
Clin Transl Sci. 2021;00:1–13. | 1www.cts-journal.com
Received:22July2021 | Revised:24August2021 | Accepted:10September2021
DOI:10.1111/cts.13168
A R T I C L E
Cardiovascular events and safety outcomes associated with remdesivir using a World Health Organization international pharmacovigilance database
Se Yong Jung1 | Min Seo Kim2,3 | Han Li4 | Keum Hwa Lee5 | Ai Koyanagi6,7,8 | Marco Solmi9,10,11 | Andreas Kronbichler12 | Elena Dragioti13 | Kalthoum Tizaoui14 | Sarah Cargnin15 | Salvatore Terrazzino15 | Sung Hwi Hong16 | Ramy Abou Ghayda17 | Nam Kyun Kim18,19 | Seo Kyoung Chung20 | Louis Jacob6,21 | Joe- Elie Salem22 | Dong Keon Yon23 | Seung Won Lee24 | Karel Kostev25 | Ah Young Kim1 | Jo Won Jung1 | Jae Young Choi1 | Jin Soo Shin26 | Soon- Jung Park27 | Seong Woo Choi28 | Kiwon Ban29 | Sung- Hwan Moon27 | Yun Young Go30 | Jae Il Shin5 | Lee Smith31
1DivisionofPediatricCardiology,DepartmentofPediatrics,YonseiUniversityCollegeofMedicine,Seoul,Korea2CollegeofMedicine,KoreaUniversity,Seoul,Korea3SamsungAdvancedInstituteforHealthSciencesandTechnology(SAIHST),SamsungMedicalCenter,SungkyunkwanUniversity,Seoul,Korea4UniversityofFloridaCollegeofMedicine,Gainesville,Florida,USA5DepartmentofPediatrics,YonseiUniversityCollegeofMedicine,Seoul,Korea6ResearchandDevelopmentUnit,ParcSanitariSantJoandeDéu,UniversitatdeBarcelona,FundacióSantJoandeDéu,CIBERSAM,Barcelona,Spain7ICREA,Barcelona,Spain8InstitutodeSaludCarlosIII,CentrodeInvestigaciónBiomédicaenReddeSaludMental,CIBERSAM,Madrid,Spain9DepartmentofPsychiatry,UniversityofOttawa,Ottawa,Ontario,Canada10DepartmentofMentalHealth,TheOttawaHospital,Ottawa,Ontario,Canada11OttawaHospitalResearchInstitute(OHRI)ClinicalEpidemiologyProgram,UniversityofOttawa,Ottawa,Ontario,Canada12DepartmentofInternalMedicineIV,MedicalUniversityInnsbruck,Innsbruck,Austria13DepartmentofHealth,MedicineandCaringSciences,PainandRehabilitationCentre,LinköpingUniversity,Linköping,Sweden14LaboratoryMicroorganismesandActiveBiomolecules,SciencesFacultyofTunis,TunisElManarUniversity,Tunis,Tunisia15DepartmentofPharmaceuticalSciences,InterdepartmentalResearchCenterofPharmacogeneticsandPharmacogenomics(CRIFF),UniversityofPiemonteOrientale,Novara,Italy16YonseiUniversityCollegeofMedicine,Seoul,Korea17UrologyInstitute,UniversityHospitalsandCaseWesternReserveUniversity,Cleveland,Ohio,USA18DepartmentofPediatrics,EmoryUniversity,Atlanta,Georgia,USA19DivisionofCardiovascularSurgery,DepartmentofThoracicandCardiovascularSurgery,YonseiUniversityCollegeofMedicine,Seoul,Korea20CollegeofMedicine,EwhaWomansUniversity,Seoul,Korea21FacultyofMedicine,UniversityofVersaillesSaint-Quentin-en-Yvelines,Montigny-le-Bretonneux,France
ThisisanopenaccessarticleunderthetermsoftheCreativeCommonsAttribution-NonCommercialLicense,whichpermitsuse,distributionandreproductioninanymedium,providedtheoriginalworkisproperlycitedandisnotusedforcommercialpurposes.©2021TheAuthors.Clinical and Translational SciencepublishedbyWileyPeriodicalsLLConbehalfofAmericanSocietyforClinicalPharmacologyandTherapeutics.
SeYongJung,MinSeoKim,andHanLicontributedequallytothiswork.
NCT:NCT04314817

2 | JUNG et al.
22DepartmentofPharmacology,INSERM,CIC-1901Paris-Est,CLIPGalilée,UNICO-GRECOCardio-oncologyProgram,Pitié-SalpêtrièreHospital,AssistancePublique–HôpitauxdeParis,SorbonneUniversité,Paris,France23DepartmentofPediatrics,SeoulNationalUniversityChildren'sHospital,SeoulNationalUniversityCollegeofMedicine,Seoul,Korea24DepartmentofDataScience,SejongUniversityCollegeofSoftwareConvergence,Seoul,Korea25UniversityClinicofMarburg,Marburg,Germany26InfectiousDiseaseResearchCenter,KoreaResearchInstituteofChemicalTechnology,Daejeon,Korea27StemCellResearchInstitute,T&RBiofabCo.Ltd,Siheung,Korea28DepartmentofPhysiology,Ischemic/HypoxicDiseaseInstitute,SeoulNationalUniversityCollegeofMedicine,Seoul,Korea29DepartmentofBiomedicalSciences,CityUniversityofHongKong,HongKongSAR,China30DepartmentofInfectiousDiseasesandPublicHealth,CityUniversityofHongKong,HongKongSAR,China31TheCambridgeCentreforSportandExerciseSciences,AngliaRuskinUniversity,Cambridge,UK
CorrespondenceJaeIlShin,DepartmentofPediatrics,YonseiUniversityCollegeofMedicine,50-1Yonsei-ro,Seodaemun-gu,C.P.O.Box8044,Seoul03722,Korea.Email:[email protected]
Funding informationThisstudywassupportedbyanewfacultyresearchseedmoneygrantofYonseiUniversityCollegeofMedicinefor2021(2021-32-0049).Thefundershadnoroleinthedesign,analyses,orinterpretationofthestudy.
AbstractOnOctober2020,theUSFoodandDrugAdministration(FDA)approvedremde-sivirasthefirstdrugforthetreatmentofcoronavirusdisease2019(COVID-19),increasing remdesivir prescriptions worldwide. However, potential cardiovas-cular(CV)toxicitiesassociatedwithremdesivirremainunknown.Weaimedtocharacterize theCVadversedrugreactions (ADRs)associatedwithremdesivirusing VigiBase, an individual case safety report database of the World HealthOrganization (WHO).DisproportionalityanalysesofCV-ADRsassociatedwithremdesivirwereperformedusingreportedoddsratiosandinformationcompo-nents. We conducted in vitro experiments using cardiomyocytes derived fromhumanpluripotentstemcellcardiomyocytes(hPSC-CMs)toconfirmcardiotoxic-ityofremdesivir.Todistinguishdrug-inducedCV-ADRsfromCOVID-19effects,werestrictedanalyses topatientswithCOVID-19and foundthat,afteradjust-ingformultipleconfounders,cardiacarrest(adjustedoddsratio[aOR]:1.88,95%confidenceinterval[CI]:1.08–3.29),bradycardia(aOR:2.09,95%CI:1.24–3.53),andhypotension(aOR:1.67,95%CI:1.03–2.73)wereassociatedwithremdesivir.InvitrodatademonstratedthatremdesivirreducedthecellviabilityofhPSC-CMsintime-anddose-dependentmanners.PhysiciansshouldbeawareofpotentialCVconsequencesfollowingremdesiviruseandimplementadequateCVmoni-toringtomaintainatolerablesafetymargin.
Study HighlightsWHAT IS THE CURRENT KNOWLEDGE ON THE TOPIC?Remdesiviruseisincreasing,butitscardiovascular(CV)adversedrugreactions(ADRs)remainlargelyunknown.Thetoxicityprofilederivesfromclinicaltrialswithconflictingresultsandofinsufficientsizetoidentifyrare,severeadverseCVreactions.WHAT QUESTION DID THIS STUDY ADDRESS?ThisstudyidentifiesCVADRsassociatedwithremdesivirbydisproportionalityanalysisusingVigiBase,aglobalindividualcasesafetyreportdatabase.WHAT DOES THIS STUDY ADD TO OUR KNOWLEDGE?ThisstudyidentifiesthreepreviouslyunreportedputativeadverseCVreactions,namely,hypotension,cardiacarrest,andbradycardia,independentlyassociated

| 3CARDIOVASCULAR EVENTS OF REMDESIVIR
INTRODUCTION
InDecember2019,thenovelsevereacuterespiratorysyn-dromecoronavirus2(SARS-CoV-2)wasidentifiedasthecausativeagentofoutbreakofpneumoniaandotherasso-ciatedsymptomslikecytokinestorm,1eventuallytermedcoronavirus disease 2019 (COVID-19).2 Remdesivir (GS-5734),aninhibitoroftheRNA-dependentRNApolymer-asesofSARS-CoV-1andMiddleEastrespiratorysyndrome(MERS)-CoV,3hasshownprotectiveeffectagainstSARS-CoV-2byeffectivelyinhibitingitsproliferationinvitro.4,5Subsequentrandomizedplacebo-controlledtrials(RCTs)and open-label trials have shown that remdesivir treat-mentloweredthemedianrecoverytimeofpatientswithCOVID-19,6–8 with some trials demonstrating decreasedmortality.6 Based on this supporting evidence, the USFood and Drug Administration (FDA) approved rem-desiviras the firstdrug treatmentagainstCOVID-19onOctober22,2020.9
Although the efficacy of remdesivir has been exten-sivelyinvestigated,theassociatedadverseevents(AEs)arenotwell-characterized.Becauseremdesivirhasnotbeenextensively used in clinical practice—other than againstEbola virus (EBOV) disease and COVID-19—sufficientsafety evidence has not been accumulated. At present,clinical trials on COVID-19 are the sole source of infor-mationoncardiovascular(CV)toxicitiesassociatedwithremdesivir, and recent RCTs have reported conflictingresults;someRCTshavereportedthatremdesivircausesmore seriousCVAEs than the standardcare,10whereasanother suggested that the CV AEs induced by remde-siviriscomparabletothatinducedbyplacebo.8AlthoughRCTs provide reliable information on drug efficacy, ob-servational studies with large sample size often outper-formRCTsincapturingrarebutfatalAEs,suchascardiacarrest or myocardial infarction.11 The increasing use ofremdesivir during the COVID-19 pandemic has createdanurgentneedtoelucidateitssafetyprofile,particularlyforCVAEsthatareofteninfrequentbutlethaltopatientswithCOVID-19.
Therefore, we conducted a large observational phar-macovigilancestudyusingtheWorldHealthOrganization(WHO) global database of individual case safety reports
(ICSRs),12 todetectCVsignalswithhighresolutionandcharacterize theCVAEsofremdesivir.TheVigiBase in-corporates thedataof20 million individuals frommorethan130countriesandasthelargestpharmacovigilancedatabase, it provides discriminating findings on drugsafety,asindicatedinourpreviousstudies.13–16
METHODS
Study design and data source
This large retrospective pharmacovigilance cohort studywasconductedusingdatafromVigiBase,theWHOglobaldeduplicated ICSR database,12 which contains recordsfromgreaterthan130countriesand20 millionindividuals,untilSeptember1,2020.Relevantadversedrugreaction(ADR)reportsfromacrosstheglobehavebeencollectedto thedatabasesince1967asper theWHOProgramforInternational Drug Monitoring (MDR), and is managedby the Uppsala Monitoring Center (UMC, Sweden).The data casemix was separated into case and non-casegroupsbasedonthetargetdrugof interest (remdesivir),whichwerethenusedforthedisproportionalityanalysis.VigiBaseacceptsreportsfromvariouscrediblesources,in-cludinghealthcareworkers,patients,andpharmaceuticalcompanies, and the sources are generally provided withpostmarketing notifications. We extracted remdesivir-associated ADR cases from the inception of the data-basetoAugust30,2020.TheethicscommitteeofYonseiUniversity Severance Hospital, Seoul, Korea, approvedthisstudyandgrantedawaiverofreviewfromtheformalinstitutionalreviewboard(no.4-2020-0868)andinformedconsentbecauseanonymousdatawereused.This studyhasbeenregisteredinclinicaltrial.govNCT04314817.
Procedures and description of the pharmacovigilance cohort
As per the Medical Dictionary for Drug RegulatoryActivities(MedDRA)version23.1(Table S1),allrelevantCV-ADRs classified by group queries were prespecified
with remdesivir usage after sensitivity analysis and adjustment for multipleconfounders.HOW MIGHT THIS CHANGE CLINICAL PHARMACOLOGY OR
TRANSLATIONAL SCIENCE?Patientswithpre-existingCVcomorbiditiesorreceivinghigherdosesofremde-sivirmaybenefitfromadditionalcardiacmonitoring.Furtherstudyiswarrantedtoconfirmthefindings.

4 | JUNG et al.
andextractedforanalysis.Currently,thereisaconsider-ablelackofspecificCVtoxicityreportsonremdesivirforits recent FDA approval (October 2020) and EmergencyUseAuthorization(EUA)fromtheFDA(2020)aswellasapprovalandconditionalmarketingauthorizationintheEuropeanUnionandverylowaccumulationofreal-worlddata. Consequently, we used some specific cardiac andvascular preferred terms (PTs) for the analysis. Of note,ICSRsassociatedwithremdesivirhavebeenaccruing inVigiBasesinceFebruary2020.Theindividualreportsin-cludedpatientcharacteristics(age,sex,andnationality),drug information (indications, dosage, regimen, admin-istrationroute,anddurationprescribed),ADR(reportedAE, MedDRA classification terms, time to onset, natureandseverityofADR,fetaloutcomes,andmortality),andgeneral administrative information (date of report, re-porter qualification, and country of origin). Because thetimetoADRonsetwasnotconsistentlyreportedforrem-desivir,weusedtreatmentdurationasanalternativetoas-sumetheonsetperiod.AccordingtotheWHOdefinition,a serious reaction was described as an ADR associatedwithdeath,life-threateningcondition,hospitaladmissionorprolongationofhospitalization, chronic incapacityorimpairment, andconsequencesdeemedclinically severebythereportingphysician.17
Sensitivity analysis
BecausethenaturaldiseasecourseofCOVID-19isknownto involve myocardial injury and further challenges theCV system,18,19 it is crucial to distinguish drug-inducedCV-ADRsfromCOVID-19inducedCVeffects.Therefore,wefurtherconductedasensitivityanalysisbycomparingtheeffectofremdesivirandotherdrugsexclusivelyintheCOVID-19 diagnosed population, offsetting the effect ofCOVID-19 in cases and non-cases. The COVID-19 sub-populationwasdefinedbyeachcaseofCOVID-19relatedMedDRAtermastheindicationofremdesiviruse.
Statistical analysis
As VigiBase incorporates a dataset comprising a largesamplesizecollectedworldwide,itprovidesagoodfitforthestudyofdisproportionality(alsoknownascase–non-case analysis), for which sufficient sample size is indis-pensable to warrant applicable power and resolution.20We used the analysis to determine whether the propor-tionofCVtoxicitiesreportedforremdesivirdiffersfromthatoccurring in thedrugcontrolgroup (fulldatabase).Whenpatientsexposedtoaparticularmedication(cases)haveahigherpercentageofADRsthanthosenotexposed
tothatdrug(non-cases),thelinkbetweentheadversere-actionandtheindividualactivedrugmaysuggestapos-sible safety concern. Information component (IC) andreportingoddsratio(ROR)are indicatorvaluesusedforthedisproportionatereportingdevelopedbyUMC,whereanIC0.25(thelowerendofa95%credibleinterval)greaterthan0or lowerconfidence interval (CI)ofRORgreaterthan1indicatessignificantassociationsofspecificADRswiththedrugs.RORwascalculatedusingthechi-square(χ2) test as per the well-established reporting method ofpharmacovigilancestudies.21Whenthefulldatabasewasnot used as a comparator and sensitivity analyses wereconducted, ROR was reported rather than the IC to ex-pressdisproportionality.15Multivariateoddsratios(ORs)with95%CIswerecalculatedusinga logistic regressionmodeltoconsiderprespecifiedvariables,suchasage,sex,and multiple COVID-19 treatment drugs, including hy-droxychloroquine,corticosteroid,lopinavir-ritonavir,andinterferon.22,23 Dexamethasone, hydrocortisone, predni-solone, and prednisone were included for corticosteroidvariableas indicated instudyprotocolandguideline forCOVID-19treatment.23,24
TheICcomparesobservedandexpectedvaluestoiden-tifyAEsthatareassociatedwithparticulardrugsusingtheBayesian neural network method developed by UMC.25Probabilistic logic in intelligent systems—proven usefulin controlling big data—is reliable for handling missingdata,andcanbeusedforcomplexvariables.25Itisoftenvulnerabletospontaneousvariabilityforrareeventswithlowexpectedcounts,butstatisticalshrinkagesafeguardsagainstspuriousassociationsandtheshrinkageobserved-to-expected(OE)ratiooffersabasicbutefficientstructurefor large-scale pattern exploration.26This sensitive algo-rithmallowstheidentificationofsignalssoonafterdrugapproval by a regulatory agency, therefore, we used thismethodtodetectearlysignalsofremdesivirandidentifyanypotentialrisk.
Thefollowingstatisticalformulawasused:
whereNexpected=[Ndrug×Nreaction]/Ntotal.Nexpectedrepresentsthenumberofcasereportsexpected
for the drug-effect combination, whereas Nobserved indi-catestheactualnumberofcasereportsforthedrug-effectcombination.Furthermore,NdrugandNreactionspecifythenumberofcasereportsforthedrugirrespectiveofAEsandfor the effect irrespective of drug, respectively.25,26 Ntotalcorrespondtothetotalnumberofcasereportsinthefulldatabase. Qualitative variables were described as count(percentage), and continuous variables were expressedasmedianwithinterquartilerange(IQR).Theremdesivirand full database cases were compared using theχ2 test
IC = log2([Nobserved + 0.5]∕[Nexpected + 0.5])

| 5CARDIOVASCULAR EVENTS OF REMDESIVIR
orFisher’sexacttestforqualitativevariablesandtheun-paired Kruskal-Wallis test for continuous variables. Posthocpoweranalysesofthecomparisonsbetweentherem-desivirandfulldatabasecasesaswellastheremdesivirandCOVID-19caseswereperformedusingtheZtestofinde-pendentproportions.Alltestsweretwo-sided,andpvalueless than 0.05 was considered significant. All analyseswereconductedusingIBMstatisticalpackagefortheso-cialsciences(SPSS)version25.0(SPSSInc.)orRsoftware,version 3.6.0 (R Foundation for Statistical Computing).Power analyses were performed with G*Power, version3.1.9.6(Heinrich-Heine-Universität-Düsseldorf).
Generation of human pluripotent stem cells- derived cardiomyocytes
The human pluripotent stem cells (hPSCs) lines, whichinclude both human embryonic stem cells (hESC: H9:Wicell)andhuman-inducedpluripotent stemcells (hiP-SCs: CMC-hiPSC-011: KNIH) were maintained with theStemMACS iPS-BREW XF, human (Miltenyi Biotec) onMatrigel (Corning).Forderivation into thecardiac line-age,hPSCswereplatedontoanMatrigel-coatedcellcul-turedish(Eppendorf)at140,000cells/cm2dish.Atday0,6 μM/mlCHIR99021(Tocris)wastreatedintotheculturedhPSCstogetherwithbovineserumalbumin(BSA;Sigma-Aldrich) and ascorbic acid (Sigma-Aldrich). After 48 h,2 μM/mlofC59,aWntinhibitor(StemgentInc.)wasfor48 h.Spontaneouslycontractingcardiaclinagecellsbegantoappearasearlyasdifferentiationday8.Subsequently,L-lacticacidwasadded into theculturemedia topurifycardiomyocytes(CM)-derivedhPSCs(hPSC-CMs).
Cell viability assay
Variousconcentrationsofremdesivir(MedChemExpress)wasaddedtohPSC-CMsfor24 hor48 h,andthecellvi-ability was determined using the CellTiter 96 AQueousOne Solution Cell Proliferation Assay (MTS; Promega)accordingtothemanufacturer’sinstructions.Absorbanceat490 nm(A490)wasmeasuredusingaSynergyTMH1multi-modemicroplatereader(Biotek).Allthecellviabil-ityassayswereperformedatleastthreetimes.
RESULTS
CV- ADR signals
ThenumberofADRsreportedforremdesivirwas2107byAugust30,2020,andatotalof22,728,189all-drugADRs
have been reported since the inception of the database.BecauseADRsassociatedwithremdesivirduringtheout-breakofEBOVwasnotreportedtoVigiBase,ADRsrelatedtoremdesivirwerefirstrecordedinVigiBaseinFebruary2020,aftertheoutbreakofCOVID-19.Thetotalnumberofall-drugADRscorrespondingtotheintervalofinterest(fromFebruary2020toAugust2020)was1,403,532.ThenumberofspecificCV-ADRsislistedinTable 1.ThetotalnumberofpatientswithCOVID-19includedinouranaly-siswas5408,andthesensitivityanalysisoftheCOVID-19population alone is described in Table 2. Median (IQR)drugtreatmentduration(days)rangedfrom0(0–4)daysforventricularfibrillationto4(1–5)daysforatrialfibrilla-tion(Table 3).TheindicationforremdesivirwasCOVID-19-positive for all reported patients. Post hoc poweranalysis of the closest proportion comparison (atrioven-tricularblock)revealedapowerof0.634,withthesecondclosestcomparison(myocarditis)revealingapower0.996.
Weidentifiedeightcandidatesamong37broadCVout-comeswhereCV-ADRsweresignificantlyhigherinrem-desivir thantheywereintheentiredatabase(non-cases;Table 1).Remdesivirwasassociatedwithhigherreportingofcardiacarrest(ROR:19.9,95%CI:16.1–24.5,IC0.25:3.19),bradycardia (ROR: 15.0, 95% CI: 12.0–18.9, IC0.25: 2.83),shock(ROR:17.8,95%CI:11.2–28.1,IC0.25:2.56),hypoten-sion(ROR:5.9,95%CI:4.7–7.3,IC0.25:1.76),atrialfibrilla-tion(ROR:7.3,95%CI:5.0–10.6,IC0.25:1.64),ventriculartachycardia(ROR:17.8,95%CI:9.5–33.4,IC0.25:1.58),ven-tricular fibrillation (ROR:22.1,95%CI:10.4–47.1, IC0.25:1.18), and acute myocardial infarction (AMI; ROR: 15.5,95%CI:8.0–30.0,IC0.25:1.06).Theresultswereconsistentwiththethoseofsensitivityanalysesrestrictedtothepa-tientswithCOVID-19only,exceptforcardiogenicshock,atrial fibrillation, and ventricular tachycardia (Table 2).Afterfurtheradjustmentforvariousconfounders,includ-ingcorticosteroiduse,cardiacarrest(adjustedOR[aOR]:1.88,95%CI:1.08–3.29),bradycardia(aOR:2.09,95%CI:1.24–3.53),andhypotension(aOR:1.67,95%CI:1.03–2.73)were significantly associated with the use of remdesivir.Posthocpoweranalysisoftheclosestproportioncompari-son(cardiogenicshock)revealedapowerof1.00.
Characteristics of patients
Remdesivir-associated CV toxicity is a novel clinical en-tity and represents a new problem for clinicians treatingCOVID-19,and, therefore, additionaldatawerecollectedtofacilitatethedescriptionoftheclinicalcharacteristicsofremdesivir-associated CV-ADR in the 2107 identified pa-tients (Table 3).AllCV-ADRsassociatedwithremdesiviroccurred more frequently in male patients (51.6%-90.0%)thaninfemalepatients.Cardiacarrest,cardiogenicshock,

6 | JUNG et al.
T A B L E 1 DisproportionalityanalysisinVigiBasefromtheinceptionofthedatabasetoAugust30,2020
RemdesivirFull database (since inception) IC/IC025
Full database (since February 2020) ROR (95% CI)
TotalnumbersofICSRsavailable 2107 22,728,189 1,403,532
NumbersofICSRsbycardiovascularADRsubgroups
Cardiacarrest 93 (4.41) 83,581 (0.37) 3.50/3.19 3340 (0.24) 19.9 (16.1– 24.5)
Bradycardia 79 (3.75) 90,496 (0.40) 3.16/2.83 3703 (0.26) 15.0 (12.0– 18.9)
Cardiogenicshock 19 (0.90) 16,292 (0.07) 3.28/2.56 737 (0.05) 17.8 (11.2– 28.1)
Hypotension 86 (4.08) 215,210 (0.95) 2.01/1.76 10,194 (0.73) 5.9 (4.7– 7.3)
Atrialfibrillation 28 (1.33) 60,278 (0.27) 2.23/1.64 2624 (0.19) 7.3 (5.0– 10.6)
Ventriculartachycardia 10 (0.47) 13,208 (0.06) 2.61/1.58 385 (0.03) 17.8 (9.5– 33.4)
Ventricularfibrillation 7 (0.33) 9482 (0.04) 2.44/1.18 218 (0.02) 22.1 (10.4– 47.1)
Acutemyocardialinfarction 9 (0.43) 17,645 (0.08) 2.15/1.06 397 (0.03) 15.5 (8.0– 30.0)
Sinustachycardia 19(0.90) 213,580(0.94) −0.06/−0.78 10,467(0.75) NA
Hypertension 13(0.62) 176,559(0.78) −0.32/−1.21 7910(0.56) NA
Pulmonaryembolism 10(0.47) 75,522(00.33) 0.49/−0.54 2074(0.15) NA
Chestpain 7(0.33) 319,538(1.41) −2.00/−3.27 23,265(1.66) NA
ElectrocardiogramQTcorrectedintervalprolonged
4(0.19) 21,278(0.09) 0.86/−0.87 1746(0.12) NA
Ischemicstroke 3(0.14) 9860(0.04) 1.31/−0.74 429(0.03) NA
Systolicdysfunction 2(0.09) 970(0.00) 2.08/−0.51 189(0.01) NA
Atrialflutter 2(0.09) 5118(0.02) 1.36/−1.22 200(0.01) NA
Supraventriculartachycardia 2(0.09) 8478(0.04) 0.96/−1.63 249(0.02) NA
Bundlebranchblockright 2(0.09) 2731(0.01) 1.73/−0.86 105(0.01) NA
Jugularveinthrombosis 2(0.09) 1010(0.00) 2.07/−0.51 29(0.00) NA
Vertebralarteryobstruction 1(0.05) 123(0.00) 1.55/−2.55 5(0.00) NA
Cerebralhemorrhage 1(0.05) 36,338(0.16) −1.37/−5.16 1373(0.01) NA
Deepveinthrombosis 1(0.05) 58,504(0.26) −1.98/−5.78 1276(0.01) NA
Lacunarinfarction 1(0.05) 1543(0.01) 1.22/−2.58 20(0.00) NA
Rightventricledysfunction 1(0.05) 405(0.00) 1.48/−2.32 31(0.00) NA
Sinusnodedysfunction 1(0.05) 1972(0.01) 1.13/−2.66 34(0.00) NA
Transientischemicattack 1(0.05) 24,093(0.11) −0.87/−4.66 653(0.05) NA
Atrioventricularblock 1(0.05) 8770(0.04) 0.19/−3.61 232(0.02) NA
Rightventricularfailure 1(0.05) 7102(0.03) 0.37/−3.43 195(0.01) NA
Coronaryarterystenosis 1(0.05) 2651(0.01) 1.01/−2.79 38(0.00) NA
Carotidarteryocclusion 1(0.05) 1994(0.01) 1.13/−2.67 51(0.00) NA
STsegmentelevation 1(0.05) 1837(0.01) 1.16/−2.64 67(0.00) NA
Hypertensiveurgency 1(0.05) 132(0.00) 1.55/−2.25 16(0.00) NA
Torsadedepointes 1(0.05) 5583(0.02) 0.56/−3.24 154(0.01) NA
Myocarditis 1(0.05) 7340(0.03) 0.34/−3.45 411(0.03) NA
Pulmonaryhypertension 1(0.05) 16,720(0.07) −0.45/−4.25 514(0.04) NA
Syncope 1(0.05) 124,759(0.55) −3.00/−6.81 4259(0.30) NA
Palpitations 1(0.05) 215,552(0.95) −3.77/−7.57 14,559(1.04) NA
Note: Valuesaren(%)unlessotherwiseindicated.Informationcomponent(IC)andits95%credibilityintervallowerendpoint(IC025)comparingcardiacADRsassociatedwithremdesivirversusentiredatabaseinVigiBase(frominceptiononNovember14,1967,toAugust30,2020).ApositiveIC025value(>0)isthetraditionalthresholdusedforstatisticalsignaldetection(inbold).Forsignificantsignals,RORandits95%CIwerealsocalculatedusingentiredatabasefromFebruary1,2020,toAugust30,2020,ascomparator(contemporarycontrolgroupforremdesivir,firstremdesivirreportinFebruary2020).Abbreviations:ADR,adversedrugreaction;CI,confidenceinterval;ICSR,individualcasesafetyreport;NA,notapplicable;ROR,reportingoddsratio.

| 7CARDIOVASCULAR EVENTS OF REMDESIVIR
TA
BL
E 2
R
epor
ting
and
adju
sted
ors
fora
ssoc
iatio
nbe
twee
nca
rdio
vasc
ular
adv
erse
reac
tions
and
use
ofr
emde
sivi
rfor
pat
ient
swith
CO
VID
-19
inV
igiB
ase
Spec
ific
AD
Rs
Exp
osur
esC
ases
Non
- cas
esT
otal
RO
R (9
5% C
I)M
inim
ally
adj
uste
d O
Ra (9
5% C
I)Fu
lly a
djus
ted
OR
b (95%
CI)
Car
diac
arr
est
Rem
desi
vir
65(3
.58%
)17
4918
143.
78 (2
.50–
5.72
)3.
91 (2
.44-
6.28
)1.
88 (1
.08–
3.29
)
Oth
erd
rugs
pre
scri
bed
forC
OV
ID-1
935
(0.9
7%)
3559
3594
1(r
efer
ence
)
Brad
ycar
dia
Rem
desi
vir
66(3
.64%
)17
4818
142.
12 (1
.49–
3.00
)1.
93 (1
.32–
2.82
)2.
09 (1
.24–
3.53
)
Oth
erd
rugs
pre
scri
bed
forC
OV
ID-1
963
(1.7
5%)
3531
3594
1(r
efer
ence
)
Car
diog
enic
shoc
kR
emde
sivi
r2
(0.1
1%)
1812
1814
1.98
(0.2
8–14
.08)
2.67
(0.2
4–29
.89)
0.99
(0.0
9–11
.40)
Oth
erd
rugs
pre
scri
bed
forC
OV
ID-1
92
(0.0
6%)
3592
3594
1(r
efer
ence
)
Hyp
oten
sion
Rem
desi
vir
72(3
.97%
)17
4218
143.
26 (2
.24–
4.75
)3.
56 (2
.31–
5.47
)1.
67 (1
.03–
2.73
)
Oth
erd
rugs
pre
scri
bed
forC
OV
ID-1
945
(1.2
5%)
3549
3594
1(r
efer
ence
)
Atr
ialf
ibri
llatio
nR
emde
sivi
r22
(1.2
1%)
1792
1814
1.75
(0.9
9–3.
12)
1.39
(0.7
6–2.
55)
2.25
(0.9
2–5.
52)
Oth
erd
rugs
pre
scri
bed
forC
OV
ID-1
925
(0.7
0%)
3569
3594
1(r
efer
ence
)
Ven
tric
ular
tach
ycar
dia
Rem
desi
vir
10(0
.55%
)18
0418
141.
10(0
.51–
2.39
)1.
09(0
.47–
2.52
)1.
36(0
.42–
4.41
)
Oth
erd
rugs
pre
scri
bed
forC
OV
ID-1
918
(0.5
0%)
3576
3594
1(r
efer
ence
)
Ven
tric
ular
fibr
illat
ion
Rem
desi
vir
7(0
.39%
)18
0718
144.
64 (1
.20–
17.9
5)5.
77 (1
.15–
28.8
9)3.
96(0
.54–
28.8
4)
Oth
erd
rugs
pre
scri
bed
forC
OV
ID-1
93
(0.0
8%)
3591
3594
1(r
efer
ence
)
Acu
tem
yoca
rdia
linf
arct
ion
Rem
desi
vir
9(0
.50%
)18
0518
148.
96 (1
.93–
41.4
9)7.
22 (1
.51–
34.4
3)3.
49(0
.51–
23.9
5)
Oth
erd
rugs
pre
scri
bed
forC
OV
ID-1
92
(0.0
6%)
3592
3594
1(r
efer
ence
)
Stat
istic
ally
sign
ifica
ntA
DR
swer
epr
esen
ted
inb
old.
Abb
revi
atio
ns:A
DR
,adv
erse
dru
gre
actio
n;C
OV
ID-1
9,c
oron
avir
usd
isea
se2
019;
OR
,odd
srat
io.
a Adj
uste
dva
riab
lesw
ere
age
and
sex.
b Adj
uste
dva
riab
lesw
ere
age,
sex,
and
CO
VID
-19
trea
tmen
tmed
icat
ions
incl
udin
ghy
drox
ychl
oroq
uine
/chl
oroq
uine
,dex
amet
haso
nea
nde
quiv
alen
ts,l
opin
avir
-rito
navi
r,an
din
terf
eron
.We
used
the
case
non
-cas
em
etho
d,w
hich
issi
mila
rto
case
-con
trol
stud
ies,
buta
dapt
edfo
rpha
rmac
ovig
ilanc
est
udie
s.W
eus
edre
port
ing
odds
ratio
s(R
OR
s)a
ndth
eir9
5%c
onfid
ence
inte
rval
(95%
CI)
toc
alcu
late
dis
prop
ortio
nalit
y.R
OR
isa
ra
tiosi
mila
rin
conc
eptt
oth
eO
Rin
cas
eco
ntro
lstu
dies
and
cor
resp
onds
toth
eex
posu
reo
ddsa
mon
gre
port
edc
ases
ofc
ardi
ovas
cula
rdis
orde
rso
vert
hee
xpos
ure
odds
am
ong
repo
rted
non
-cas
e.C
ases
wer
ein
divi
dual
ca
sesa
fety
repo
rtsw
hich
show
edsi
gnifi
cant
sign
als(
defin
eda
sIC
025>
0).N
on-c
ases
wer
ein
divi
dual
cas
esa
fety
repo
rtsc
onta
inin
gal
loth
era
dver
see
vent
srep
orte
dlin
ked
with
the
resp
ectiv
edr
ug.T
oid
entif
ypa
tient
sw
ithC
OV
ID-1
9,a
nyfo
llow
ing
keyw
ords
app
eari
ngin
the
indi
catio
nfie
ldw
ere
incl
uded
:CO
VID
-19,
CO
VID
19,S
AR
S-C
OV
-2,S
AR
S-C
OV
2,a
ndC
OV
IDw
ith/w
ithou
tpne
umon
ia.T
here
leva
ntte
rmo
f“co
rona
viru
sin
fect
ion”
was
con
ceiv
eda
sCO
VID
-19
infe
ctio
nin
rem
desi
virg
roup
.How
ever
,for
non
-rem
desi
virg
roup
,the
term
was
exc
lude
dto
avo
idth
efa
lse-
posi
tive
resu
ltsd
ueto
cor
onav
irus
infe
ctio
nsn
otc
orre
spon
dto
C
OV
ID-1
9.

8 | JUNG et al.
TA
BL
E 3
C
hara
cter
istic
sofr
epor
ted
ICSR
swith
car
diac
AD
Rsa
ssoc
iate
dw
ithre
mde
sivi
rin
Vig
iBas
e(la
sta
cces
sed
Aug
ust3
0,2
020)
Car
diac
arr
est
(n =
93)
Bra
dyca
rdia
(n
= 7
9)C
ardi
ogen
icsh
ock
(n =
19)
Hyp
oten
sion
(n
= 8
6)A
. fib
(n =
28)
VT
(n =
10)
AM
I (n
= 9
)V
. fib
(n =
7)
Reg
ions
repo
rtin
g93
(100
.0)
79 (1
00.0
)19
(100
.0)
86 (1
00.0
)28
(100
.0)
10 (1
00.0
)9
(100
.0)
7 (1
00.0
)
Am
eric
as91
/93
(97.
8)78
/79
(98.
7)19
/19
(100
.0)
82/8
6(9
5.3)
27(9
6.4)
9/10
(90.
0)8/
9(8
8.9)
6/7
(85.
7)
Euro
pe2/
93(2
.2)
1/79
(1.3
)0/
19(0
.0)
3/86
(3.5
)1
(3.6
)1/
10(1
0.0)
1/9
(11.
1)1/
7(1
4.3)
Aus
tral
ia0/
93(0
.0)
0/79
(0.0
)0/
19(0
.0)
1/86
(1.2
)0
(0.0
)0/
10(0
.0)
0/9
(0.0
)0/
7(0
.0)
Asi
a0/
93(0
.0)
0/79
(0.0
)0/
19(0
.0)
0/86
(0.0
)0
(0.0
)0/
10(0
.0)
0/9
(0.0
)0/
7(0
.0)
Afr
ica
0/93
(0.0
)0/
79(0
.0)
0/19
(0.0
)0/
86(0
.0)
0(0
.0)
0/10
(0.0
)0/
9(0
.0)
0/7
(0.0
)
Rep
ortf
rom
cl
inic
altr
ials
4/93
(4.3
)0/
79(0
.0)
0/19
(0.0
)1/
86(1
.2)
1(3
.6)
1/10
(10.
0)0/
9(0
.0)
1/7
(14.
3)
Rep
ortin
gm
onth
s93
(100
.0)
79 (1
00.0
)19
(100
.0)
86 (1
00.0
)28
(100
.0)
10 (1
00.0
)9
(100
.0)
7 (1
00.0
)
2020
.02–
2020
.05
0/93
(0.0
)0/
79(0
.0)
0(0
.0)
2(2
.3)
1/28
(3.6
)1/
10(1
0.0)
0(0
.0)
1/7
(14.
3)
2020
.06
1/93
(1.1
)7/
79(8
.9)
6(3
1.6)
22(2
5.6)
6/28
(21.
4)2/
10(2
0.0)
0(0
.0)
4/7
(57.
1)
2020
.07
1/93
(1.1
)1/
79(1
.3)
0(0
.0)
1(1
.2)
0/28
(0.0
)0/
10(0
.0)
0(0
.0)
0/7
(0.0
)
2020
.08
91/9
3(9
7.8)
71/7
9(8
9.9)
13(6
8.4)
61(7
0.9)
21/2
8(7
5.0)
7/10
(70.
0)9
(100
.0)
2/7
(28.
6)
Rep
orte
r91
(97.
8)77
(97.
5)18
(94.
7)81
(94.
2)26
(92.
9)10
(100
.0)
9 (1
00.0
)7
(100
.0)
Hea
lthc
are
prof
essi
onal
91/9
1(1
00.0
)76
/77
(98.
9)18
/18
(100
.0)
79/8
1(9
7.6)
26/2
6(1
00.0
)10
/10
(100
.0)
9/9
(100
.0)
7/7
(100
.0)
Non
-hea
lthc
are
prof
essi
onal
0/91
(0.0
)1/
77(1
.0)
0/18
(0.0
)2/
81(2
.4)
0(0
.0)
0/10
(0.0
)0
(0.0
)0/
7(0
.0)
Age
gro
ups
90 (9
6.8)
74 (9
3.7)
19 (1
00.0
)84
(97.
6)28
(100
.0)
10 (1
0.0)
9 (1
00.0
)7
(100
.0)
<18
yea
rs1/
90(1
.1)
1/74
(1.4
)0/
19(0
.0)
1/84
(1.2
)0/
28(0
.0)
0/10
(0.0
)1
(11.
1)0/
7(0
.0)
18–4
4 ye
ars
6/90
(6.7
)11
(14.
8)0/
19(0
.0)
8/84
(9.5
)0/
28(0
.0)
3/10
(30.
0)2
(22.
2)2/
7(2
8.6)
45–6
4 ye
ars
37/9
0(4
1.1)
28(3
7.8)
11/1
9(5
7.9)
34/8
4(4
0.5)
12/2
8(4
2.9)
1/10
(10.
0)1
(11.
1)0/
7(0
.0)
65–7
4 ye
ars
29/9
0(3
2.2)
12(1
6.2)
7/19
(36.
8)19
/84
(22.
6)6/
28(2
1.4)
4/10
(40.
0)2
(22.
2)5/
7(7
1.4)
≥75
year
s17
/90
(18.
3)23
(31.
1)1/
19(5
.3)
22/8
4(2
6.2)
10/2
8(3
5.7)
2/10
(20.
0)3
(33.
3)0/
7(0
.0)
Sex
93 (1
00.0
)78
(98.
7)19
(100
.0)
85 (9
8.9)
28 (1
00.0
)10
(10.
0)9
(100
.0)
7 (1
00.0
)
Mal
e48
/93
(51.
6)41
/78
(52.
6)13
/19
(68.
4)45
/85
(52.
9)16
(57.
1)9/
10(9
0.0)
5/9
(55.
6)4
(57.
1)
Fem
ale
45/9
3(4
8.4)
37/7
8(4
7.4)
6/19
(31.
6)40
/85
(47.
1)12
(42.
9)1/
10(1
0.0)
4/9
(44.
4)3
(42.
9)
Seri
ousA
DR
s93
(100
.0)
79 (1
00.0
)19
(100
.0)
86 (1
00.0
)28
(100
.0)
10 (1
00.0
)9
(100
.0)
7 (1
00.0
)
91/9
3(9
7.8)
65/7
9(8
2.3)
19/1
9(1
00.0
)86
/86
(100
.0)
26/2
8(9
2.9)
8(8
0.0)
9/9
(100
.0)
7/7
(100
.0)
Out
com
es20
(21.
5)19
(24.
1)8
(42.
1)8
(9.3
)7
(25.
0)4
(40.
0)3
(33.
3)3
(42.
9)
Dea
ths
19/2
0(9
5.0)
4/19
(21.
1)2/
8(2
5.0)
4/8
(50.
0)0
(0.0
)1
(25.
0)2/
3(6
6.7)
2/3
(66.
7)

| 9CARDIOVASCULAR EVENTS OF REMDESIVIR
hypotension, and ventricular fibrillation were the com-monlyreportedCV-ADRsinpatientsagedbetween45and74 years.Bradycardia,atrialfibrillation,ventriculartachy-cardia,andAMIprimarilyoccurredinpatientsgreaterthan75 yearsofage.TheproportionsofseriousCV-ADRsweregenerallyhigh,rangingfrom80%forventriculartachycar-diato100%forcardiogenicshock,hypotension,AMI,andventricular fibrillation. Almost all cases were reported aspartofclinicalcareandnotclinicaltrials,andmostweread-ditionallyreportedbyhealthprofessionals(Tables S2–S9).
Outcomes
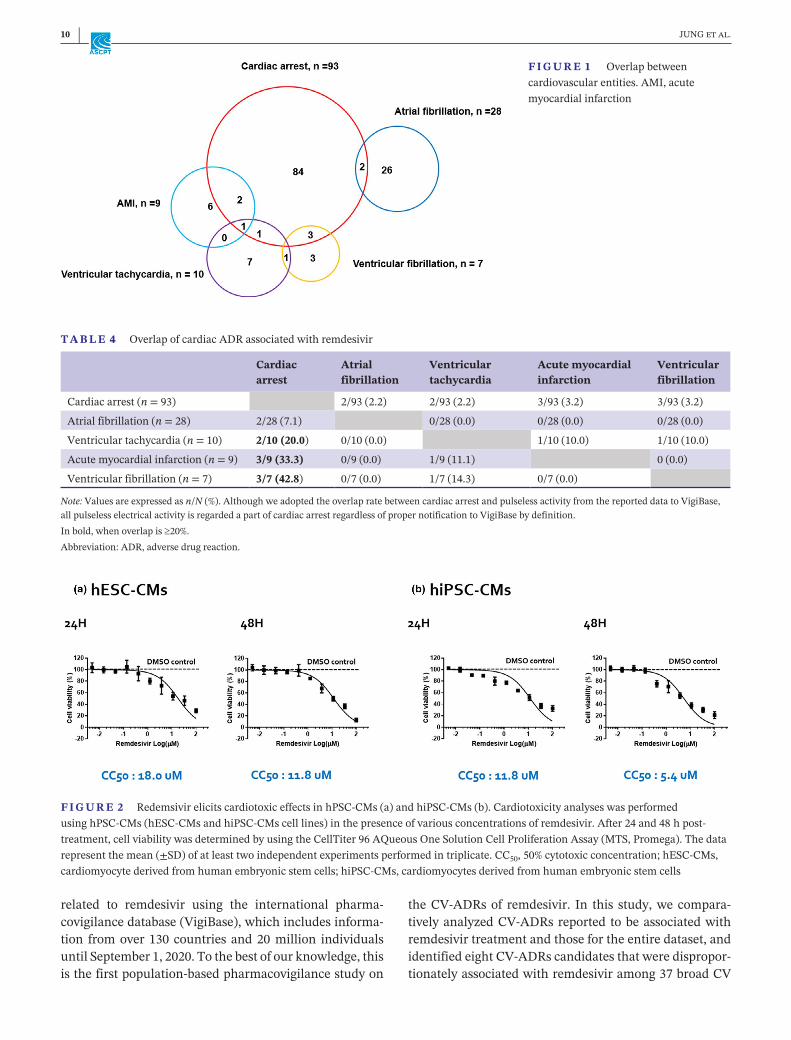
Theoverlapsbetween identifiedCV-ADRsare shown inFigure 1andTable 4.AMIcaseswere frequentlyassoci-atedwithconcurrentconditions(Table 4),suchascardiacarrest (33.3%) and, in rare cases, ventricular tachycar-dia (11.1%). Ventricular fibrillation was often associ-ated with cardiac arrest (42.8%). Most of these eight CVeventsoccurredwithotherseriousADRs,exceptforatrialfibrillation.
Remdesivir induced cardiotoxicity on hPSC- CMs in vitro
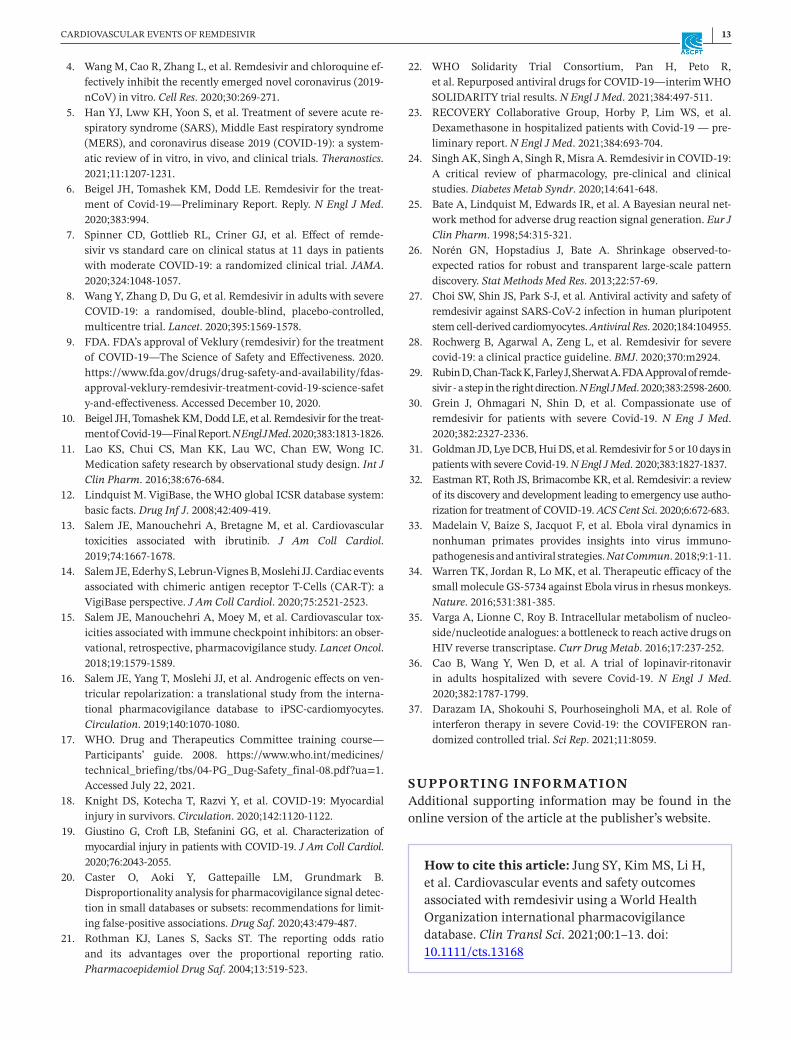
Toexaminewhetherremdesivircould inducecardiotox-icity in the human heart within the range of half maxi-maleffectiveantiviralconcentration (EC50), theculturehPSC-CMs were treated with increasing concentrationsofremdesivir,andthecellviabilitywasmeasuredat24 hand48 haftertreatmentusingcellproliferationassay.Weobserved that remdesivir treatment induced substantialcytotoxic effects in CMs derived from both hESCs andhiPSCs(Figure 2).Inaddition,treatmentwithremdesivirforalongertime(48 h)demonstratedsignificantlylowercell viability of hPSCS-CMs as compared to 24 h post-treatment, indicatingtime-anddose-dependentreactionandpotentialinducedcardiotoxicitybyremdesivir.Thesefindings are consistent with previous reports of dose-dependentremdesivirtoxicity.27
DISCUSSION
OnOctober22,2020,theFDAapprovedremdesivirasthefirst drug to treat hospitalized patients with COVID-19,andtheapprovalmayhaverapidlyincreasedremdesiviruseworldwide.Thelargeincreaseinremdesivirdemandand associated ADR reports warrant urgent pharma-covigilant evaluations of this drug.28,29 We conducted aclinical characterization of CV-ADRs disproportionally
Car
diac
arr
est
(n =
93)
Bra
dyca
rdia
(n
= 7
9)C
ardi
ogen
icsh
ock
(n =
19)
Hyp
oten
sion
(n
= 8
6)A
. fib
(n =
28)
VT
(n =
10)
AM
I (n
= 9
)V
. fib
(n =
7)
Dru
gtr
eatm
ent
dura
tion
81 (8
7.1)
61 (7
7.2)
16 (8
4.2)
74 (8
6.0)
23 (8
2.1)
8 (8
0.0)
8 (8
8.9)
7 (1
00.0
)
Med
ian
days
(IQ
R,
min
-max
)2.
0(0
.0–4
.0,
0.0–
13.0
)4.
0(0
.0–4
.0,
0.0–
10.0
)2.
0(0
.0–4
.0,
0.0–
9.0)
3.0
(1.0
–4.0
,0.
0–10
.0)
4.0
(1.0
–5.0
,0.
0–9.
0)2.
0(0
.8–4
.0,
0.0–
8.0)
1.0
(0.0
–3.5
,0.
0–9.
0)0.
0(0
.0–4
.0,
0.0–
8.0)
Indi
catio
ns86
(92.
5)64
(81.
0)19
(100
.0)
73 (8
4.5)
23 (8
2.1)
9 (9
0.0)
9 (1
00.0
)7
(100
.0)
CO
VID
-19
86/8
6(1
00.0
)64
/64
(100
.0)
19/1
9(1
00.0
)73
/73
(100
.0)
23/2
3(1
00.0
)9/
9(1
00.0
)9
/9(1
00.0
)7/
7(1
00.0
)
Not
e: V
alue
sare
n(%
)orn
/N(%
),un
less
oth
erw
ise
indi
cate
d.A
vaila
bilit
yof
dat
ais
men
tione
din
bol
dan
dto
pro
ws.
Ase
vere
AD
Rw
asd
efin
eda
slife
thre
aten
ing,
cau
sing
top
ersi
sten
tors
igni
fican
tdis
abili
ty,o
rre
quir
ing
hosp
italiz
atio
n(fi
rsto
rpro
long
ed)o
rwhe
nca
usin
gde
ath.
Abb
revi
atio
ns:A
DR
,adv
erse
dru
gre
actio
n;A
.fib
,atr
ialf
ibri
llatio
n;A
MI,
acut
em
yoca
rdia
linf
arct
ion;
CO
VID
-19,
cor
onar
viru
sdis
ease
201
9;IC
SR,i
ndiv
idua
lcas
esa
fety
repo
rt;I
QR
,int
erqu
artil
era
nge;
min
-max
,m
inim
um-m
axim
um;V
.fib
,ven
tric
ular
fibr
illat
ion;
VT,
ven
tric
ular
tach
ycar
dia.
TA
BL
E 3
(C
ontin
ued)
10 | JUNG et al.
related to remdesivir using the international pharma-covigilancedatabase(VigiBase),whichincludesinforma-tion from over 130 countries and 20 million individualsuntilSeptember1,2020.Tothebestofourknowledge,thisisthefirstpopulation-basedpharmacovigilancestudyon
the CV-ADRs of remdesivir. In this study, we compara-tivelyanalyzedCV-ADRsreported tobeassociatedwithremdesivirtreatmentandthosefortheentiredataset,andidentifiedeightCV-ADRscandidatesthatweredispropor-tionatelyassociatedwithremdesiviramong37broadCV
F I G U R E 1 Overlapbetweencardiovascularentities.AMI,acutemyocardialinfarction
T A B L E 4 OverlapofcardiacADRassociatedwithremdesivir
Cardiac arrest
Atrial fibrillation
Ventricular tachycardia
Acute myocardial infarction
Ventricular fibrillation
Cardiacarrest(n=93) 2/93(2.2) 2/93(2.2) 3/93(3.2) 3/93(3.2)
Atrialfibrillation(n=28) 2/28(7.1) 0/28(0.0) 0/28(0.0) 0/28(0.0)
Ventriculartachycardia(n=10) 2/10 (20.0) 0/10(0.0) 1/10(10.0) 1/10(10.0)
Acutemyocardialinfarction(n=9) 3/9 (33.3) 0/9(0.0) 1/9(11.1) 0(0.0)
Ventricularfibrillation(n=7) 3/7 (42.8) 0/7(0.0) 1/7(14.3) 0/7(0.0)
Note: Valuesareexpressedasn/N(%).AlthoughweadoptedtheoverlapratebetweencardiacarrestandpulselessactivityfromthereporteddatatoVigiBase,allpulselesselectricalactivityisregardedapartofcardiacarrestregardlessofpropernotificationtoVigiBasebydefinition.Inbold,whenoverlapis≥20%.Abbreviation:ADR,adversedrugreaction.
F I G U R E 2 RedemsivirelicitscardiotoxiceffectsinhPSC-CMs(a)andhiPSC-CMs(b).CardiotoxicityanalyseswasperformedusinghPSC-CMs(hESC-CMsandhiPSC-CMscelllines)inthepresenceofvariousconcentrationsofremdesivir.After24and48 hpost-treatment,cellviabilitywasdeterminedbyusingtheCellTiter96AQueousOneSolutionCellProliferationAssay(MTS,Promega).Thedatarepresentthemean(±SD)ofatleasttwoindependentexperimentsperformedintriplicate.CC50,50%cytotoxicconcentration;hESC-CMs,cardiomyocytederivedfromhumanembryonicstemcells;hiPSC-CMs,cardiomyocytesderivedfromhumanembryonicstemcells

| 11CARDIOVASCULAR EVENTS OF REMDESIVIR
outcomes;thesewerecardiacarrest,bradycardia,shock,hypotension, atrial fibrillation, ventricular tachycardia,ventricularfibrillation,andAMI(Table 1).Todistinguishdrug-inducedCV-ADRs fromCOVID-19-inducedCVef-fects,18,19 we further restricted the analysis to patientswithCOVID-19andtheresultswereconsistent,exceptforcardiogenicshock,atrialfibrillation,andventriculartach-ycardia.However,theeffectsizes(ROR)ofallCV-ADRsweresmallerthanthoseoftheresultsoftheoverallpopu-lation,indicatingthattheRORsofCV-ADRsderivedfromtheoveralldatabasewereoverestimated,perhapsduetothe intrinsic COVID-19 CV deleterious effects (Tables 1and2).After furtheradjustment forpotentialconfound-ers(i.e.,corticosteroiduse),cardiacarrest(aOR:1.88,95%CI:1.08–3.29),bradycardia(aOR:2.09,95%CI:1.24–3.53),andhypotension(aOR:1.67,95%CI:1.03–2.73)weresig-nificantlyassociatedwiththeuseofremdesivir.
TheprevalenceintheVigiBaseforcardiacarrest,bra-dycardia, and severe hypotension was reported to be ashighas3.58%,3.64%,and3.97%,respectively,inpatientswith COVID-19 taking remdesivir, whereas they were0.97%, 1.75%, and 1.25%, respectively, in patients withCOVID-19takingotherdrugs(Table 2);therateofcardiacarrestandserioushypotensionwithremdesivir reportedinthisstudywasmarginallyhigherthanthepooledinci-dencerateofcardiacarrestandseverehypotensionfromclinicaltrials(1.3%and1.0%,respectively,asdescribedinTable S10).7,8,10,30,31Thediscrepanciescouldbeexplainedinpartbydifferencesintheincludedcases.Ofnote,thetotal number of remdesivir users in VigiBase (2107 pa-tients) corresponds to a total number of any ADRs re-ported on remdesivir (e.g., hepatotoxicity) and does notincluderemdesiviruserswithoutanyADRs;therefore,ac-tualADRratemaybemuchlowerinthegeneralpopula-tionandtheprevalenceratesreportedinVigiBaseshouldnotbetakenasabsoluteprevalenceratesinthereal-worldsettings.
GileadSciencesbegandevelopingremdesivirasearlyas2009asanagentagainstRNA-basedviruseswithhightransmission potential.32 Early studies mainly focusedon the efficacy of remdesivir against SARS and EBOV,becauseitprotectedprimatekidneyepithelialcells fromSARS-induced cytotoxicity,32 and significantly improvedthesurvivalofEBOV-infectedprimatemodels.33,34Theef-fectivenessofremdesivirwaspreservedtovaryingdegreesagainstvariousotherviruses,includingthehumanimmu-nodeficiencyvirus(HIV),MERS-CoV,anddeltacoronavi-ruses.3,35Althoughremdesivirdemonstrateseffectivenessagainst several viruses, it was not extensively used inmainstreamclinicalpracticeuntilitwasrepurposedasapotentialtherapeuticagentforCOVID-19in2020,andwassubsequentlyintegratedintoclinicalpracticeasaspecifictreatment.28 In addition, parallel studies evaluating its
effectiveness in reducing mortality and time-to-recoveryhavebeenconducted.8,10,30
Numerous efficacy studies and increased applicationofremdesivirhavenotbeenmatchedbypopulation-basedsafetyevaluations.Asremdesivirisarelativelynovelagentinthemarket,itsADRevaluationissubstantiallylackingcompared to other repurposed drug agents used to man-ageCOVID-19.Todate,afewclinicaltrialshavereportedmajor CV-ADRs associated with remdesivir (Tables S10andS11),7,8,10,30,31butthesetrialshaveinvestigatedeffectsonly in severalhundredpatients,whichmaynotcapturerarebutfatalCV-ADRsand,thus,thesefindingscannotbeextrapolatedtolargepopulations.Pharmacovigilancestud-iesusingVigiBase,withICSRsfrom20 millionindividuals,areuniquelypoisedtoidentifyADRsthatclinicaltrialsmaynotdetect,asdemonstratedinpreviousstudies.13–16,36Thepresentstudyrepresentsthefirstlarge-casepharmacovigi-lanceevaluationofremdesivirandprovidesnovelinsightsintoremdesivirADRclinicalspectrums.
GiventhatCOVID-19cancausemyocardialinjuryandchallengestheCVsystembyinflammatoryactivationandhypoxia,18,19itisuncertainifthehigherratesofCVeventsinpatients taking remdesivirarecausedbyadverse reac-tions of remdesivir or by severe COVID-19. To confirmthebiologicalcausation,wedesignedinvitroexperimentsusing hPSC-CM and found that remdesivir indeed re-ducedcellviabilityofhPSC-CMs;thecytotoxiceffectofthedrugincreasedwiththeescalationofdosage.Someofourgrouppreviouslydemonstratedthatremdesivirhashigherpotency for reducing cell viability, whereas less likely tointroduce arrhythmogenic risk compared with hydroxy-chloroquine,albeitbothdrugseventuallycausecardiotox-icityandarrhythmogenicriskathighconcentration27;ourindependentexperimentshereinreplicatedthefindingsde-notedbyChoietal.underamock-infectedcontrolsetting.Althoughtheexperimentswerelimitedtoinvitroandthedataalonedonotguaranteetheextrapolationoftheresultsto clinical settings, they provided a biological plausibilityforourobservationalfindings.Altogether,ourfindingsatthe population-level captured cardiotoxicity associatedwithremdesivirdistinguishedfromtheCOVID-19naturalcourses,andthesefindingsmayhelpphysiciansbeawareofpotentialCVadverseconsequencesfollowingremdesivir.
Study limitations
Ourstudyhassomelimitationsthatareworthnoting.First,althoughweconductedasensitivityanalysiswithpatientswithCOVID-19andsubsequentmultivariableanalysestominimize the confounding effect on CV outcomes by thenatureofCOVID-19,somedegreesofconfoundingmayper-sistasabias.Remdesivirtrialshavedemonstratedgreatest

12 | JUNG et al.
efficacy in moderate to severe COVID-19.22 It is possiblethattheCV-ADRsfromcasesthatwarrantremdesivirtreat-mentreflectmoresevereunderlyinginfectionratherthandrugtoxicity.AlthoughotherdrugsusedtotreatCOVID-19atthetime,suchaslopinavir-ritonavir,37interferon,37anddexamethasone,23 were either used primarily for or mosteffectiveinmoderatetosevereinfection,thepossibilityofthisbiascouldnotbeentirelyeliminated.Wefurthercon-ductedexperimentalresearchtounderstandthegenuineef-fectofthedrugonhPSC-CMs,yettheresultsareprimarilylimitedtoinvitroandthusshouldnotbeoverinterpreted.Second, national drug authorities may have overlookedsomedrug-inducedCV-ADRcasesandnotincludedtheseeventsinVigiBase, introducingpotentialreportingbiases.Inaddition,comorbiditieswerenotcompletelyreportedtoVigiBaseandthusadjustmentforthebaselinecharacteris-ticswaslimited.DisproportionalityanalysesareprimarilyusedtogenerateADRsignalsinanexploratorymannerandcannotbeinterpretedtoquantifytheriskofanygivenADR.However,thecountermeasureofthisstudyliesonthemostextensiveADRdatatodatethatincludeICSRsfrommorethan130nations,whichhelpsclassifyrarebutfatalADRs.Nevertheless,ourresultsfromVigiBasewouldbebettertobevalidatedbyimportantpharmacovigilancedababaseasFDAAEreportingsystem.Third,thedosageofremdesivirusedforinvitroexperimentsmaydifferfromthatusedfortreatment. As such, the experimental dosages should betakensimplyasinferencesofadose-responserelationshipandevidenceofcausality,andnotactualtherapeuticeffectmeasures.Last,ourstudydidnotbeginwithtotalexposuredataforremdesivirbut,rather,reliesondisproportionalityanalysesbetweenADRsofremdesivirandthetotalnumberofADRsreportedtothedatabase.However,theadvantageofVigiBaseandthemethodsusedinthisstudy(dispropor-tionateanalysis)hasbeenwell-establishedthroughnumer-ous studies13–16,36 and may provide reliable and sufficientevidencetosupportpotentialsafetyconcernswiththein-creasedadministrationofremdesivir.
STUDY HIGHLIGHTS
RemdesivirisadministeredforCOVID-19,butCVsafetydataarelimited,conflicting,andderivefromasmallse-lection of clinical trials. This study attempts to identifyandquantifyadverseCVoutcomesassociatedwithrem-desiviruse.Wefindthatremdesivirputativelyassociatedwithcardiacarrest,bradycardia,andhypotension,whichhasbeeninpartvalidatedinvitroasacytotoxiceffectonhPSC-derivedcardiomyocytes.Cliniciansshouldbeawareof potential CV consequences following remdesivir use,albeit infrequent. Adequate cardiac monitoring shouldbeinstitutedtomaintainatolerablesafetymarginwhen
usingremdesiviruntilfurthermatchedprospectiveobser-vationalstudiesconfirmtheCVsafetyofremdesivir.
ACKNOWLEDGEMENTSThe authors appreciate members of the custom searchteam at the Uppsala Monitoring Centre (Uppsala,Sweden) research section, who were invaluable to thesuccessful performance of this study. The supplied datafromVigiBasewasobtainedfromvarioussourcesandthelikelihoodofacausalrelationshipwasnotthesameinallreports.Finally,theresultsandconclusionsofthisstudydonotrepresenttheopinionoftheWHO.
CONFLICT OF INTERESTAllauthorshavenoconflictofinterest.
AUTHOR CONTRIBUTIONSJ.I.S.,S.Y.J.,M.S.K.,H.L.,K.H.L.,S.C.,S.H.H.,S.K.C.,L.J.,J.S.,D.K.Y.,S.W.L.,K.K.,A.Y.K.,K.B.,andL.S.wrotethemanuscript.J.I.S.,S.Y.J.,M.S.K.,A.Ko.,M.S.,A.Kr.,R.A.G.,N.K.K.,L.J.,J.S.,D.K.Y.,S.W.L.,K.K.,J.W.J.,andJ.Y.C.de-signedtheresearch.J.I.S.,S.Y.J.,M.S.K.,H.L.,E.D.,K.T.,S.C.,S.T.,N.K.K.,J.S.S.,S.J.P.,S.W.C.,K.B.,S.H.M.,Y.Y.G.,and L.S. performed the research. J.I.S., S.Y.J., M.S.K.,K.H.L.,A.Ko.,A.Kr.,S.H.H.,R.A.G.,N.K.K.,J.S.,D.K.Y.,S.W.L., and K.B analyzed the data. J.I.S., S.Y.J., M.S.K.,H.L.,M.S.,E.D.,J.S.,J.S.S.,S.J.P.,S.W.L.,andK.B.contrib-uted new reagents/analytical tools. This manuscript hasbeenreviewedandapprovedbyallauthors.
ORCIDSe Yong Jung https://orcid.org/0000-0003-1337-563XKeum Hwa Lee https://orcid.org/0000-0002-1511-9587Ai Koyanagi https://orcid.org/0000-0002-9565-5004Andreas Kronbichler https://orcid.org/0000-0002-2945-2946Salvatore Terrazzino https://orcid.org/0000-0002-4909-1121Louis Jacob https://orcid.org/0000-0003-1071-1239Joe- Elie Salem https://orcid.org/0000-0002-0331-3307Dong Keon Yon https://orcid.org/0000-0003-1628-9948Seung Won Lee https://orcid.org/0000-0001-5632-5208Jae Il Shin https://orcid.org/0000-0003-2326-1820
REFERENCES 1. Kim JS, Lee JY, Yang JW, et al. Immunopathogenesis and
treatment of cytokine storm in COVID-19. Theranostics.2021;11:316-329.
2. HelmyYA,FawzyM,ElaswadA,SobiehA,KenneySP,ShehataAA.TheCOVID-19pandemic:acomprehensivereviewoftax-onomy,genetics,epidemiology,diagnosis,treatment,andcon-trol.J Clin Med.2020;9:1225.
3. BrownAJ,WonJJ,GrahamRL,etal.Broadspectrumantiviralremdesivir inhibits human endemic and zoonotic deltacoro-naviruseswithahighlydivergentRNAdependentRNApoly-merase.Antiviral Res.2019;169:104541.
| 13CARDIOVASCULAR EVENTS OF REMDESIVIR
4. WangM,CaoR,ZhangL,etal.Remdesivirandchloroquineef-fectivelyinhibittherecentlyemergednovelcoronavirus(2019-nCoV)invitro.Cell Res.2020;30:269-271.
5. HanYJ,LwwKH,YoonS,etal.Treatmentofsevereacutere-spiratorysyndrome(SARS),MiddleEastrespiratorysyndrome(MERS),andcoronavirusdisease2019(COVID-19):asystem-aticreviewofinvitro,invivo,andclinicaltrials.Theranostics.2021;11:1207-1231.
6. BeigelJH,TomashekKM,DoddLE.Remdesivirforthetreat-ment of Covid-19—Preliminary Report. Reply. N Engl J Med.2020;383:994.
7. Spinner CD, Gottlieb RL, Criner GJ, et al. Effect of remde-sivirvs standardcareonclinical statusat11days inpatientswithmoderateCOVID-19:arandomizedclinical trial.JAMA.2020;324:1048-1057.
8. WangY,ZhangD,DuG,etal.RemdesivirinadultswithsevereCOVID-19: a randomised, double-blind, placebo-controlled,multicentretrial.Lancet.2020;395:1569-1578.
9. FDA.FDA’sapprovalofVeklury(remdesivir)forthetreatmentofCOVID-19—TheScienceofSafetyandEffectiveness.2020.https://www.fda.gov/drugs/drug-safety-and-availability/fdas-approval-veklury-remdesivir-treatment-covid-19-science-safety-and-effectiveness.AccessedDecember10,2020.
10. BeigelJH,TomashekKM,DoddLE,etal.Remdesivirforthetreat-mentofCovid-19—FinalReport.N Engl J Med.2020;383:1813-1826.
11. Lao KS, Chui CS, Man KK, Lau WC, Chan EW, Wong IC.Medicationsafetyresearchbyobservationalstudydesign.Int J Clin Pharm.2016;38:676-684.
12. LindquistM.VigiBase,theWHOglobalICSRdatabasesystem:basicfacts.Drug Inf J.2008;42:409-419.
13. SalemJE,ManouchehriA,BretagneM,etal.Cardiovasculartoxicities associated with ibrutinib. J Am Coll Cardiol.2019;74:1667-1678.
14. SalemJE,EderhyS,Lebrun-VignesB,MoslehiJJ.Cardiaceventsassociated with chimeric antigen receptorT-Cells (CAR-T): aVigiBaseperspective.J Am Coll Cardiol.2020;75:2521-2523.
15. SalemJE,ManouchehriA,MoeyM,etal.Cardiovasculartox-icitiesassociatedwithimmunecheckpointinhibitors:anobser-vational,retrospective,pharmacovigilancestudy.Lancet Oncol.2018;19:1579-1589.
16. SalemJE,YangT,MoslehiJJ,etal.Androgeniceffectsonven-tricularrepolarization:atranslationalstudyfromtheinterna-tional pharmacovigilance database to iPSC-cardiomyocytes.Circulation.2019;140:1070-1080.
17. WHO. Drug and Therapeutics Committee training course—Participants’ guide. 2008. https://www.who.int/medicines/technical_briefing/tbs/04-PG_Dug-Safety_final-08.pdf?ua=1.AccessedJuly22,2021.
18. Knight DS, KotechaT, RazviY, et al. COVID-19: Myocardialinjuryinsurvivors.Circulation.2020;142:1120-1122.
19. Giustino G, Croft LB, Stefanini GG, et al. Characterization ofmyocardialinjuryinpatientswithCOVID-19.J Am Coll Cardiol.2020;76:2043-2055.
20. Caster O, Aoki Y, Gattepaille LM, Grundmark B.Disproportionalityanalysisforpharmacovigilancesignaldetec-tioninsmalldatabasesorsubsets:recommendationsforlimit-ingfalse-positiveassociations.Drug Saf.2020;43:479-487.
21. Rothman KJ, Lanes S, Sacks ST. The reporting odds ratioand its advantages over the proportional reporting ratio.Pharmacoepidemiol Drug Saf.2004;13:519-523.
22. WHO Solidarity Trial Consortium, Pan H, Peto R,etal.RepurposedantiviraldrugsforCOVID-19—interimWHOSOLIDARITYtrialresults.N Engl J Med.2021;384:497-511.
23. RECOVERY Collaborative Group, Horby P, Lim WS, et al.DexamethasoneinhospitalizedpatientswithCovid-19—pre-liminaryreport.N Engl J Med.2021;384:693-704.
24. SinghAK,SinghA,SinghR,MisraA.RemdesivirinCOVID-19:A critical review of pharmacology, pre-clinical and clinicalstudies.Diabetes Metab Syndr.2020;14:641-648.
25. BateA,LindquistM,EdwardsIR,etal.ABayesianneuralnet-workmethodforadversedrugreactionsignalgeneration.Eur J Clin Pharm.1998;54:315-321.
26. Norén GN, Hopstadius J, Bate A. Shrinkage observed-to-expected ratios for robust and transparent large-scale patterndiscovery.Stat Methods Med Res.2013;22:57-69.
27. ChoiSW,ShinJS,ParkS-J,etal.AntiviralactivityandsafetyofremdesiviragainstSARS-CoV-2infectioninhumanpluripotentstemcell-derivedcardiomyocytes.Antiviral Res.2020;184:104955.
28. RochwergB,AgarwalA,ZengL,etal.Remdesivir for severecovid-19:aclinicalpracticeguideline.BMJ.2020;370:m2924.
29. RubinD,Chan-TackK,FarleyJ,SherwatA.FDAApprovalofremde-sivir-astepintherightdirection.N Engl J Med.2020;383:2598-2600.
30. Grein J, Ohmagari N, Shin D, et al. Compassionate use ofremdesivir for patients with severe Covid-19. N Eng J Med.2020;382:2327-2336.
31. GoldmanJD,LyeDCB,HuiDS,etal.Remdesivirfor5or10daysinpatientswithsevereCovid-19.N Engl J Med.2020;383:1827-1837.
32. EastmanRT,RothJS,BrimacombeKR,etal.Remdesivir:areviewofitsdiscoveryanddevelopmentleadingtoemergencyuseautho-rizationfortreatmentofCOVID-19.ACS Cent Sci.2020;6:672-683.
33. MadelainV,BaizeS,JacquotF,etal.Ebolaviraldynamicsinnonhuman primates provides insights into virus immuno-pathogenesisandantiviralstrategies.Nat Commun.2018;9:1-11.
34. WarrenTK,JordanR,LoMK,etal.TherapeuticefficacyofthesmallmoleculeGS-5734againstEbolavirusinrhesusmonkeys.Nature.2016;531:381-385.
35. VargaA,LionneC,RoyB.Intracellularmetabolismofnucleo-side/nucleotideanalogues:abottlenecktoreachactivedrugsonHIVreversetranscriptase.Curr Drug Metab.2016;17:237-252.
36. Cao B, Wang Y, Wen D, et al. A trial of lopinavir-ritonavirin adults hospitalized with severe Covid-19. N Engl J Med.2020;382:1787-1799.
37. DarazamIA,ShokouhiS,PourhoseingholiMA,etal.Roleofinterferon therapy in severe Covid-19: the COVIFERON ran-domizedcontrolledtrial.Sci Rep.2021;11:8059.
SUPPORTING INFORMATIONAdditional supporting information may be found in theonlineversionofthearticleatthepublisher’swebsite.
How to cite this article:JungSY,KimMS,LiH,etal.CardiovasculareventsandsafetyoutcomesassociatedwithremdesivirusingaWorldHealthOrganizationinternationalpharmacovigilancedatabase.Clin Transl Sci.2021;00:1–13.doi:10.1111/cts.13168







