Department of Thoracic/Head & Neck Medical Oncology
Management of EGFR-Mutant NSCLC Resistant to EGFR-TKI therapy
Anne S. Tsao, M.D.
Associate Professor
The University of Texas
MD ANDERSON
CANCER CENTER
Director, Mesothelioma Program
Director, Thoracic Chemo-XRT Program

EGFR mutations
Common mutationsMechanisms of resistance to EGFR TKIs
Outline: Long-term management EGFR mutated NSCLC patients
Current EGFR TKI Resistance Management
Oligo-metastatic disease resistance
Options: chemo chemo + EGFR TKI combination chemo then EGFR TKI chemo with intermittent EGFR TKI
Novel agents that target
EGFR pathway
AfatinibAfatinib-cetuximab for T790M
CO-1686
MetMAb (onartuzumab)Met inhibition

EGFR mutations
• Found in 10% - 15% of all lung cancer patients and 85% who clinically respond to EGFR TKIs
• Found more commonly in never-smokers, adenocarcinomas, BAC, women, Asians
• Predominantly located in EGFR exons 19 - 21
• EGFR mutations are not the same. There are sensitive mutations and acquired resistance mutations (T790M).
• 85% of EGFR mutations are either deletion exon 19 or L858 mutation.
Pao, Miller. J Clin Oncol. 2005;23:2556-2568; Wu et al. J Thorac Oncol. 2007;2:430-439.

12-00 12-02
Patient with EGFR mutation deletion exon 19

Newly diagnosed3-16-07
3 months of erlotinib6-18-07
Patient with L858 EGFR mutation
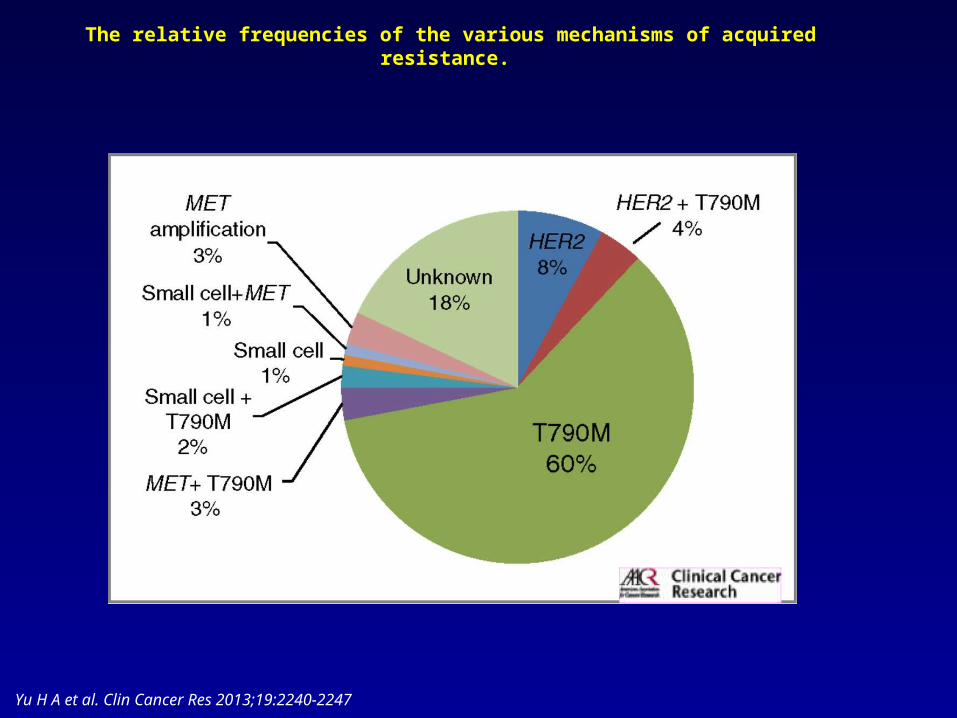
The relative frequencies of the various mechanisms of acquired resistance.
Yu H A et al. Clin Cancer Res 2013;19:2240-2247

EGFR T790M: Frequently Found inTumor Cells From Patients With Acquired Resistance
to EGFR TKIs
Pao W, et al. PLoS Med. 2005;2:e73; Balak MN, et al. Clin Cancer Res. 2006;12:6494-6501.

T790M blocks erlotinib binding and leads to a resistant phenotype
Michalczyk et al. Bioorganic & Medicinal Chemistry 16 (7): 3482; April 2008

EGFR mutations
Common mutationsMechanisms of resistance to EGFR TKIs
Outline: Long-term management EGFR mutated NSCLC patients
Current EGFR TKI Resistance Management
Oligo-metastatic disease resistance
Options: chemo chemo + EGFR TKI combination chemo then EGFR TKI chemo with intermittent EGFR TKI
Novel agents that target
EGFR pathway
AfatinibAfatinib-cetuximab for T790M
CO-1686
MetMAb (onartuzumab)Met inhibition
EGFR mutant on TKI develops oligometastatic PD
• Continue EGFR TKI • Utilize radiation therapy or surgical resection• Close monitoring
• Several studies demonstrate additional PFS benefit (6.2-10 months) and possibly OS (41 months) benefit with this strategy.
Weickhardt et al. JTO 7: 1807-1814, 2012; Yu et al. ASCO 2012 abstract 7527, JCO 30 , 2012

Weickhardt et al. JTO 7: 1807-1814, 2012
EGFR mutation and ALK mutation patients with oligo-progressive disease + local therapy have PFS benefit

EGFR Mutant Disease Progression on EGFR TKI
Molecular:-Unknown
(other pathways)-MET-PIK3CA-SCLC-HER2
Clinical PD appearance:
- Rapid disease PD globally-Slow growth globally-Growth in several areas, but not all

Flare of Disease after EGFR TKI discontinuation in acquired resistance
• Rapid disease acceleration leading to hospitalization and/or death after EGFR TKI cessation occurs in up to 23% (n=14) of patients in MSKCC series (n=61).
Riely et al. Clinical Cancer Research 2007, Chaft et al. CCR 17 (19): 6298-6303, 2011
Current Options in EGFR TKI resistant patient with EGFR mutation
Chemotherapy
Chemotherapy + EGFR TKI combination
Chemotherapy
Chemotherapy with intermittent EGFR TKI
EGFR TKI

Chemo is safeChemo then maintenance erlotinib is safe
Chemo + EGFR TKIs are safe
Chemotherapy
Chemotherapy + EGFR TKI combination
Chemotherapy
Chemotherapy with intermittent EGFR TKI
EGFR TKI SATURN
INTACT I, IITRIBUTE, TALENT
FAST ACT
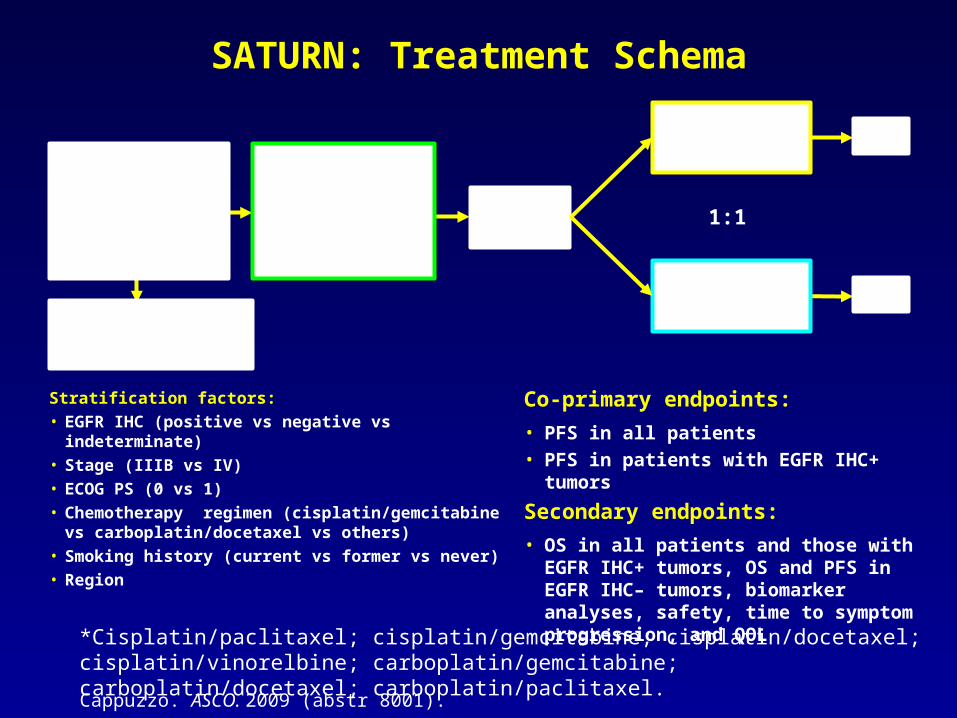
*Cisplatin/paclitaxel; cisplatin/gemcitabine; cisplatin/docetaxel; cisplatin/vinorelbine; carboplatin/gemcitabine; carboplatin/docetaxel; carboplatin/paclitaxel.
1:1
Chemotherapy-naïve advanced
NSCLCN=1949
No PDN=889
4 cycles of first-line platinum
doublet chemotherapy*
Placebo PD
Erlotinib150 mg/day
PD
Mandatory tumor sampling
SATURN: Treatment Schema
Stratification factors:
• EGFR IHC (positive vs negative vs indeterminate)
• Stage (IIIB vs IV)
• ECOG PS (0 vs 1)
• Chemotherapy regimen (cisplatin/gemcitabine vs carboplatin/docetaxel vs others)
• Smoking history (current vs former vs never)
• Region
Co-primary endpoints:
• PFS in all patients• PFS in patients with EGFR IHC+ tumors
Secondary endpoints:
• OS in all patients and those with EGFR IHC+ tumors, OS and PFS in EGFR IHC– tumors, biomarker analyses, safety, time to symptom progression, and QOL
Cappuzzo. ASCO. 2009 (abstr 8001).
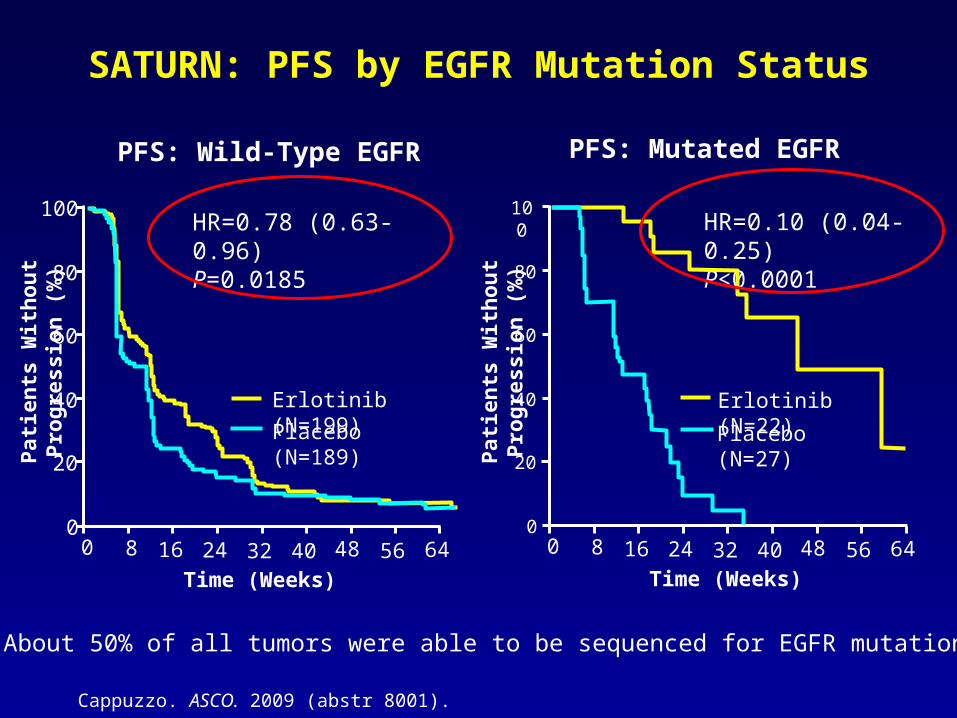
SATURN: PFS by EGFR Mutation Status
• About 50% of all tumors were able to be sequenced for EGFR mutation
Time (Weeks)
Pat
ien
ts W
ith
ou
t P
rog
ress
ion
(%
)
Pat
ien
ts W
ith
ou
t P
rog
ress
ion
(%
)
PFS: Wild-Type EGFR PFS: Mutated EGFR
HR=0.78 (0.63-0.96)P=0.0185
HR=0.10 (0.04-0.25) P<0.0001
0
20
40
60
80
100
0 8 16 24 32 40 48 56 640
20
40
60
80
100
Erlotinib (N=22)
Placebo (N=27)
Erlotinib (N=199)
Placebo (N=189)
Cappuzzo. ASCO. 2009 (abstr 8001).
Time (Weeks)
0 8 16 24 32 40 48 56 64

Chemo is safeChemo then maintenance erlotinib is safe
Chemo + EGFR TKIs are safe
Chemotherapy
Chemotherapy + EGFR TKI combination
Chemotherapy
Chemotherapy with intermittent EGFR TKI
EGFR TKI SATURN
INTACT I, IITRIBUTE, TALENT
FAST ACT

Continuing EGFR TKI +/- Chemo may have benefit
Trial PatientsContinued EGFR TKI +
chemo
Goldberg et al. 34 chemo + E44 chemo
RR improvedNo PFS or OS difference
Faehling et al. 27 chemo + EGFR TKI14 chemo
Improved OS
Yoshimura et al. 27 pemetrexed + EGFR TKI ORR 26%, DCR 78%Median PFS 7 months
Median OS 11.4 months
Delayed additional therapy
Oxnard et al. 42 EGFR TKI 45% > 3 months19% > 12 months
Goldberg et al. ASCO 2012 Abstract 7524, Yoshimura N. et al. JTO 8 (1):96-101, 2013; Faehling et al. ASCO 2012 Abstract 7572; Oxnard et al. ASCO 2012 Abstract 7547
ASPIRATION Phase II Asian multicenter trial for NSCLC EGFR mutation patientsusing continuation erlotinib beyond PD1
Enrollment: April 2011 – Dec 2014 Plan 207 patients

2 Trials to compare ongoing EGFR TKI for Acquired Resistance

Chemo is safeChemo then maintenance erlotinib is safe
Chemo + EGFR TKIs are safe
Chemotherapy
Chemotherapy + EGFR TKI combination
Chemotherapy
Chemotherapy with intermittent EGFR TKI
EGFR TKI SATURN
INTACT I, IITRIBUTE, TALENT
FAST ACT

Potential Antagonism Chemo + EGFR TKI
• There are concerns over combining erlotinib-chemo as erlotinib arrests the cancer cells in the G1 checkpoint and chemo usually works best in the mitotic phase.
Solit et al, Clin Can Res 2005; Davies A et al. CLC 7 (6): 385-388, 2006; Encyclopedia of Science Cell Biology http://www.daviddarling.info/encyclopedia/C/cell_cycle.html

First-Line Asian Sequential Erlotinib plus chemo Trial (FASTACT)
1:1
Untreated NSCLC IIIB/IVNo prior EGFR
TKI
Platinum (d1) Gemcitabine (d1, 8)
+ PlaceboD15-28 Q4weeks
x 6 cycles
Placebo
Platinum (d1) Gemcitabine (d1, 8)
+ ErlotinibD15-28 Q4weeks
x 6 cycles
Erlotinib
1o endpoint: 8-week non-PD rate2nd: PFS, 16-week non-PD rate, ORR, TTP, OS
Lee J et al. ASCO 2012 Abstract 8031
n=154

FAST ACT 1 PFS favored GC-erlotinib
Lee J et al. ASCO 2012 Abstract 8031
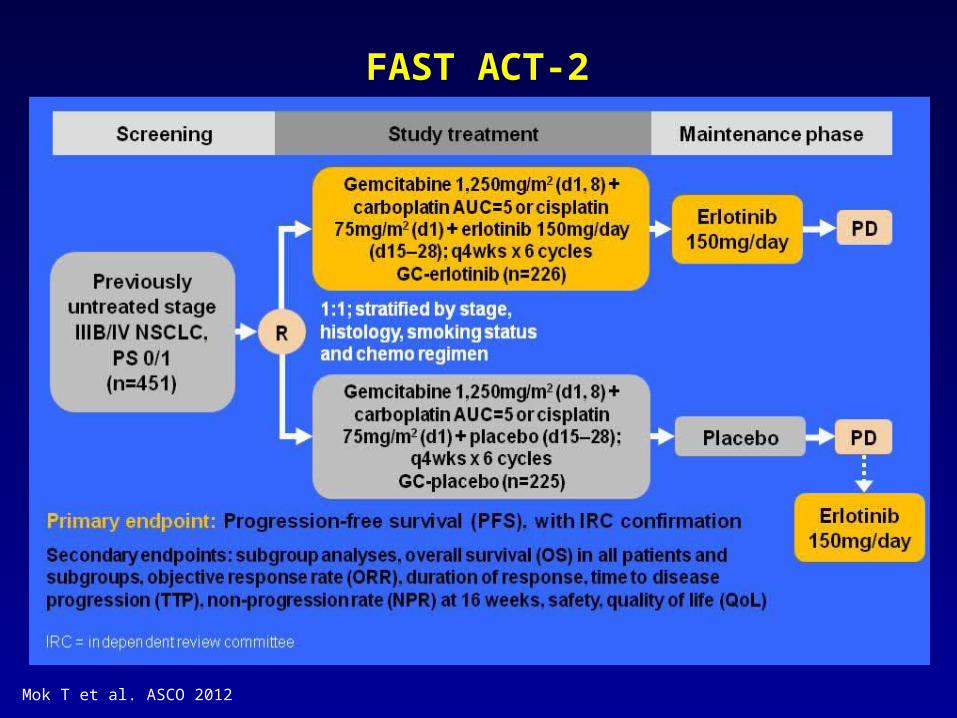
FAST ACT-2
Mok T et al. ASCO 2012

Mok T et al. ASCO 2012
FAST ACT II: ITT PFS favors erlotinib-GC
Critique: •FAST ACT 2 has a maintenance portion with the EGFR TKI and this affects clinical outcomes
• SATURN maintenance trial proves PFS benefit in EGFR mutant patients
Tsao Summary on Acquired Resistance
• For local oligo-PD, continue EGFR TKI and apply local therapy.
• For more global PD: 4 options until future trials elaborate on acquired resistance– Chemo
– Chemo + EGFR TKI
– Chemo then EGFR TKI
– Chemo intercalated with EGFR TKI
• Ultimately – Re-biopsy and molecular profile will determine the optimal therapy

EGFR mutations
Common mutationsMechanisms of resistance to EGFR TKIs
Outline: Long-term management EGFR mutated NSCLC patients
Current EGFR TKI Resistance Management
Oligo-metastatic disease resistance
Options: chemo chemo + EGFR TKI combination chemo then EGFR TKI chemo with intermittent EGFR TKI
Novel agents that target
EGFR pathway
AfatinibAfatinib-cetuximab for T790M
CO-1686
MetMAb (onartuzumab)Met inhibition

Novel agents targeting EGFR TKI resistant disease
Agent Inhibitor type Preclinical benefit against T790M
Clinical Trial phase
Dacomitinib(Pfizer)
Irreversible TKI of EGFR, HER2, HER 4
yes II, III
Afatinib(Boehringer Ingelheim)
Irreversible TKI of EGFR, HER2, HER4
yes II, III
CO-1686(Clovis)
Selective covalent inhibitor EGFR mutations
yes I/II (T790M selection)
AZD9291 Irreversible TKI to mutant EGFR
yes I
Onartuzumab(Genentech)
Monoclonal antibody that targets MET receptor
n/a II, III
Tivantinib (ArQule) MET-R TKI n/a II, III
Volitinib (AZ) cMET TKI n/a I
Ariad 26113 EGFR, ALK, ROS1 I

[TITLE]
Yang et al. ASCO 2012 Abstract LBA7500

Yang et al. ASCO 2012 Abstract LBA7500
Phase III Lung LUX-3 Trial
1269 screened, 452 EGFR mutation (+) => 345 randomized

[TITLE]
Yang et al. ASCO 2012 Abstract LBA7500

ORR favored afatinib
Yang et al. ASCO 2012 Abstract LBA7500
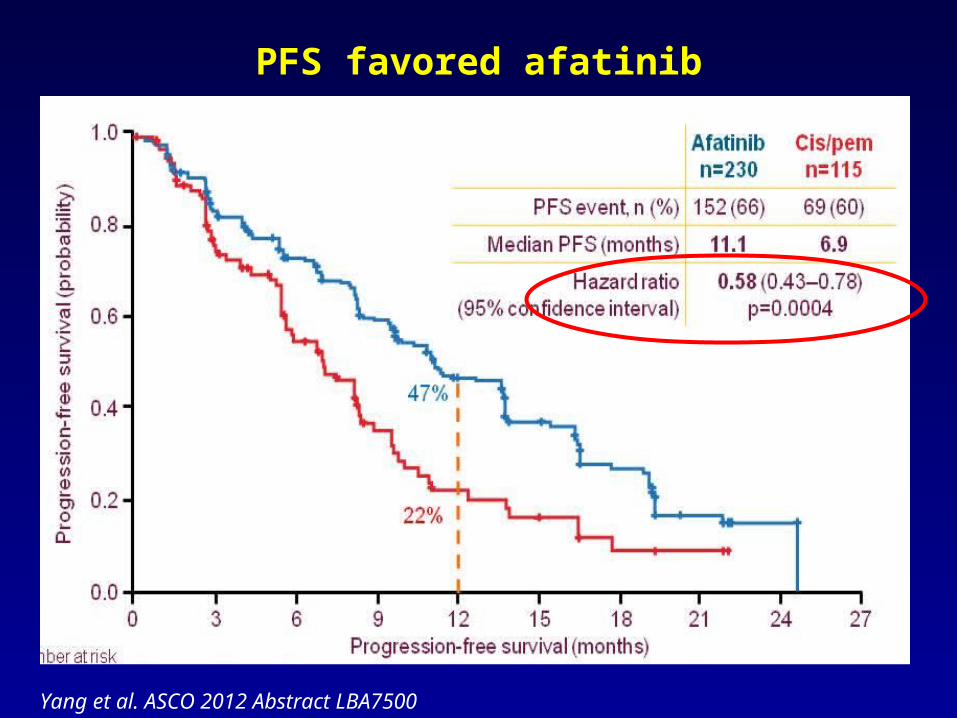
PFS favored afatinib
Yang et al. ASCO 2012 Abstract LBA7500
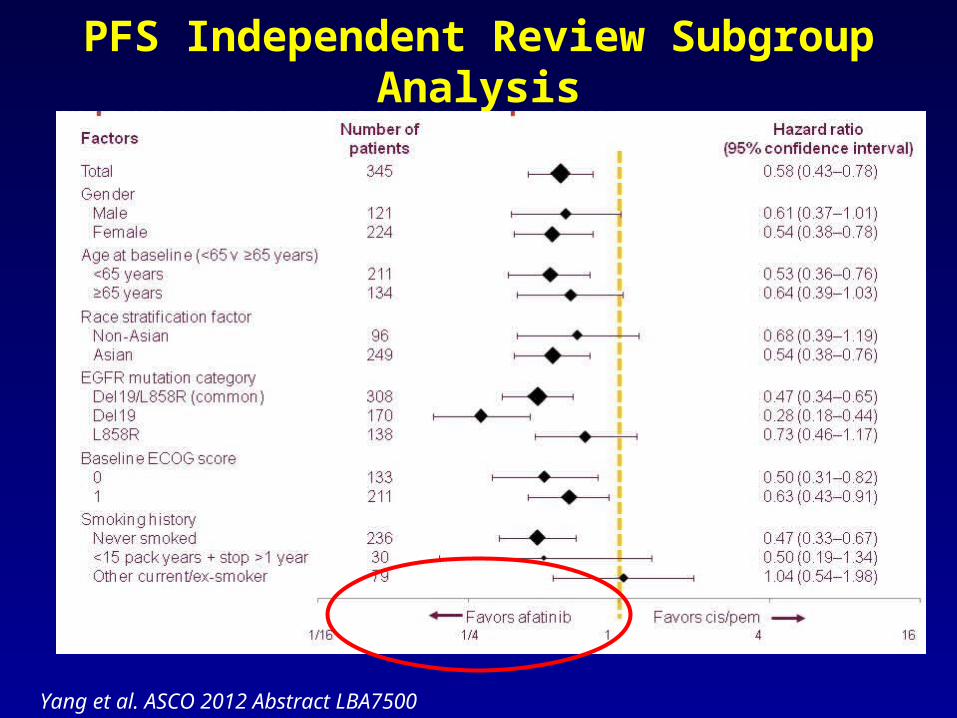
PFS Independent Review Subgroup Analysis
Yang et al. ASCO 2012 Abstract LBA7500

PFS Common Mutants (Del 19/L858R)
Yang et al. ASCO 2012 Abstract LBA7500
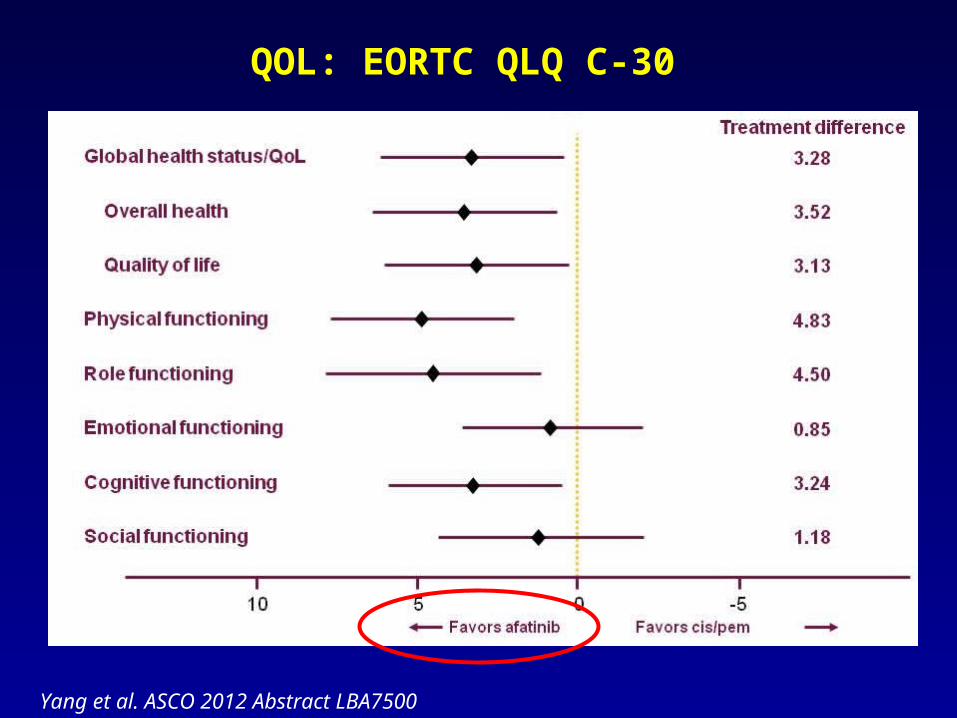
QOL: EORTC QLQ C-30
Yang et al. ASCO 2012 Abstract LBA7500

Summary LUNG LUX-3
• Front-line afatinib improved QOL, RR, DCR, and median PFS over cisplatin-pemetrexed in both the overall EGFR mutation population and in the common EGFR mutation (del19/L858) patients.
• Subgroup analysis showed benefit across most of the subgroups.
• No new safety signals with diarrhea and rash as the most frequent AEs.
Yang et al. ASCO 2012 Abstract LBA7500

• Afatinib was approved July 12, 2013 by the FDA for first-line NSCLC patients with EGFR mutations (del exon 19 and exon 21 L858R) as detected by an FDA-approved assay.
• It remains unknown which EGFR TKI (erlotinib, gefitinib, or afatinib) should be used first or whether these agents can be sequenced in the EGFR mutation population.
• Additional studies are needed to clarify this issue.
• Afatinib is currently under development in combination with cetuximab for resistant EGFR T790 mutant patients.
• Future more broad application of afatinib is anticipated.
Summary Afatinib

Regales et al. JCI 2009
Combination of Afatinib and Cetuximab is effective against EGFR T790M

Afatanib/Cetuximab
• No DLTs at afatinib 40mg po daily plus cetuximab 250 mg/m2 or 500mg/m2 IV q2 weeks
• Expansion cohort dosing: afatinib 40mg po daily + cetuximab 500mg/m2 IV q2 weeks
• Data on the first 100 patients available
Lynch, T. IASLC Targeted Therapies Meeting Feb 2013; Janjigian, et al. ESMO 2012

Responses at MTD by T790M mutation
Lynch, T. IASLC Targeted Therapies Meeting Feb 2013; Janjigian, et al. ESMO 2012

Eligibility:•Recurrent or advanced NSCLC•Sensitizing EGFR mutation (i.e., exon 19 deletion, L858R)•Chemotherapy and TKI-naïve•PS 0-2
Afatinib PO 40mg daily
+Cetuximab
IV 500mg/m2 Q2 weeks
N=138
Afatinib PO 40mg daily
N=138
Primary Endpoint:Progression-Free Survival
Secondary Endpoints:ORR, OS, Safety, Tolerability, QOL
Exploratory Biomarkers:Pre-and post-Rx T790M testing, whole exome sequencing, HER2 and MET FISH
Initial Evaluation:PET-CT Brain CT or MRI ECG, Echo/MUGA Tumor molecular analysis
CT scans q8 wks
A randomized phase II/III trial of afatinib plus cetuximab versus afatinib alone in treatment-naïve patients with advanced, EGFR mutation positive NSCLC
Lynch, T. IASLC Targeted Therapies Meeting Feb 2013

CO-1686 is a novel TKI specifically targeting mutated EGFR
• Novel, oral, selective covalent inhibitor of EGFR mutations in NSCLC• Inhibits key activating and T790M resistance mutations• Minimal activity against wild type EGFR
• First-in-human study ongoing in EGFR-mutation positive pts with recurrent advanced NSCLC, started with free base capsule formulation, hydrobromide salt form of CO-1686 with improved drug availability and reduced variability completed dose escalation.
• Early evidence of efficacy presented at ASCO 2013, WCLC 2013, free base dosed to 900 mg BID
• Roche Molecular Systems companion diagnostic collaboration• Potential for use as first-line therapy
Modified from Soria WCLC 2013

Phase I Schema
Dose 1 (n=3)
Phase IIExpansion Phase
Dose 2 (n=3)
Dose 4 (n=3)
Dose 6 (n=6)
Dose 5 (n=3-6); MTD
Dose 3 (n=3)
40 T790M pts
Target Exposure
45
Phase 2 Cohort A-T790M : 1. Disease progression while on treatment with EGFR-directed therapy. Prior CT including intervening CT before planned initiation of CO-1686, is allowed (washout for EGFR TKI min 3 days, chemo 14 d)Phase 2 Cohort B-T790M 1. Disease progression while on treatment with the first single agent EGFR-directed therapy within the last 30 days, with no intervening treatment before planned initiation of CO-1686 .
92 patients will be enrolled into Phase 1 (57 on CO-1686 free base and approximately 35 on CO-1686 HBr).
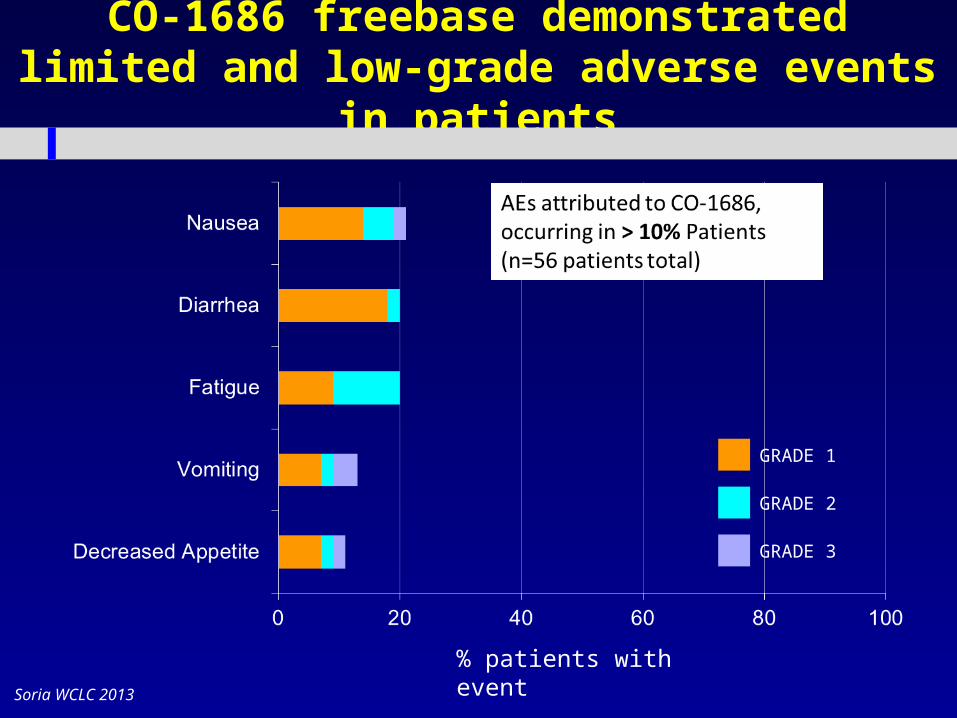
CO-1686 freebase demonstrated limited and low-grade adverse events in patients
GRADE 1
GRADE 2
GRADE 3
% patients with eventSoria WCLC 2013

*
67% RECIST response rate in evaluable T790M+ patients treated at 900mg BID
EGFRi immediately before CO-1686 *
1 2 2 2 4 2 2 1 1
Weeks on treatment
******
*
Number of Previous EGFR TKI
lines
6
22 15 1824 11 8 21 30
8 of 9 patients progressed on TKI immediately prior to CO-1686
*
Soria WCLC 2013
Promising clinical activity observed with
CO-1686 – no evidence of WT inhibition• 67% RECIST response rate in evaluable T790M+
patients treated at 900mg BID (free base)
• A hydrobromide (HBr) formulation of CO-1686 with improved exposure has been introduced and a RP2D of 750mg BID has been identified
• CO-1686 is well tolerated with no acneiform rash, consistent with absence of WT-EGFR inhibition• AEs all grades: nausea-25%, fatigue-21%, impaired glucose
tolerance/hyperglycemia 21%
• The pivotal phase 2/3 TIGER program starts 1H14• Efficacy updates at ELCC2014 and ASCO2014
Modified from Soria WCLC 2013

CO-1686 phase 2/3 development: TIGER program
TIGER: Third-generation Inhibitor of mutant EGFR in lung cancER All are global studies in mutant EGFR NSCLC:
− TIGER1: Phase 2/3 randomized registration study in newly-diagnosed patients (vs. erlotinib)
− TIGER2: Phase 2 registration study in 2nd line T790M+ patients directly progressing on first TKI
− TIGER3: Phase 2 registration study in later-line T790M+ patients, progressing on second or later TKI or subsequent chemotherapy
− TIGER4: Phase 2 study in 2nd or later-line patients with T790M detected with a blood/plasma assay
− TIGER5: Phase 3 randomized confirmatory study in 2nd or later-line patients (vs. chemo)

EGFR mutations
Common mutationsMechanisms of resistance to EGFR TKIs
Outline: Long-term management EGFR mutated NSCLC patients
Current EGFR TKI Resistance Management
Oligo-metastatic disease resistance
Options: chemo chemo + EGFR TKI combination chemo then EGFR TKI chemo with intermittent EGFR TKI
Novel agents that target
EGFR pathway
AfatinibAfatinib-cetuximab for T790M
CO-1686
MetMAb (onartuzumab)Met inhibition

ASCO 2011 Abstract #7505 MetMab Onartuzumab
Met activation is implicated in resistance to erlotinib/gefitinib in pts with activating EGFR mutations.
Met expression is associated with a worse prognosis in NSCLC
MetMab is an anti-Met one-armed antibody that inhibits hepatocyte growth factor (HGF)-mediated activation
Spigel et al. ASCO 2011 Abstract 7505
MetMAb
Met
HGF HGF
Met
GrowthMigrationSurvival
Noactivity

Spigel et al. ASCO 2011 Abstract 7505
Abstract #7505 Phase II Onartuzumab

Met IHC Biomarker
Spigel et al. ASCO 2011 Abstract 7505
“Met Diagnostic Positive” = >50% tumor cells with moderate or strong staining intensity93% had adequate tissue for analysis and 52% were “Met Diagnostic Positive”

Spigel et al. ASCO 2011 Abstract 7505
MetMAb + erlotinib in ITT
PFS HR 1.09OS HR 0.8
Spigel et al. ASCO 2011 Abstract 7505
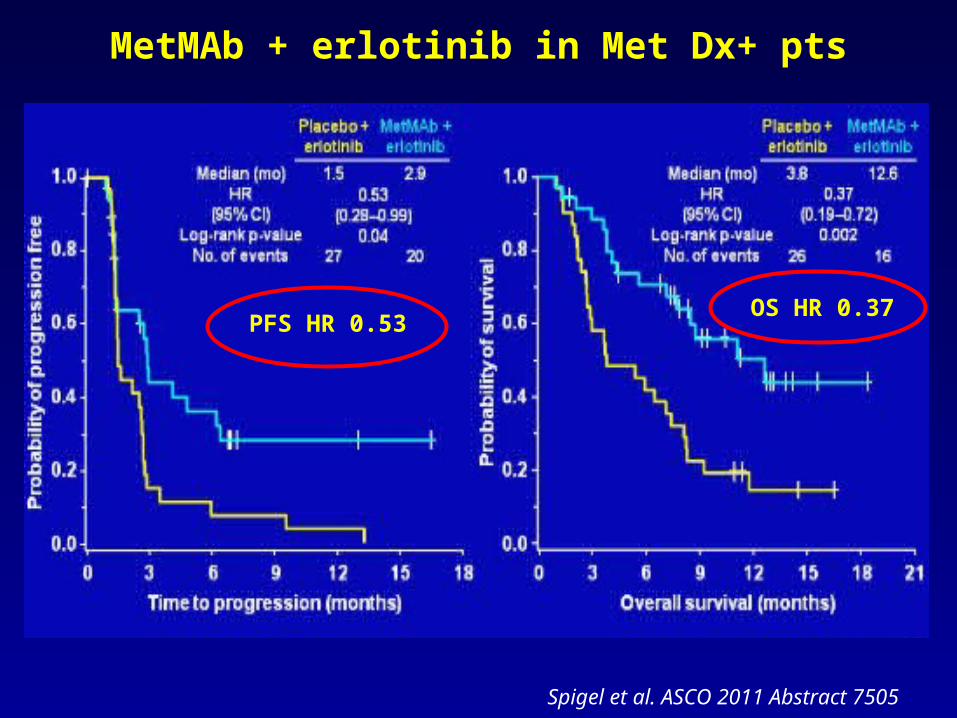
MetMAb + erlotinib in Met Dx+ pts
PFS HR 0.53OS HR 0.37

Spigel et al. ASCO 2011 Abstract 7505
MetMAb + erlotinib in Met Dx- pts
PFS HR 1.82OS HR 1.78
Spigel et al. ASCO 2011 Abstract 7505
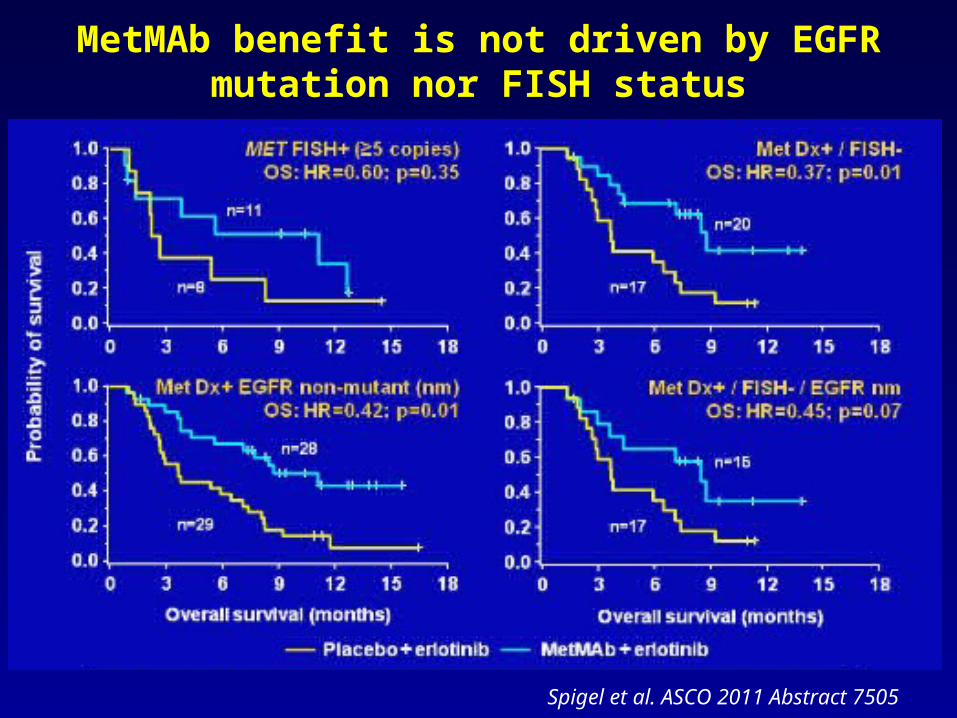
MetMAb benefit is not driven by EGFR mutation nor FISH status

Spigel et al. ASCO 2011 Abstract 7505
PFS HR 1.71
OS HR 2.61
Met expression correlates to worse outcome in erlotinib + placebo treated pts.

Spigel et al. ASCO 2011 Abstract 7505
Most commonly reported AE frequency > 10%

Phase II
• Met IHC expression inversely correlates with prognosis.
• MetMAb + erlotinib was well-tolerated with no new safety signals.
• MetMAb + erlotinib improved PFS and OS in Met Diagnostic Positive patients.
• A phase III study of MetMAb + erlotinib in Met Diagnostic positive patients started enrollment January 2012 and has completed accrual.

Tsao Conclusions on Clinical Management for EGFR mutation patients with Acquired Resistance
Feb 2013
Oligo-PDContinue EGFR TKI +
localized therapy
Global PD
Chemo
Chemo then EGFR TKI
Chemo + EGFR TKI
Chemo intercalated with EGFR TKI

Tsao Conclusions: Molecular Age Will Come
Molecular Rebiopsy:-Unknown
(other pathways)-MET-PIK3CA-SCLC-HER2
Sequist L et al. Sci Transl Med 2011;3:75ra26-75ra26
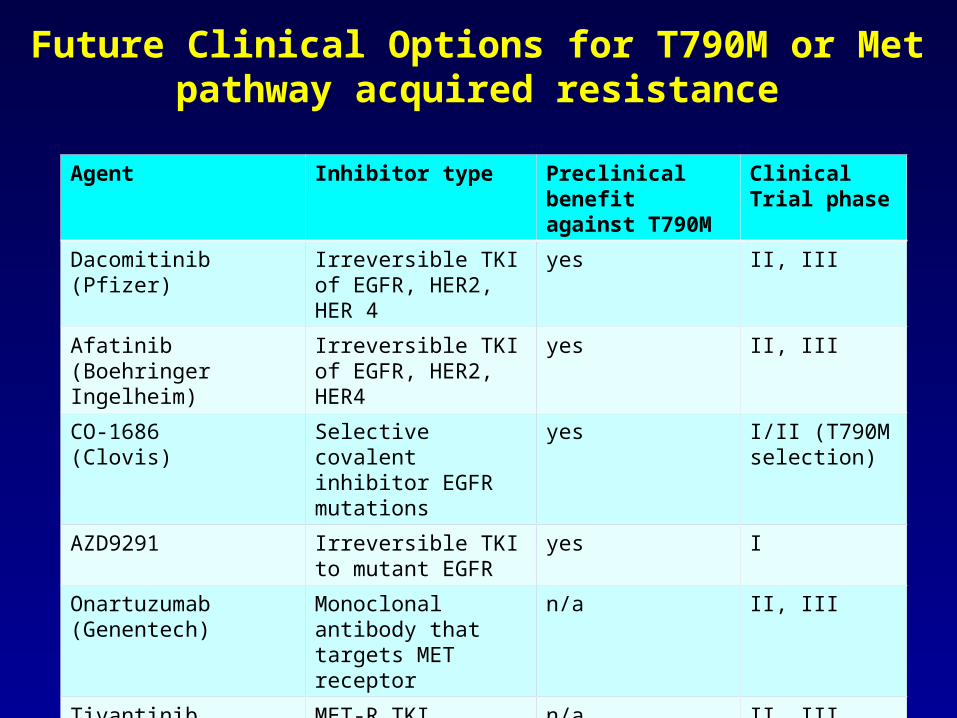
Future Clinical Options for T790M or Met pathway acquired resistance
Agent Inhibitor type Preclinical benefit against T790M
Clinical Trial phase
Dacomitinib(Pfizer)
Irreversible TKI of EGFR, HER2, HER 4
yes II, III
Afatinib(Boehringer Ingelheim)
Irreversible TKI of EGFR, HER2, HER4
yes II, III
CO-1686(Clovis)
Selective covalent inhibitor EGFR mutations
yes I/II (T790M selection)
AZD9291 Irreversible TKI to mutant EGFR
yes I
Onartuzumab(Genentech)
Monoclonal antibody that targets MET receptor
n/a II, III
Tivantinib (ArQule) MET-R TKI n/a II, III
Volitinib (AZ) cMET TKI n/a I
Ariad 26113 EGFR, ALK, ROS1 I



![Suppression of Mig-6 overcomes the acquired EGFR-TKI ......chromosome 1p36 [19]. Mig-6 expression is induced by EGFR signaling via the RAS-MAPK pathway, as well as other mitogenic](https://cdn.vdocument.in/doc/165x107/6142a51db7accd31ec0ed536/suppression-of-mig-6-overcomes-the-acquired-egfr-tki-chromosome-1p36-19.jpg)



