Download - Dental Sleep Medicine Insider
January 2015
Insider DENTAL SLEEP
MEDICINE

www.DentalSleepSolutions.com
THE CLINICAL CORNER 10 Seconds or10 Minutes?
Have you ever had a patient in a TAP device need more protrusion
than the device permits? Did you send it back to the lab, incurring repair
fees & leaving your patient without their device? I used to do the same
thing, but there is a simple way to reposition the hook within 10 minutes &
an even simpler way to do it in less than 10 seconds. The key to a success-
ful Dental Sleep Medicine practice is efficiency & dedicating a few
minutes to watching this video will save you a ton of time during your Den-
tal Sleep career. Grab some popcorn, a handpiece, and enjoy….
With Dr. Gy Yatros
Watch:

877.95.SNORE
10 Seconds or10 Minutes?

Keller’s ClearDream
Clear Improvements on an Old Design
In recent years, the dental sleep medicine community has seen myriad new appli-ances enter the market, often claiming to revolu-tionize how you approach oral appliance therapy (OAT). These claims are al-most always unfounded and can lead to uncertainty among clinicians about what’s real and what is mere hype. That’s why I was skeptical about Keller’s newest product, the Clear-Dream, from the outset. I mean, a dorsal is a dorsal is a dorsal, right? Whether it’s blue or pink or green, who cares. However, with little hype or baseless claims, the ClearDream speaks for itself by taking the familiar, prov-en concepts and adding several significant improve-ments. I found there to be three key differentiators when compared with other similar devices. Just by looking at the Clear-Dream, the first difference is immediately apparent. It is made using a clear mate-rial, not colored acrylic like all other dorsals. This is im-portant not for esthetic purposes but because the device is fabricated using Keller’s proprietary clear, clinically unbreakable, non-porous Crystal Clear 450 material. As a result, the
Dr. Tarun Agarwal Raleigh Dental Arts
Raleigh, NC
To prescribe a ClearDream for your patient, schedule a pickup, or learn more,
click here or call 888-919-7577.
www.KellerLab.com
device won’t absorb stain and odor, nor will the fins break as can occur with many other appliances. Constant repairs or remakes eat into profits quickly, so durability is para-mount. I know this claim about durability is true be-cause it’s the same material they use for NTI Plus splints. Another benefit of the Crystal Clear material is its highly retentive nature, avoiding the need for ball clasps in all but the most extreme situations. This means I don’t incur a bunch of charges for addi-tional ball clasps just to en-sure the trays don’t dislodge. At the other end of the spec-trum, there is an option for a heat-activated Thermofit lin-er for patients with deep un-dercuts or for additional com-
www.DentalSleepSolution.com
fort. When I’ve used this option, they drop right in and usually re-quire zero adjustments. Chairtime is valuable and with the Clear-Dream I don’t have to block out extra time because I know I won’t be grinding on acrylic all after-noon. Now, if only my crowns dropped in this easily. The second major difference seems to be a key feature of ClearDream’s design philosophy; less material and increased pa-tient comfort. Utilizing the Crystal Clear material allows for a slim-mer, more streamlined, and more comfortable device without com-promising durability. There is sig-nificantly less acrylic in the anteri-or than other dorsals with no faci-al coverage on the maxillary arch and only slight incisal overlap on the mandibular segment which creates an anterior opening. The opening also reduces bulk which
increases comfort and may increase patient compliance. A reduction in overall bulk isn’t limited to the anterior either. The lingual surfaces of the ClearDream are contoured to the teeth; a design feature that maximizes tongue space. The ClearDream allows for 5.5mm of advancement from the initial set position. Like with any dorsal device, it’s im-perative you capture an accu-rate George Gauge bite. Along with the bite, I send VPS im-pressions but Keller can also make them with models or digital scans (something I find useful, since I’m currently dig-itizing my entire process). Oc-casionally, I have notches add-ed when I need to use elastics. The last key differentiator is the price. At only $299 for the hard acrylic version and $319 for the Thermofit-lined Clear-Dream, you’re getting the best dorsal device on the market for the lowest price point. To para-phrase Gordon Christensen, for a product to be worth using, it has to be better, faster, cheap-er, and easier. The ClearDream meets all of these criteria.

increase patient compliance. A
the teeth; a design feature that
rate George Gauge bite. Along
casionally, I have notches add-ed when I need to use elastics.
the price. At only $299 for the
Dream, you’re getting the best dorsal device on the market for the lowest price point. To para-phrase Gordon Christensen, for a product to be worth using, it has to be better, faster, cheap-er, and easier. The ClearDream

As a clinician and educator for over two dec-ades, I have had the pleasure of witness-
ing the astonishing evolution of the Sleep Medicine field. For many, dental sleep medicine is a new opportunity for them to change the way their practice treats patents. I’m just one dentist, but for me, the ability to screen and offer patients oral de-vices broadens my experience while greatly improving my career satisfaction. It’s not often that a patient comes in and says, “Hey Doc, I need a mandibular ad-vancement device” BUT about 10% of your adult patients of rec-ord would probably benefit from one. This is precisely why I stress the importance of proper screen-ing and testing.
Until just a few years ago, medicine saw limited use of home sleep test
devices on a large scale but today, a Polysomnography (PSG) is seldom
considered to be the ‘gold standard’ test for OSA. The industry is experienc-
ing a continued increase in the use of home sleep testing with utilization surpas-sing traditional in-laboratory PSG soon. With new companies constantly en-tering to the market, it can be difficult to determine what makes sense for the prac-tice and who delivers on their commit-ments to you and your patients .
PSG vs. HST
The first of the testing methods I’ll touch on is the Polysomnogra-phy (PSG), the traditional ‘gold standard’ according to many in the in-
dustry (O’Brien, 2012), is a sleep study that is usually performed in a sleep lab or a hospital and is ‘attended’ or observed by a Registered Polysomnogram
Technician (RPSGT). A PSG, is used to diagnose sleep apnea among other sleep disorders including bruxism, parasomnias such as REM sleep behav- ior disorder, peri-
odic limb movements, and abnormal brain waves indicating nocturnal sei- zures. Some of these disorders cannot be detected by typical Home Sleep Tests (HST). Pa- tients must com-plete testing inside the facilities of a lab or hospital and in some instances there is medical reason to have the patient monitored in the lab/hospital setting i.e. Patient requires oxygen and bi-level PAP therapy. Unfortunately, the costs associated with PSG are rather high, pa-tients in outlying areas may experience difficulty locating a facility nearby, and patient ac-ceptance is rather low due to the high number of leads and unfamiliar setting. The second method of testing is the Home Sleep Test. The HST is a sleep study that can be performed in the patient’s home and is used to diagnose obstructive sleep apnea. Home sleep studies have been used for years overseas, but the United States have considered HST experimental and required attended in-lab PSG to diagnose Obstructive Sleep Apnea. In 2008, Medicare changed their stance on HST and shortly after, private in- surance compa-nies followed suit. This has resulted in increased access to care for patients and lower costs for payers. One of the palpable advantages that Home Sleep Tests have over a traditional Polysomnography is patient convenience. Incorporating HST into my practice has been met with very favorable feedback from my patients be-cause of the comfort and ease of the process. The accuracy has been fine and I have not experienced the need for re-
HST in my Practice
with Dr. Payam Ataii
877.95.SNORE

877.95.SNORE
There are many services that can help a practice get set up with HST but not all are created equally. I have had the benefit of working with a national company based out of Los Angeles called EZ Sleep. They offered the relationship with a sleep physician, set me up with the screening and testing assets for my practice, as well as offered training that myself and the staff used to learn how to screen patients and get them tested appropriately. One of the things that new dentist find it difficult to do is enter the dental sleep medicine arena. They do not know where or how to start a relationship with a medical doctor that can interpret the sleep results and diagnose if the patient has obstructive sleep apnea (OSA). This was one area that was an added benefit that came with the EZ Sleep package and product. For my practice we submit the screening, if a test is needed, it is scheduled with the patient, and once the test is completed, the results are sent to me with an easily un-derstood page describing the report and results of my pa-tients’ sleep test. This allows me to provide my patients with life-saving treat-ment while also increasing productivity and setting my prac-tice apart from the multitude of other practices nearby.
Contact Info www.EzSleeptest.com
310 North Westlake Boulevard, Suite 110 Westlake Village, CA 91362
Phone: (888) 240-7735
testing. In a 2012 study, results displayed that HST results were not inferior to the standard PSG (Rosen, Auckley, Benca, 2012). HSTs are also interpreted by a medical health professional as a PSG. For sufferers of sleep apnea who may live in remote areas and do not have easy access to sleep labs, this means increased access to sleep testing. Depending on which path you choose, you may be able to dispense the tests from your office but much simpler, companies such as EZ Sleep, ship HST devices to any home within the company’s reach and they help provide instructions and care for my patients. Lastly, with the changing medical/dental cost environment, a HST is a more cost effective option than the PSG, as it is estimated to be less than half the price of a traditional PSG. For this reason, many are making the move to HSTs in order to cut costs. It’s important to note that reimbursement for HST varies among payers and even the various Medicare coverage areas. These policies can seem to be a moving target and this is another benefit of working with EZ Sleep. I don’t have to dedicate a team member to figuring all of this out. Instead, they provide the insurance pre-authorization for HST and ensure that I have all of the necessary documentation. This allows me and my team to focus on other matters.
Adding Dental Sleep Medicine to My Practice

Let’s face it, we know how dental insur-
ance works. The tooth was broken, I diag-
nosed it, then I fixed it, now pay me, please.
Send in a claim with an X-ray and a short
narrative and it’s paid. Dental plans have
$750 to $3000 yearly maximums so the gate
keepers work hard to not pay claims, but
they know the faucet will turn off at some
point.
Medical plans are completely different
from dental plans. They have million dollar
maximums or frequently, no maximum at
all. Gate keepers are guarding that pile of
cash with their lives! Considering UHC is
currently holding 84th place at $80.96 Bil-
lion on the Forbes Global List, it’s obvious
they are doing a stellar job protecting that
gold like a dragon in a fairy tale. Now, if
every policy holder was running around get-
ting 3D imaging and blood panels drawn for
every tummy ache they assumed was a tu-
mor, UHC might not even get onto the pres-
tigious Forbes list. To stop patients from
deciding what treatment they need based on
Google and WebMD, medical plans use pre-
authorizations to decide if the treatment or
testing is “medically necessary”. By getting
the prescription for treatment and Letter of
Medical Necessity (LOMN) proof is provid-
ed to the plan that the patient needs the oral
appliance, and we are playing by the rules.
Pre-authorizations are not a luxury, they are
a necessity and the LOMN is the most im-
portant piece of the puzzle for an approval.
This magical letter is the key to unlock the
safe and get payment for the treatment you
are delivering. But wait! There is more! This
act of correspondence not only gets you paid
by the insurance companies, but also gives
you credibility and opens communication
with primary care doctors, sleep doctors, and
pulmonary specialists. You want as many
physicians aware of how easy you are to
work with and you want them to know their
patients will be treated with the utmost care,
compassion, and professionalism. Utilizing
patients’ benefits and minimizing out of
pocket costs can be more important. You
want the patient to get the root canal done so
you can fit the crown, right? So you refer to
the office that gets your patient treated and
sent back to you. The DDS who treats sleep
apnea for cash and doesn't play the medical
insurance game is equivalent to the specialist
who costs so much that your patient actually
gets mad at you for sending them.
While medical offices are as familiar with
the LOMN as we are with referrals for 3rd
molar extractions, they still want it to be
easy and take as little time as possible. DS3
gives you the tools to send letters introduc-
ing yourself as a skilled dentist treating sleep
apnea with an interest in treating mutual pa-
tients. It’s simple and with a couple mouse
clicks, it can be printed for mailing or trans-
mitted via digital fax. Medical offices appre-
ciate that the LOMN is already filled out -
just sign here and send back please.
www.DentalSleepSolutions.com
LETTER OF MEDICAL NECESSITY: WHAT, WHY, & THE BIGGEST QUESTION:
“HOW DO I GET ONE?” LOMN. These four ominous letters have been the road
block for many dental offices, including my own….
GoGo Tip of the Month:
Send the letter and LOMN to
the primary care physician, the
sleep doctor, heart specialist or
any other specialist who has
had any involvement with the
patient’s diagnosis and/or treat-
ment. Whomever sends it back
signed first - wins! You only
need one to give to the insur-
ance gate keeper. Contact me
with any questions & have a
happy & productive 2015!
Lesia Crawford,
CEO, GoGo Billing
877-874-4646 ext. 1

1 www.DentalSleepSolutions.com
One of my mentors has
been Dr. Keith Thornton, inven-
tor of the TAP devices for ob-
structive sleep apnea (OSA). I
made my first TAP over 13 years
ago and estimate that I have
delivered more than 1,000 TAPs
since then, and it remains a key
part of my armamentarium. I
don’t use it for every patient,
but I find it is almost always at
the top of my list. It does a
fabulous job of treating moder-
ate to severe apnea. We have
multiple case studies now
where with the TAP we have
reduced Apnea Hypopnea In-
dexes (AHI) from 100 to below
10.
Regardless of efficacy, wearing
To Tripod or Not to Tripod.
a Mandibular Repositioning
Device (MRD) can be a chal-
lenge for some patients, and
part of that challenge is over-
coming side-effects. One po-
tential side-effect is ongoing
TM Joint issues. Sometimes it is
muscle, sometimes the joint
itself, sometimes both. Here
are a few clinical tips to ad-
dress ongoing joint pain and
generalized achiness in the
joint area.
First, determine if the pain is
unilateral or bilateral, acute or
chronic. Remember that doc-
umenting joint and TMJ dys-
function in DS3 beforehand is
ALWAYS a good idea! Also,
remember that we work in
three planes, NOT just the an-
terior posterior.
Unilateral Pain Make sure the TAP hits on-
ly in the anterior ar-
ea. Frequently, pain on just
one side is caused by an im-
balance from the device hit-
ting on only one side in the
posterior area. Typically the
side that is hitting is the side
that is hurting. Simply reduce
the posterior
thickness on
that side until
it no longer
touch-
es. You’ll see
this happen
more in pa-
By. Dr. Richard Drake
tients with a steep Curve of
Spee. Also check that the
advancement mechanism is
not misaligned, pulling the
patient too far to the right or
left as they protrude. Again,
the joint that is being restrict-
ed from moving is usually the
one that hurts. Lastly, sleep-
ing only on one side with a
hand under the face can
cause unilateral joint is-
sues. Consider tripod in all
of these cases as discussed
below.
Bilateral Pain Most often, pain on both
sides is caused from titrating
too far forward too
fast. Slow down. Back up a
bit. Utilize the Cl II hook on
the TAP 3 Elite. Check to
make sure there are no pos-
terior interferences as the
patient moves forward (just
like above). Consider add-
ing posterior stops so that
you “tripod” the TAP. It hits in
front on the advancement
mechanism as well as the
posterior R and L all at the
same time. You’ll want to
wait until you get close to
your treatment position to do
this, because further adjust-
ment forward means you’ll
have to adjust the posterior
segments every so often as
you titrate the MRD forward.
1.877.95.SNORE
SUMMARY
The joys of treating OSA successfully far outweigh the speed bumps, or
side effects, along the way. Having a few tricks up your sleeve to help
patients get over the speed bumps makes you a better doctor and helps
patients wear their devices and treat their apnea more successfully.
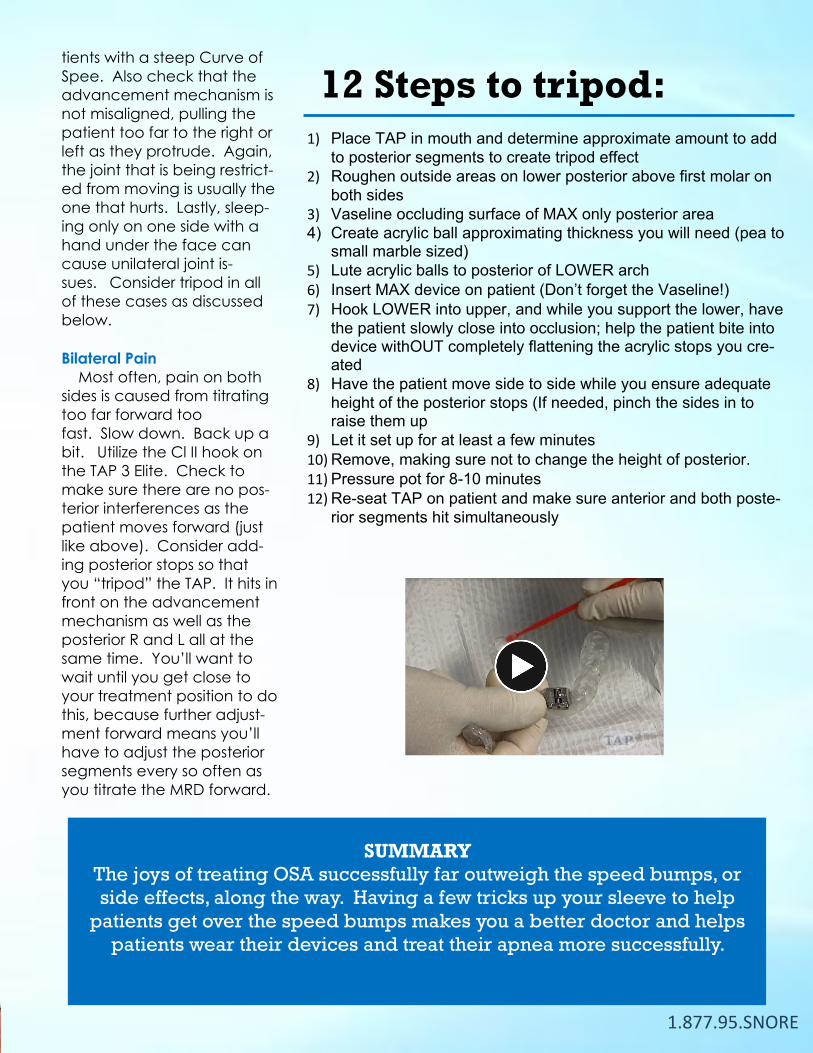
12 Steps to tripod:
1) Place TAP in mouth and determine approximate amount to add
to posterior segments to create tripod effect 2) Roughen outside areas on lower posterior above first molar on
both sides 3) Vaseline occluding surface of MAX only posterior area 4) Create acrylic ball approximating thickness you will need (pea to
small marble sized)
5) Lute acrylic balls to posterior of LOWER arch 6) Insert MAX device on patient (Don’t forget the Vaseline!) 7) Hook LOWER into upper, and while you support the lower, have
the patient slowly close into occlusion; help the patient bite into device withOUT completely flattening the acrylic stops you cre-ated
8) Have the patient move side to side while you ensure adequate
height of the posterior stops (If needed, pinch the sides in to raise them up
9) Let it set up for at least a few minutes 10) Remove, making sure not to change the height of posterior. 11) Pressure pot for 8-10 minutes 12) Re-seat TAP on patient and make sure anterior and both poste-
rior segments hit simultaneously

Dawson Academy
on the Oral-Systemic The D.I.S.H. The D.I.S.H. on the Dawson Institute of Systemic Health
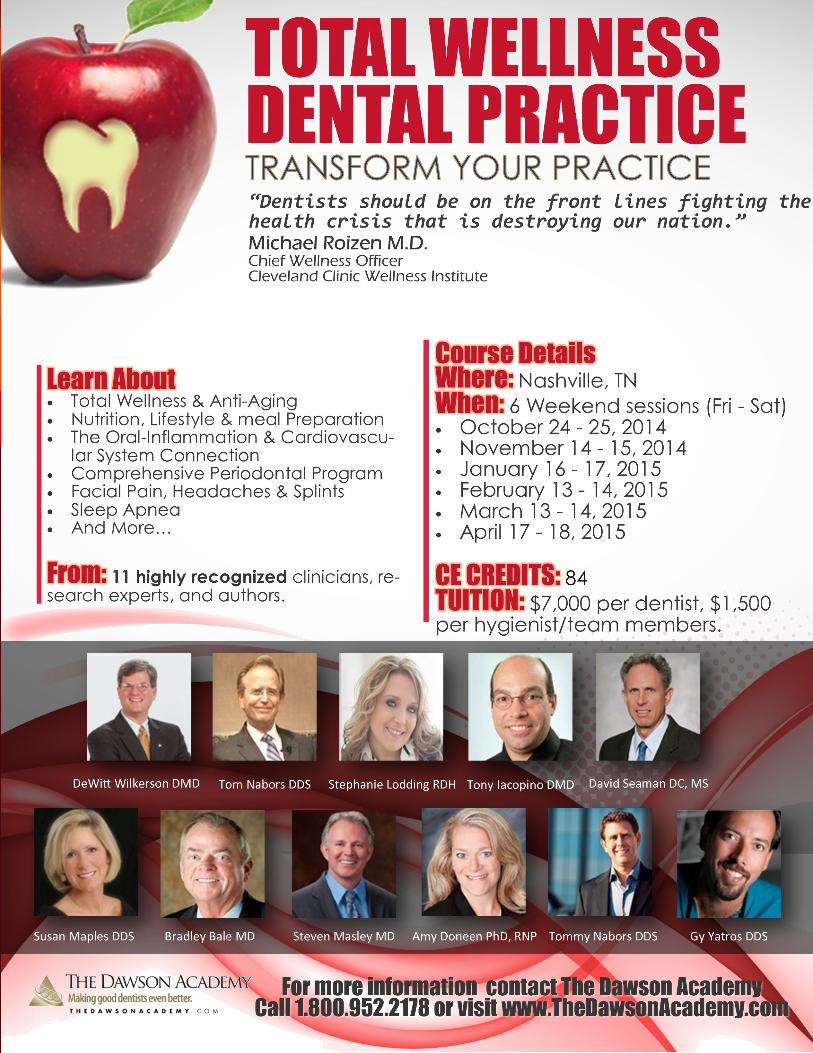
The Dawson Academy is pleased to bring the Total Wellness Dental Prac-tice seminar series to Brentwood, TN beginning in April, 2015. In 2012, we attended the second annual confer-ence of the American Academy for Oral Systemic Health (AAOSH). It was held at the Cleveland Clinic, featuring some of the top medical clinicians and researchers in the world on the sub-ject of total wellness. The meeting completely altered the way we view Dentistry. Michael Roizen M.D., Medi-cal Director of the Cleveland Clinic Wellness Institute, shared evidence proving that our nation will soon be bankrupt due to increasing healthcare costs, especially the cost of managing chronic diseases associated with met-abolic syndrome/obesity, diabetes, heart disease, dementia, physical in-activity, smoking, and stress. Accord-ing to Dr. Roizen, there will only be two options to manage this growing crisis: rationing of health care by the federal government and insurance companies, or the public gets smart, and we start taking responsibility for own health through personal lifestyle
By Dr. DeWitt Wilkerson
changes. Dr. Roizen pointed out that a large study showed that 89% of people with adult, type 2 diabetes can lower their blood sugar levels to within normal limits, without the use of medications, by imple-menting a few simple lifestyle changes. Recent DNA studies have also proven that lifestyle is more important to longevity and quality of life than is our genetic predispos-tion. He challenged dental teams to be on the frontlines fighting this battle that is destroying our nation, pointing out that we spend more time with our patients than any oth-er health professionals. We left the conference with an enlarged vision of Dentistry.
In April, 2015 The Dawson Academy will bring scholars, researchers, and clinicians, to the Mountain West Institute, personally training dental teams to expand their practice mis-sion to include total wellness screening, coaching, and therapy. Our newest course series, The Total Wellness Dental Practice, will assist dental teams to become patient ad-vocates for total health and gate-keepers of systemic inflammation. Systemic inflammation is the fire within that feeds accelerated aging, lowered energy levels, poor memory, chronic pain, and disease. Common causes are oral pathogenic bacteria in the bloodstream, sleep apnea, a pro-inflammatory western diet, physical inactivity, smoking, and stress. Dental teams can effec-tively address all these sources of chronic inflammation.
The participants in this course series will learn from noted authorities
including Bradley Bale MD, Steven Masley MD, DeWitt Wilkerson DMD, Tom Nabors DDS, Tony Iacopino DMD, Susan Maples DDS, David Seaman DC,MS, Stephanie Lodding RDH, and Gy Yatros DMD
Just some of the topics covered in the continuum include how to use salivary testing to guide antimicro-bial periodontal/systemic therapy; home sleep studies to guide screening and monitoring of treat-ment of obstructive sleep apnea; principles of prevention of diabe-tes, heart attacks, and strokes; ex-ercise physiology; stress manage-ment techniques; nutritional princi-ples; smoking cessation counseling; networking within the medical community, and many other princi-ples of Dental Medicine.
For more information contact the Dawson Academy, www.TheDawsonAcademy.com.
You are urged to accept the chal-lenge to create The Total Wellness Dental Practice in your own office. Wouldn’t it be wonderful, if in ad-dition to saving teeth, you could also save lives? We would be
thrilled to help you!
Dr. Wilkerson is Senior Faculty/Director of Dental Medicine for the Dawson Academy for Advanced Dental Study, in St. Petersburg, Florida. He is Past President of the American Equilibration Society and serves on the Board of Directors for the American Academy for Oral Systemic Health (AAOSH). He can be contacted at
www.DentalSleepSolutions.com

Contact: Cindy Herbert 877.95.SNORE
DENTALSLEEPSOLUTIONS.COM 1 5
From OSA, LSAT, & AHI to RDI, RERA, & OAT, DSM has an acronym for it. Two that dentistry has become increasingly con-cerned with are HIPAA (Health Insurance Portability & Accounta-bility Act) and HITECH (Health Information Technology for Eco-nomic and Clinical Health Act) which govern how patients’ health records are protected, maintained, and transmitted. Are you aware that every HIPAA violation is punishable by fines of $50k - $250k?!?! A recent Den-talTown article states, “These laws translate to a very real con-cern because the simple fact is that your Gmail account isn’t secure and Dropbox is a joke.
Every time we use these free and easy services to innocently com-municate with each other about anything having to do with a patient or a case, we’re in violation. Every single time we send or receive information is a new potential fine because of how the information is transmitted.” Fortunately, for DS3 Members, this is not a concern. DS3 is indeed a HIPAA & HITECH compliant EMR. It is the only dedi-cated dental sleep medicine soft-ware that meets these criteria. Stay ahead of the curve, avoid hefty fines, & contact me today to ensure that your DSM patient data is se-cure with DS3.
Contact: Brandie Havell 877.95.SNORE
BY DS3 SUPPORT SPECIALIST CINDY HERBERT
DS3 Members ask and want to
know: “How can we get more sleep patients?” It’s a common question we hear at Dental Sleep Solutions, and we spend a fair bit of our time brainstorming ideas to help you get more patients.
The lowest hanging fruit is your existing patient base who walk through your doors every day. You are screening your patients with the DS3 screener, right? Beyond that, we recommend that you cultivate re-lationships with local physi-cians. Office visits from a staff mem-ber who delivers business cards, practice brochures, and even referral forms are a great start. Even better if the Doctor will follow up with a visit himself. I recommend that you visit two offices every single week. A year later, 100 local physicians will at least know who you are. Quite often, after doing this, I would get a call from the office manager whom I had handed my brochures to. “Do you think you could help my husband not snore so much?” Absolutely! From humble beginnings I have seen doctors cre-ate significant and consistent referral sources. It is not rocket science but you have to put in the work and rest assured, it will pay handsomely. Many physician offices are open to
lunch and learns. Dr. Drake re-cently did one in San Antonio for a rather large ENT group. Their practice has seven physicians and a staff of 32. We brought box lunches from a local deli and pre-sented a 30 minute power point about how we could work together while they ate their sandwich-es. Two docs showed up and 29 staff members. Cost me less than $500 and a couple hours’ of time.
How long did it take to start getting referrals? Less than 24 hours!
Dental Sleep Solutions has pre-pared power points for our Mem-bers to utilize. You’ll need to cus-tomize them with your personal information, of course, as well as to the specific audience, but these power points can be a powerful tool to help you get more pa-tients. Start the conversation with how that particular specialist can help you. ENT’s, for example, we implore to help our patients breathe better through their nose. Once they know that you understand the referral process is a two way street, they are much more receptive to your message and more willing to refer patients
to you. Customize each one to the type of physician you are visiting.
PCP: Treating OSA will make patient’s healthier. Period. Across the board.
ENT: I need someone I can re-fer to who can increase nasal paten-cy, treat GERD, allergies
Cardiologist: We can help con-trol hypertension, A fib, V fib, coro-nary artery disease
Gastro / Endocrine / Nutrition-ists: We can help patients lose weight, better control GERD, better control glucose and insulin levels
Rheumatology: Patients who sleep better feel better and complain less Sleep docs / pulmonologists: Just throw me a bone, a crumb, a patient who refuses to wear PAP after a dozen different masks!
Screen your patient base
Office visits to physicians (two per week, 100 per year) Lunch & Learns (one per quarter, increase to one per month)
Contact me for a sample PowerPoint
that you can use when giving
Lunch & Learns
www.DentalSleepSolutions.com

1.877.95.SNORE
We need an ad

www.DentalSleepSolutions.com
MEMBER WHO’s WHO
of Metro Dental Sleep Medicine
Dr. Khalil, how long have you been practicing & have you always been in the St. Louis metropolitan area? I was actually born & raised in Ethiopia &
lived there until I finished high school. Then I em-
igrated to the U.S. & attended Wheaton in IL for
some undergrad courses & finished with a bache-
lors in chemistry at Indiana State. I got a master’s
of public health (MPH) at University of Illinois-
Chicago & then got my DMD at Washington Uni-
versity in 1983.
So, then after graduating from Wash U, you went into private practice? Not exactly. I did a general practice residency at
the VA in STL from ’83-’84 & then practiced in
Austin, TX for 1 year. I worked with the Elks Mo-
bile Dental Clinic for about 3 years treating handi-
capped kids & teenagers out of a mobile van all
across the eastern half of Missouri. Then I was on
faculty at Wash U. teaching general dentistry for 2 years before
I went into private practice in St. Louis about 1990. 25 years
now, gosh where has the time gone?
What sparked your interest in Dental Sleep Med-icine? 4 years ago I was diagnosed with OSA. My physician
told me I had moderate OSA & didn’t need CPAP & suggested
that a dental device might be a good idea. He asked if I could
make one myself & I said yes. I began attending a lot of sleep
CE. The MD said he needed a dentist nearby so I agreed to
open a dedicated sleep office in the same plaza. He also en-
couraged me to continue building my own referral network & I
started looking at DSM in a much more comprehensive way. I
recognized there were 3 major hurdles to overcome. The first is
the technical part of making devices which was actually rela-
tively easy. Secondly, was medical billing which required a
deep level of learning & persistence, & finally, building rela-
tionships with the gateway entry point of OSA which is the
diagnosing physicians.
Of the 3 hurdles you mentioned, which do you think is most significant? First of all, you can’t treat without a diagnosis but like
all of us, most physicians are very busy treating their patients
with tons of issues that may or may not be sleep-related. The
first hurdle is getting the MD’s to recognize the importance of
identifying & treating sleep disordered breathing, particularly
OSA. Secondly, they need to recognize that dentists can pro-
vide a legitimate, acceptable, & effective treatment option.
Lastly, it’s important to establish enough rapport & confidence
with MD’s to get them to regularly refer their OSA patients to
dentists for treatment with OAT.
How did you overcome this hurdle? To address the issue of awareness, I began treating
some of my existing dental patients & showed the few refer-
ring MD’s what outcomes of treatments were. The more they
saw positive results, the more confidence they had to continue
referring. This also built my confidence to begin going to other
physicians & sharing these results. I started going to MD’s
with no sleep experience. I’d ask them if they have ever heard
from a patient that they weren’t wearing their CPAP’s. Their
ears would perk up & they’d say, “I don’t know what to do, but
I would sure love to have an alternative.” I would suggest a
‘lunch and learn’ for their staff & I’d pick up their favorite
With DS3 Support Specialist Staci Holbrook
breakfast or lunch from wherever they’d want. I went
into a 4 physician group practice after having this dis-
cussion with them. I brought bagels and coffee for a
‘breakfast and learn.’ One doctor immediately recog-
nized in their patient base that people needed this &
within 24 hours he began referring patients. Then an-
other MD in that same office began referring shortly
after.
Secondly, I regularly send reports to MD’s
regarding pre/post treatment stats to show improve-
ment. I use the DS3 system because it keeps them in-
formed about our shared patients. This is one more
way to stay at the front of their mind. Lastly, I meet
with them to continue building rapport. I visit with
them for 5-10 minutes to discuss patient outcomes via
conference call, text, whatever. One MD I visited
over holidays told me ‘you almost killed 1 of my pts.’
I was taken aback & asked why. He said, “Your de-
vice helped him so much that he decided on his own
to stop taking his insomnia
meds so even though he was
breathing well, he still had in-
somnia. He fell asleep at the
wheel & his wife had to grab
the steering wheel. You
stopped his snoring &
treated his OSA but
his insomnia persists.”
To me, this highlights importance of multidisciplinary
approach & ongoing communication. As dentists, we
tend to focus so much on OSA and forget that it is
merely one of dozens of SDB classifications.
What tools can you not practice Dental Sleep Medicine without?
A diagnosis of OSA Clinical dental & TMJ
screening which I use DS3 for George Gauge & im-
pressions Good software. DS3 is the best to do it. I’ve
used others but it is far and above superior. It address-
es the biggest hurdle which is dealing with referring
MD’s with the well-written letters. Without that, you
are dead in the water. No SIGNIFICANT business-
person can live without their relationship with the
bank. The bank doesn’t care if you make or lose mon-
ey as long as you communicate with them. If you
keep them apprised of what is going on, good or bad,
they will work with you. It is frequently the same
with referring physicians. DS3 allows me to do this
by mailing or digitally faxing correspondence directly
from my software.
What impact has DSM had on your prac-tice, on your professional satisfaction, &
your stature within the medico-dental community? Speaking opportunities? Over past 4 years, I’ve gone from just begin-
ning & that year I treated about 40 patients. By the
end of 2013, I made 60 devices. In 2014, I made 163
devices, nearly a 300% growth rate. This has had a
huge personal & professional impact on me. I have
made a huge positive impact on many patients’ lives.
Professionally, I’ve tripled the income in my sleep
practice. We’ve grown exponentially & this has creat-
ed confidence that allows me to approach even more
MD’s to help treat this epidemic.
In this time, I’ve been asked to speak to sever-
al study clubs and other groups. I started the Midwest
Dental Sleep Medicine Study Club with some col-
leagues and learn more every day about emerging re-
search and how we can better improve patients’ lives.
Describe your DSM experience in 5 words? Enjoyable. Rewarding.
Meaningful. Profitable. Fulfilling.
How can others replicate your success?
You have to
make a paradigm shift
from treating teeth to the
connection of three seemingly disparate spheres.
Teeth, TMJ, & the airway. As dentists, we are well
trained in teeth, marginally well trained in evaluating
& treating the joints but the airway is foreign to us.
We write it off as something that ENTs & MD’s deal
with. We have to focus on airway first, TMJ second,
& teeth last. Until you make that shift, you are unlike-
ly to grow. We’ve been saving teeth, now we must
save lives.
To Contact Dr. Khalil
Dr. Saba Khalil 314.740.1395
1.877.95.SNORE
STAY TUNED FOR OUR FEBRUARY EDITION Devices Too Tight or Too Loose? Simple Techniques You Can Use to Avoid
Sending It Back to the Lab
Do You Really Need to Keep Your DSM Patient Records Separate from Your
Dental Records?
Medicare; To Be or Not to Be? We'll Answer the Question...
DS3 Member Who's Who with Dr. Stacey Layman
& Much, Much More!!!
The DS3 Team would like to wish you all a Happy & Fulfilling...







