
Challenges In Financing An Efficient Health Care System
“Health Sans Frontieres” European Health Forum, Gastein 2006
Armin FidlerSector Manager for Health, Nutrition, Population,
Europe and Central AsiaThe World Bank
2
Why Everyone Talks About Health Financing ….
• Health and Economics – Why the health sector takes center stage:– Efficiency of public spending: Health as a large public outlay– Social safety nets, poverty, catastrophic events:
• Poverty as a determinant and an outcome of ill health– Labor market implications: Health as an engine of economic
growth?• Health as a commodity and “luxury good”?
• Major Cost Drivers as experienced during the transition period in NMS– Hospital Infrastructure– Pharmaceuticals– Staff salaries, labor mobility– Medical Technology

3
How To Go About Containing Costs?
• “Control knobs” to modulate health expenditures – Supply side: Health Technology Assessment (HTA)
• Master Planning for Infrastructure and equipment
• Demographic, epidemiological, economic factors
– Demand side: Demand modulation• Co-payments
• OTC pharmaceuticals
• But also: “supply induced demand” – critical role of physicians and the availability of technology.
4
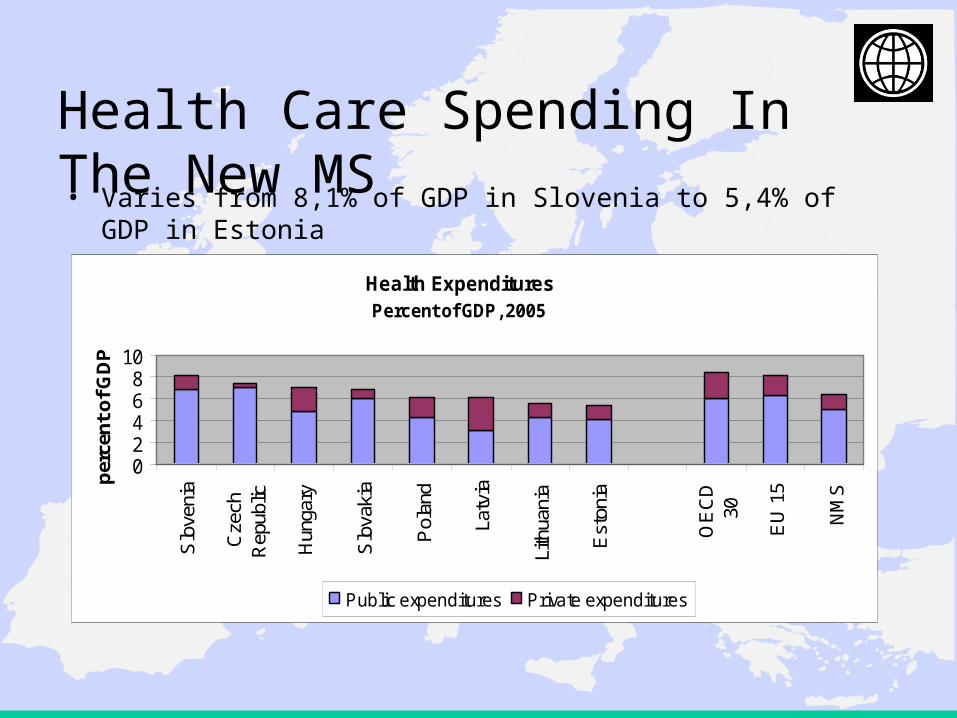
Health Care Spending In The New MS• Varies from 8,1% of GDP in Slovenia to 5,4% of GDP in Estonia
Health ExpendituresPercent of GDP, 2005
02468
10
Slo
veni
a
Cze
chR
epub
lic
Hun
gary
Slo
vaki
a
Pol
and
Latv
ia
Lith
uani
a
Est
onia
OE
CD
30
EU
15
NM
S
per
cen
t o
f G
DP
Public expenditures Private expenditures

5
Examples from the EU NMS
• Recent reforms: CZ, EE, H, LV, LT, PL, SK, SI (+RO, BG)
– carried out health sector reforms of variable scope – but no
discernable trend as far as directions and results.
• Health expenditures: not out of line compared to OECD, but
sector in debt where expenditures consistently exceed
revenues derived from payroll tax and budget allocations.
• Near term outlook: Drive for modernization, upgrading of
technology and legacy of past creates pressure on expenditures
and mandates to raise extra revenue and to contain costs.

6
Economic Growth: Strong growth has partially cushioned growth of health expenditures
Growth Rates, 2003-2005
02468
1012
2003 2004 2005
Source: Eurostat

7
Death Rates From Main Causes• Scope for reducing mortality?• Lifestyle – public health (primary+secondary prevention)• Role of investment in evidence-based treatment protocols and modern technology?
0200400600800
10001200
Cze
chR
epub
lic
Est
onia
Hun
gary
Latv
ia
Lith
uani
a
Pol
and
Slo
vaki
a
Slo
veni
a
EU
-15
aver
age
SD
R p
er 1
00,0
00
All Causes Circulatory System Cerebro-vascular
Source: WHO-EURO, HFA Database, 2005

8
30 Percent Of Population In NMS Above 65 Years Of Age By 2025
Broad Age Groups, Trends and Projections
-10
0
10
20
30
40
50
60
70
80
1995 2000 2005 2010 2015 2020 2025
Pop<15 Pop 15-64 Pop>60
9
Ageing And Changing Demographics• Difficult to quantify the impact that an ageing population
will have on health expenditures – Bulk of health expenditures will still occur in last year of life– But increased life expectancy despite multi-morbidity will take toll
• But there is little doubt that an increasing proportion of people over 65 will exert some upward pressures on health care costs
• A critical issue is long-term care for the very old, which can become a significant financial burden as informal family-based care begins to decline– Few NMS have drawn up credible long-term strategies for LTC– EHFG Session on Saturday, sponsored by EU and WB!
10
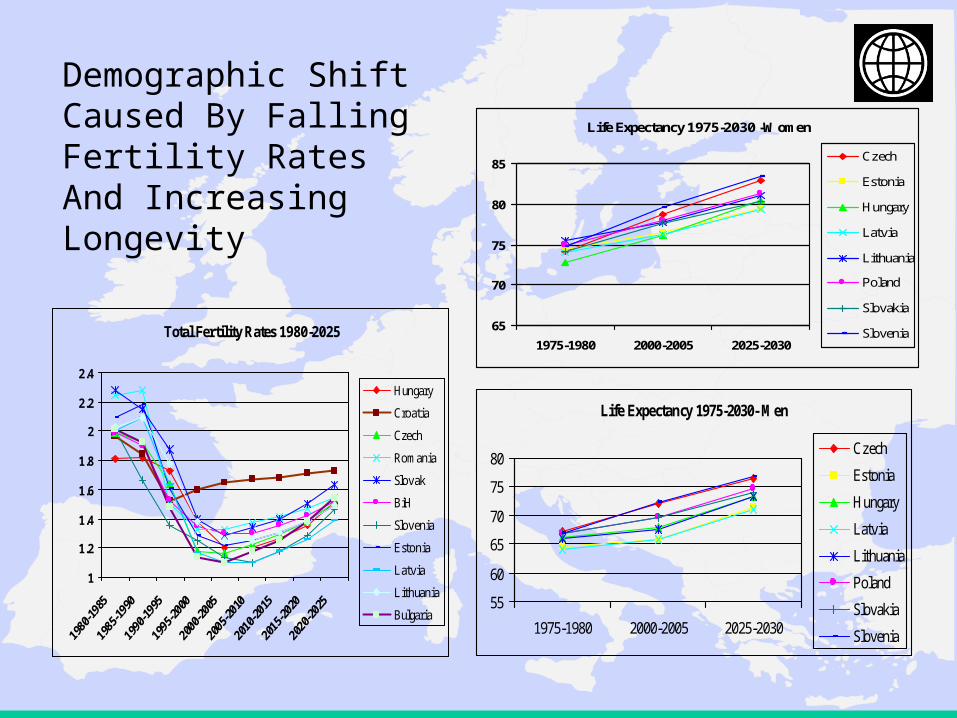
Demographic Shift Caused By Falling Fertility Rates And Increasing Longevity
Total Fertility Rates 1980-2025
1
1.2
1.4
1.6
1.8
2
2.2
2.4
Hungary
Croatia
Czech
Romania
Slovak
BiH
Slovenia
Estonia
Latvia
Lithuania
Bulgaria
Life Expectancy 1975-2030- Men
55
60
65
70
75
80
1975-1980 2000-2005 2025-2030
Czech
Estonia
Hungary
Latvia
Lithuania
Poland
Slovakia
Slovenia
Life Expectancy 1975-2030 -Women
65
70
75
80
85
1975-1980 2000-2005 2025-2030
Czech
Estonia
Hungary
Latvia
Lithuania
Poland
Slovakia
Slovenia

11
Principle Challenges for a Sustainable Health Financing System
(i) Hospital Infrastructure
(ii) Pharmaceuticals
(iii) Staff salaries
(iv) Medical Technology
12
(i) Hospital Infrastructure• Extensive hospital infrastructures expensive to maintain
– many structures not appropriate (location, use , size)
• Oversupply of hospital infrastructure in NMS is a historic legacy –
– but also highly prevalent in OECD
• Almost all countries have taken steps to reduce hospitals and
acute-care hospital beds
– but there are only few success stories.
• The problem of debts and contingent liabilities in countries with
dominant public hospital sector

13
(ii) Pharmaceuticals
• Drugs and medical devices seem to be the single largest cost drivers in most countries
• Rx total cost = Price x Volume• Questions related to:
– Extent of publicly financed benefit vs. OTC– Role of co-payments to control prescription and
consumption– Clinical practice guidelines and prescription practices based
on evidence– HTA and pharmaco-economics

14
(iii) Human Resources - Wages• Salaries account for more than 50 - 60% of health expenditures in most
countries, this trend is increasing the pressure on overall health spending
• The pressure on salaries has increased in EU NMS
– Health sector salaries in NMS rise faster then the average salaries in the economy
– from low starting point
• Example: Lithuania
70% of medical staff leaving Lithuania indicates “higher salaries” in the target
country as reason for leaving, 50% leaves because of the “higher living
standard” and 40% because of “better career possibilities”.
15
(iv) Medical Technology
• Absorption of available and new technologies puts pressure on health expenditures
• Modern health care is most information and technology-intense industry – difficult to saturate!– ECA countries – transformation from pre-transition
production model to modern health delivery system – not fully concluded yet, despite 15 years of reform and investments
– Therefore much room for either big mistakes and “dead ends” but also opportunities to leapfrog to leadership position – avoiding mistakes of others.
16
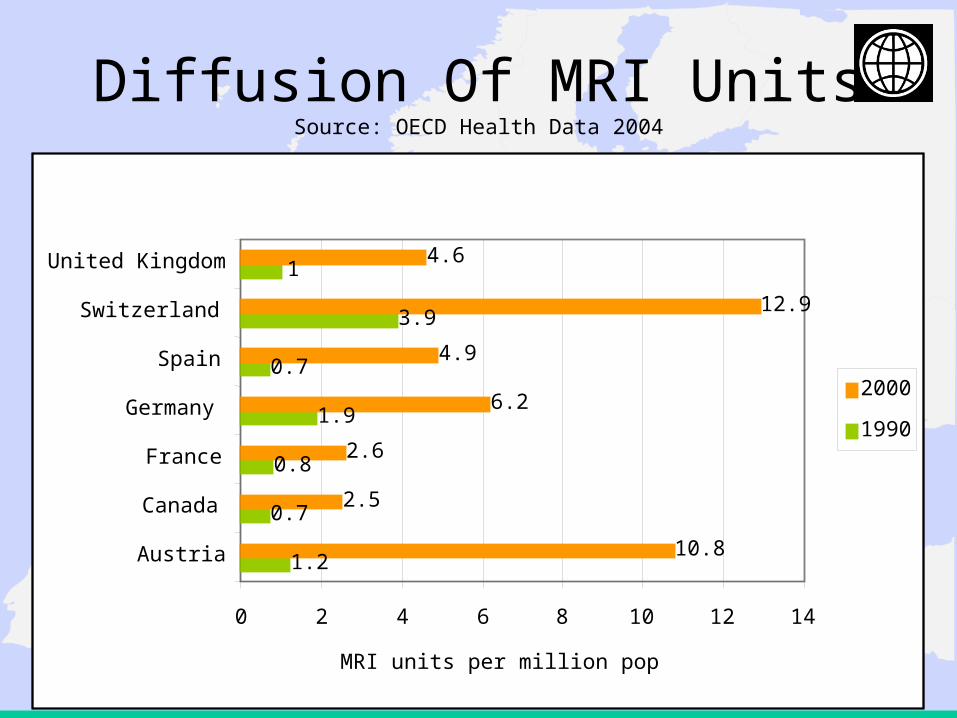
Diffusion Of MRI UnitsSource: OECD Health Data 2004
1.2
0.7
0.8
1.9
0.7
3.9
1
10.8
2.5
2.6
6.2
4.9
12.9
4.6
0 2 4 6 8 10 12 14
Austria
Canada
France
Germany
Spain
Switzerland
United Kingdom
MRI units per million pop
2000
1990
17
Health Technology Assessment (HTA)
• “policy research that systematically examines short- and long-term consequences of health and resource use, of the application of a health technology, a set of related technologies or a technology related issue”
• “a bridge between the world of research and the world of decision-making”
• Together with evidence-based medicine (EBM) and clinical practice guidelines (CPG) it builds a body of best practice initiatives
– Session on HTA and Quality of Care (Jan Bultman, WB) at EHFG
18
Objectives Of HTA
• Assist decision makers in deciding which technologies to adopt (C-E, certificate of use, etc.)
• Encourage the appropriate use of health technology, based on established evidence
• Provide impartial comprehensive information through the collection and analysis of information concerning the effectiveness and cost of health technology and health impact

19
Evidence When HTA Used Effectively
• Provides information from an independent, impartial perspective
• Supports and assists decision makers in making informed policies and decisions in health care
• Is an essential element of a health care system that seriously
• Creates a bridge between researchers, decision-makers, health care providers and the public
• Leverages health research investment in order to create a cost-effective health care system
20
Health Sector Modernization – Recalibration of Financing And...
• MoH stewardship – intergovernmental action (MOF – HIF)- Final goal must be population health outcomes - Payer could efficiently purchase “wrong” health service!
• MOF – HIF: Difficulty in many countries to sustainably raise revenues for health:
• informal sector, evasion of tax liability, unfunded mandates, HIF mandates
• Insurance and payment reform- Share of public vs. private and experimenting with different
models (Single payer, earmarked taxes, MSAs, regional funds, etc)• Human Resources critical for the entire system:
- Need to focus on evidence-based medicine and public health, management + economics)
• Information Technologies- Most critical for payers and providers, but most difficult to
procure and run effectively – constant source of corruption scandals







