
Clinical and immuno-pathologicalaspects of Chikungunya infection
“Immunopathology & intervention strategies” Panel
Marc LECUIT, MD PhDInstitut Pasteur, Inserm
Necker Hospital, Paris Descartes University
This presentation has been edited and unpublished results have been deleted

Immunopathology and intervention strategies
• How does CHIKV cause disease?
• What is known about the immunological responses andpathophysiological events of CHIK in the human host ?
• What approaches are being pursued in terms ofdevelopment of therapeutics as anti-virals or vaccines forCHIK ?
• What impact would an antiviral drug have onpathogenesis ?

How does CHIKV cause disease ?
– Clinical data• Fever, arthralgia, myalgia, rash• Severe forms: encephalopathy, elderly and neonates• Febrile arthralgia + lymphopenia < 1000; PPV > 80%
– Lessons from the mouse animal model andhistopathological analysis of human tissue samples
• Infected tissues are those in which symptoms manifest• Fibroblast are major target cells• Tissue envelopes are particularly targeted• Viral dissemination to the CNS, with CSF, meninges and ependyme
being infected• CNS access via choroid plexuses, but not brain microvessels• No apparent neuropathology• No placental infection per se, but per-natal vertical transmission
through placental breachesGérardin et al. PloS Med. 2008Staikovski et al., submittedCouderc et al. PLoS Path. 2008

020406080
100
0 2 4 6 8 10 12 14 16 18 20Day p.i.
surv
ivor
s (%
)IFNAR+/- adult mice IFNAR-/- adult mice
(idem for wt neonates)
020
4060
80100
0 2 4 6 8 10 12 14 16 18 20
surv
ivor
s (%
)
Day p.i.
Viru
s tit
er(T
CIID
50/m
l or g
)
102
103
104
105
106
107
serum
muscle
joint sk
inbra
in
In IFNAR+/-, CHIKV infects only tissuesclassically symptomatic in humans
a model for mild infection
Viru
s tit
er(T
CIID
50/m
l or g
)
102103104105106107
seru
m
muscle
joint sk
inbrai
n
108109
In IFNAR-/-, CHIKV disseminatesto the CNS (as in neonates)
a model for severe infection
Absence of type I interferon receptor (IFNAR)confers susceptibility to CHIKV
Couderc et al. PLoS Path. 2008
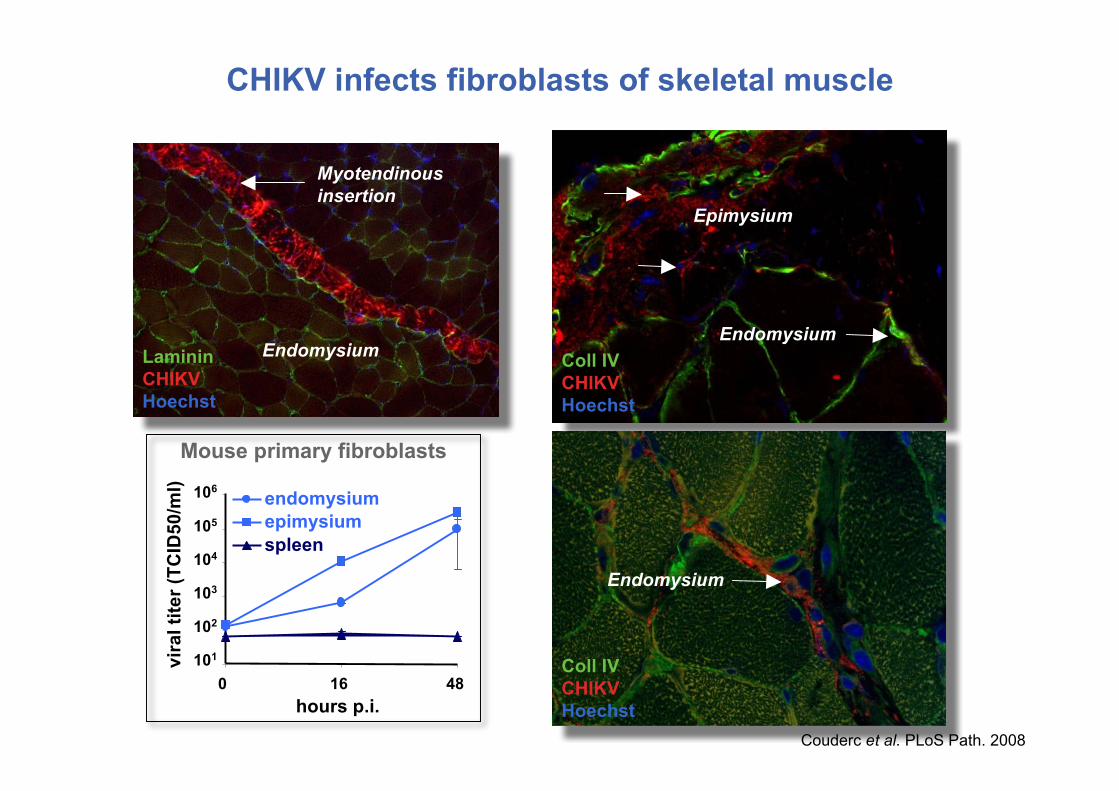
Endomysium
Coll IVCHIKVHoechst
Epimysium
Endomysium
Mouse primary fibroblasts
0 16 48hours p.i.
vira
l tite
r (TC
ID50
/ml) endomysium
epimysiumspleen
106
105
104
103
102
101
EndomysiumLamininCHIKVHoechst
Myotendinousinsertion
Coll IVCHIKVHoechst
Endomysium
CHIKV infects fibroblasts of skeletal muscle
Coll IVCHIKVHoechst
Couderc et al. PLoS Path. 2008

Endomysium Endomysium
CHIKV infects fibroblastsof the joint capsule and the dermis
Capsule
CHIKVHoechst
Coll. IVCHIKVHoechst
Deep dermis
SkinJoint
CHIKVHoechst
CHIKVHoechst
Couderc et al. PLoS Path. 2008

Similar cell tropism in human infected tissues
Couderc et al. PLoS Path. 2008

CHIKVHoechst
CHIKV infects choroid plexuses and disseminatesto the meninges and ependymal enveloppes
CHIKV-infected IFNAR-/- mouse
Coll. IVGFAPCHIKVHoechstBrain parenchyma
Brain microvessels
CHIKVGFAPHoechstEpendyma
Choroid plexuses
Couderc et al. PLoS Path. 2008

102
103
104
105
106
107
108
maternalserum fetuses
Viru
s tit
er
(TC
ID50
/ml o
r g)
Mother 1Mother 2Mother 3Mother 4
Materno-fetal transmissionassay in IFNAR-/- mice
CHIKV does not directly target the placental barrier
BeWo cells(syncytiotrophoblast)
CHIKVHoechst
101
102
103
104
105
106
Hours post infection
Viru
s tit
er(T
CID
50/m
l)0 24 48
No CHIKV infection of thesyncytiotrophoblast barrier
- CHIKV not detected in human placenta- Viral transmission only around the term
The fetus is most likely infected vialabor-induced placental barrier breaches ratherthan actual placental infection
Gérardin et al. PLoS Med. 2008Couderc et al. PLoS Path. 2008

What is known about the immunological responses andpathophysiological events of CHIK in the human host ?
– Critical role of type-I IFN• IFNAR, IFNAR-WT chimeras
– Adaptive immune system not critical to control infection• Viremia declines before the appearance of antibodies
– Generation of protective and in vitro/in vivo neutralizingantibodies in human and mice
– Possible role of macrophages in the inflammatory responseaccounting for post-acute symptoms (as for RRV)

Severe forms and encephalopathy in elderly and newborn
Correlation between viremia and severity
Attempt to decrease viral load in vivo- antiviral, vaccines- Immunotherapy and immunoprophylaxis
Severity
Viremia
What approaches are being pursued in terms of developmentof therapeutics as anti-virals or vaccines for CHIK ?

Severe forms and encephalopathy in elderly and newborn
Correlation between viremia and severity
Attempt to decrease viral load in vivo- antiviral, vaccines- Immunotherapy and immunoprophylaxis
Severity
Viremia
Strategy : 1. Harvest human immune plasma from convalescent individuals• selection based on clinical criteria, confirmed by Elisa
2. Purify IgGs from these pooled human plasma samples• according to a standard purification process used to produce
a commercial polyvalent human IgGs preparation3. Test for antiviral therapeutic and preventive activity
What approaches are being pursued in terms of developmentof therapeutics as anti-virals or vaccines for CHIK ?

CHIKV-IgGs therapeutic activity
0
20
40
60
80
100
0 2 4 6 8 10 12 14 16 18 20
Days post infection
surv
ivor
s (%
)
H0 piH8 pi
H24 pi
PBS
PBS
CHIKV-IgGs
PBS
CHIKV-IgGs
0
20
40
60
80
100
0 2 4 6 8 10 12 14 16 18 20
Days post infection
surv
ivor
s (%
)
H24 pi
H0 piH8 pi
H48 piPBS
IFNAR-/-
10 PFU CHIKV
WT NN106 PFU CHIKV
Couderc et al. JID, in press

What approaches are being pursued in terms of developmentof therapeutics as antivirals or vaccines for CHIK ?
– Preventive and therapeutic effect of polyclonal IgGs purifiedfrom convalescent patients
• Ready to be tested in human
– Understanding of CHIKV basic virology: entry and post entrysteps to help design inhibitors of viral attachment, envelopefusion, decapsidation and replication
– E1E2 as antigens for vaccine development (anti E1E2 IgGs areneutralizing)
– Candidates can be tested easily in our mouse model

What impact would an antiviral drug have on pathogenesis ?
– High viremia is associated with severity• Lowering viremia would most likely lowers symptoms
– Anti-inflammatory drugs may reduce post-acutesymptoms

T. Couderc, O. Disson, N. Gangneux, D. JudithG. Nikitas, S. Grayo, C. Deschamps, F. LaferriereInstitut Pasteur & Inserm, Paris-F
C. Schilte & M. AlbertInstitut Pasteur & Inserm
F. ChrétienInstitut Pasteur & Inserm
M. Grandadam & P. DesprèsInstitut Pasteur
F. Rey, J. Voss Institut Pasteur & CNRS
N. CayetInstitut Pasteur
A. Michault, P. Gérardin, G Barau et al.Groupe Hospitalier Sud-Réunion, La Réunion-F
N. Kandhoudi, J.F. ProstLFB Laboratories, Paris-F







