
Dept Social Medicine
Researchers interacting with Researchers interacting with Policymakers, Managers Policymakers, Managers
and Professionalsand Professionals
Niek KlazingaLimerick, August 31, 2007

Dept Social Medicine
• What is Health Services / Systems Research?
• Who wants to know what and why?
• Examples
• General conclusions

Dept Social Medicine
Definition IoMDefinition IoM• Health Services Research is a multidisciplinary field of inquiry,• basic and applied,• that examines the use, costs, quality, accessibility, delivery, organization, financing and outcomes of health care• to increase the knowledge and understanding of the structure, processes and effects of health services• for individuals and populations
Field and Lohrs 1995 JECP

Dept Social Medicine
Health Services Research is the multidisciplinary field of scientific investigation that studies how social factors, financing systems, organizational structures and processes, health technologies, and personal behaviours effect access to health care, the quality and cost of health care and ultimately our health and well-being.
Lohr, Steiwachs 2002

Dept Social Medicine
Health Services Research Health Services Research a working modela working model
• describe health services in terms of structure, process, outcome
• consider medical practice (health services) as one determinant of health status together with genotype, social and physical environment and behaviour
• examples studies of structure (manpower, organization, financing) studies of structure and process (influence insurance system on use) studies of structure and outcome (mortality in teaching/non teaching hospitals) studies of process (appropriateness hospitalization) studies of process and outcome (compliance and symptoms) studies of outcome
Starfield 1973 NEJM

Dept Social Medicine
What is Health Services What is Health Services Research?Research?
• Systematic way of knowledge production
• Valid knowledge• Generalizable knowledge• Applicable knowledge• Focused on functioning of health care
services and health systems

Dept Social Medicine
Types of questions in HSRTypes of questions in HSR
• Descriptive questions• Explorative questions• Testing questions• Instrumental questions• Theoretical interpretative
questions

Dept Social Medicine
Methods in HSRMethods in HSR• Literature study• Interviews, observations, focus
groups• Questionnaires• Case studies• Trend analyses / cohorts• Pre-post studies• Case-control studies• Quasi-experimental design• RCT

Dept Social Medicine
OBJECT OF STUDYOBJECT OF STUDY
• Organisation
• Process
• Intervention
• Outcomes

Dept Social Medicine
THEORETICAL PERSPECTIVESTHEORETICAL PERSPECTIVES
• Quality of Care
• Managerial / Administrative
• Innovation / Change
• Learning organization
• Professionalization theory

Dept Social Medicine
EVALUATION RESEARCHEVALUATION RESEARCH
• Experimental
• Economic
• Managerial
• Developmental
Øvretveit 1998
Dept Social Medicine
Interaction with policymakers,Interaction with policymakers,managers and professionals on:managers and professionals on:
• research goals
• research design
• data-collection
• reporting
Dept Social Medicine
Example Dutch PerformanceExample Dutch Performance
Framework for the Health SystemFramework for the Health System
2002 - 20072002 - 2007
Dept Social Medicine
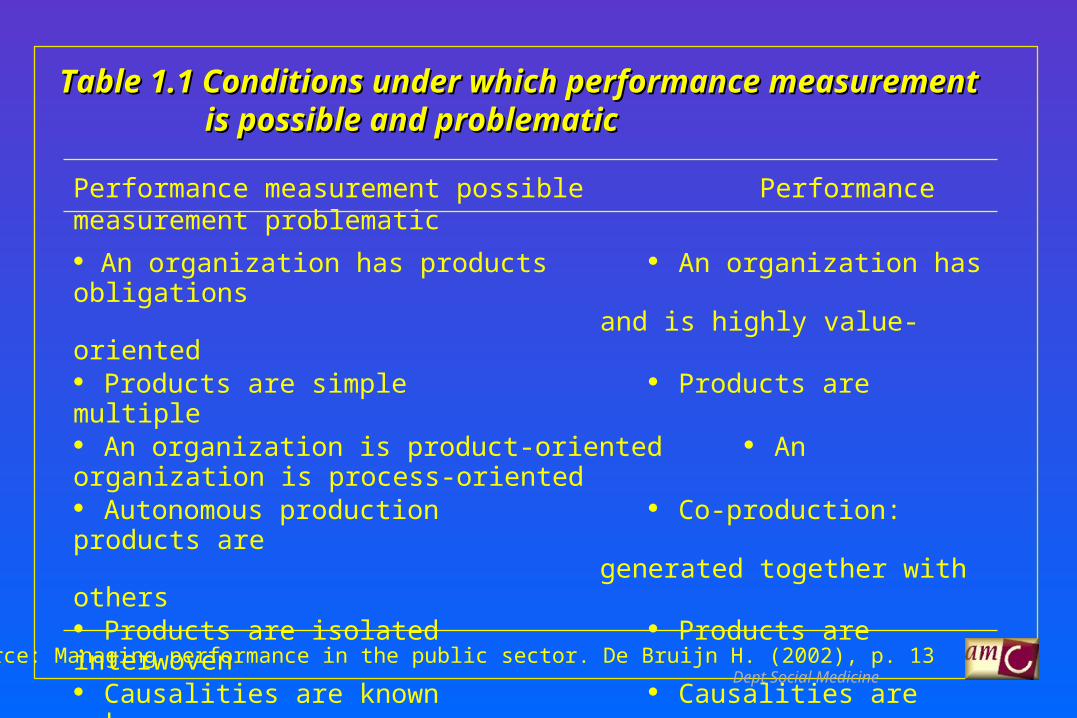
Table 1.1 Conditions under which performance measurementTable 1.1 Conditions under which performance measurement is possible and problematicis possible and problematic
Performance measurement possible Performance measurement problematic
An organization has products An organization has obligations
and is highly value-oriented Products are simple Products are multiple An organization is product-oriented An organization is process-oriented Autonomous production Co-production: products are
generated together with others Products are isolated Products are interwoven Causalities are known Causalities are unknown Quality definable in Quality not definable in performance indicators performance indicators Uniform products Variety of products Environment is stable Environment is dynamic
Source: Managing performance in the public sector. De Bruijn H. (2002), p. 13

Dept Social Medicine
Dutch Performance FrameworkDutch Performance Framework
• start policy process• functions• conceptual choices• indicator development• interaction researchers, policy makers and the health care field

Dept Social Medicine
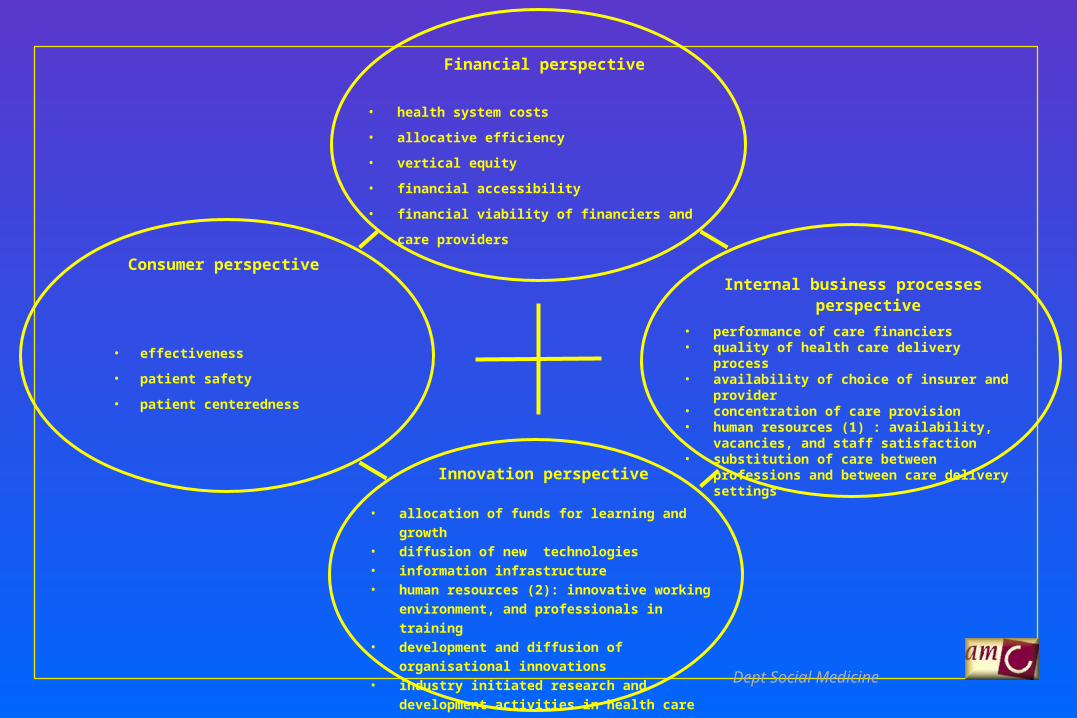
Financialperspective
Consumerperspective
Innovationperspective
Internal businessprocessesperspective
HealthHealth Care: prevention, cure,care and welfare
Lifestyle
Population Healthinformation Management information
Lalonde-modelLalonde-model Balanced scorecardBalanced scorecard
Geneticlayout
Environmentfactors
Performance:
Dept Social Medicine
Internal business processes perspective
• performance of care financiers• quality of health care delivery process• availability of choice of insurer and provider• concentration of care provision• human resources (1) : availability, vacancies,
and staff satisfaction• substitution of care between professions and
between care delivery settings
Consumer perspective
• effectiveness
• patient safety
• patient centeredness
Innovation perspective
• allocation of funds for learning and growth• diffusion of new technologies• information infrastructure• human resources (2): innovative working
environment, and professionals in training • development and diffusion of organisational
innovations• industry initiated research and development
activities in health care
Financial perspective
• health system costs
• allocative efficiency
• vertical equity
• financial accessibility
• financial viability of financiers and care providers

Dept Social Medicine
Lessons learnedLessons learned
• phases of conceptualization, ownershipand execution
• link with health care reforms• link with sectoral organization of the
department of health• link with information policies• link with accountability agenda• link with international developments

Dept Social Medicine

Dept Social Medicine
HEALTH How healthy are the Dutch?
NON-HEALTHCARE DETERMINANTS OF HEALTHAre the non-healthcare factors that also determine health as well as if/how healthcare is
used changing favorably?
HEALTH SYSTEM DESIGN AND CONTEXTWhat are the important design and contextual information that may be specific to the Dutch health system and which are
necessary for interpreting the quality of healthcare?
E
Q
U
I
T
Y
End-of-life care
Living with illness or disability
Getting better
Staying healthy
AccessibilityPatient-centeredness
SafetyEffectiveness
Healthcare Needs
Cost AccessQuality
Dimensions of Healthcare Performance
HEALTHCARE SYSTEM PERFORMANCEHow does the healthcare system perform? What is the level of care across the range of patient care needs? What does this
performance cost?
Efficiency(Value for money)

Dept Social Medicine
System goals (3)
Indicatordomains (15)
Indicators (125)
Keyfindings (120)
Summary
State Dutch Health CareState Dutch Health Care
A
B
Dept Social Medicine
Accessibility
• Freedom of choice • Waiting times• Accessibility in line with demand• Financial barriers for citizens• Concentration of supply• Development of health care professions
Quality:
• Effectiveness• Safety • Consumers and patient satisfaction• Accreditation• Innovation
Financial sustainability
• Development of macro costs• Monitoring the market• Productivity• Financial position of health care suppliers
Main performance fields from a macro Main performance fields from a macro perspectiveperspective

Dept Social Medicine
Chapter 2. Quality
2.2 Effectiveness of preventionPercentage of (adolescent) smokers
Percentage of (adolescent) people with overweightLevel of participation in population surveys and screenings
Vaccination rate (National Vaccination Programme (RVP), influenza vaccination, hepatitis B)Percentage of patients with diabetes with good glucose control
Effectiveness of lifestyle advice in primary carePercentage of schools that offer effective lifestyle programmes
Percentage of employers (companies) with an occupational health policyHealth protection: consumers’ trust in food safety, emergency treatment of home accidents and an indicator for medical assistance in accidents and disasters
Percentage of high-risk youth that is reached by adolescent health carePercentage of deprived areas with an intersectoral approach to health (no information available)
Perinatal mortality2.3 Effectiveness of cure
Percentage of cases in which general practitioners do not prescribe medicines they are advised against to prescribe for a particular syndromePercentage of cases in which general practitioners prescribe medicines that are advised for a specific syndrome
Percentage of cases in which general practitioners prescribe according to guidelinesPercentage of referrals by general practitioners to medical specialists
Percentage of referrals by general practitioners to other primary care workers In-hospital mortality for heart failureIn hospital mortality for pneumonia
In-hospital mortality for bypass surgeryHospital Standardized Mortality ratio
30-days mortality following acute myocardial infarction30-days mortality following stroke
Asthma mortality per 100,000 people aged 5-39Breast cancer mortality per 100,000 womenColon cancer mortality per 100,000 people
Cervical cancer mortality per 100,000 womenBreast cancer 5-year survival rateColon cancer 5-year survival rate
Cervical cancer 5-year survival ratePercentage of (over) 65-year old hip fracture patients with surgery initiated within 48 hours
Number of diabetes-related major amputations in 100,000 diabetics aged 18-75

Dept Social Medicine
2.4 Effectiveness of long-term carePercentage of people with impairments who indicate that the appliances supplied solve their problems
Percentage of people with somatic complaints who return to their own environment after a stay in a nursing home (as an indicator of the scope of temporary stay function of nursing homes)
Clients’ experiences with home care, nursing homes and care for the disabledVolume of possibly preventable health care problems (such as falls) in nursing home residents
Percentages of patients with decubitus with home care or in nursing homesJudgements of the Health Care Inspectorate on nursing home care
Percentage of home care or nursing home patients who are admitted to a hospital at least once a yearNumber of psychogeriatric patients who live in a small-scale residential care facility
2.5 Effectiveness of care for mental and substance-use conditionsResult of prevention measures and target groups that are reached
Changes in mental and social functioning of patientsDevelopment of the number of suicides and suicide attempts
Percentage of the target group that is reached by care professionalsDevelopment of the number of discharges in mental health care and substance-use care
2.6 Consumers’ experiences with health careGeneral consumers’ trust: do Dutch people have faith in the health care system, irrespective of their actual use of care?
Experiences of consumers: what is opinion of care consumers on the care received? 2.7 Patient safety
Percentage of general practitioners and pharmacists that participate in Farmacotherapeutic Consultations Medication monitoring in pharmacies
Volume of high-risk surgery in hospitalsIncidence of serious adverse effects of blood transfusion
Prevalence of decubitus in hospitalsPrevalence of decubitus in long-term care facilities
2.8 Quality systemsPercentage of institutions that have been certified or accredited
Percentage of institutions that have the necessary quality documentsPercentage of institutions that use special protocols or guidelines that outline procedures for risky or complex processes
Percentage of institutions that use (sub-)systems for feedback of patients and consumers2.9 Innovations
Investments in development and research in the care sector; international comparisonNumber of biotechnology patents in the Netherlands
Utilization and speed of diffusion of minimally non- invasive surgical techniquesUse of process innovations, such as ‘integrated care pathways’ and ‘CVA integrated care’
Application of ICT in various health care sectors
Development in the ratio of surgical day-treatments to the total number of surgical treatments
Dept Social Medicine
Chapter 3. Access3.2 Patient choices in the access to care
Actual use of a number of new choices in care: personal care budget and health insurerWishes of citizens with respect to choices (of health care professional, sources of information and forms of care)
3.3 Accessibility of acute carePercentage of urgent ambulance rides that meets response time targets
Number of urgent ambulance rides that exceeds the standard response time (15 minutes)Number of people who are able to reach the nearest emergency department or out-of-hours primary care centre by car within 30 minutes
Number of urgent callers to out-of-hours general practitioner centres who are answered by an expert within one minuteNumber of people waiting for an organ transplant
3.4 Waiting timesPercentage of patients who are satisfied with the speed with which they are seen by a general practitioner, specialist or dentist
Number of people who wait for care (scope of the waiting list)(Expected) time to treatment (waiting time)
Number of people who have to wait for care longer than the Treeknorm3.5 Accessibility according to need
Comparison of care utilization by low and high educated populations, corrected for health inequalityComparison of care utilization by immigrants and the native population, corrected for health inequality
Care utilization in deprived areas of large cities and by marginal groupsSatisfaction of asylum seekers with medical care
3.6 Financial accessibilityInsurance status of the population, including the number of uninsured
Costs of care for citizensVolume of co-payments and out-of-pocket payments
Tax refunds because of medical expensesAdditional care costs of chronically ill patients
Use of financial compensation provisions by chronically ill patientsPercentage of the family income that is spent on medical expenses by high- versus low- income groups
Share of the total healthcare costs in the Netherlands paid by high- and low-income groups separately (income solidarity in health care)3.7 Geographical accessibility
Accessibility of facilities by required travel time and by number of care facilities per municipality or regionNumber of inpatient and outpatient facilities per region per 10,000 inhabitants
3.8 PersonnelNumber of vacancies in the health care sector that are hard to fill
Rate of sickness absence in health careCurrent unfilled vacancies
Degree to which the current intake of care providers has been tuned to developments in care demandNumber of people that is not registered with a general practitioner or dentist
3.9 Professions and trainingNumber of doctors and nurses per 100,000 inhabitants
Professional ratios: Number of one type of care provider to another type of care provider (e.g. number of dental hygienists to a dentist)Medical-technical tasks carried out by doctor assistants
Number of practice assistants with a higher vocational trainingNumber of experienced graduate physician assistants and nurse practitioners, and number in training
Qualification level of care and nursing staffPercentage of Dutch people who provide informal care

Dept Social Medicine
Chapter 4. Costs
4.2 Macro costsHealth care expenditure according to the Health Budget (BKZ) (Ministry of Health, Welfare and Sports)
Health care expenditure according to the Health Accounts (Statistics Netherlands)Health care expenditure according to the System of Health Accounts (OECD)
Expenditure on the different care sectorsExpenditure on BKZ-relevant care by financing source
Share of health care expenditure in the Gross Domestic ProductShare of health care expenditure in the increase in the Gross Domestic Product
Price development in health careDevelopment in care volume
Costs of care per capita4.3 Health care market
Variation in insurance premiums (health insurance market)Market concentrations of care providers and insurers (health insurance market/ health care purchase market)
Access barriers to the health care market (all sub-markets)Care purchased by insurers (health care purchase market)
Vertical integration (all sub-markets)Mobility of insured persons (health insurance market)Risk selection by insurers (health insurance market)
Transfer of costs (health insurance market)4.4 Productivity of health care
Development of production volume in six care sectors, divided by the number of employees in fte and corrected for reduction of working hoursRecent developments in labour productivity in hospitals compared to recent developments in labour productivity of the Dutch economy as a whole
Number of hospital discharges per fte hospital employee4.5 Financial position of care institutions
ProfitabilitySolvencyLiquidity
Reserves for acceptable costsLevel of participation in the Guarantee Fund for the Care Sector

Dept Social MedicineDraft; not for publication

Dept Social MedicineDraft; not for publication

Dept Social MedicineDraft; not for publication

Dept Social Medicine
Figure 12b. Breast cancer, 5-year relative survival rates. (data for two years when available)
Draft; not for publication

Dept Social Medicine
Lessons learned 2Lessons learned 2
• major information challenges• keeping the links with the policy makers• more need for trends and benchmarking• better visualization• revival BSC• revival link to strategy and policy

Dept Social Medicine

Dept Social Medicine

Dept Social Medicine
Interaction with policymakers,Interaction with policymakers,managers and professionals on:managers and professionals on:
• performance agenda and system reform
• international benchmaking (OECD)
• patient experiences (CQ-Index/CAHPS)
• hospital performance (PATH)
• professional performance (Aire)

Dept Social Medicine
General conclusionsGeneral conclusions
• agreement on goals, timing and generalizability
• agreement on theories and concepts
• study design should fit the question
• interaction on data-collection and reporting
• infrastructure R & D in the health system
• applying principles knowledge management
and learning in the health system







