Chapter 9: Communication & Collaboration in Nursing
Bonnie M. Wivell, MS, RN, CNS
Therapeutic Use of Self
Hildegard Peplau was first to focus on nurse-patient relationships, Interpersonal Relations in Nursing (1952)
Therapeutic use of self: forming a trusting relationship that provides comfort, safety, and nonjudgmental acceptance of patients to help them improve their health status.
It calls for self-awareness & use of effective communication techniques.
Communication skills can be developed
Traditional Nurse-Patient Relationship Orientation phase
“Getting to know you” Nurse and patient assess one another Early impressions are important Pt. should learn RN name, credentials, responsibility Beginning development of trust
Admit what you don’t know, but find out the answers Develop an initial understanding of patient problem/needs
Tasks of this phase Pt. will have enough trust to participate in relationship RN and pt. see each other as unique individuals & worthy
of respect, Set goals and identify problems (contract –
formal/informal)

Traditional Nurse-Patient Relationship Working phase
Tasks/goals worked on Pt. may alternate with periods of intense effort and
resistance to change Nurse must be patient, listen to patient’s feelings/needs
Termination phase End relationship Feelings of loss for both discussed Gifts & continued contact should be avoided (not a
social relationship)
Role of Self-awareness Important to be aware of own feelings, stereotypes,
blind spots, & biases—may interfere with nonjudgmental acceptance
Guard against nurse need to be liked/needed—get own emotional needs met outside of nurse-patient relationship.
Not all patients like their nurse & not all nurses like their patients
Not all patients share nurse’s beliefs, values, ethics Self-awareness keeps nurse non-judgmental , avoid
stereotyping, build a therapeutic relationship
Professional Boundaries Professional boundaries: “the space between
the nurse’s power and the client’s vulnerability.”
Nurse responsible for delineating & maintaining boundaries; nurse-client relationship does not meet needs of nurse; no post-termination relationships; no social relationships
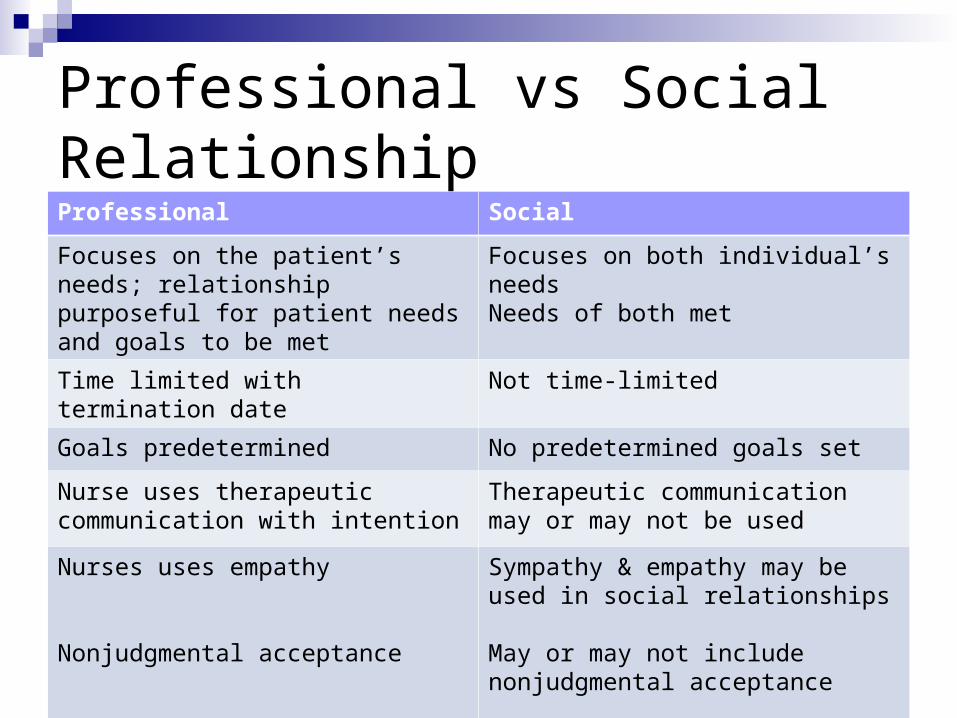
Professional vs Social RelationshipProfessional Social
Focuses on the patient’s needs; relationship purposeful for patient needs and goals to be met
Focuses on both individual’s needsNeeds of both met
Time limited with termination date Not time-limited
Goals predetermined No predetermined goals set
Nurse uses therapeutic communication with intention
Therapeutic communication may or may not be used
Nurses uses empathy
Nonjudgmental acceptance
Sympathy & empathy may be used in social relationships
May or may not include nonjudgmental acceptance

Principles for DeterminingProfessional Boundaries Nurse responsible to delineate boundaries Nurse work within “zone of helpfulness” Nurse examine any boundary crossing, aware of implications;
avoid repeated crossing Variables that impact: setting; community; client needs; nature
of therapy Actions that meet nurse’s needs overstep boundaries and are
boundary violations Avoid dual relationships of both personal & business Post-termination relationships complex as client may need
additional services & difficult to determine when relationship terminated

Reflective Practice
Patients’ values, beliefs and lifestyles may challenge the nurses’ own
Can produce discomfort as nurses become aware of the tensions and anxieties
Are your personal values challenged by the realities of practice?
Time to reflect on experiences and interactions allows us the ability to develop insight into self
Re-conceptualizing the Nurse-Patient Relationship Assumptions of the Nurse-Patient relationship
which no longer hold true It is linear and proceeds through several phases,
each building on the preceding one Building trust is essential during early phases of the
relationship Time and repeated contacts are required to establish
an effective relationship Patients desire relationships with nurses, wish to
receive services from them, and will cooperate and comply with those nurses.
Theory of Human Relatedness
Approach each nurse-patient contact as an opportunity for connection and goal achievement rather than as one step in a lengthy relationship-building process
Approach the patients with a sense of the patient’s autonomy, choice and participation
Put relationship on equitable ground – nurse doesn’t need to have the power
Communication
Exchange of thoughts, ideas, or information and is basis of relationships—dynamic
Verbal (speech) and nonverbal (gestures, tone & volume of voice, posture, actions, facial expressions) Do these match—congruent?
Ruesch’s major elements: sender, message, receiver, feedback, context.
Operations: Perception (interpretation of incoming signal into meaning), evaluation (analysis of information ), transmission (expression of information—verbal/nonverbal)
Influences: gender, culture, interests & mood, clarity, length
How Communication Develops Infants use SOMATIC language = crying; reddening of
the skin; fast, shallow breathing; facial expressions; and jerking of the limbs Decreases with maturity
ACTION language consists of reaching out, pointing, crawling toward a desired object, or closing the lips and turning the head when an undesired food is offered
VERBAL language is last to develop Amount of stimuli can enhance or retard development of
language skills Development of communication is determined by inborn
and environmental factors Nonverbal communication development is influenced by
environment
Successful Communication
Feedback: giving back information to sender
Appropriateness: reply fits circumstances
Efficiency: simple, clear words paced suitably
Flexibility: base message on immediate situation rather than on preconceived notion
Becoming a Better Communicator Active listening: communicating interest and
attention Eye contact Nod, mumble, encourage continuation Open posture Pay attention, focus on patient not the task Reflect feelings, meaning Allow patients to vent concerns or frustrations
3 faults: interrupting, finishing sentences for others, lack of interest
You can become a better communicator with conscious practice and awareness
Helpful Response Techniques
Empathy: awareness, sensitivity to, and identify with feelings of another (Sympathy shares feelings of another)
Open-ended questions: require more than yes or no answers. “Tell me about…..”
Giving information: sharing knowledge recipient not expected to know; don’t share your opinion
Reflection: encourages patient to think through problems for themselves
Silence: allows time for reflection & thinking; be with your patient

Blocks to Communication
Failing to see each individual as unique: stereotyping; preconceived ideas; prejudices
Failing to recognize levels of meaning: verbal cues
Using value statements and clichés Using false reassurance: “It will be alright.” Failing to clarify
Holistic Communication “The art of sharing emotional and factual
information. It involves letting go of judgments and appreciating the patient’s point of view.”
Speeds healing Decreases anxiety Pts complain less Call for attention less often Feel understood and valued More likely to comply with treatment plan

Communication in Workplace
Use same communication skills with colleague Face to face communication best, important Use of e-mail lacks facial expression, tone of
voice, and contextual cues—no non-verbal Be courteous, give full attention, no cell phone
use while speaking with others Avoid jargon, acronyms, abbreviations Keep short & purposeful: SBAR Receiving messages—read, listen, and evaluate
entire message before responding.

Multicultural Workplace Diversity in age, race, gender, ethnicity, country
of origin, sexual orientation, and disability is present
Culture is the lens through which all other aspects of life are viewed
Culture determines one’s health beliefs and practices
Strategies on page 229 of text Use clear, simple messages and clarify intent TRUST must exist for communication to be
effective

Collaboration
Implies working jointly with other professionals, all of whom are respected for their unique knowledge and abilities, to improve a patient’s health status or to solve an organizational problem.

Collaboration with Co-workers
Acknowledgement of cultural diversity Respect for each other & difference in opinion Emotional maturity Confidence in own knowledge; know limits Willingness to learn Cooperative spirit Belief in common purpose Willingness to negotiate Acknowledge conflict and solve problems
Organizational Collaboration
Flat organizational structure Encouragement and support of individuals to
act autonomously Recognition of team accomplishments Cooperation Valuing of knowledge and expertise Support equality and interdependence Creativity and shared vision are valued
RN-MD Collaboration
Gender differences Care-cure conflict Emotionally-based conflicts are
attributable to relationships Task-based conflicts are a result of
differences of opinion over how to approach a task or achieve a mutual goal

Collaboration with Assistive Personnel Assistive personnel need to feel welcome,
appreciated, and respected RNs need to feel competent as managers
of pt. care and have unlicensed personnel comply with requests and give feedback about assigned activities
Mutual respect and understanding
Important to Patient Care
Positive relationships have a positive impact on patient care
Relationship based care includes relationships with: Patient/family Self Colleagues
Effective communication skills practiced and intentionally used, and communication blocks avoided, improve relationships

Chapter 10: Illness, Culture, & Caring: Impact on Patients, Families, & Nurses
Bonnie M. Wivell, MS, RN, CNS

Illness Illness is a highly personal experience Disease is an alteration at the tissue/organ level
causing reduced capacities or reduction of normal life span
One may feel ill in the absence of disease Patient’s perceptions of change in body image
or loss of function/body part play a role in whether they see themselves as ill
Illness is experienced differently by individuals and their families
Culture determines how individuals and families react to illness

Acute vs Chronic Illness Acute: characterized by severe symptoms that
are relatively short-lived, appear suddenly, progress steadily & subside; may not require medical attention; acute illness can lead to chronic illness, i.e. MI → CHF
Chronic: usually develops gradually, requires ongoing medical attention, and may continue for duration of person’s life. Are caused by permanent changes that leave residual disability.
Remission: when symptoms subside Exacerbation: when symptoms reappear or
worsen
Stages of Adjustment to Illness Stage I: Disbelief & Denial Stage II: Irritability & Anger Stage III: Attempting to gain control Stage IV: Depression & Despair Stage V: Acceptance & Participation Not all go through every stage and may
not go through them at same rate or in same order

The Sick Role Children learn sick role through parental
modeling Culture determines certain criteria for “sick” Sick role for Anglo-Americans (Parsons, 1964)
Exempt from social responsibilities Cannot expect to care for self Should want to get well Should seek medical advice Should cooperate with medical experts
Current expectation is person accepts responsibility for their own care & want to get well; Healthy behavior encouraged. If don’t cooperate labeled ”noncompliant”.

Illness Behaviors Internal influences: personality
Dependence/independence needs Coping: ability to assess and manage demands Hardiness: resistance to stressful life events Learned resourcefulness: promoting adaptive, healthy
lifestyles Resilience: pattern of successful adaptation despite
challenging or threatening circumstances Disposition: personality, health, cognition Family factors: warmth, support, organization Outside support: supportive network and success at
school or work Spirituality: inner strength related to belief in a higher
power

Spirituality Occurs over lifetime & internal process Role in health care being researched Benson & Stark(1996) Prayer for relaxation Spiritual nursing goes beyond chaplain Holistic nursing: physical, psychological, social,
& spiritual NANDA nursing diagnosis of spiritual distress:
“disturbance in belief or value system that provides strength, hope, & meaning to life.”

Illness Behaviors External influences:
Past experiences Culture: pattern of learned behavior and values that
are reinforced Communication patterns strongly influenced by culture (i.e.
nodding head to be polite not in understanding) Personal space norms depend on cultural experience (i.e.
touching can be major form of communication or be considered disrespectful)
Role expectations: nurse being passive vs authoritarian Values of nurse may conflict with pt’s cultural values (ex.
pain management) Ethnocentrism: to view one’s own cultural group as superior
to others

History of Cultural Competence Early 1970s: SONs began including cultural
concepts 1981: Transcultural Nursing Society
incorporated 1988: Certification began 1989: Journal of Transcultural Nursing published Dr. Madeleine Leininger, Founder of
Transcultural Nursing

Cultural Considerations Cultural competence: nurse’s knowledge of
cultural influences that affect a pt’s response to healthcare and interventions
Consider culture including health and religious beliefs in providing culturally sensitive care
Avoid stereotyping—one size does not fit all Cultural conditioning: Culture-bound;
unconscious of own innate values/beliefs and assume all are alike Personal Space Role Expectations

Cultural Considerations Cont’d.
Ethnopharmacology = understanding responses to prescribed meds and genetic variations in responses to drugs
Ethnocentrism = the inclination to view one’s own cultural groups as superior to others and to view differences negatively
Cultural assessment: “merely asking people their preferences, what they think, who we should talk to in making a decision.”
Impact of Illness on Patient
Behavioral & emotional changes Changes in patient role within family Disturbance of family dynamics Severe illness may affect physical
appearance & functioning Emotions of guilt, anger, anxiety
Impact of Illness on Family
Acute and chronic illness changes family functioning
Feelings experienced go up & down Sometimes family members withdraw from each
other—fear feelings may not be okay Family members uncertain how to treat & relate
to sick member Shift of responsibilities within family

Anxiety Definition: Response to some real or
perceived threat Symptoms:
Physical: Increase HR, BP, Respirations, insomnia, N/V, fatigue, sweaty, tremors
Emotional: restlessness, irritable, feelings of helplessness, crying & depression
Cognitive: inability to concentrate, forgetfulness, inattention to surroundings & preoccupation

Anxiety Levels Mild: Increased alertness & ability to focus,
improved concentration, expanded learning Moderate: Concentration limited to one thing,
including body movements, rapid speech, subjective awareness of discomfort
Severe Anxiety: Thoughts scattered, verbal communication difficult, discomfort, purposeless movements
Panic: Disorganized, difficulty distinguishing real from unreal, random movements, unable to function without assistance

Stress Definition: response of interaction between the individual
and environment—includes all responses body makes to maintain equilibrium & deal with demands
Plays a major role in the development of illness PUD HTN Autoimmune disorders Reduces immune response resulting in delayed healing and
greater susceptibility to infection such as cold or flu Evaluate lifestyles—triggers; individual perception;
capable of handling/coping? Relaxation techniques
Impact of Anxiety & Stress Nurse should consider impact of client’s
anxiety/stress levels when providing care. What other emotions may be involved? Today’s reduced hospital stays increases
need for client/family to learn needed care How will anxiety/stress impact learning? These & what other things reduce the
client/family’s ability to learn that impacts the client’s hospitalization and outcome?

Barriers to Learning1. High Anxiety2. Sensory deficits (vision, hearing)3. Pain4. Fatigue5. Hunger/thirst6. Language differences7. Differing health values8. Low literacy9. Lack of motivation10. Environmental factors (noise, lack of privacy)

Principles of Adult Learning Prior experiences resources for learning Readiness to learn r/t social or dev. task Motivation to learn greater if immediately
useful—what does client want/need to learn?
Arrange learning environment to facilitate learning Meet physical needs before teaching
session

Teaching Tips Identify and remove barriers to learning Evaluate what already know Short frequent sessions better than long Realistic goals set with patient Respect cultural implications Avoid medical jargon Move from simple to complex Actively engage patient in learning Use multiple senses: see, hear, tell, watch, do Give feedback: positive and what to do better Written materials at 5th grade level & in patient language Evaluate pt understanding & clarify misunderstanding

Compassion Fatigue
Nurses often report that the needs of patients and families, as well as their own spouses and children, take priority over their own needs
The nurse is then left feeling stretched, overwhelmed, frustrated, unappreciated, and resentful
Negative feelings interfere with the ability to maintain a caring attitude and drain caring out of our interactions with others
Nurse Caring for Self Jean Watson: “caring the essence of nursing
practice” “Caregivers who are filled with stress &
negativity cannot provide an atmosphere conducive to healing.”
Choose a facility that supports caring and professional nursing practice – Magnet facilities
Important to develop a balanced life Create a balanced life care plan for yourself –
see page 266 of text

Self-Learning
Please read The Introduction and Chapter 1 of Relationship Based Care A Caring and Healing Environment







