Concussion to Consequence: Managing Sport-Related Concussion On & Off the FieldOvid Webcast--October 18, 2011Ovid Webcast--October 18, 2011
Today’s Host
Anne Dabrow Woods MSN, RN, CRNP, ANP-BC
Chief Nurse, Lippincott Williams & Wilkins and Ovid Technologies
2
and Ovid Technologies
Publisher of American Journal of Nursing
Today’s Webcast is brought to you by…
American Medical Society for Sports Medicine
3
Also by…
4
Ovid and LWW work together to deliver the resources that health professionals
5
the resources that health professionals worldwide rely on every day

Today’s Speakers
Margot Putukian, MD, FACSMDirector of Athletic Medicine, Head Team Physician, Princeton University
Associate Professor, Robert Wood Johnson UMDNJ
Past-President, American Medical Society for Sports Medicine
NFL, Head, Neck & Spine Committee
6
NFL, Head, Neck & Spine Committee
John D. Corrigan, PhDProfessor, Ohio State UniversityDepartment of Physical Medicine and Rehabilitation
Editor-in-Chief of the Journal of Head Trauma Rehabilitation
Acute Concussion Identification & Management
7
Margot Putukian, MD., FACSM
Director of Athletic Medicine, Head Team Physician, Princeton University
Associate Professor, Robert Wood Johnson UMDNJ
Past-President, American Medical Society for Sports Medicine
NFL, Head, Neck & Spine Committee
Concussion Challenges
• Elusive injury
• Variability in presentation, can be subtle
• No clear marker, no
definitive test
8
definitive test
• Ideal management ?
• Track recovery ?
• Prevention?
• When “is it safe?”
• Research Evolving
Definition of Concussion Concussion in Sport, “Zurich Guidelines” McCrory et al, Clin J Sport Med. 19(3):185-200, May 2009
• Pathophysiological process affecting the brain
caused by direct or indirect biomechanical forces
• Common features:
– Rapid onset of usually short-lived neurological
impairment, typically resolves spontaneously
9
impairment, typically resolves spontaneously
– Clinical symptoms that reflect a functional
disturbance rather than structural injury
– Range of symptoms that may or may not involve
loss of consciousness (<10%)
• Standard neuroimaging is usually normal
Recognition of Injury
• Recognition of injury not always easy;
– Symptoms are not specific to concussive injury
– Presentation may be delayed for several hours-days
• High index of suspicion
• Differential diagnosis; trauma-induced
10
• Differential diagnosis; trauma-induced
migraine, skull fracture, bleed or
other more serious
brain injury
• Standardized approach
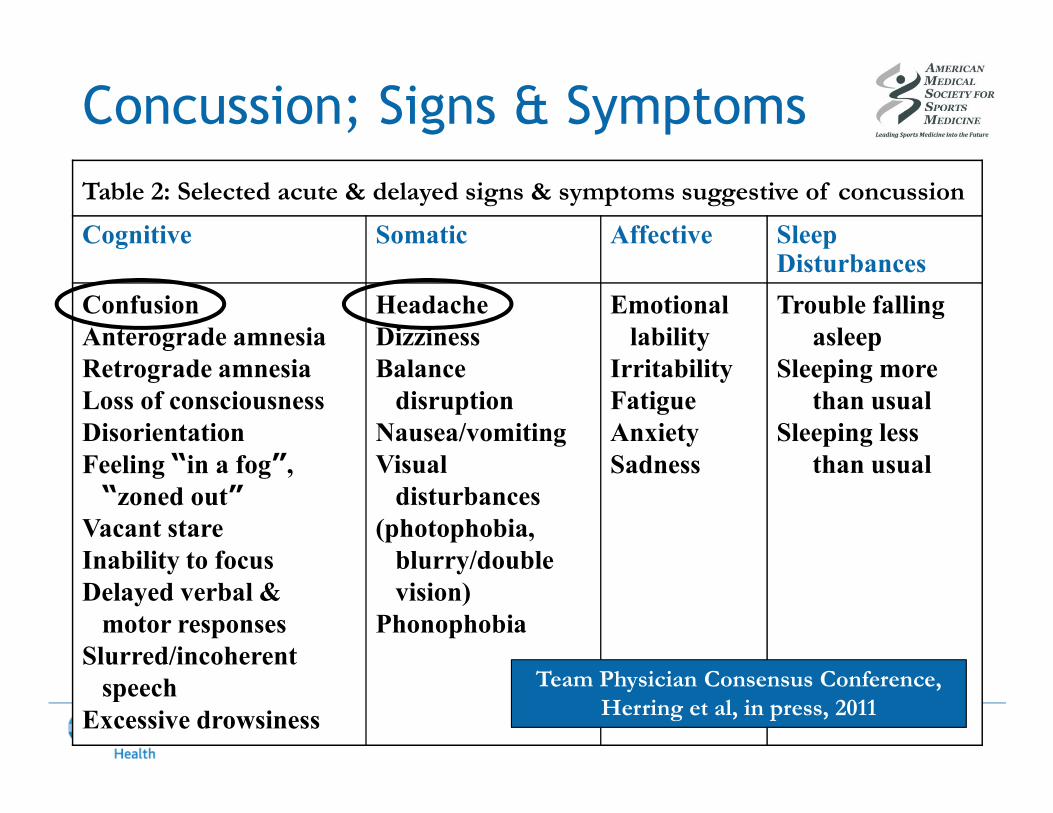
Concussion; Signs & Symptoms
Table 2: Selected acute & delayed signs & symptoms suggestive of concussion
Cognitive Somatic Affective SleepDisturbances
Confusion
Anterograde amnesia
Retrograde amnesia
Loss of consciousness
Headache
Dizziness
Balance
disruption
Emotional
lability
Irritability
Fatigue
Trouble falling
asleep
Sleeping more
than usual
11
Loss of consciousness
Disorientation
Feeling “in a fog”,
“zoned out”
Vacant stare
Inability to focus
Delayed verbal &
motor responses
Slurred/incoherent
speech
Excessive drowsiness
disruption
Nausea/vomiting
Visual
disturbances
(photophobia,
blurry/double
vision)
Phonophobia
Fatigue
Anxiety
Sadness
than usual
Sleeping less
than usual
Team Physician Consensus Conference,
Herring et al, in press, 2011
Pre-Season Assessment
• Concussion plan for “high risk” sports
• EDUCATION
• Identify modifiers; known to prolong or
complicate recovery
• Baseline evaluation; symptoms, neurological
12
• Baseline evaluation; symptoms, neurological
exam including cognitive and balance exam
• Emergency protocols & procedures Identify facility that is trauma center w/ neurosurgical capabilities
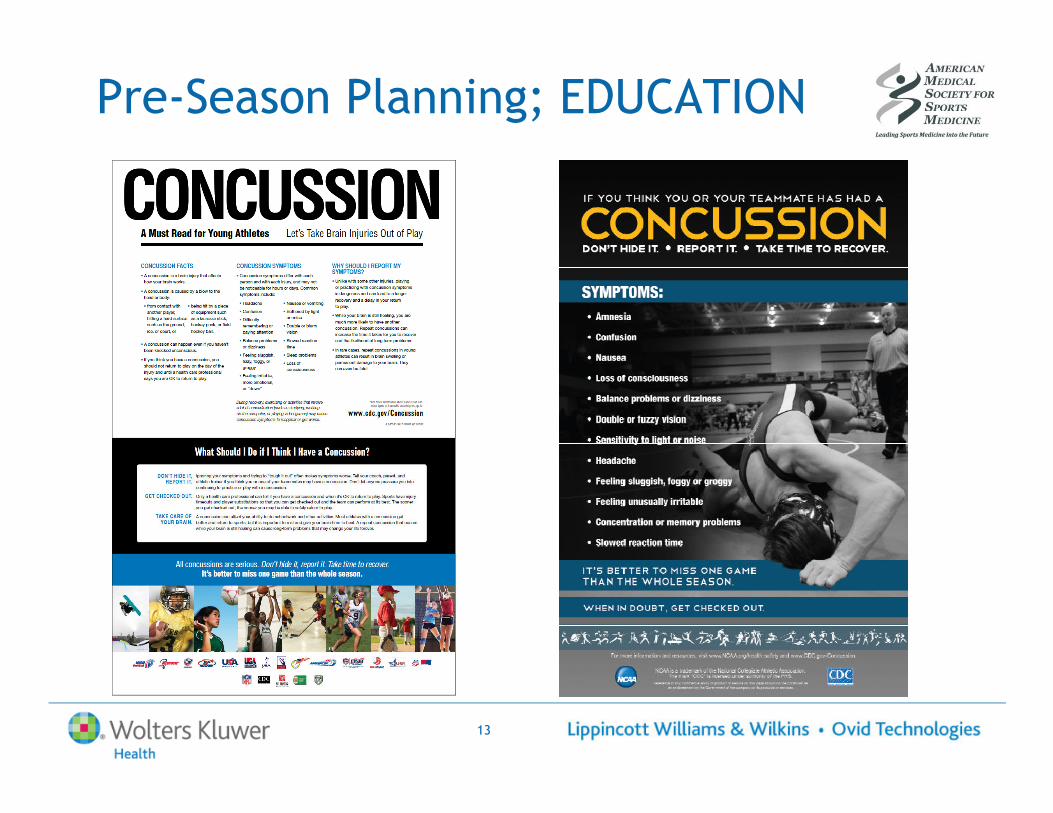
Pre-Season Planning; EDUCATION
13
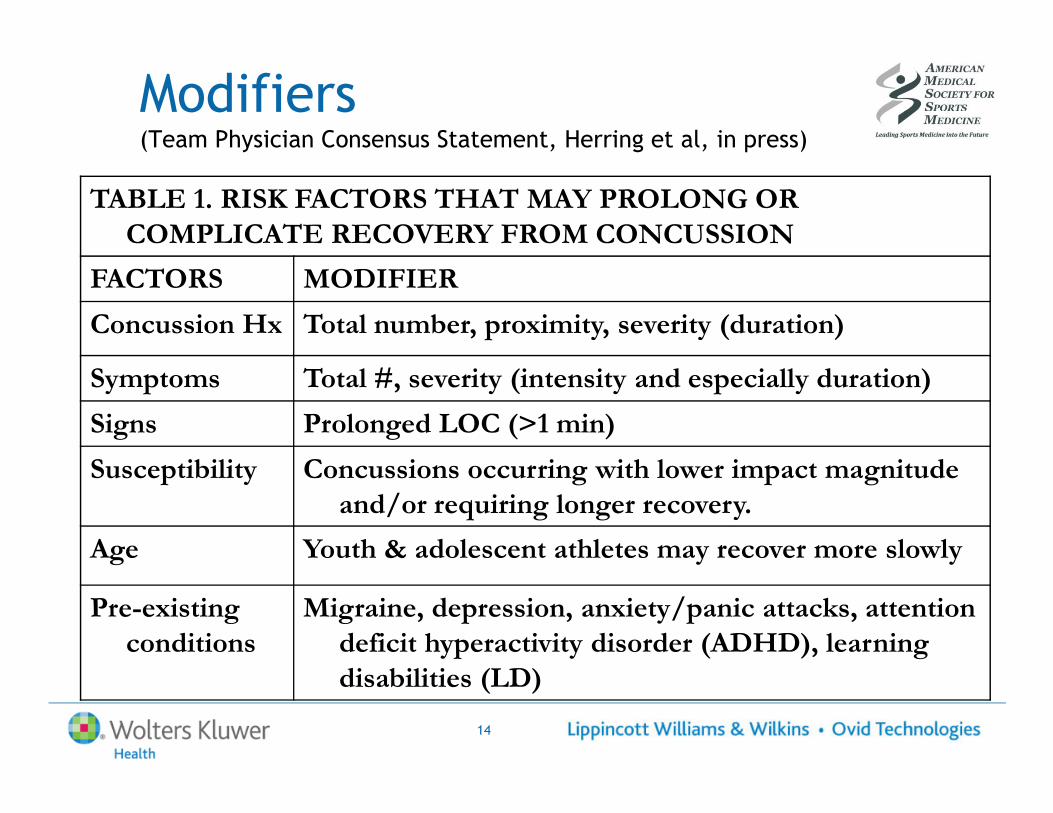
Modifiers (Team Physician Consensus Statement, Herring et al, in press)
TABLE 1. RISK FACTORS THAT MAY PROLONG OR
COMPLICATE RECOVERY FROM CONCUSSION
FACTORS MODIFIER
Concussion Hx Total number, proximity, severity (duration)
Symptoms Total #, severity (intensity and especially duration)
Signs Prolonged LOC (>1 min)
14
Signs Prolonged LOC (>1 min)
Susceptibility Concussions occurring with lower impact magnitude
and/or requiring longer recovery.
Age Youth & adolescent athletes may recover more slowly
Pre-existing
conditions
Migraine, depression, anxiety/panic attacks, attention
deficit hyperactivity disorder (ADHD), learning
disabilities (LD)
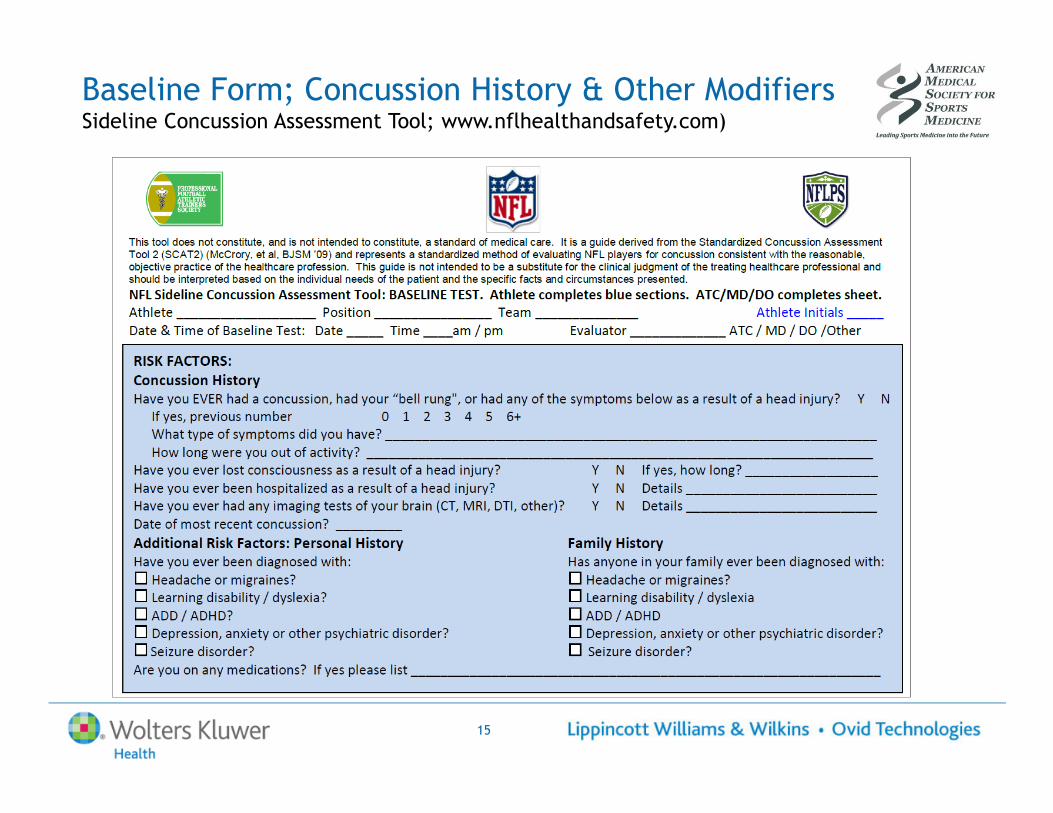
Baseline Form; Concussion History & Other Modifiers (NFL Sideline Concussion Assessment Tool; www.nflhealthandsafety.com)
15
Sideline / On Field Assessment
• Recognition and evaluation of athlete with
concussion is essential role of medical
staff covering practice/games
16
• No same day return to play for athlete
suspected of or diagnosed with
concussion, even if symptoms resolve as
athletic event evolves
Sideline Evaluation• ABC’s (airway, breathing, circulation)
• Neurologic & mental status
• Rule out c-spine, skull
fracture, intracranial bleed
• Spine board & transport to
appropriate facility if (+)
17
appropriate facility if (+)
• Remove from play; close
observation
• Detailed history &
concussion evaluation
None Moderate Severe
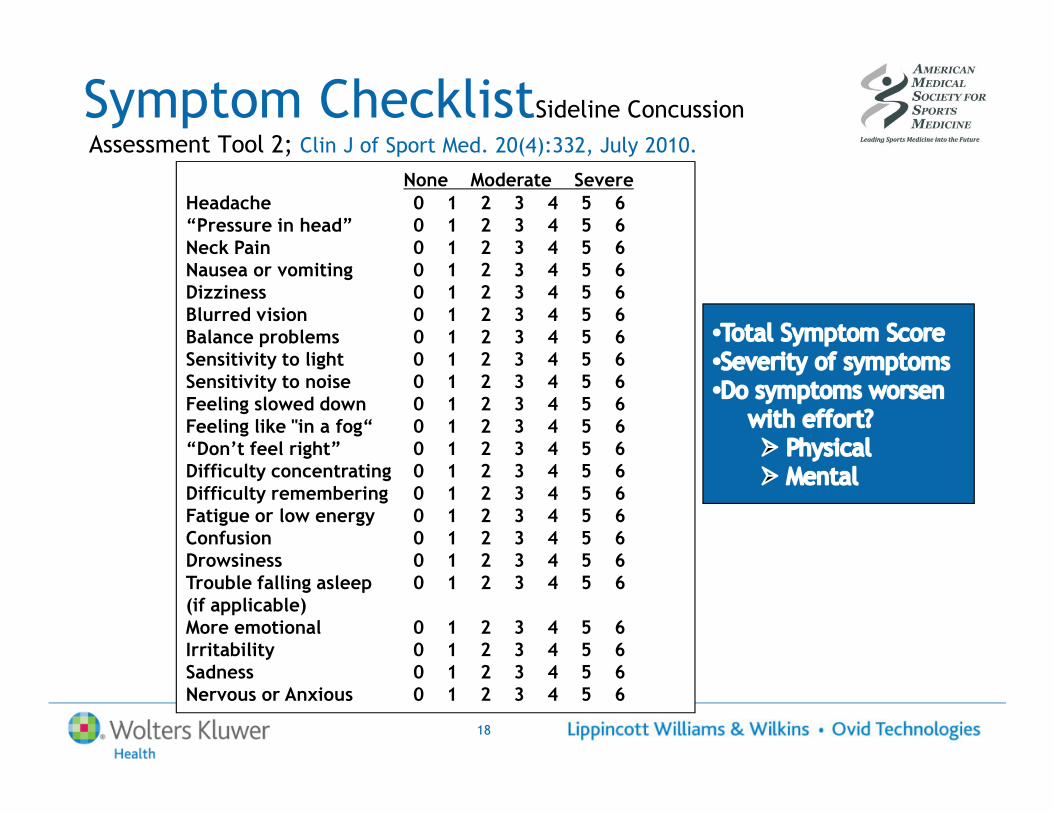
Headache 0 1 2 3 4 5 6“Pressure in head” 0 1 2 3 4 5 6Neck Pain 0 1 2 3 4 5 6Nausea or vomiting 0 1 2 3 4 5 6Dizziness 0 1 2 3 4 5 6Blurred vision 0 1 2 3 4 5 6Balance problems 0 1 2 3 4 5 6Sensitivity to light 0 1 2 3 4 5 6Sensitivity to noise 0 1 2 3 4 5 6Feeling slowed down 0 1 2 3 4 5 6
Symptom ChecklistSideline Concussion
Assessment Tool 2; Clin J of Sport Med. 20(4):332, July 2010.
18
Feeling slowed down 0 1 2 3 4 5 6Feeling like "in a fog“ 0 1 2 3 4 5 6“Don’t feel right” 0 1 2 3 4 5 6Difficulty concentrating 0 1 2 3 4 5 6Difficulty remembering 0 1 2 3 4 5 6Fatigue or low energy 0 1 2 3 4 5 6Confusion 0 1 2 3 4 5 6Drowsiness 0 1 2 3 4 5 6Trouble falling asleep 0 1 2 3 4 5 6(if applicable)More emotional 0 1 2 3 4 5 6Irritability 0 1 2 3 4 5 6Sadness 0 1 2 3 4 5 6Nervous or Anxious 0 1 2 3 4 5 6
Sideline Evaluation SCAT2, Clin J Sport Med. 20(4):332, July 2010
• Is the athlete acting differently?
• Was there loss of consciousness?, If so, for
how long?
• Was there problems with balance or unsteadiness?
• Orientation Questions:
19
• Orientation Questions:– What month is it?
– What’s the date?
– What day is it?
– What year is it?
– What time is it, (within an hour) ?
Sideline EvaluationSCAT2, Clin J of Sport Med. 20(4):332, July 2010
• Modified Maddocks;– What venue?
– What ½ is it?,
– Who just scored?,
– Who did we play last week?
– Did we win?
• Cognitive Evaluation
20
• Cognitive Evaluation– 5 word recall, 3 trials
– Months backwards
– Digit Span Backwards
– Delayed recall
• Balance Evaluation BESS
• Finger to nose X 5
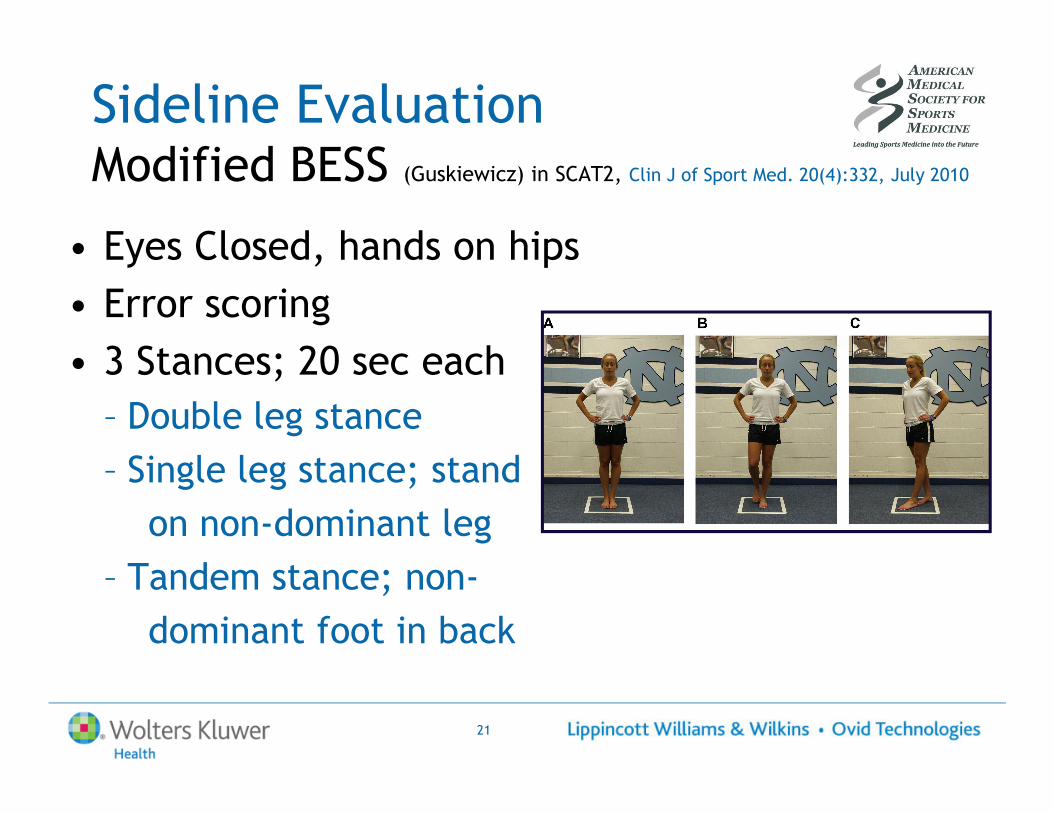
Sideline EvaluationModified BESS (Guskiewicz) in SCAT2, Clin J of Sport Med. 20(4):332, July 2010
• Eyes Closed, hands on hips
• Error scoring
• 3 Stances; 20 sec each
– Double leg stance
21
– Double leg stance
– Single leg stance; stand
on non-dominant leg
– Tandem stance; non-
dominant foot in back
When to Refer to the ERSCAT2, Clin J of Sport Med. 20(4):332, July 2010
• Prolonged disturbance of conscious state
• Focal neurological deficit
• Worsening symptoms
• Lethargy / drowsiness
22
• Significant or worsening headache
• Nausea / vomiting
• Seizures
• These are the indications for CT / MRI to exclude skull fracture or bleed
Disposition
• Athlete should be improving & monitored
• If any deterioration, consider transport
for emergency evaluation / exclude
more serious brain injury
23
more serious brain injury
• Post Injury Care; if stable and able to go
home under care of responsible adult
Post Injury Care
• Physical & Cognitive rest
• Plan for follow up care
• Home care information;
– When to go to ER
– Avoid aspirin, NSAIDs, alcohol
24
– Avoid aspirin, NSAIDs, alcohol
– No exertion / lifting
– Avoid cognitive work
• Consider Neuropsychological
testing
• May need to make school/work accommodations
• Determine severity of injury once all
symptoms have cleared, neurologic
exam (including cognitive evaluation,
and balance normal)
Severity of Injury
25
and balance normal)
• Nature, burden, duration of symptoms
may be more indicative of severity
Severity of Injury;
• Memory problems, persistent confusion
associated with concussions that take
longer for recovery Collins CJSM ’03, Erlanger ’03
26
• Headache lasting > 60 hrs, self report of
“fatigue/fogginess”, or > 4 symptoms
associated with delayed RTP Makdissi AJSM ‘10
• Many factors to consider in NP testing
• Provides reliable assessment &
quantification of brain functioning by
examining brain - behavior relationships
Neuropsychological (NP) Testing
27
• Many factors to consider in NP testing
• Not uncommon to see deficits in cognitive
function by NP testing persist after
symptoms have abated… opposite also true
Collins AJSM ’03, Collins CJSM ’03, Echemendia ’01, Lovell ’03, McCrory ’05, Broglio ’07, VanKampen ’06,
Echemendia NAN 10/21/08
Neuropsychological Testing
Types of tests
• Computerized
• Paper / pencil
• Hybrid
Measure broad range of cognitive function:
• Speed of information processing
• Memory recall
28
• Memory recall
• Attention & concentration
• Reaction Time
• Scanning & visual tracking ability
• Problem solving abilities
Use of Neuropsychological Testing
• Contribution to management & RTP
• Protocols for using NP as part of
“concussion plan” is evolving
• One “tool in the toolbox”
29
• One “tool in the toolbox”
• Cannot be used on own to make or rule
out diagnosis or “clear” athlete
• Neuropsychologists are in the best
position to interpret tests
Take Home; Return to Play
• Return to Play (RTP) decision challenging
• Consider Modifiers;
• Individualized progression
– Symptom free at rest
30
– Symptom free at rest
& w/ exertion
– Normal neurological exam (including cognitive and balance evaluation)
– Gradual progression w/ incremental increase• Physical demands & risk for contact
Age as Modifier• Recovery appears to take longer in the
young athlete
• Maturing brain may
be at particular risk
• Second Impact
31
• Second Impact
Syndrome reported
primarily in athletes < 18
• Education of athletes & parents
particularly important in young
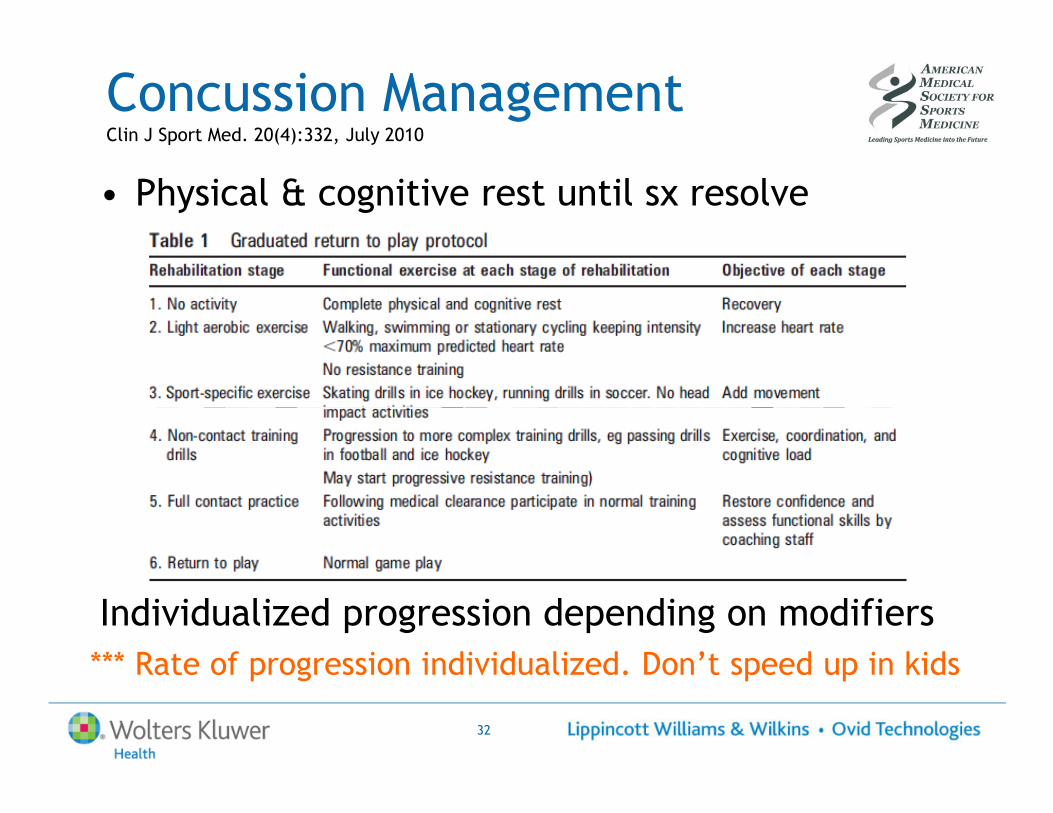
Concussion Management Clin J Sport Med. 20(4):332, July 2010
• Physical & cognitive rest until sx resolve
32
Individualized progression depending on modifiers
*** Rate of progression individualized. Don’t speed up in kids
Prevention?
• Mouthguards / Helmets?
• Rule Changes / Changing the “culture of the game”
• Neck strengthening / conditioning
• Education
• NFL as role model;
33
• NFL as role model; – Significant change in rules; no same day RTP, defenseless
players, hits to head, $$ penalties
– Education
– Standardized sideline evaluation
– Ongoing research efforts
– Long term / cumulative effects of head trauma
Future Directions
• Role of new neuroimaging techniques, genetics?
• Risk factors & modifiers?– Why do some athletes seem to be at greater risk for injury
and/or take longer to recover?
• Role of Neuropsychological testing; ideal protocol?
34
• Role of Neuropsychological testing; ideal protocol?
• Depression & suicide?
• Gender effect?
• Rehabilitation?
• Ideal tools for assessment and tracking recovery?
• MORE RESEARCH NECESSARY
Additional Resources
• “Zurich Guidelines”; McCrory et al, Clin J Sport Med. 19(3):2009
• SCAT2: Clin J Sport Med. 20(4):332, July 2010
• Team Physician Consensus Statement, Herring et al, in
press, Med Sci Sports Exerc
• http://www.amssm.org/ Find a Doc, Statement on
35
• http://www.amssm.org/ Find a Doc, Statement on
Concussion in Athletes in review
• http://www.cdc.gov/concussion/sports/
• www.nflhealthandsafety.com
• http://www.aan.com/go/practice/concussion
Lifetime Risks of Concussions
36
John D. Corrigan, PhDProfessorDepartment of Physical Medicine and RehabilitationOhio State University
What are the long-term consequences?
• The concussion has cleared.
• The athlete’s sport has relatively greater risk for concussion.
• You are asked, “should this athlete
37
• You are asked, “should this athlete
risk a subsequent concussion?”
What do we know?
Zurich guidelines Consensus Statement on Concussion in Sport, 3rd
International Conference, McCrory et al., Clin J Sport Med 2009 19(3).
• “Recognizing the importance of a concussion history, and appreciating the fact that many athletes will not recognize all the concussions they may have suffered in the past, a detailed concussion history is of value.” (p. 189)
38
Zurich guidelines Consensus Statement on Concussion in Sport, 3rd
International Conference, McCrory et al., Clin J Sport Med 2009 19(3).
• “Recognizing the importance of a concussion history, and appreciating the fact that many athletes will not recognize all the concussions they may have suffered in the past, a detailed concussion history is of value.” (p. 189)
39
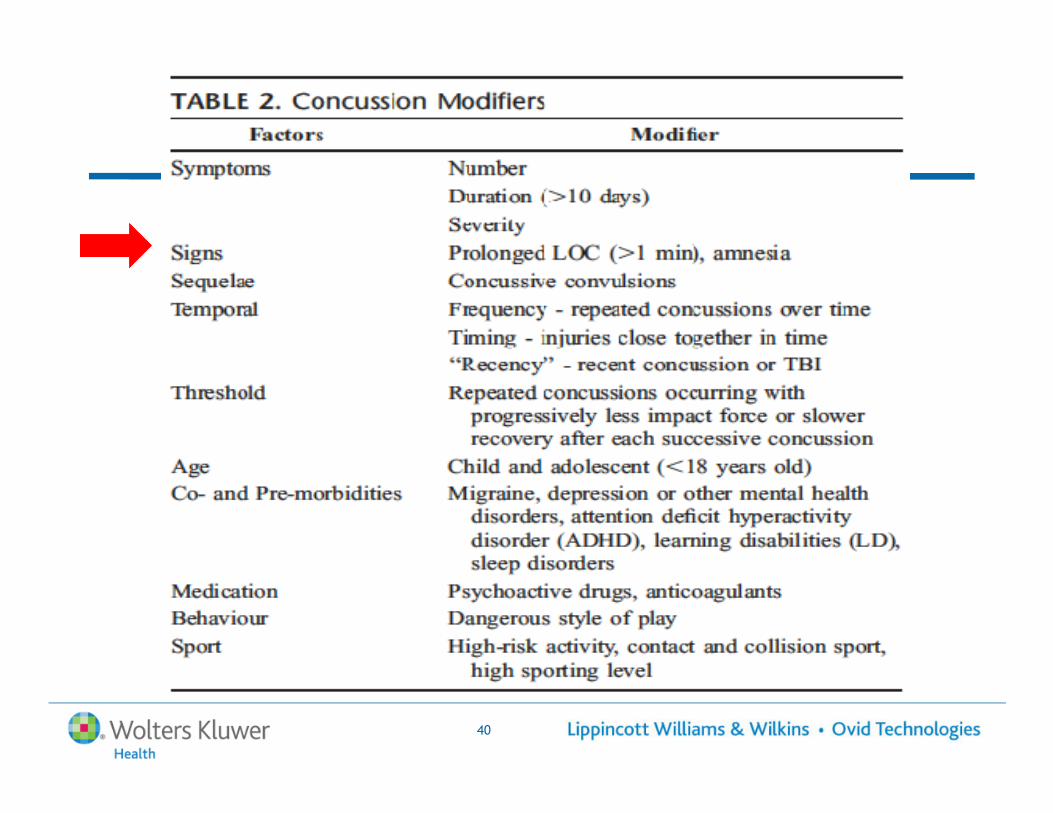
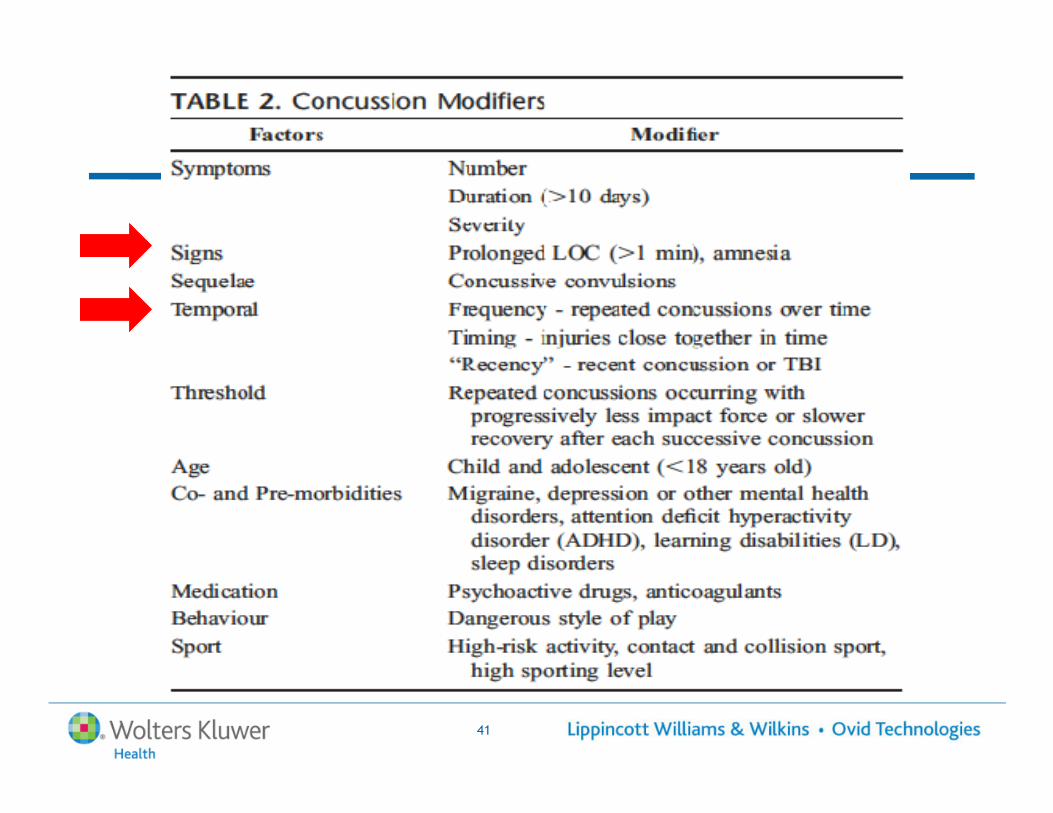
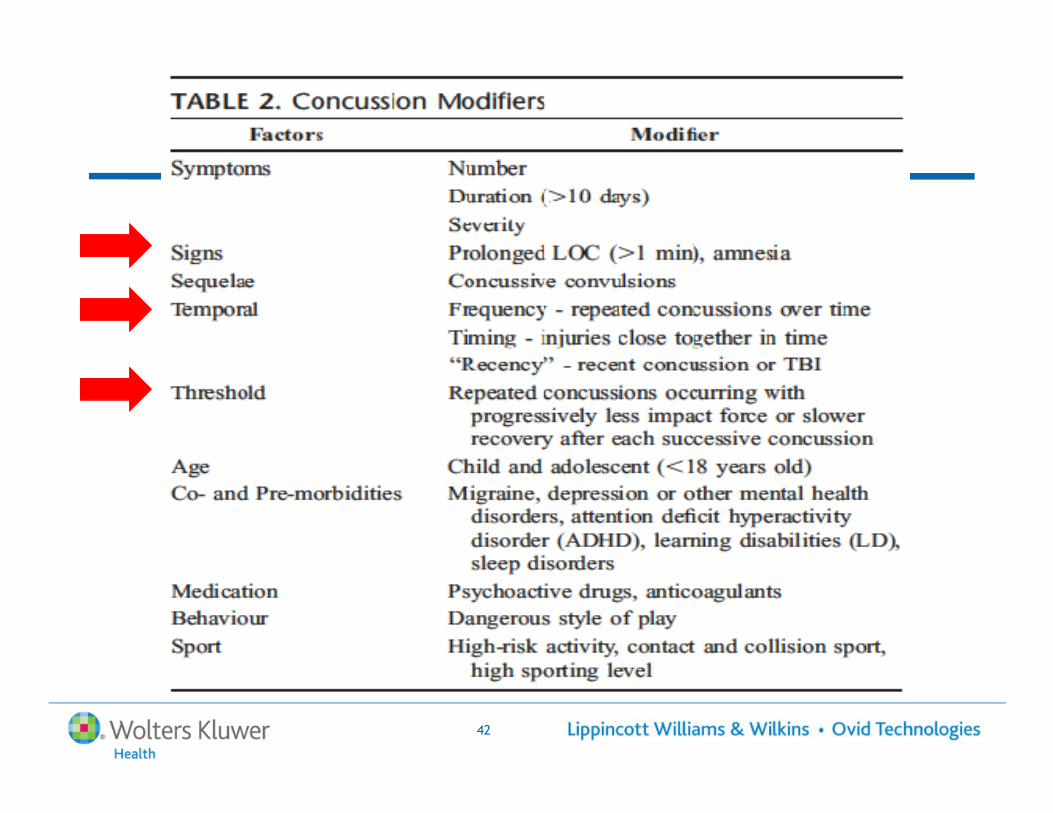
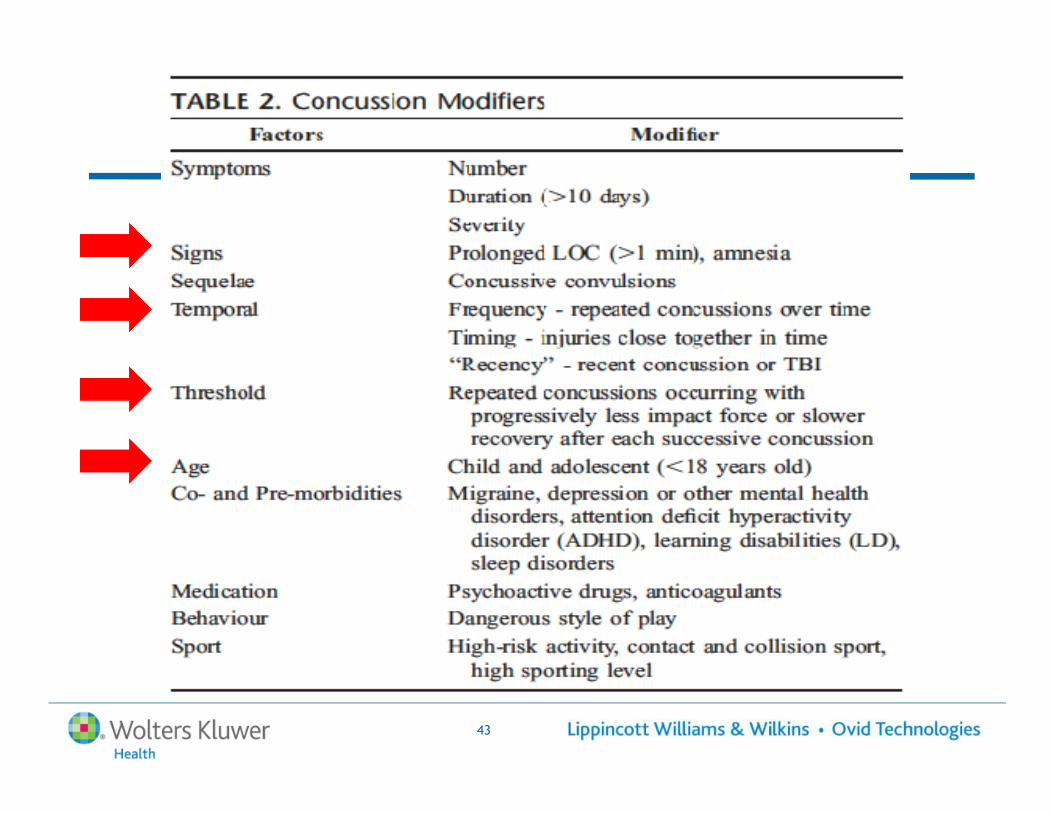
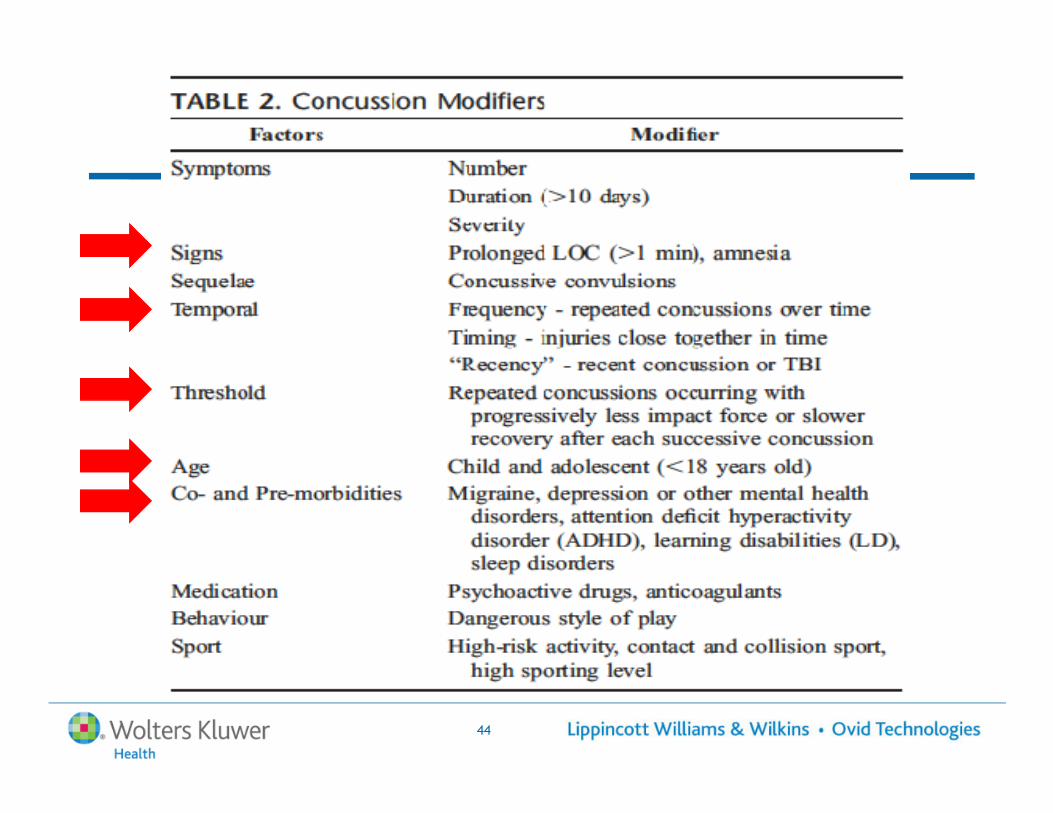
• “The consensus panel agreed that a range of modifying factors may influence the investigation and management of concussion and in some cases may predict the potential for prolonged or persistent symptoms.” (p. 189)
40
41
42
43
44
What’s new?
1. Emerging data on delayed consequences of traumatic brain injury, including mild TBI
45
What’s new?
1. Emerging data on delayed consequences of traumatic brain injury, including mild TBI
46
2. Emerging data on factors other than severity that increase thelikelihood of long-termconsequences
2009 Institute of Medicine Report
Gulf War and Health
Volume 7:
47
Long-Term Consequences of
Traumatic Brain Injury
Consequences of TBI Persisting or Developing Six or More Months Post-injury
• Seizures• Ocular- & visual-motor disturbances
• Cognitive deficits• Post-concussive
48
• Post-concussive symptoms
• Depression• Aggression• Suicide• Unemployment• Social isolation
Consequences of TBI Persisting or Developing Six or More Months Post-injury
• Seizures• Ocular- & visual-motor disturbances
• Cognitive deficits• Post-concussive
• Psychosis• Premature death• Progressive dementia
• Parkinsonism
49
• Post-concussive symptoms
• Depression• Aggression• Suicide• Unemployment• Social isolation
• Parkinsonism• Diabetes insipidus• Endocrine dysfunction
• Hypopituitarism• Growth hormone insufficiency
Consequences of TBI Emerging orRe-Emerging Later in Life
• Seizures• Ocular- & visual-motor disturbances
• Cognitive deficits• Post-concussive
• Psychosis• Premature death• Progressive dementia
• Parkinsonism
50
• Post-concussive symptoms
• Depression• Aggression• Suicide• Unemployment• Social isolation
• Parkinsonism• Diabetes insipidus• Endocrine dysfunction
• Hypopituitarism• Growth hormone insufficiency
Consequences of Mild TBI
• Seizures• Ocular- & visual-motor disturbances
• Cognitive deficits• Post-concussive
• Psychosis• Premature death• Progressive dementia
• Parkinsonism
51
• Post-concussive symptoms
• Depression• Aggression• Suicide• Unemployment• Social isolation
• Parkinsonism• Diabetes insipidus• Endocrine dysfunction
• Hypopituitarism• Growth hormone insufficiency
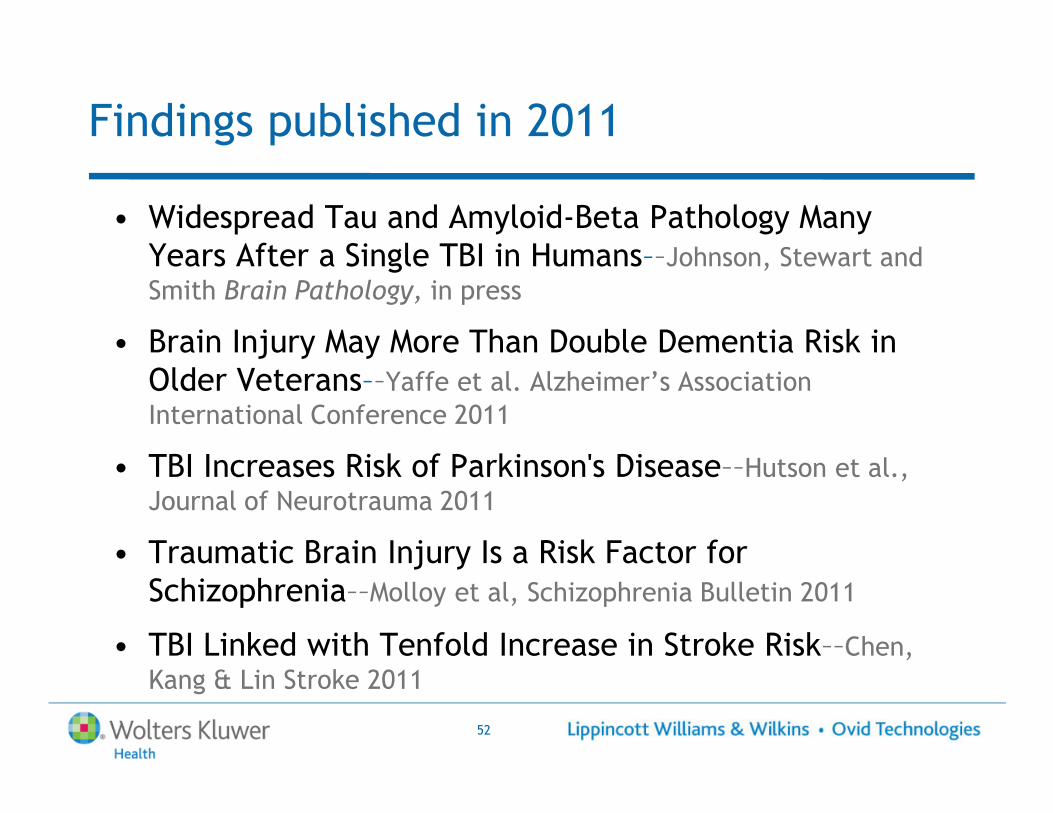
Findings published in 2011
• Widespread Tau and Amyloid-Beta Pathology Many Years After a Single TBI in Humans––Johnson, Stewart and Smith Brain Pathology, in press
• Brain Injury May More Than Double Dementia Risk in Older Veterans––Yaffe et al. Alzheimer’s Association International Conference 2011
52
International Conference 2011
• TBI Increases Risk of Parkinson's Disease––Hutson et al., Journal of Neurotrauma 2011
• Traumatic Brain Injury Is a Risk Factor for Schizophrenia––Molloy et al, Schizophrenia Bulletin 2011
• TBI Linked with Tenfold Increase in Stroke Risk––Chen, Kang & Lin Stroke 2011
#2 New Findings about Lifetime History of TBI
• Moderate and severe TBI’s are not the only ones that leave residual consequences.
• Not just TBI’s resulting in loss of consciousness
• New findings suggesting:
53
• New findings suggesting:
– Repeated, mild TBI’s
– Mild TBI’s early in life
Repeated Mild TBI’s
• “Multiple mild” TBI’s observed in athletes, members of the armed services exposed to blasts, victims of child abuse, victims of intimate partner
54
child abuse, victims of intimate partner violence, and substance abusers
• Concerns regarding subconcussive blows among athletes, as well as service members exposed to blasts
Early developmental TBI’s
• Clients in substance abuse treatment have higher incidence of childhood TBI’s than general public.
• Prisoners have high prevalence of early childhood TBI’s.
55
TBI’s.
Early developmental TBI’s
• Clients in substance abuse treatment have higher incidence of childhood TBI’s than general public.
• Prisoners have high prevalence of early childhood TBI’s.
56
TBI’s.
• General public with TBI’s before age 15 more likely disabled in adulthood.
• Birth cohorts show early TBI’s predispose to later behavioral problems.
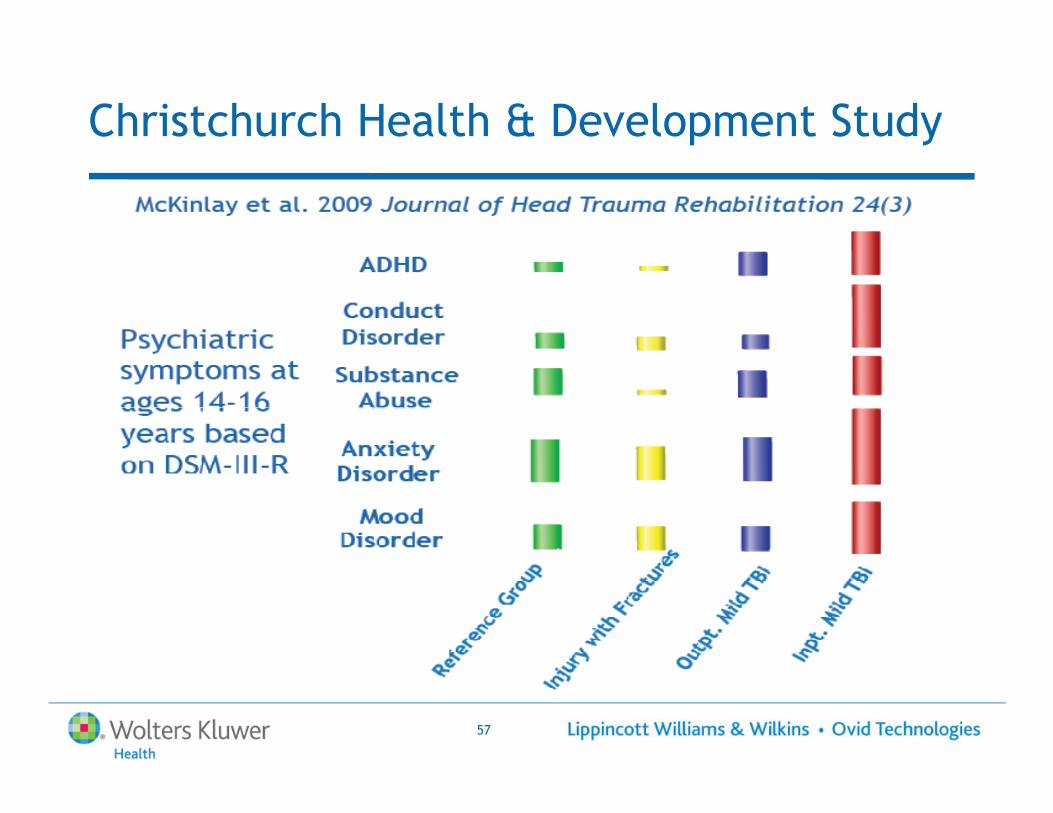
Christchurch Health & Development Study
57
A Major Missing Piece of Information
How does a temporary disruption of brain function become permanent damage?
• Metabolic?
• Genetic or epigenetic?
58
• Functional (i.e., electrical/neurochemical)?
• Structural?
Does the “spacing” between blows make
a difference?
“When can an athlete risk a subsequent concussion?”
• For now, must be answered on an athlete-by-athlete basis.
• History of altered consciousness without loss of consciousness less risky than concussions with loss of consciousness.
• No guidance for how much loss of consciousness is
59
• No guidance for how much loss of consciousness is inconsequential when evaluating previous TBI’s.
• Reason for concern about experiencing a subsequent TBI while still healing from a previous, and cannot rule-out the risk of subconcussive blows.
• Reason for concern about childhood TBI’s even if mild.
Stay in-touch with this topic
� Visit the AMSSM website www.amssm.org
� Find the latest coverage in The Journal of Head Trauma Rehabilitation www.headtraumarehab.com
� Try OvidMD for free in Oct 2011 by signing up at www.ovid.com . OvidMD is a clinical tool for clinicians that provides quick answers to clinical questions based on relevant current full-text content from Ovid and UpToDate™ .
60
content from Ovid and UpToDate™ (separate subscription required).

Q&A Session
61
Webcast Archive and Survey
� This webcast will be archived in approximately 3-4 days, and will be available for 12 months via www.Ovid.com/webcasts. You will be notified by e-mail when the archive is available
� Sign up for on-demand viewing of our previous webcasts at:
62
� Sign up for on-demand viewing of our previous webcasts at: www.Ovid.com/webcasts
� Your feedback is very valuable to us. Please complete our post webcast survey and you could win a $100 USD AMEX gift certificate!

Thank You!







