dx/Tx, often including acupuncture, yoga, massage, nutrition, exercise, structural therapies
. Foundational belief that poor lifestyle choices are the root cause of many modern chronic diseases, and that drugs and surgery are not the solution.
© Ellie Campbell 2018 14

Functional medicine is a systems biology–based approach to health care that focuses on identifying and addressing the root cause of disease.
It embraces much of the philosophy of Integrative medicine as described above
BUT ALSO
Views the body as one integrated system, not a collection of independent organs divided up by medical specialties. It treats the whole patient, not just the symptoms.
© Ellie Campbell 2018 15

Marries current progress in
basic medical sciences
with clinical medicine to address
the growing problems associated with
chronic disease.
© Ellie Campbell 2018 16

Roger Williams PhD (B5 and Folic Acid)
Linus Pauling PhD (how atoms become molecules)
Weston Price DDS (anthropologist)
Jeffrey Bland PhD • Institute For Functional Medicine in 1991
Mark Hyman MD
Josh Axe DC (online…your patients read
him!)
© Ellie Campbell 2018 17

Mission of IFM • educate
and • provide clinical support for the implementation of
functional medicine across disciplines within the
healthcare sector.
© Ellie Campbell 2018 18

© Ellie Campbell 2018 19

Whaddya Have? that you need to get rid of
Whaddya need? that you are missing,
in order to get better
Whaddya GOT?? Whaddya NEED??
© Ellie Campbell 2018 20

A framework and paradigm to address the underlying causes of chronic disease using a systems approach to root cause resolution.
We don’t ask WHAT your diagnosis is, we ask WHY you have symptoms
We look for antecedents, triggers and mediators
© Ellie Campbell 2018 21
environment, lifestyle, diet, activity patterns, psycho-social-spiritual factors, and stress.
These lifestyle choices and environmental exposures can push us toward (or away from) disease by turning on—or off—certain genes
© Ellie Campbell 2018 22

© Ellie Campbell 2018 23
Transgenerational fear

© Ellie Campbell 2018 24
In 90 DAYS of TLC !! 48
GENES up-regulated and 453
down-regulated after the
intervention. Ornish 2008

IF EPIGENETICS ARE CONTROLLED BY
ENVIRONMENTAL TOXICANTS ALLERGY AND SENSITIVTY INFECTION DIET AND LIFESTYLE
SHOULDN’T MEDICAL DOCTORS AND
PRACTITIONERS BE ADDRESSING THEM???
© Ellie Campbell 2018 25

1. An understanding of the biochemical individuality of each human being, based on the concepts of genetic and environmental uniqueness;
2. Incorporating a patient-centered rather than a disease-centered approach to treatment;
3. Seeking a dynamic balance among the internal and external body, mind, and spirit;
© Ellie Campbell 2018 26
4. Addressing the web-like interconnections of internal
physiological factors;
5. Identifying health as a positive vitality - not merely the absence of disease- and emphasizing those factors that encourage the enhancement of a vigorous physiology;
6. Promoting organ reserve as the means to enhance the health span, not just the life span, of each patient
7. Functional Medicine is a science based profession
© Ellie Campbell 2018 27

Assimilation: digestion, absorption, microbiota/GI, respiration Defense and repair: immune, inflammation, infection/microbiota Energy: energy regulation, mitochondrial function Biotransformation and elimination: toxicity, detoxification Transport: cardiovascular and lymphatic systems Communication: endocrine, neurotransmitters, immune messengers Structural integrity: subcellular membranes to musculoskeletal integrity
© Ellie Campbell 2018 28

Where does the SYMPTOM come from? ie what are the antecedents and triggers
What keeps is GOING? • ie what are the mediators
And what can be done to CHANGE a
dis-eased homeostatic BALANCE point
the patient is locked into? • ie what are the underlying points of leverage
where the intervention can be most effective?
© Ellie Campbell 2018 29

Simply addressing Chief Complaint
and History of Present Illness to arrive at a DIAGNOSIS
RATHER: a comprehensive story filtered through the lens of antecedents, triggers and mediators to understand key imbalances
© Ellie Campbell 2018 30

31 © Ellie Campbell 2018

The most important precept to remember
about Functional Medicine is that restoring
balance—in the patient’s environmental
inputs and in the body’s fundamental
physiological processes—
is the key to restoring health.
© Ellie Campbell 2018 32

Phytonutrients and supplements (incl EO and homeopathic remedies)
Meditation Diet Vitamin and Mineral therapy (oral and IV) Manipulative therapies Acupuncture and TCM/Ayurveda Surgery Drugs Exercise including yoga and Tai Chi Counseling Oxidative and regenerative therapies Detoxification strategies (including chelation)
© Ellie Campbell 2018 33
G= Gather Information
O= Organization Information
T= Tell the Complete Story Back to
the Patient
O= Order and Prioritize
I= Initiate Treatment
T= Track Outcomes
© Ellie Campbell 2018 34

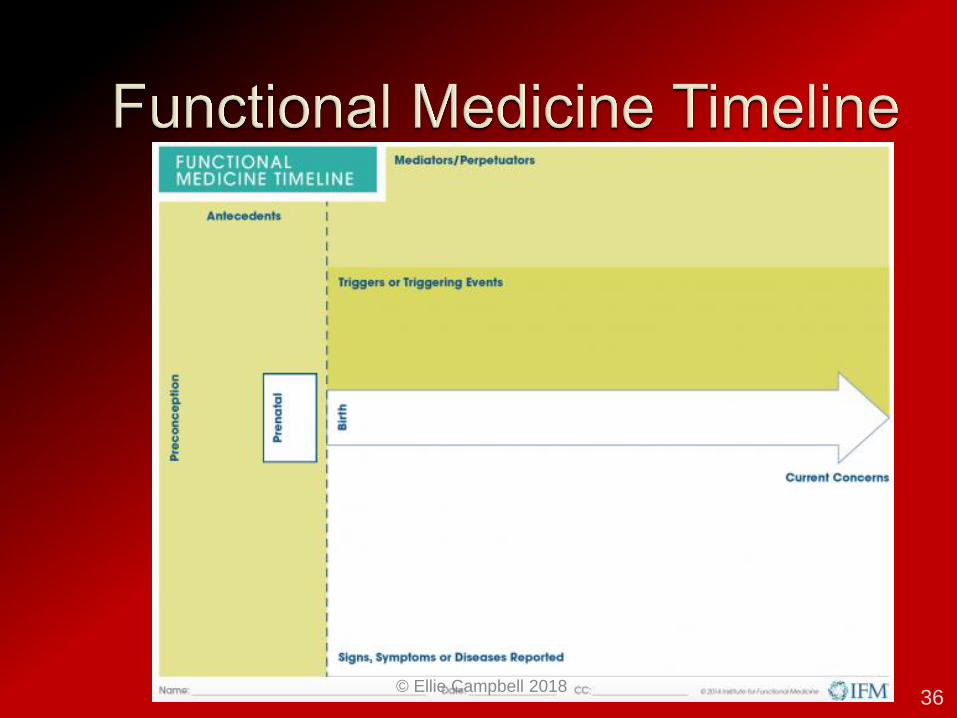
The Functional Medicine Timeline
The Functional Medicine Matrix
© Ellie Campbell 2018 35
© Ellie Campbell 2018 36

Factors the predispose to acute
or chronic illness
Discrete events or entities that
provoke disease or symptoms
Contribute to the
manifestation of disease
© Ellie Campbell 2018 37

© Ellie Campbell 2018 38

TRADITIONAL ALLOPATHIC MODEL:
Chief Complaint: 54 y/0 WM Substernal Chest pain, DOE HPI: 3 months duration, worse with exercise,
relieved by rest. Underlying obesity, HTN and hyperlipidemia
TREATMENT: stress test +/- echo and CXR, give handout on BMI risk and lower CHOLESTEROL with statin, aspirin, +/- ACE-I, NTG;
come back when you need PCI /CABG
© Ellie Campbell 2018 39

LIPIDS
INFLAMMATION
CORRUPTED
CHOLESTEROL
40 © Ellie Campbell 2018
Review the Matrix and Time line
Test genetics: ApoE, KIF6, Haptoglobin, Cyp450, MTHFR
Test underlying root causes:
Vit D deficiency, OSA, IGT, dyslipoproteinemia, grief,
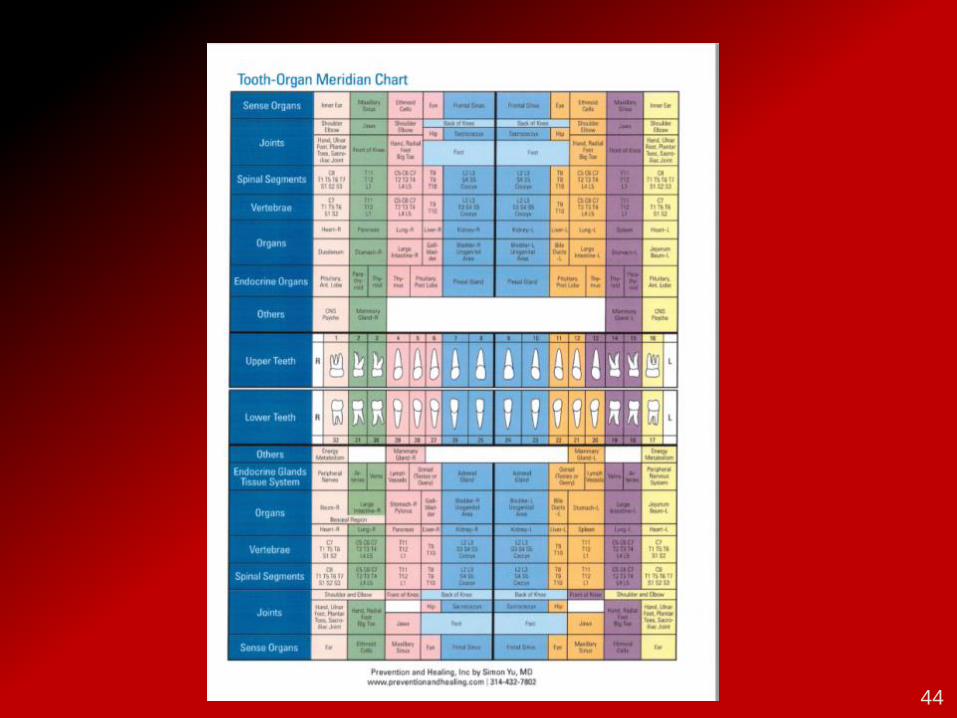
dental disease and meridians, inflammatory markers,
toxicants esp. heavy metals
TREATMENT: TLC!!! Therapeutic lifestyle changes,
begin GF diet, targeted supplementation, dental
consult, chelation therapy, emotional support,
coaching and counseling. Meds for now, wean off as
possible © Ellie Campbell 2018
41

© Ellie Campbell 2018 42
FuncMed Tree
Matrix
ATM
Genes
Organ Dysfxn
S & S

© Ellie Campbell 2018 43
© Ellie Campbell 2018 44

Post MI >50 y/o; Creat <2.0 Overall 26% reduction combined endpoint (death, MI,
CVA, revasc, angina hosp) p=0.0002 NNT 6.5
DIABETICS: blew them away
Overall 51% reduction combined endpoint (death, MI, CVA, coron revasc, angina hosp) p<0.001 5 yr NNT 5.5
43% Reduction in MORTALITY p=0.011 5 yr NNT 12
© Ellie Campbell 2018 45

TACT2 trial recruiting [email protected] $37 million award 2016
TACT (Trial to Assess Chelation) 2013 Dr Gervasio (Tony) Lamas Post MI >50 y/o; Creat <2.0
Overall 26% reduction combined endpoint
(death, MI, CVA, revasc, angina hosp) p=0.0002 NNT 6.5
© Ellie Campbell 2018 46

Framing Root Causes as ATM:
USING our PARADIGM OF
ANTECEDENTS TRIGGERS MEDIATORS
© Ellie Campbell 2018 47

IMPROVE CLINICAL OUTCOMES
(GET BETTER RESULTS, NO CVA/MIs)
INCREASE REVENUE TO THE PRACTICE • Opportunity for testing non-covered labs
• Opportunity for testing US with CIMT (non-covered)
• Opportunity for retailing supplements
• Opportunity for home sleep apnea testing
• Opportunity for pathogenic oral flora testing
• Consider creating “all inclusive packages”
© Ellie Campbell 2018 48

VIRTUALLY ALL OF MY PATIENTS GET GENE TESTED
• MTHFR
• APO E
SELECTED PATIENTS ALSO GET TESTED
• CYP 1A2
• CYP 2C19
• KIF6 (Kinesin family member 6)
• 9P21
• 4q25, Hp, IL-1,IL-6, IL-17A, ETC ETC ETC
49 © Ellie Campbell 2018

The root of all medical evil
50 © Ellie Campbell 2018

AMERICAN BODIES ARE ON
FIRE WITH INFLAMMATION
IN FACT INFLAMMATION IS
PROBABLY ALL 3: • ANTECEDENT
• TRIGGER
• MEDIATOR
51 © Ellie Campbell 2018
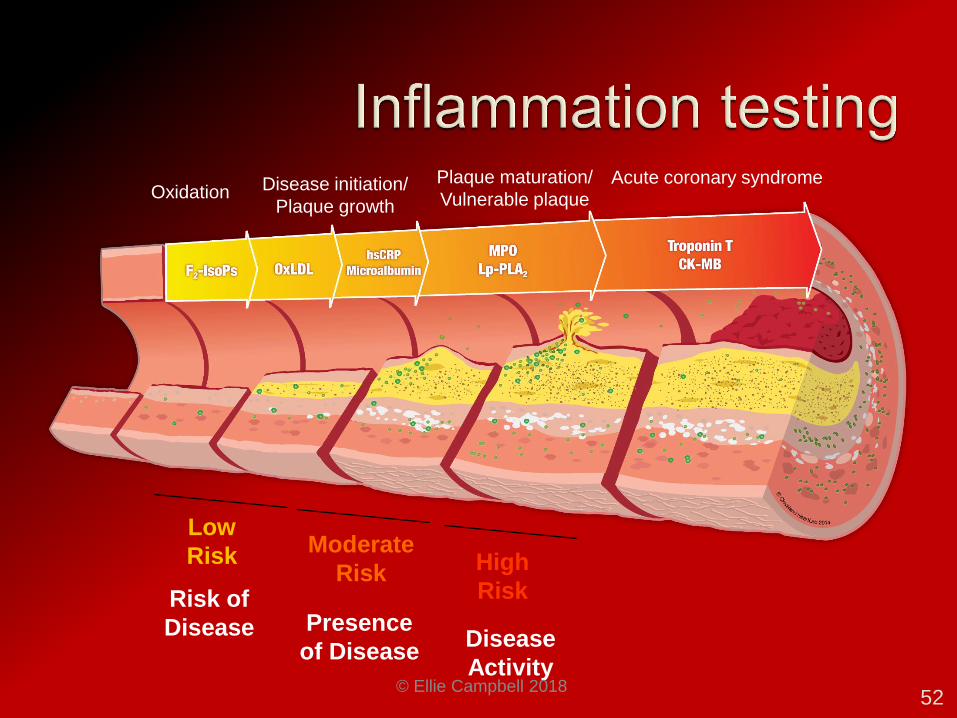
Risk of
Disease
Low
Risk Moderate
Risk
Presence
of Disease
High
Risk
Disease
Activity
Oxidation Disease initiation/
Plaque growth
Plaque maturation/
Vulnerable plaque
Acute coronary syndrome
52 © Ellie Campbell 2018

Learn how to determine whether active arterial plaquing exists • using vascular US
• and CIMT testing
The carotid arteries are a window to the
view systemic atherosclerosis
NB: CIMT is NOT done by mobile US screenings or even by most radiology departments!
Need special tech.
53
© Ellie Campbell 2018
Size matters –test for size/number • Whereas LDL itself is NOT correlated to CVD risk ,
lipoprotein particle size and particle number are
correlated
sdLDL is BAD
54 © Ellie Campbell 2018

Lipoprotein(a) is a really bad actor
Test for Lipo(a) !!!!
• DIRECTLY CAUSES MI
• Drives CV risk despite statin therapy
• Inhibits fibrinolysis
• Is decreased slightly by niacin
• (future role for PCSK9 inhibitors)
55 © Ellie Campbell 2018

ORAL HEALTH MATTERS MORE THAN EVER
Since 2014, GOOGLE SCHOLAR articles
“oral flora cardio”= 689; “dental cardiac” =15,800;
“oral microbiome CVD”= 2670; “periapical abscess coronary disease”= 1,200
56 © Ellie Campbell 2018

ORAL HEALTH MATTERS
MORE THAN EVER
Test for OSA
57 © Ellie Campbell 2018

58 © Ellie Campbell 2018
Do Not Smoke BMI <25 TC <200 mg/dL BP <120/80 FBG <100 mg/dL EXERCISE:
• 150 min. moderate
• or 75 min vigorous exercise PER WEEK
(=only 11 min per day!!) Diet 4 of 5 (DASH diet)
• 4.5 cups/d of fruit and veggies • ≥ 2- 3.5 oz fish/week • ≤ 3 -12 oz sugar sweetened beverages/week • ≥ 3 -1 oz servings of fiber rich whole grains/day • ≤ 1500 mg salt/day
59 © Ellie Campbell 2018

Time for a paradigm shift in our care model
Our crisis management approach is no
longer sustainable. It is time for primary care
to shift from lumenology to arteriology.
PCPs think cardiologists are
managing prevention and
cardiologist thinks PCPS are!! We must ALL put more resources in to
prevention BECAUSE IT WORKS!!!
60 © Ellie Campbell 2018

ROOT CAUSE RESOLUTION
WHADDYA GOT?
WHADDYA NEED?
ANTECEDENTS
TRIGGERS
MEDIATORS
TIMELINE and MATRIX
© Ellie Campbell 2018 61

TO CONTINUE TO PRACTICE IN A BROKEN PARADIGM
TO SUPPORT A MODEL THAT IS DRIVING DOCTORS TO BURNOUT, BANKRUPTY OR SUICIDE
TO SUPPORT THE PHARMA MACHINE THAT IS SUPPORTING THE EDUCATION OF FUTURE PHYSICIANS
THAT THE CURRENT SYSTEM DOES NOT GET PATIENTS BETTER OR PREVENT DISEASE?
© Ellie Campbell 2018 62
Wouldn’t you rather have tools and
a system to change and improve
your patients symptoms and
reduce their risk of chronic
inflammatory disease????
© Ellie Campbell 2018 63

64 © Ellie Campbell 2018

© Ellie Campbell 2018 65
DEFENSE AND REPAIR

IFM www.functionalmedicine.org ICIM www.icimed.com AAEM www.aaemonline.org AMMG https://www.agemed.org ACAM www.acam.com A4M www.A4M.com ABIHM--->ABIM http://www.aihm.org
© Ellie Campbell 2018 66

Introduction to Functional Medicine
AMA Accreditation Statement
The Institute for Functional Medicine
designates this enduring material for a
maximum of 1.5 AMA PRA Category 1
Credits™.
https://www.ifm.org/learning-
center/introduction-functional-medicine/
© Ellie Campbell 2018 67
http://www.functionalmedicineuniversity.co
m/public/department151.cfm
Founder:
Ronald Grisanti D.C.,D.A.B.C.O.,
D.A.C.B.N.,M.S., CFMP
© Ellie Campbell 2018 68

https://www.schoolafm.com/
Founder: Tracy Harrison
© Ellie Campbell 2018 69

https://www.functionalmedicine.org/afmcp/ho
me/
Applying Functional Medicine in clinical practice
1-2X a year CME
March 04-09 2019 Chicago
34.5 hours of CME $3,500
© Ellie Campbell 2018 70

Functional Forum ON LINE first Monday of every month –hold a meet up group
Lecture to your community: become the expert in your space
Share your message: put your business card in wellness books at the library or bookstore
“Accidentally” leave your website on the screen at the Apple store
Host a Walk with a Doc or Shop with a Doc event
© Ellie Campbell 2018 71
CAMPBELL FAMILY MEDICINE CUMMING GA
2005 CASH–ONLY PRACTICE
Charge by the hour…3 years failure
2008 CONVERTED TO SOLO, CASH ONLY
MEMBERSHIP BASED CONCIERGE MODEL 3FT/ 3PT STAFF
Chris Ewin MD 1:2:1 MD
© Ellie Campbell 2018 72

200 ACTIVE CASES @ $250/month
WORK IN OFFICE 3.5 DAYS/WEEK
(time for family, travel, lecturing, teaching, networking, volunteering)
GROSS REVENUE $750,000+
TITHE: 5% CASH 5% SERVICE
© Ellie Campbell 2018
73

FREE IS VALUELESS
BASED ON HABITAT FOR HUMANITY
SWEAT EQUITY
15 HOURS OF COMMUNITY SERVICE
=3 MONTHS OF MEMBERSHIP RIGHTS
$50/HOUR EQUIVALENT
CARE WITH DIGNITY
WIN/WIN/WIN
© Ellie Campbell 2018 74

THE ANTIDOTE TO PHYSICIAN
BURNOUT
THE SOLUTION FOR THE
BROKEN SYSTEM
A SUCCESSFUL NEW
PARADIGM © Ellie Campbell 2018
75

DPC/membership practice
PLUS
Functional Medicine
© Ellie Campbell 2018 76

AFTER 12 YEARS, many mistakes and many successes,
I BELIVE THAT FUNCTIONAL MEDICINE
PRACTICED IN A CONCIERGE MEDICAL MODEL
CAN SAVE DOCTORS AND OTHER PROVIDERS
SAVE THE PATIENT’S
LIVES AND LIVLIHOODS
SAVE MONEY
© Ellie Campbell 2018 77

8 HOUR NON-CME BUSINESS DEVELOPMENT COURSE
HOW TO ATTRACT PATIENTS • INCLUDING FREE MARKETING STRATEGIES
HOW TO DESIGN A CASH PRACTICE • CONCIERGE, MEMBERSHIP, PROGRAMS
COACHING ROLE-PLAY EXERCISES • TO CONVERT PROSPECTS TO PATIENTS
• TO ENGAGE PATIENT WELLNESS BEHAVIOR
© Ellie Campbell 2018 78


© Ellie Campbell 2018 80

© Ellie Campbell 2018 81

© Ellie Campbell 2018 82

THANK YOU MICHAEL TETREAULT
The Dream
The Vision
The Implementation
The Fellowship
OF CONCIERGE MEDICINE TODAY
© Ellie Campbell 2018 83







