Slide 1
Christopher Robbins
BSN, RN, CGRN
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 2
I have nothing to disclose.
___________________________________
___________________________________
___________________________________
___________________________________
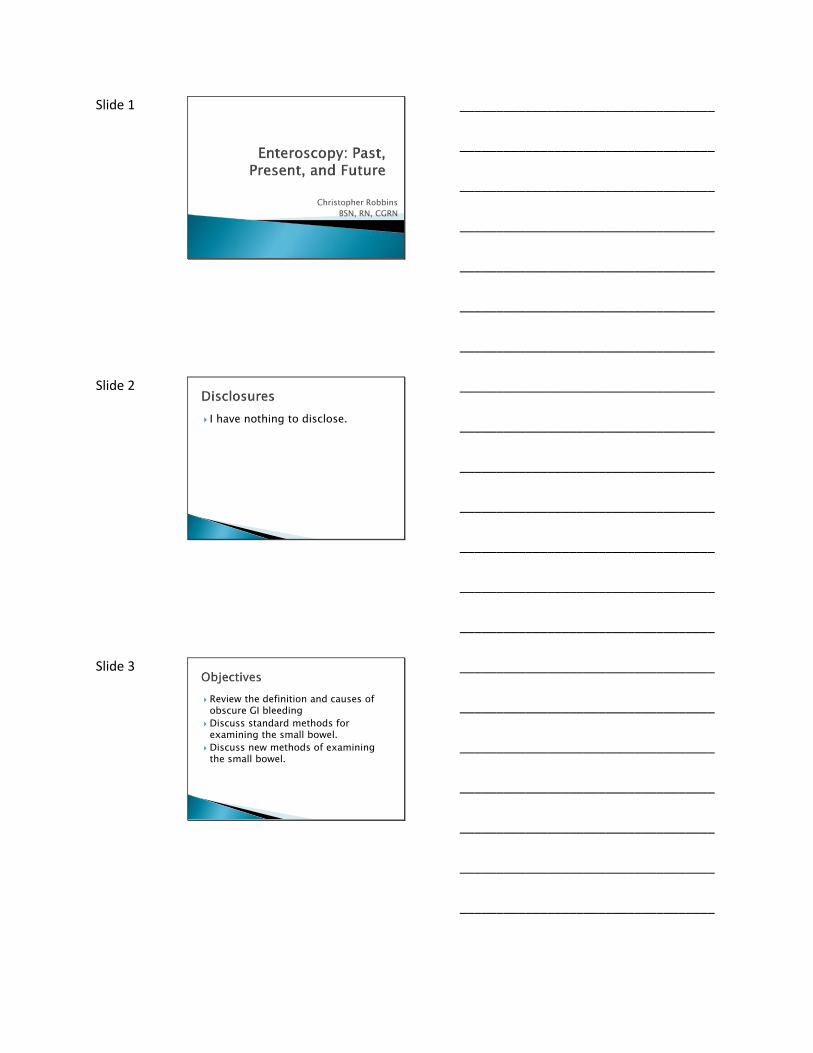
___________________________________
___________________________________
___________________________________
Slide 3
Review the definition and causes of obscure GI bleeding
Discuss standard methods for examining the small bowel.
Discuss new methods of examining the small bowel.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 4
Upper GI Bleeding◦ Proximal to papilla
Mid-gut (SB bleeding)◦ From second portion of duodenum to the terminal
ileum
Lower GI Bleeding◦ Colonic
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 5
Obscure GI bleeding (OGIB) has been defined as bleeding of unknown origin that persists or recurs after an initial negative endoscopic evaluation, including colonoscopy and/or upper endoscopy (EGD).
5-10% of all GI bleeding events
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 6
2.7 years
> 7 diagnostic tests
> 5 Hospitalizations
20-40 transfusions
Foutch et al. – GI Endo ‘90; Flickinger et al. – Am J Surg ‘89; Goldfarb et al. – Dis Manage ‘02
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 7
Patient < 40 Patient > 40
Tumors *
Meckel’s Diverticulum
Dieulafoy*
Crohn’s disease
Celiac disease *
Vascular malformations
Angioectasias Dieulafoy* NSAIDs Celiac disease* Tumors (lymphoma)* Crohn’s disease
Raju et al. – Gastro ‘07
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 8
• Meckel’s diverticulum> Remnant of vitelline duct in distal
ileum
> Prevalence of 1 – 3%
> Most common cause of small bowel bleeding in patients under the age of 25
> Ectopic gastric tissue causes ulceration
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 9
Large, tortuous submucosalarteriole
Bleeds through a mucosal defect
75% in stomach
14% in duodenum
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 10
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 11
Hemobilia
Hemosuccus pancreaticus
Aorto-enteric fistula
Ectopic varices
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 12
Hemobilia◦ Neoplasm, vascular aneurysm,
liver abscess, trauma, liver biopsy
Hemosuccus pancreaticus◦ Pancreatic pseudocysts,
pancreatitis, neoplasms
◦ Erosion into a vessel with communication with PD
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 13 Aorto-Enteric Fistula
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 14
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 15
Upper GI Lower GI
Cameron’s ulcers
Gastric varices
PUD
GAVE
Agioectasias Neoplasms
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 16
After APC
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
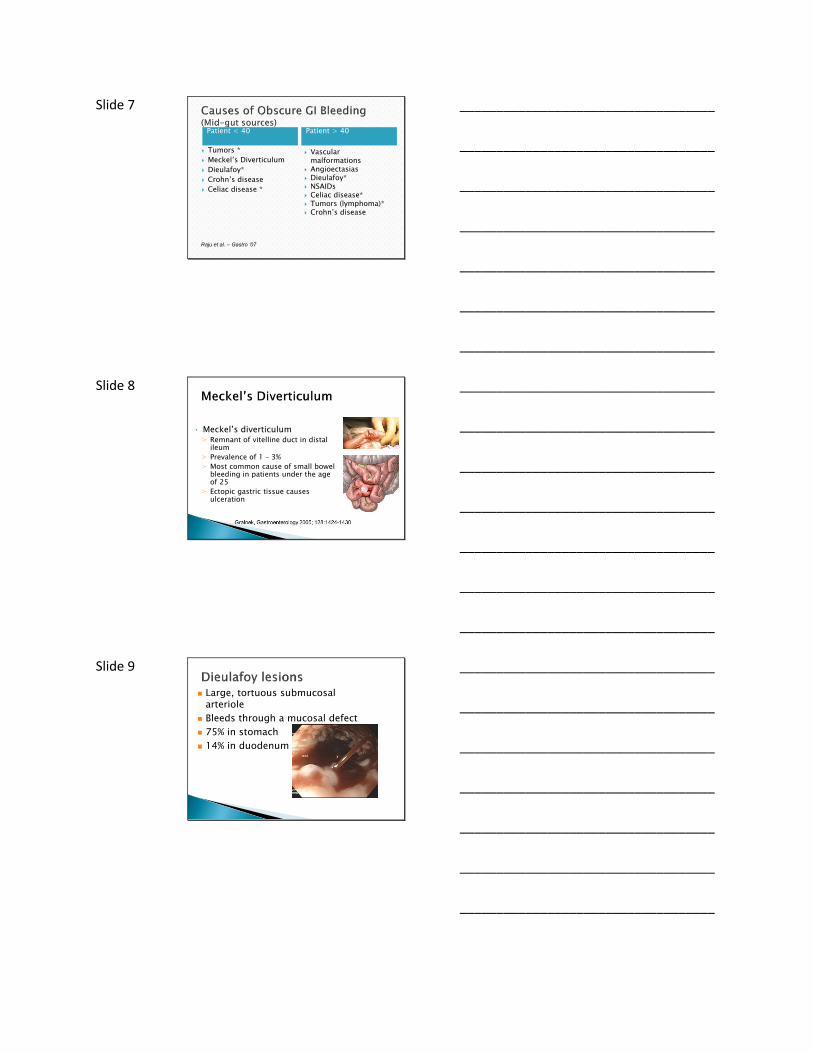
Slide 17
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
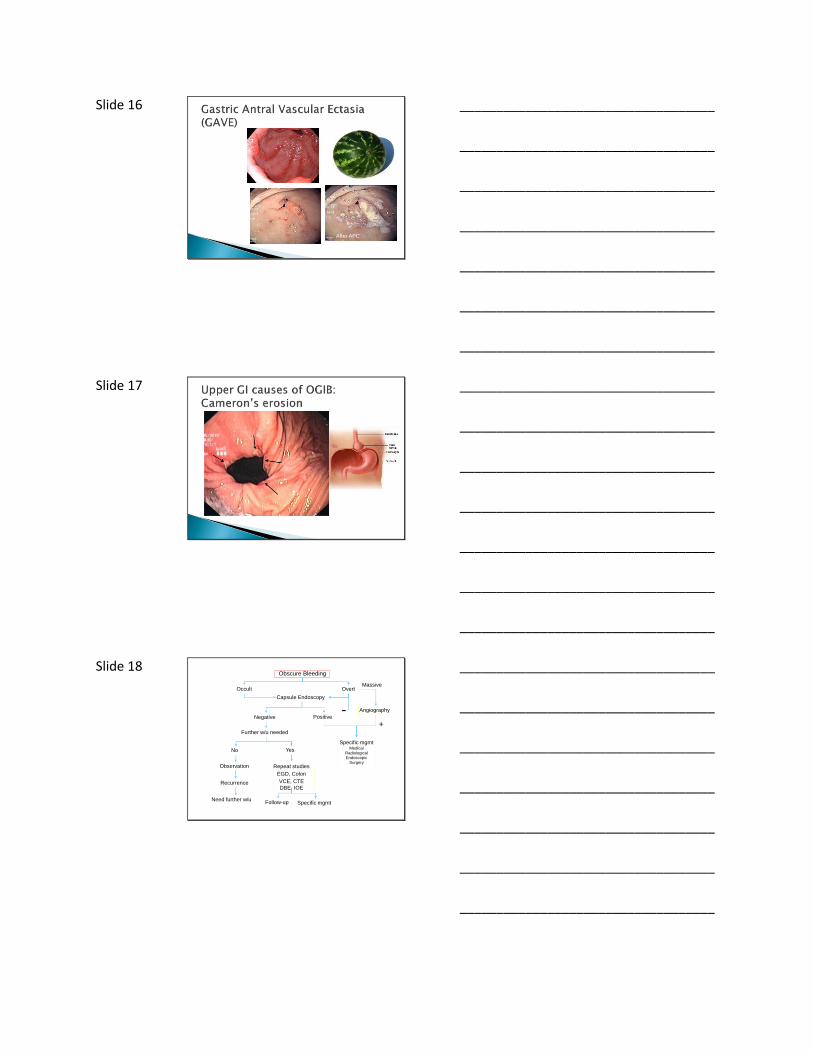
Slide 18 Obscure Bleeding
Occult Overt
Capsule Endoscopy
Massive
+Further w/u needed
Specific mgmtMedical
RadiologicalEndoscopic
Surgery
Angiography
Observation Repeat studies
EGD, Colon
VCE, CTE
DBE, IOERecurrence
Need further w/uFollow-up Specific mgmt
Negative Positive
YesNo
-
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 19
VCE First◦ Very good screening test
◦ Helps to determine further testing
Push enteroscopy
Deep enteroscopy
Surgery
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 20
Visualizes all GI Tract
Non Invasive
Good yield
+/- Specificity
VCE
Raju et al. – Gastro ‘07
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 21
Propelled via peristalsis
Captures ~ 60,000 images
Ambulatory office procedure
Naturally excreted
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 22
1. Optical dome2. Lens holder3. Lens4. LEDs
(Light Source)5. Electronic Chip
converts Images to Radio Waves
6. (2) Battery7. Electronic
transmitter8. Antenna
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 23
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 24
Pennazio M, Santucci R, Rondonotti E, et al. Gastroenterology 2004; 126: 643-653
82.6 %Negative predictive
value
97.0 %Positive predictive
value
95.0 %Specificity
88.9 %Sensitivity
(Analysis of patients with verified final diagnosis, n = 56)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 25
Time efficient, patient friendly, sensitive method to visualize the small bowel
Disadvantages ◦ No therapeutics
◦ Unable to control movement
◦ Unable to clear bubbles and debris
ASGE
March 15, 2013
Oak Brook, IL
Capsule Endoscopy User’s Course
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 26
Very low yield
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 27
Time consuming
Diagnostic yield in average OGIB is ~25%
Location accuracy of bleed is ~30-50% of the time
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 28 Infuse technetium-labeled RBC’s
Nuclear imaging obtained over 60 – 90 min
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 29
Yield is ~ 25-30%
Good for bleeding and non-bleeding AVM’s
Bloomfeld et al. – Am J Gastro ‘00
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 30
Active bleeding Coil embolization Post treatment
Kobayashi J Surg Rad 2011 Jan 1; 2 (1)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 31
Contrast injected into small bowel
X-rays obtained
Improved yield over small bowel series
Yield is poor:◦ 10%-25%
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 32
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
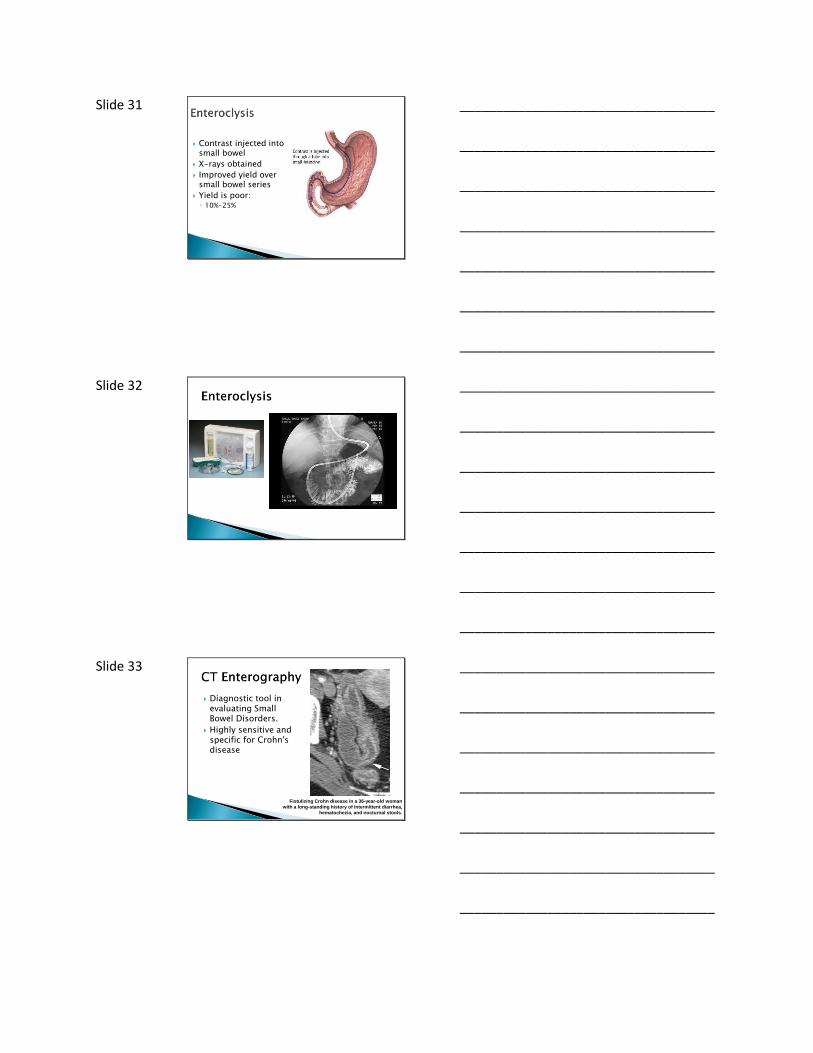
Slide 33
Diagnostic tool in evaluating Small Bowel Disorders.
Highly sensitive and specific for Crohn'sdisease
Fistulizing Crohn disease in a 36-year-old woman
with a long-standing history of intermittent diarrhea,
hematochezia, and nocturnal stools.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 34
Visualized to Proximal SB
Invasive
Yield is fair (operator dependent)
Very specific
Average + yield ~35%
Better yield in overt bleeding and AVM’s
Push Enteroscopy
Raju et al. – Gastro ‘07
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 35
Double-balloon Enteroscopy (2001)
Single-balloon Enteroscopy (2007)
Rotational Enteroscopy (2006)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 36
Three divisions Duodenum Jejunum Ileum
Average length ~ 22 feet or 670 cm
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
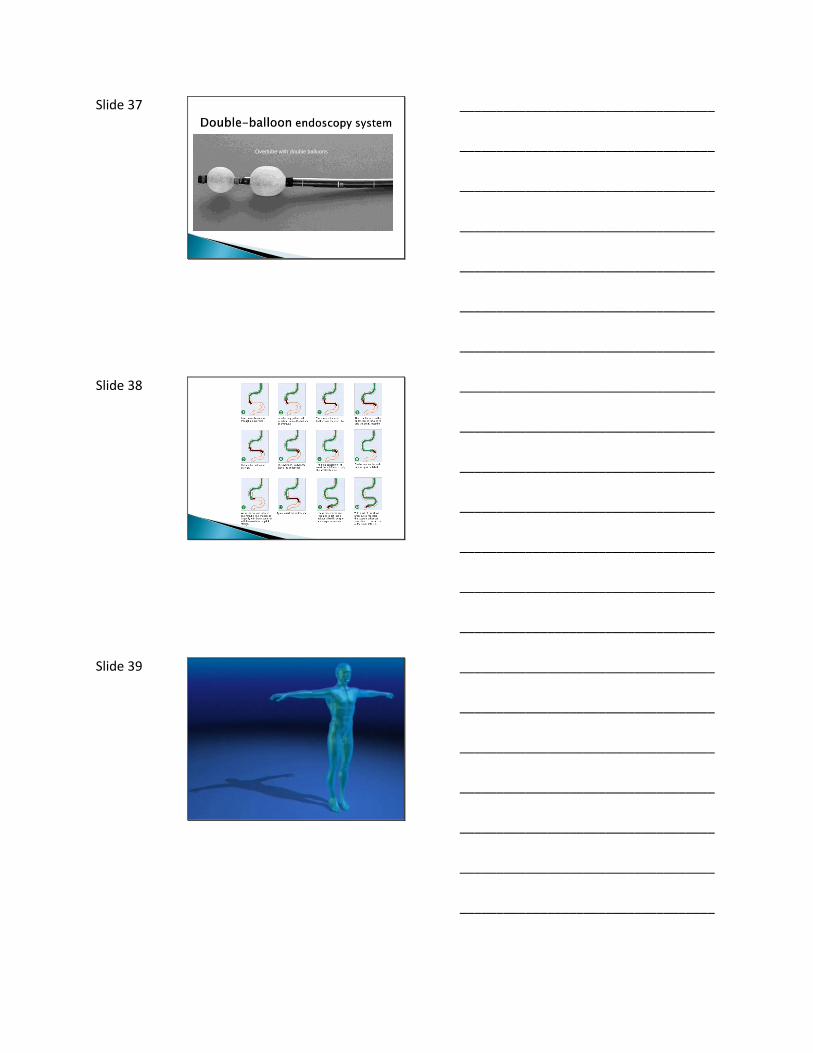
Slide 37
Overtube with double balloons
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 38
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 39
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 40
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 41
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 42
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 43
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 44
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 45
Rotational Enteroscopy usually requires < 15 minutes to reach maximum depth
Physicians report easier controlled withdrawal compared to balloon endoscopy
Scope removal without position loss
Procedures are well tolerated with few reported complications
The short time required allows for upper and lower exams in the same setting
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 46
Avg. Time to Max. Depth 25 minutes
Avg. Total Procedure Time 45 minutes (all procedures)
35 minutes (diagnostic without therapy)
Avg. Depth 247 cm
65% Diagnostic Yield
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 47
Comparative Performance
DeviceAverage Procedure
TimeDepth Therapy Source
Rotational Enteroscopy
45 min 250 Yes National Independent Study 2008
Double Balloon
73 min 233 YesASGE Technology Status Report-
Enteroscopes: 2007
Single Balloon 77 min 239 YesMeta-analysis of 5 published studies
2007-2008
Pill Camera8 hrs. to record
30-120 min. to readAll No
ASGE Technology Status Report –Wireless Capsule: 2006
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 48
Rotational Enteroscopyhelps facilitate deep enteroscopy and ERCP in altered anatomy patients◦ Roux-en-Y
Aids insertion
Provides high level of control and stabilization
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
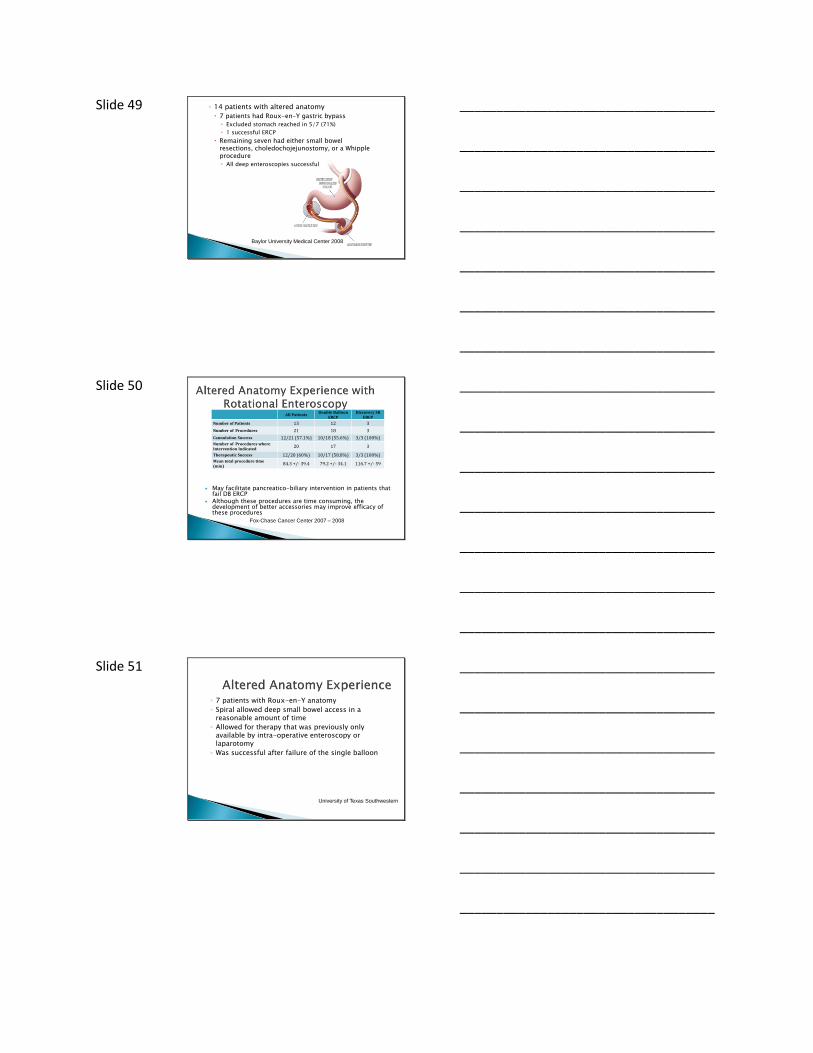
Slide 49 ◦ 14 patients with altered anatomy
7 patients had Roux-en-Y gastric bypass
Excluded stomach reached in 5/7 (71%)
1 successful ERCP
Remaining seven had either small bowel resections, choledochojejunostomy, or a Whipple procedure
All deep enteroscopies successful
Baylor University Medical Center 2008
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 50
All PatientsDouble Balloon
ERCPDiscovery SB
ERCP
Number of Patients 13 12 3
Number of Procedures 21 18 3
Cannulation Success 12/21 (57.1%) 10/18 (55.6%) 3/3 (100%)Number of Procedures where Intervention Indicated
20 17 3
Therapeutic Success 12/20 (60%) 10/17 (58.8%) 3/3 (100%)Mean total procedure time (min)
84.3 +/- 39.4 79.2 +/- 34.1 116.7 +/- 59
May facilitate pancreatico-biliary intervention in patients that fail DB ERCP
Although these procedures are time consuming, the development of better accessories may improve efficacy of these procedures
Fox-Chase Cancer Center 2007 – 2008
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 51
◦ 7 patients with Roux-en-Y anatomy
◦ Spiral allowed deep small bowel access in a reasonable amount of time
◦ Allowed for therapy that was previously only available by intra-operative enteroscopy or laparotomy
◦ Was successful after failure of the single balloon
University of Texas Southwestern
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 52
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 53
Fits over standard endoscopes and pediatric colonoscopes◦ 11.1mm-11.6mm OD
100cm overall length / 18mm OD
5.5mm spiral height
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 54
Aids insertion & advancement of the endoscope and helps reduce the colon.
Allows scope to be pushed into the ileum while stabilizing the colon.
Standard reduction maneuvers are performed to inspect the ileum.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 55
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 56
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 57
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 58
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 59
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 60
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________







